
Abstract

Keywords
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease frequently associated with cutaneous manifestations, either as part of disease activity or as consequences of long-term therapy. Cutaneous manifestations include malar rash (acute lupus) that typically spares the nasolabial fold, photosensitivity, oral ulcers, subacute cutaneous lupus erythematous (may present as annular scaling erythematous patches on sun-exposed surfaces, as a psoriasiform eruption or as tumid papules on the lids, face and scalp in neonatal lupus), discoid lupus (atrophic disfiguring plaques frequently on the nose and earlobes) and alopecia. Regarding consequences of long-term therapy, topical corticosteroids induce skin atrophy, systemic corticoids may cause violaceous striae, acne, hirsutism, androgenetic alopecia, and hydroxychloroquine may cause a greyish-blueish hyperpigmentation of both the skin and mucosae. Hydroxychloroquine is a cornerstone of SLE management, but prolonged exposure may lead to uncommon dermatologic adverse effects. 1 In addition, certain alopecias and keratinization disorders have been reported in association with autoimmune or systemic conditions, though their coexistence remains rare. 2
We report the case of a 76-year-old female patient who presented to the Dermatology Department with asymptomatic facial hyperpigmentation that had slowly progressed over 2 years and significantly affected her self-esteem. She also reported progressive hair loss over the preceding 5 years and the development of palmar filiform keratotic lesions during the last year. She denied plantar lesions and had no relevant family history. Her medical history included SLE diagnosed at 43, when she presented with malar rash, photosensitivity, arthralgias and alopecia. At the time, she had thrombocytopenia, high ANA titer (1:640), high anti-DS-DNA titers (1382 UI/mL), anti-Ro positive and low C4. She had been receiving continuous treatment with hydroxychloroquine for over 20 years (cumulative dose approximately 2920 g), with good disease control (SLEDAI 0). Physical examination revealed frontal and temporal hairline recession, madarosis, diffuse brown-greyish facial macules and patches (Figure 1(a)) and punctate hyperkeratotic projections on the palms (Figure 1(b)). A clinical diagnosis of frontal fibrosing alopecia was made. Skin biopsies confirmed hydroxychloroquine-induced hyperpigmentation and palmar spiny keratoderma. Malignancy was excluded with a PET-scan. Management focused on the patient’s primary concern, facial hyperpigmentation, with initiation of 20% azelaic acid cream and reduction of the hydroxychloroquine dosage, after discussing with Rheumatology. A satisfactory response was achieved, with improvement in symptoms and the patient’s self-esteem. (a) Frontal fibrosing alopecia and hydroxychloroquine-induced hyperpigmentation: Frontal and temporal hairline recession is noted, as well as madarosis and diffuse facial brown-greyish macules and patches. (b) Spiny keratoderma: Patient presenting with punctate hyperkeratotic projections on her palms.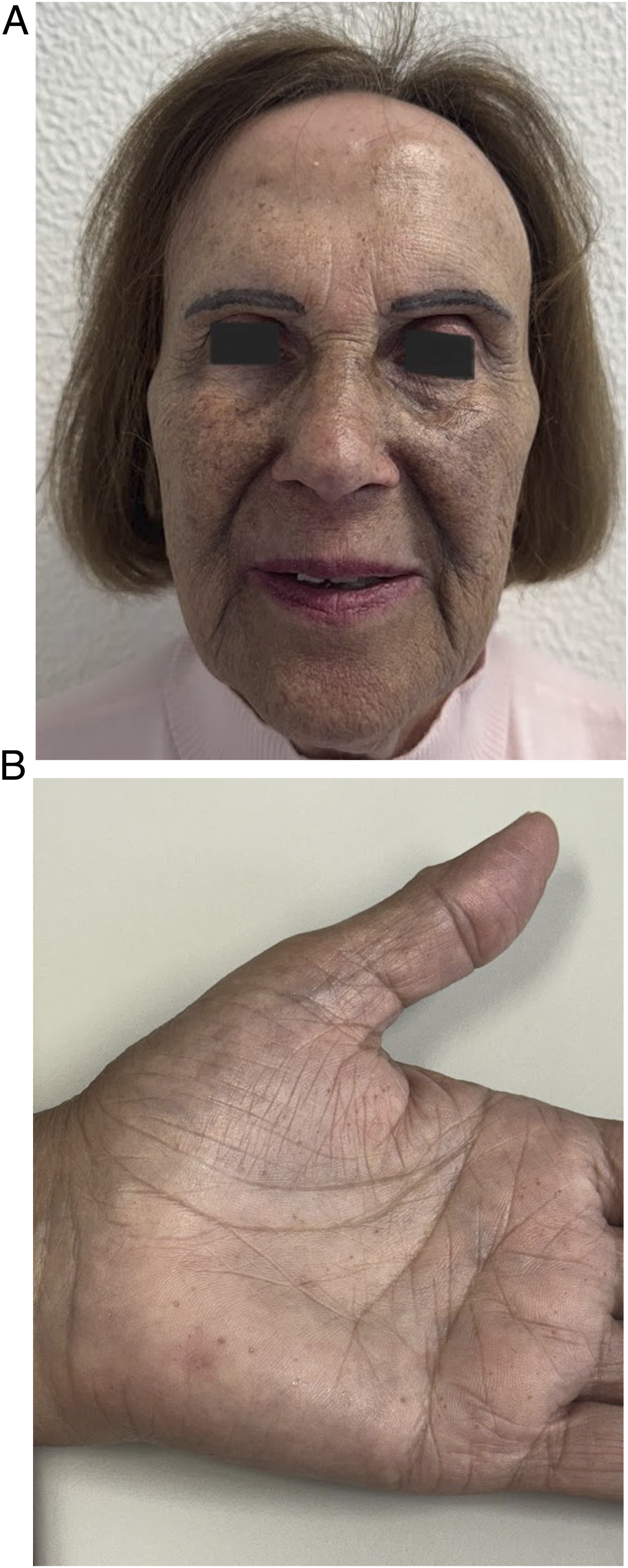
