
Abstract
Objective
Our objective was to explore the correlation between serum (sGal-3) and urinary galectin-3 (uGal-3) levels and renal fibrosis (RF) severity in lupus nephritis (LN) patients, besides assessing their diagnostic performance for identifying moderate/severe interstitial fibrosis and tubular atrophy (IFTA).
Methods
This cross-sectional controlled study recruited 150 participants: 50 LN patients, 50 diagnosed with systemic lupus erythematosus (SLE) without LN, and 50 healthy controls. Both sGal-3 and uGal-3 levels were measured using ELISA. Histopathological assessment included evaluation of IFTA severity. Patients with LN were stratified into mild IFTA (<26%) and moderate/severe IFTA (≥26%). Moreover, we performed correlation, ROC curve, and multivariable logistic regression analyses.
Results
LN patients showed significantly higher sGal-3 and uGal-3 levels than other groups (p < 0.001). Both biomarkers exhibited strong positive correlations with IFTA percentage (sGal-3: rho = 0.76; uGal-3: rho = 0.81; p < 0.001). Unlike those with mild IFTA, moderate/severe IFTA patients had significantly higher sGal-3 and uGal-3 levels (p < 0.001). Based on ROC analysis, uGal-3 had higher discriminatory ability for moderate/severe IFTA (AUC = 0.903) than sGal-3 (AUC = 0.801). In multivariable logistic regression, both sGal-3 and uGal-3 levels were independently associated with moderate/severe IFTA after adjusting for renal function parameters.
Conclusions
Both sGal-3 and uGal-3 levels are significantly associated with RF severity in LN. The uGal-3 had superior diagnostic performance for moderate/severe IFTA and may be a promising non-invasive RF biomarker in LN. Validation in large-scale prospective studies is warranted.
Introduction
Chronic renal injury as well as progressive fibrotic remodeling constitute major pathological mechanisms underlying the deterioration of kidney function in several glomerular disorders: lupus nephritis (LN). As a serious systemic lupus erythematosus (SLE) complication, LN contributes significantly to long-term morbidity and fatality. Although immunosuppressive therapies have advanced considerably, LN continues to be a major contributor to end-stage renal disease (ESRD). Histopathological characteristics such as interstitial fibrosis and tubular atrophy (IFTA), alongside vascular and glomerular abnormalities, represent important predictors of renal survival and prognosis in LN individuals. At present, renal biopsy remains the reference standard for evaluating these pathological alterations: structural injury and chronicity indices. Nevertheless, biopsy represents an invasive procedure associated with potential complications and limited feasibility for repeated assessments, thereby restricting its application in continuous disease monitoring alongside longitudinal evaluation. 1 These limitations highlight the pressing urgency for reliable non-invasive biomarkers capable of reflecting ongoing renal structural damage, especially fibrosis, aiming at supporting early diagnosis, risk stratification, and improved clinical LN management.
Galectin-3 (Gal-3), a β-galactoside-binding lectin, represents a renal injury biomarker by contributing to cellular differentiation, proliferation, immune regulation, and extracellular matrix remodeling, all of which contribute to the progression of renal fibrosis.2,3 Overexpressed Gal-3 promotes fibroblast activation, inflammatory responses, and tissue remodeling, resulting in renal scarring and progressive functional deterioration. A biopsy-based investigation reported significantly elevated plasma Gal-3 concentrations in chronic kidney disease (CKD) patients, unlike individuals without CKD. Furthermore, Gal-3 levels displayed a negative relation to eGFR and a positive relation to histopathological fibrosis markers, including tubular atrophy, interstitial fibrosis, and vascular intimal fibrosis. 3 Additionally, patients within the highest urinary Gal-3 (uGal-3) tertile demonstrated more severe renal dysfunction, higher levels of proteinuria, and an increased likelihood of progression to ESRD. Collectively, uGal-3 may be a valuable non-invasive biomarker of renal structural injury and disease progression. 4
Since fibrosis and tubular atrophy represent irreversible pathological alterations that are strongly connected to unfavorable long-term outcomes, early identification of fibrotic remodeling possesses major clinical importance in LN. 5 Serum Gal-3 (sGal-3) showed significantly high levels in LN patients, unlike healthy controls and SLE patients without renal involvement, which were related to impaired renal function and histopathological indicators of chronic injury, including IFTA. 4 In addition, immunohistochemical analyses have demonstrated enhanced glomerular and tubular Gal-3 expression in renal tissue obtained from patients with LN, with expression levels positively correlating with both disease activity and chronicity indices. 6 Taken together, these observations suggest that Gal-3 may function as a mechanistic mediator linking autoimmune renal damage to fibrotic progression in LN.
Nevertheless, limited studies have concurrently evaluated both sGal-3 and uGal-3 concentrations in LN, and standardized cutoff values for assessing fibrosis severity in this patient population remain unavailable. Furthermore, previous studies conducted in broader CKD populations rather than LN-specific cohorts have reported inconsistent findings regarding the prognostic utility of Gal-3 for cardiovascular and renal outcomes. Owing to the distinct LN immunopathological features, including simultaneous glomerular and tubulointerstitial damage as well as immune complex deposition, further validation of Gal-3 as a disease-specific, non-invasive indicator in biopsy-confirmed LN is warranted. 7
Accordingly, we aimed to investigate if patients with biopsy-proven LN demonstrate significantly elevated sGal-3 and uGal-3 levels compared with matched control groups: healthy subjects and SLE patients without LN. Additionally, we examined the associations between these biomarkers and major clinical parameters of renal dysfunction, including eGFR and proteinuria, as well as histopathological markers of fibrosis, such as IFTA and chronicity index scores.
