
Abstract
Objective
To examine patient-reported adherence to the American College of Rheumatology (ACR) reproductive health guidelines among females of childbearing age with systemic lupus erythematosus (SLE) seen at a tertiary care center.
Methods
Females with SLE aged 18–50 years who were evaluated by a rheumatologist at a tertiary care center from January 2022 to March 2024 were invited to complete an online survey. The survey assessed whether reproductive health topics had been discussed with their rheumatologists, including: contraception, pregnancy planning (i.e., medication compatibility and disease remission), and hydroxychloroquine (HCQ) use during preconception and pregnancy. Descriptive statistics were used to summarize the characteristics of all participants and reproductive health outcomes. Exploratory bivariate analyses identified factors associated with use of effective or highly effective contraception (EHEC), contraceptive counseling, and screening for pregnancy plans among females of reproductive potential.
Results
The cross-sectional study included 102 participants (mean age 35 years). Most participants identified as White (36.3%) or Asian/Pacific Islander (32.4%). Among participants with pregnancy history after SLE diagnosis (n = 34), most reported having pregnancy planning discussions, including HCQ use, with their rheumatologist. However, fewer than one-third of all participants reported receiving contraceptive counseling by their rheumatologist in the past year. In exploratory analyses, contraceptive counseling varied significantly by race, employment status, disease duration, and who was most likely to initiate reproductive health conversations. EHEC use varied significantly by race, with numerically higher use among White participants (59.4%).
Conclusion
Our findings highlight specific gaps in reproductive healthcare among females with SLE, alongside areas of high adherence with guidelines. Notable differences in contraceptive use and counseling underscore important opportunities to deliver quality care in this high-risk patient population.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that disproportionately affects women of childbearing age.1 Pregnancy in SLE requires careful planning,2 including optimal disease control and ensuring that medications are compatible prior to conception. The American College of Rheumatology (ACR) has set forth comprehensive guidelines on the management of reproductive health in patients with rheumatic diseases.3 For females with SLE of reproductive potential, rheumatologists are recommended to provide counseling across key domains: contraceptive use; pregnancy planning (i.e., disease remission and medication compatibility); and continuation of hydroxychloroquine (HCQ) prior to and during pregnancy. The extent to which these guidelines are incorporated into the real-world care of females with SLE remains unclear.
Appropriate contraceptive use is essential for reducing the risk of unintended pregnancy among women of reproductive potential. This is particularly important in women with SLE, who are at higher risk of pregnancy-related morbidity and mortality, due largely to increased disease activity, chronic organ damage, and exposure to teratogenic medications. 2 Effective or highly effective contraception (EHEC) is the favored method outlined by the ACR guidelines, with preference for highly effective methods (i.e., long-acting reversible contraceptives [LARC] such as intrauterine devices and implants) due to their low failure rate and lack of estrogen. Studies prior to the release of the ACR Reproductive Health guidelines revealed variable rates of contraception use among females with SLE of childbearing age,3–6 including low use of LARC methods (3% to 13%).4–6 Inconsistent use of contraception and dependance on less effective methods (i.e., condoms) place many patients with SLE at high risk of unintended pregnancies. 5
Optimal disease control, including continued use of HCQ before and during pregnancy, is critical to minimizing the risk of adverse pregnancy outcomes among females with SLE. Claims-based studies highlight suboptimal prescription of HCQ prior to and during pregnancy including discontinuation of the medication.7,8 A population-based study which captured both prescriptions and fills of medications found that although a majority of patients with SLE filled a prescription for HCQ prior to and during pregnancy, approximately 30% did not have a prescription by their provider. 9 The findings suggest that adherence may not be purely patient-driven. Physician and system-level determinants need to be accounted for. Taken together, these patterns of low uptake may stem from conversations on reproductive health, or lack thereof, in the clinical setting. A survey-based study reported gaps in reproductive health conversations among a cohort of predominantly Hispanic population in an urban setting. 10 The prevalence of these discussions in other clinical settings is not well understood, warranting further investigation.
Collectively, these studies highlight suboptimal uptake of different domains of reproductive health counseling among females with SLE. However, most were conducted prior to the release of the ACR 2020 Reproductive Health Guidelines and within limited clinical settings. Patient-reported experiences of reproductive health counseling following the release of the guidelines remain understudied. Understanding the uptake of these guidelines from the patient perspective is essential to identify persistent gaps and inform targeted interventions to improve care.
We therefore conducted a cross-sectional study using a modified survey instrument to evaluate patient-reported experiences among females with SLE of childbearing age (18–50 years) who received care from rheumatologists at a tertiary care center following the release of ACR Reproductive Health guidelines. We hypothesize that gaps in reproductive health counseling persist across key domains — including contraceptive use, pregnancy planning, and HCQ use — among females with SLE of childbearing age despite the release of ACR guidelines.