This case illustrates an unusual coexistence of three dermatological conditions – frontal fibrosing alopecia (FFA), hydroxychloroquine-induced hyperpigmentation and spiny keratoderma (SK) – in a patient with longstanding SLE. Each of these findings carries clinical relevance on its own, but their concurrence raises important considerations regarding the chronic cutaneous consequences of autoimmune disease and its long-term management. FFA is a cicatricial alopecia that primarily affects perimenopausal women. Although most often idiopathic, FFA has been associated with autoimmune backgrounds (e.g lupus erythematosus), suggesting that immune dysregulation may play a role in its pathogenesis. 1 Hydroxychloroquine-induced hyperpigmentation, although uncommon, represents a significant skin complication associated with long-term antimalarial use, a common treatment in patients with SLE, that occurs more frequently on the anterior shins, face, oral mucosa and upper limbs. 2 It becomes increasingly likely with cumulative exposure, 3 underscoring the importance of regular monitoring of patients receiving long-term antimalarial therapy. SK is a rare skin disorder affecting the palms and/or soles that has been associated with other systemic diseases, mainly malignancies (such as leukaemia and multiple myeloma) and chronic kidney disease.4,5 Although rare cases of diffuse palmoplantar keratoderma associated with SLE have been described, to our knowledge, this is the first case describing a co-occurrence of SK and SLE. We hypothesize that spiny keratoderma may represent an underreported and underdiagnosed condition, not merely paraneoplastic, but also associated with chronic inflammatory diseases.
This report of a rare combination of three skin diseases in a patient with SLE treated with long-term hydroxychloroquine highlights the importance of dermatological surveillance in patients with autoimmune diseases and/or those receiving long-term antimalarials therapy. Early identification of these manifestations may help prevent complications and optimise therapeutic management.
Footnotes
Consent for publication
The patient in this manuscript has given written informed consent for the use of their de-identified, anonymized, aggregated data and their case details (including photographs) for publication.
Author contributions
Inês Tribolet de Abreu: Data curation, Writing- Original draft preparation, Inês Pereira Amaral: Investigation, Methodology, Leonor Lopes: Conceptualization, Supervision.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.