Patients and methods
Study design and participants
Between July 2025 and November 2025, this cross-sectional observational study recruited 150 participants from the outpatient clinics and inpatient units of the Rheumatology and Nephrology Departments and were equally assigned (n = 50/group) into three age- and sex-matched groups 1 : patients with biopsy-proven LN 2 ; non-LN SLE patients 3 ; healthy controls.
Eligible participants were aged 18 years or older who met the 2019 EULAR/ACR classification criteria for SLE. 8 Patients with clinically suspected nephritis underwent renal biopsy according to KDIGO recommendations, which advise biopsy in cases of albuminuria and/or decreased eGFR. 9 Individuals were excluded if they had a history of active malignancy, sepsis, diabetes mellitus, chronic hepatic disorder, uncontrolled hypertension, established cardiovascular disease, or coexisting autoimmune disorders.
The Research Ethics Committee authorized the study (36264PR1300/7/25), which adhered to the Declaration of Helsinki, with all participants signing informed consent.
Clinical evaluation
Participants were subjected to a detailed clinical assessment of disease duration, therapeutic history, clinical manifestations, and previous renal biopsy results when available. Based on the SLEDAI, disease activity was determined and classified into the following categories: inactive disease (SLEDAI = 0), mild,1–5 moderate,6–10 high,11–19 and very high (≥20). 10 Demographic and clinical characteristics were systematically documented for all participants. In patients with SLE, current treatment regimens, including corticosteroid therapy and immunosuppressive medications, were also recorded. Blood and urine specimens were obtained while patients were under stable treatment conditions, without any major therapeutic changes immediately preceding sample collection.
Laboratory investigations
From all participants, venous blood and midstream urine specimens were obtained under sterile conditions either at the renal biopsy time for LN patients or during routine clinical follow-up visits for healthy controls and patients with SLE without LN, prior to any interventional procedures. Laboratory assessments comprised complete blood count (CBC), serum creatinine, blood urea nitrogen, serum albumin, anti-dsDNA antibodies, antinuclear antibodies (ANA), complement levels (C3 and C4), urinary protein-to-creatinine ratio (UPCR), alongside sGal-3 and uGal-3 levels.
CBC analysis was carried out on EDTA-anticoagulated blood samples using an ERMA automated hematology analyzer (Japan). Serum urea, albumin, and creatinine concentrations were analyzed through the INDIKO Plus automated chemistry analyzer (Finland). Both C3 and C4, as well as urinary protein levels, were measured by the Cobas c311 automated analyzer (HITACHI, Germany). To ascertain ANA and anti-dsDNA antibody levels, ELISA was performed through ORGENTEC Diagnostika kits (ORG600 and ORG604; Germany). Through the AssayMax Human Gal-3 ELISA Kit, we assessed sGal-3 and uGal-3 concentrations (EG3311-1; AssayMax, USA). ELISA procedures followed the instructions, and absorbance was recorded at 450 nm via a calibrated microplate reader.
Histopathological evaluation
Based on the ISN/RPS classification system, renal biopsy samples from LN patients were evaluated, and IFTA extent was semi-quantitatively assessed: grade 0 (<5%), 1 (5–25%), 2 (26–50%), and 3 (>50%). The chronicity index was also calculated. These histologic parameters served as reference standards for correlating structural damage with both sGal-3 and uGal-3 levels. For analytical purposes, patients were stratified into mild IFTA (grades 0–1; <26%) and moderate/severe IFTA (grades 2–3; ≥26%).
Statistical analysis
Statistical analyses were carried out with SPSS software (v 26.0, IBM Corp., Armonk, NY, USA). Data normality was ascertained via the Shapiro–Wilk test. Data are presented as mean ± SD or median (IQR), while presenting qualitative variables as frequencies and percentages. Between-group comparisons were performed by the independent t-test, one-way ANOVA, Mann–Whitney U test, or chi-square test, as appropriate. Correlations were ascertained through Spearman’s rank correlation coefficient.
The ROC curve analysis was conducted to evaluate sGal-3 and uGal-3 diagnostic performance for identifying moderate/severe IFTA (≥26%). The DeLong test was utilized to compare ROC curves. Binary logistic regression analysis was employed to identify independent moderate/severe IFTA predictors. Model calibration was ascertained via the Hosmer–Lemeshow test, and multicollinearity was determined using the variance inflation factor (VIF). A two-sided p < 0.05 indicated significance.
Results
Baseline characteristics
Baseline characteristics of the participants.
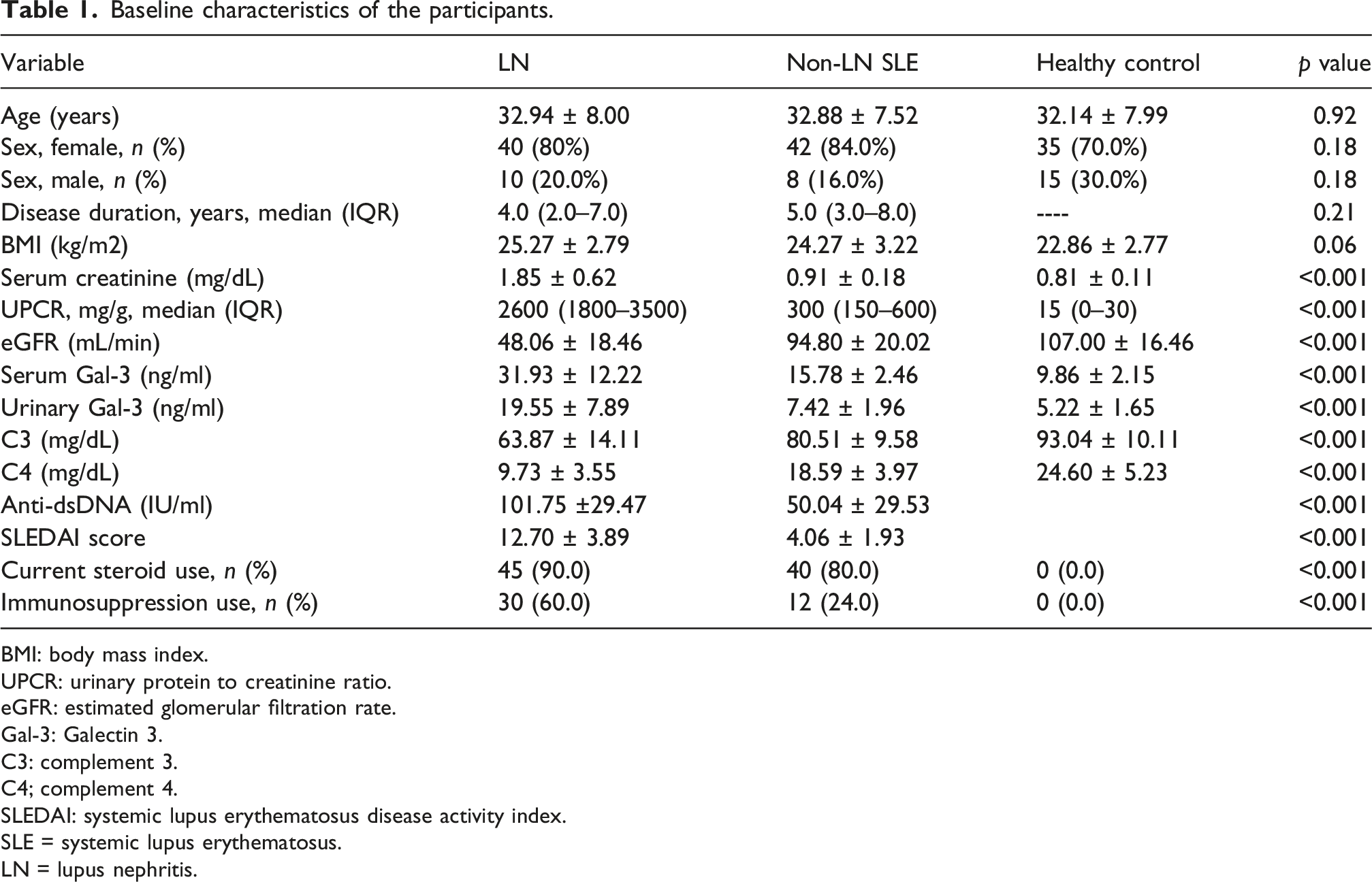
BMI: body mass index.
UPCR: urinary protein to creatinine ratio.
eGFR: estimated glomerular filtration rate.
Gal-3: Galectin 3.
C3: complement 3.
C4; complement 4.
SLEDAI: systemic lupus erythematosus disease activity index.
SLE = systemic lupus erythematosus.
LN = lupus nephritis.
Gal-3 levels and IFTA severity
Comparison of serum and urinary Gal-3 levels according to IFTA severity in LN patients.

Gal-3: Galectin 3
IFTA = interstitial fibrosis and tubular atrophy.
Gal-3 levels and histopathological parameters
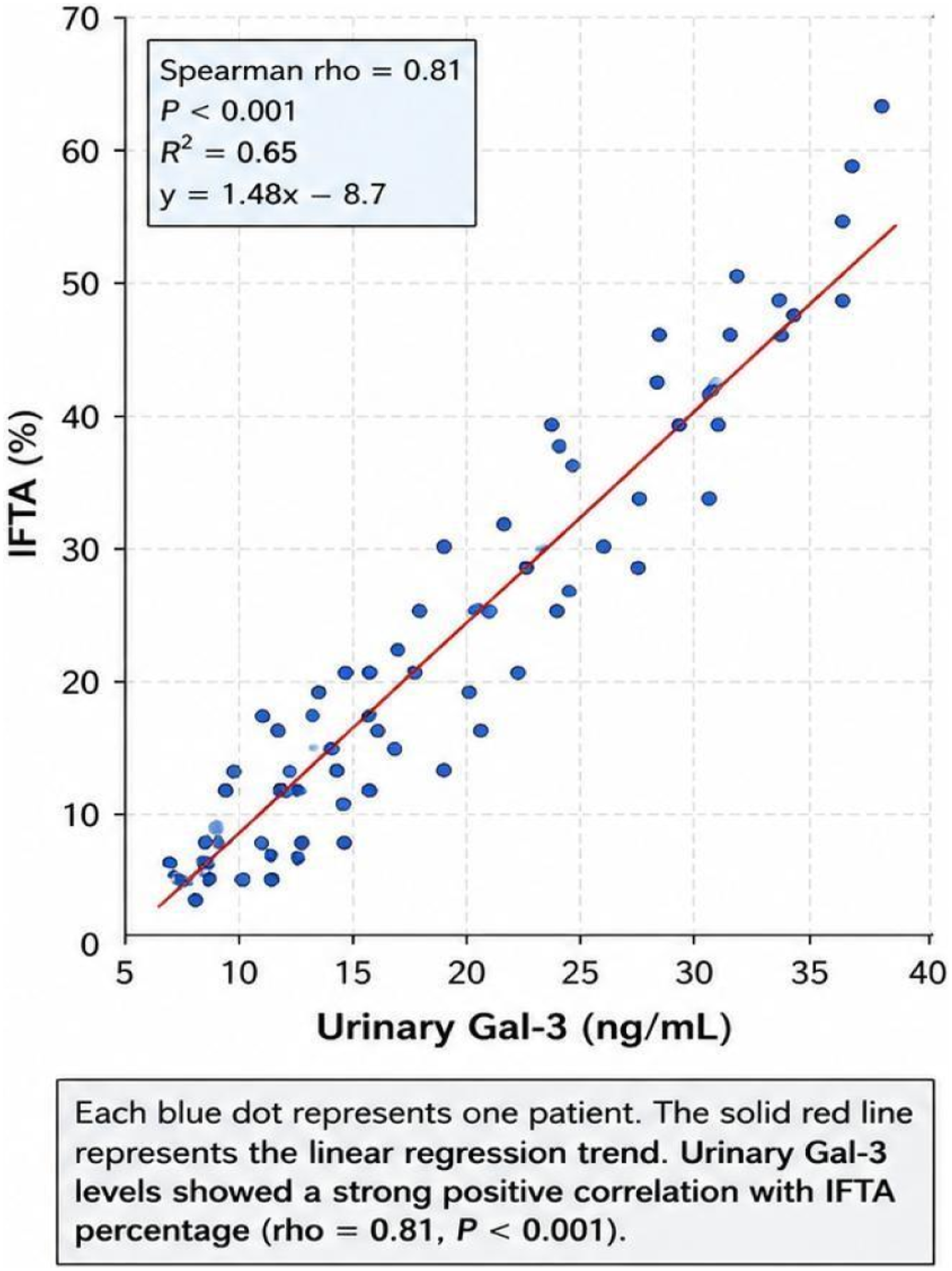
The outcomes manifested a significant positive correlation between Gal-3 levels and IFTA percentage in LN patients. SGal-3 correlated positively with IFTA percentage (rho = 0.76; p < 0.001), while uGal-3 demonstrated a stronger positive correlation (rho = 0.81; p < 0.001). Scatter plots illustrated progressive increases in both sGal-3 and uGal-3 levels with increasing severity of renal fibrosis (RF) (Figures 1–2). Correlation between serum Gal-3 and IFTA percentage in LN patients. Correlation between urinary Gal-3 and IFTA percentage in LN patients.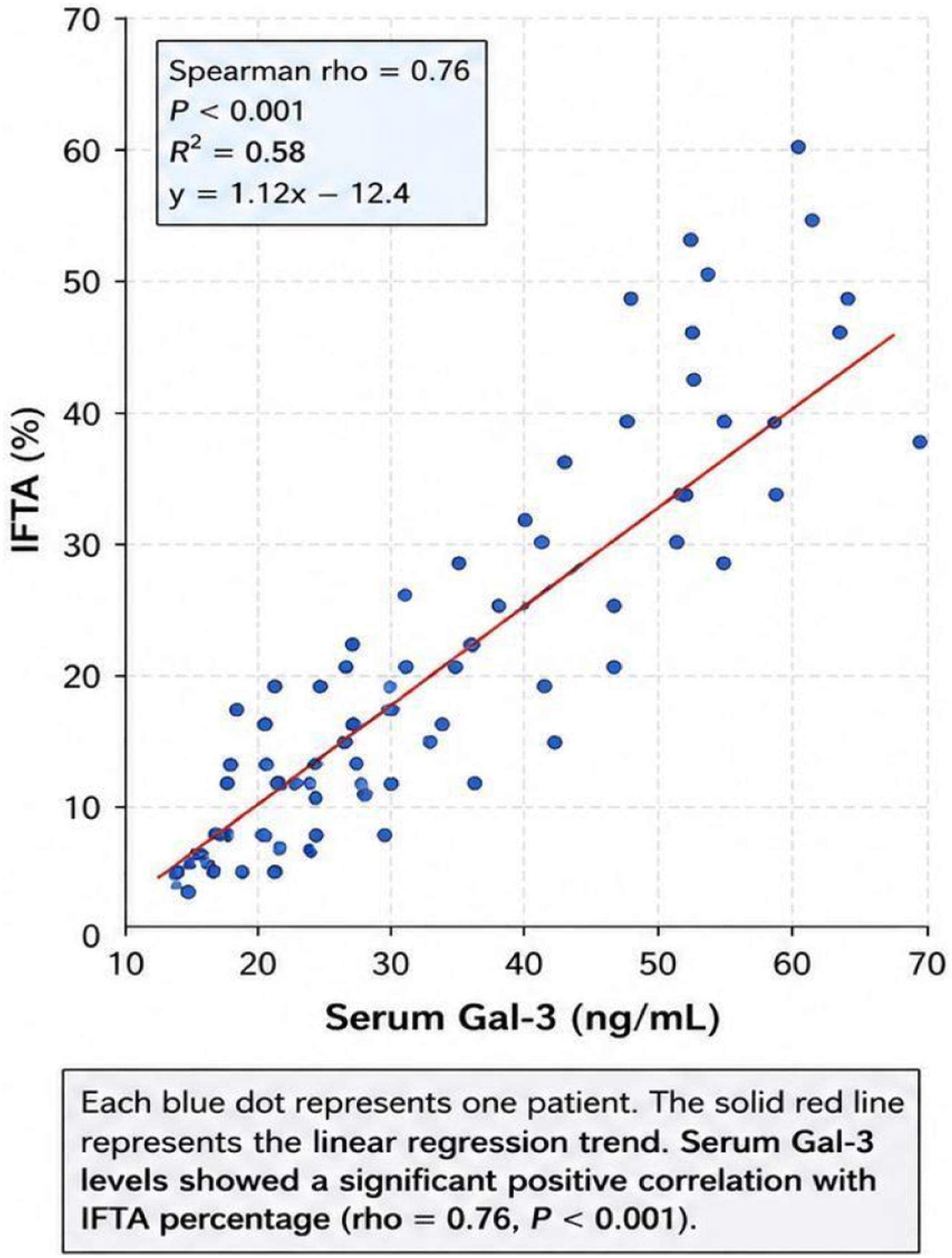
Correlation between serum/Urinary Gal-3 and clinical-histopathological parameters in LN patients (N = 50).
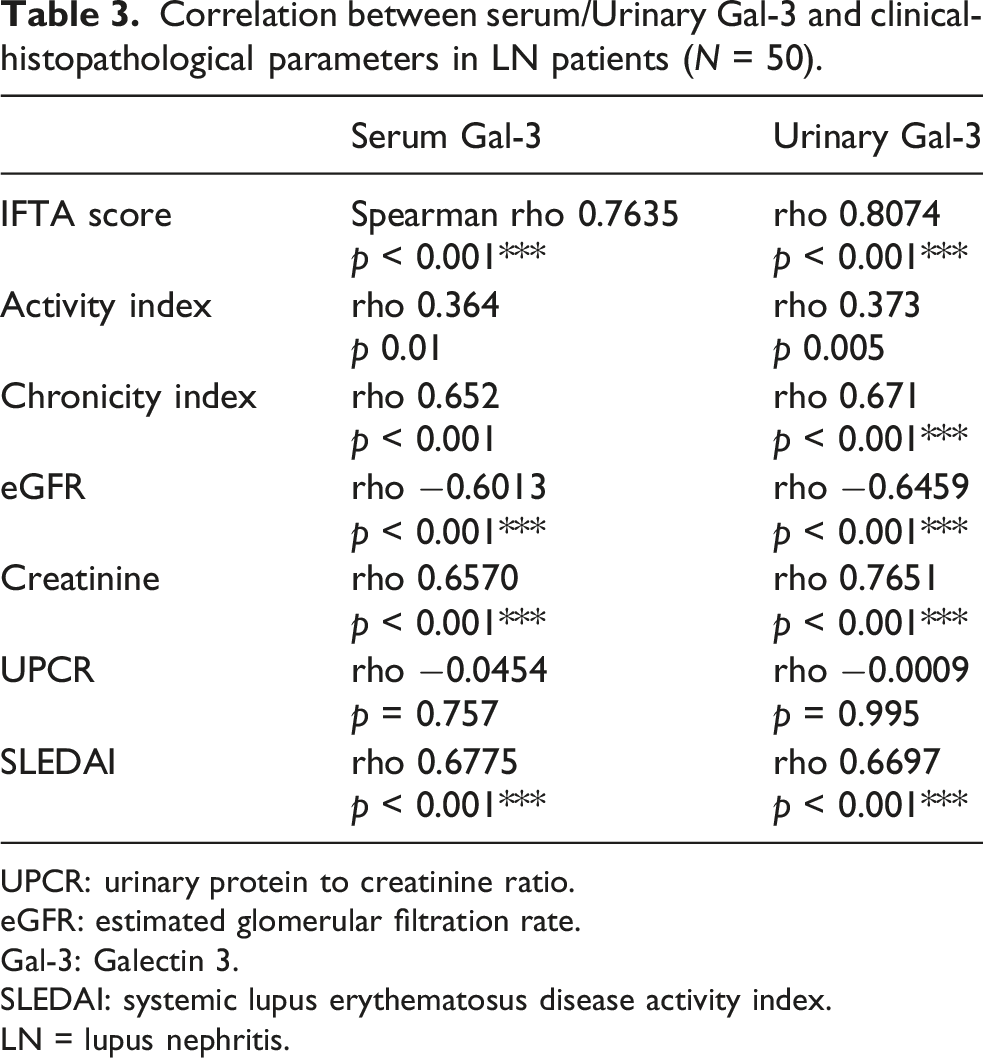
UPCR: urinary protein to creatinine ratio.
eGFR: estimated glomerular filtration rate.
Gal-3: Galectin 3.
SLEDAI: systemic lupus erythematosus disease activity index.
LN = lupus nephritis.
Gal-3 variation across LN classes
Serum and urinary Gal-3 levels across LN classes and IFTA distribution.
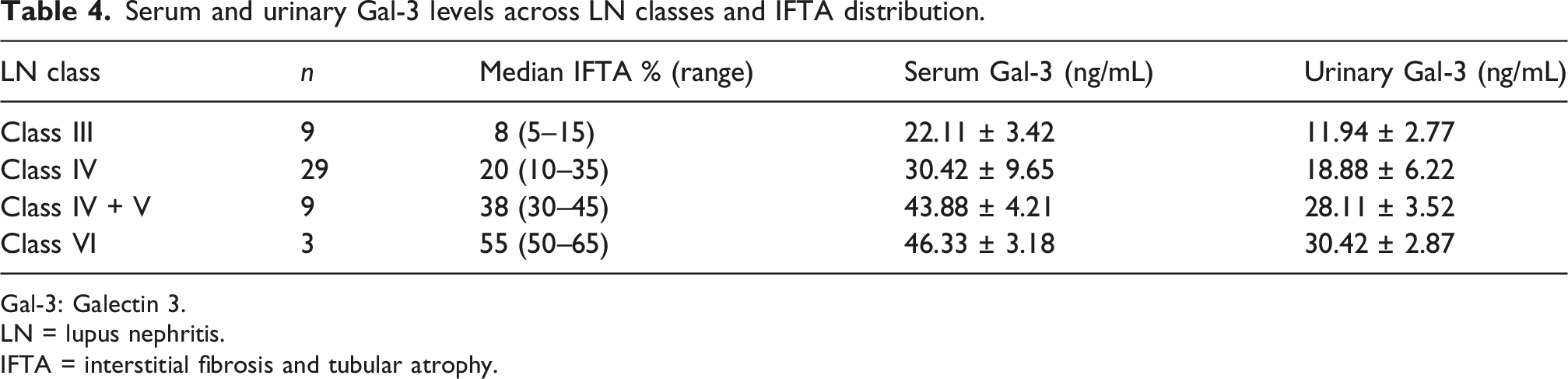
Gal-3: Galectin 3.
LN = lupus nephritis.
IFTA = interstitial fibrosis and tubular atrophy.
Distribution of LN patients according to IFTA severity
Distribution of LN patients according to IFTA severity.
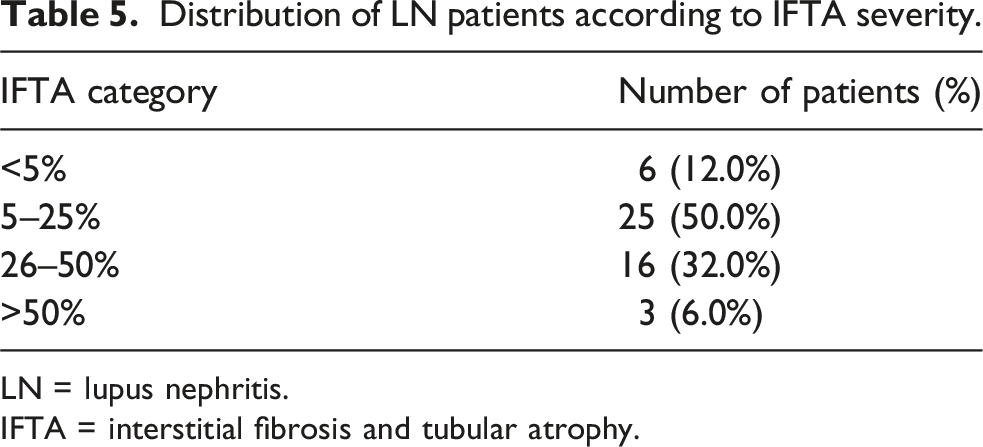
LN = lupus nephritis.
IFTA = interstitial fibrosis and tubular atrophy.
Diagnostic performance of both sGal-3 and uGal-3 for moderate/Severe IFTA
ROC analysis of serum and urinary Gal-3 for detection of moderate/severe IFTA (≥26%).
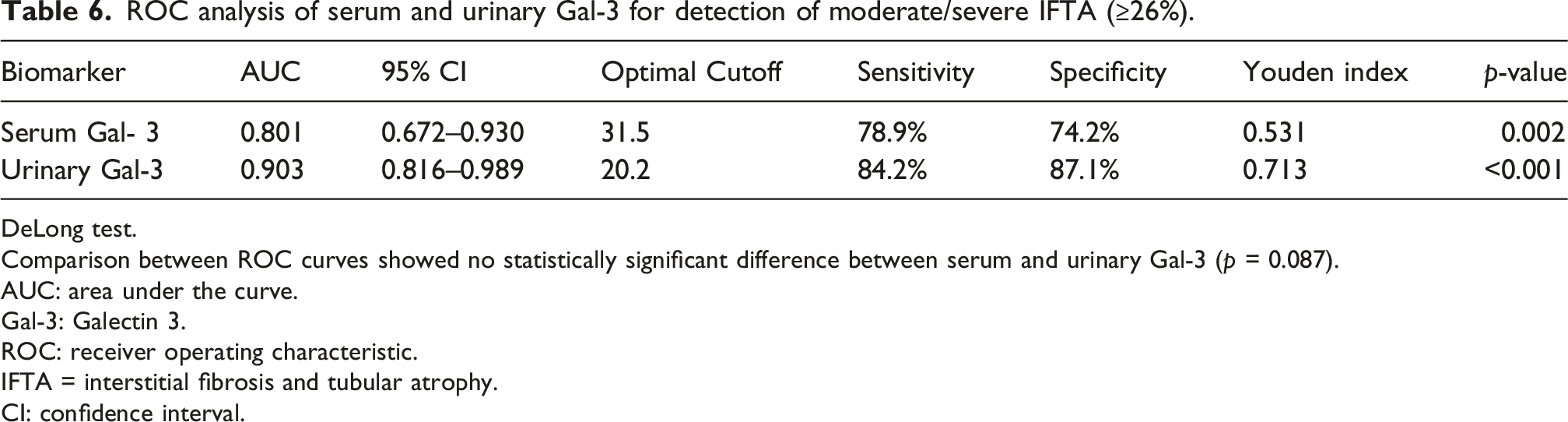
DeLong test.
Comparison between ROC curves showed no statistically significant difference between serum and urinary Gal-3 (p = 0.087).
AUC: area under the curve.
Gal-3: Galectin 3.
ROC: receiver operating characteristic.
IFTA = interstitial fibrosis and tubular atrophy.
CI: confidence interval.
Multivariable logistic regression analysis
Multivariable logistic regression analysis for predictors of moderate/Severe IFTA in LN patients (serum model).
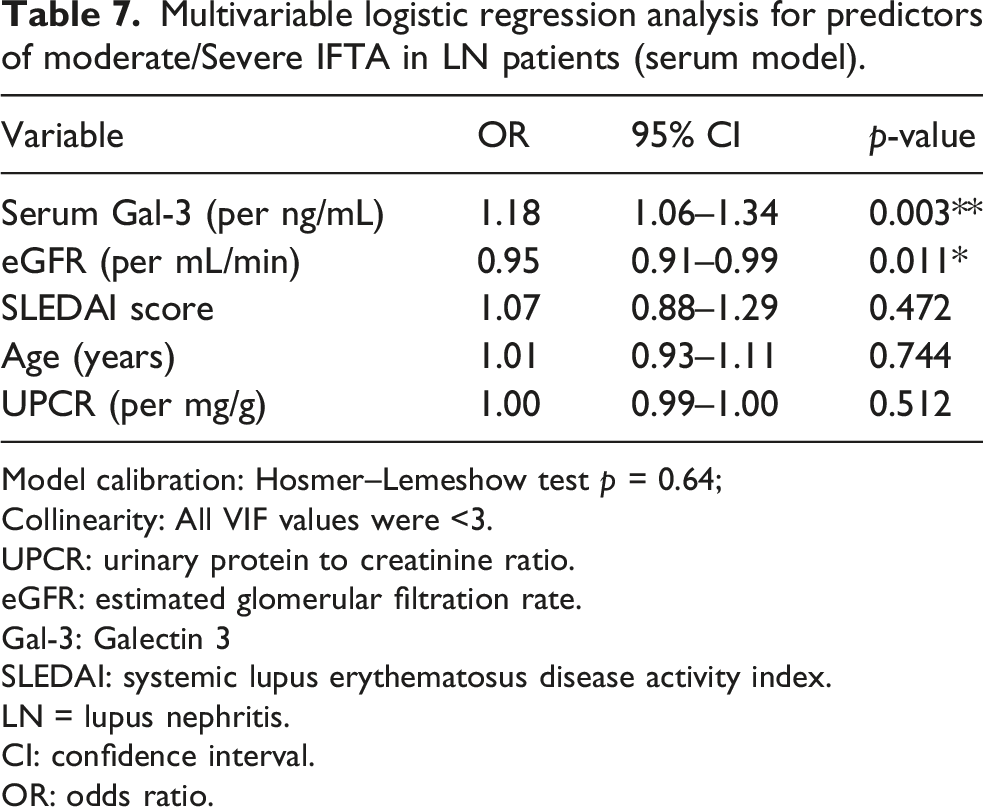
Model calibration: Hosmer–Lemeshow test p = 0.64;
Collinearity: All VIF values were <3.
UPCR: urinary protein to creatinine ratio.
eGFR: estimated glomerular filtration rate.
Gal-3: Galectin 3
SLEDAI: systemic lupus erythematosus disease activity index.
LN = lupus nephritis.
CI: confidence interval.
OR: odds ratio.
Multivariable logistic regression analysis for predictors of moderate/severe IFTA in LN patients (urinary model).
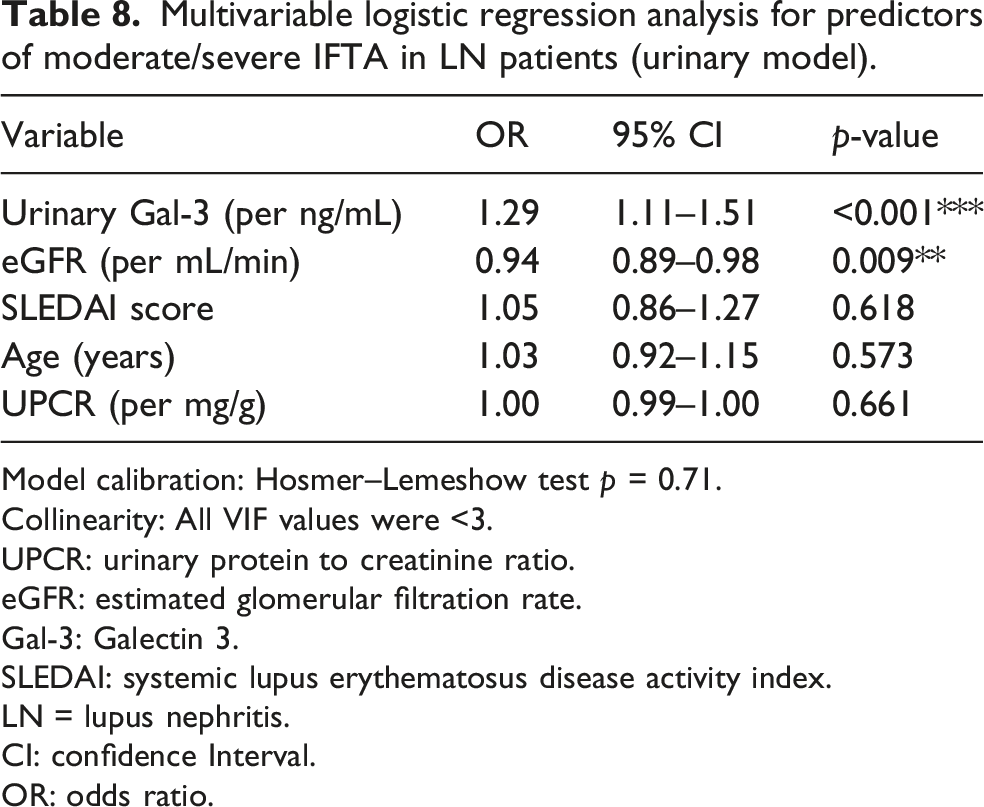
Model calibration: Hosmer–Lemeshow test p = 0.71.
Collinearity: All VIF values were <3.
UPCR: urinary protein to creatinine ratio.
eGFR: estimated glomerular filtration rate.
Gal-3: Galectin 3.
SLEDAI: systemic lupus erythematosus disease activity index.
LN = lupus nephritis.
CI: confidence Interval.
OR: odds ratio.
Model calibration was acceptable for both models. Multicollinearity diagnostics showed no evidence of severe collinearity among predictors, with all VIF values below 3.
Discussion
LN is still among the most serious SLE complications, markedly implicated in CKD progression and long-term morbidity. RF, particularly IFTA, constitutes the eventual frequent pathway of progressive renal damage and is strongly associated with poor renal outcomes, independent of underlying glomerular pathology. Consequently, identifying reliable non-invasive biomarkers that reflect the extent of RF has become a priority in nephrology research. In this study, LN patients displayed significantly higher sGal-3 and uGal-3 levels than those with non-LN SLE and healthy controls. Furthermore, Gal-3 levels demonstrated significant associations with histopathological indices of fibrosis, indicating its potential role as a renal fibrotic remodeling biomarker in LN.11,12
Gal-3 is implicated in macrophage activation, inflammation, fibroblast proliferation, extracellular matrix deposition, and tissue remodeling. Clinically, Gal-3 contributes directly to fibrogenesis in several organs, including the kidney, heart, and liver. Within renal tissue, Gal-3 expression is related to tubular epithelial injury, myofibroblast activation, and the progression of tubulointerstitial fibrosis. These mechanisms provide a biological basis for the positive correlations observed between Gal-3 levels and IFTA severity in our cohort, aligning with previous studies evaluating Gal-3 in CKD and inflammatory renal disorders, thereby reinforcing its plausibility as a fibrotic burden marker.13–15
Herein, a key finding is that uGal-3 outperformed sGal-3 in reflecting renal fibrotic burden. UGal-3 demonstrated stronger correlations with IFTA percentage, higher discriminatory performance in ROC analysis, and greater predictive value in multivariable regression models. This observation may be ascribed to the fact that urinary biomarkers more directly mirror local intrarenal pathological processes, whereas circulating biomarkers may be influenced by systemic inflammation, impaired renal clearance, and extra-renal sources. Similar patterns have been reported for other urinary fibrosis biomarkers, including MCP-1, TGF-β, and neutrophil gelatinase-associated lipocalin (NGAL).16–18 Thus, uGal-3 may represent a more kidney-specific indicator of tubulointerstitial injury and fibrosis in LN.
Moreover, we observed a progressive increase in both sGal-3 and uGal-3 levels across advancing LN classes and increasing degrees of IFTA involvement. Patients with proliferative lesions (Class III/IV) and advanced chronic lesions (Class VI) exhibited the highest biomarker levels. This pattern supports the hypothesis that Gal-3 expression parallels ongoing inflammatory and fibrotic activity. Given that chronic histopathological changes strongly influence long-term renal prognosis in LN, biomarkers reflecting chronicity rather than isolated inflammatory activity may offer significant clinical utility. In this context, Gal-3 may facilitate the non-invasive monitoring of fibrosis progression and chronic renal injury in patients with LN.12,15,19
A methodological consideration in interpreting these results is the close association between RF and declining renal function. Reduced eGFR may contribute to elevated circulating Gal-3 levels by impairing renal clearance. Thus, sGal-3 may partially reflect declining renal function rather than serving as a purely fibrosis-specific biomarker. Indeed, sGal-3 correlated significantly with serum creatinine and eGFR in our cohort. However, multivariable logistic regression analyses manifested that Gal-3 remained independently related to moderate/severe IFTA after adjusting for eGFR and other covariates. Additionally, collinearity diagnostics revealed no severe multicollinearity among predictors. These findings suggest an independent association between Gal-3 and RF beyond simple filtration impairment, although residual confounding cannot be entirely excluded.20–22
ROC analysis indicated good diagnostic performance for both sGal-3 and uGal-3 in identifying moderate/severe IFTA, with uGal-3 showing superior discrimination. However, caution is warranted when interpreting these promising AUC values, given the relatively small sample size and the study’s exploratory nature. Small cohorts increase the risk of model overfitting and may limit generalizability to external populations. Although calibration analysis by the Hosmer–Lemeshow goodness-of-fit test demonstrated acceptable model fit, larger multicenter validation studies are necessary before clinical implementation can be recommended.23,24
The study is constrained, first, its cross-sectional design precludes establishing causal relations and does not permit assessing longitudinal variations in Gal-3 levels over time. Second, the study’s single-center nature and the relatively small sample size may constrain the generalization of the findings. Third, uGal-3 concentrations were not normalized to urinary creatinine, which may introduce variability related to urine concentration and hydration status. Fourth, medication exposure, particularly intensive immunosuppressive therapy in LN patients, may have influenced biomarker levels. Finally, despite adjustment for eGFR, the complex interplay between RF, inflammation, and renal function decline may still contribute to residual confounding. Future prospective multicenter studies with serial biomarker assessment and standardized urinary normalization should define Gal-3 clinical utility in LN.21,25
Despite these limitations, this study provides evidence supporting the potential Gal-3 utility as a non-invasive RF biomarker in LN. The combined evaluation of sGal-3 and uGal-3, particularly uGal-3, may provide clinically relevant information on chronic tubulointerstitial injury and fibrosis severity. If validated in larger longitudinal cohorts, Gal-3-based approaches may improve risk stratification, facilitate earlier detection of chronic renal injury, and enable individualized monitoring strategies for patients with LN.12,14,18
Conclusion
Both sGal-3 and uGal-3 levels were significantly heightened in patients with biopsy-proven LN, unlike those having non-renal SLE and healthy controls. Gal-3 levels demonstrated strong associations with histologically quantified IFTA, with uGal-3 showing superior discriminative performance for moderate/severe fibrosis. Collectively, Gal-3, particularly in urine, may be a promising non-invasive renal fibrotic burden biomarker in LN. However, given the cross-sectional design, further longitudinal studies should establish its prognostic value and specificity across different etiologies of CKD.
Footnotes
Author contributions
A.M.F.: Study Conception and Design, Clinical Data Collection, and Writing-Original Draft. R.Y.H.: Data Interpretation and Literature Review. A.M.E.: Writing – Review & Editing. A.M.R.: Clinical Data Collection and Data Interpretation. A.E.: Statistical Analysis and Data Collection. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon request.