Methods
Study design and population
A cross-sectional survey was administered to females with SLE of childbearing age (18–50 years) who recently received care at Stanford Health Care. Eligible participants were identified through the Stanford Research Repository (STARR), a comprehensive data platform that includes electronic health records of patients seen at Stanford (Figure 1). To minimize misclassification and confirm eligibility, medical charts were manually reviewed by two rheumatologists (AS, YC) based on the following criteria: (1) a clinical diagnosis of SLE by a rheumatologist, and (2) receipt of rheumatology care at Stanford between 01/01/2022 and 03/31/2024 with ongoing regular follow-up in the clinic. Selection of eligible patients.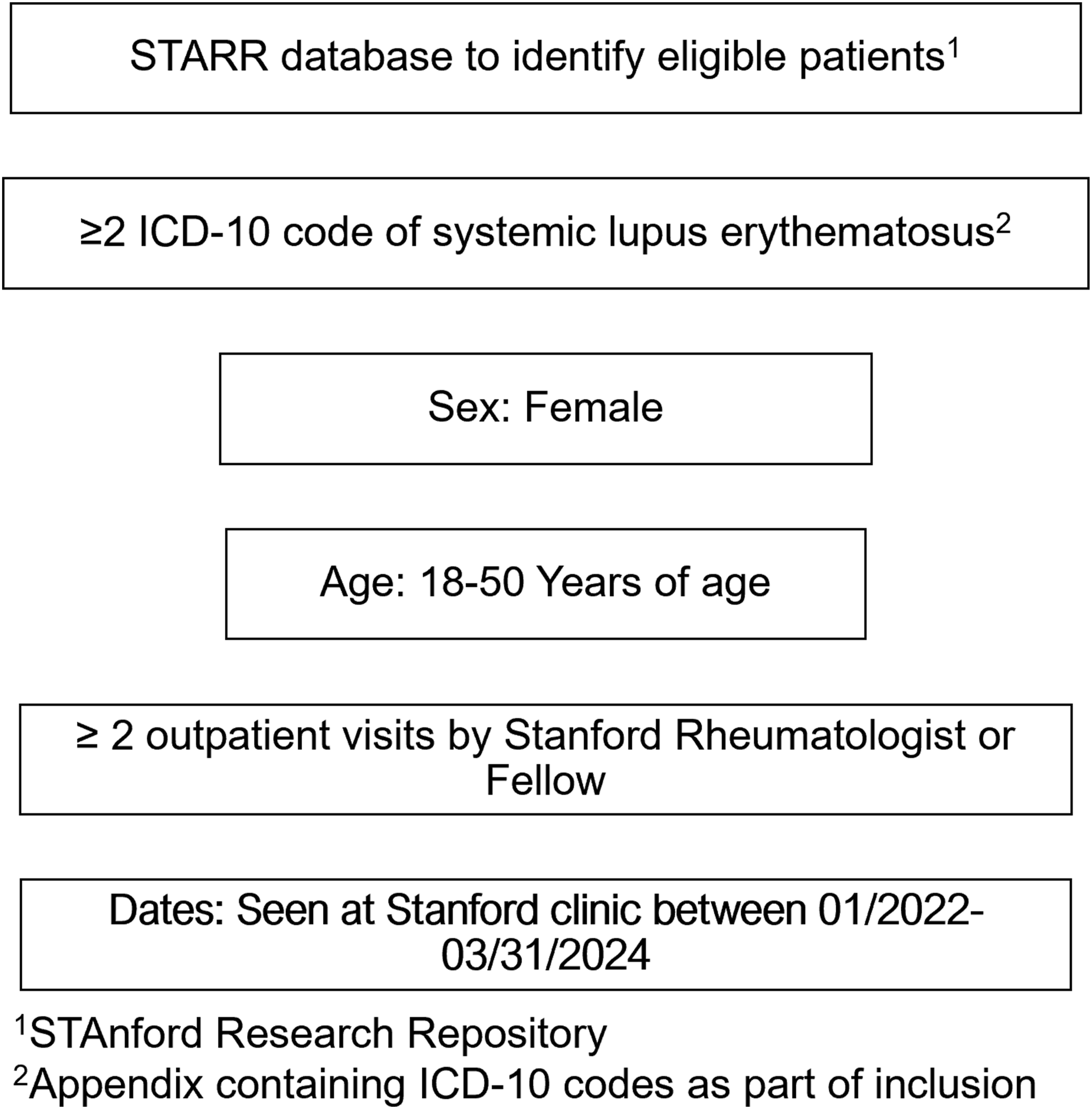
Survey design and content
We used a modified version of a survey previously developed and distributed at the University of Southern California - Los Angeles General Medical Center (USC-LAGMC) to evaluate adherence to reproductive health guidelines. 11 The original survey was designed for and piloted with a predominantly Hispanic SLE patient population, with the goal of understanding patient–provider discussions surrounding reproductive health. It was informed by clinical experience and aligned with ACR Reproductive Health Guidelines. 11 Modifications were made to reflect the clinical context at Stanford Health Care. Respondents self-reported demographics as well as medical and reproductive histories and then answered a series of questions about discussions with their rheumatologist. The survey was developed and administered using REDCap (Appendix) with branching logic to tailor questions to the participant based on self-reported obstetric history. Questions regarding contraceptive use and counseling were administered to all participants; questions pertaining to pregnancy (i.e., counseling on disease remission, medication compatibility) and HCQ use while pregnant were restricted to participants who reported pregnancy following SLE diagnosis. Participants who completed the survey received a $20 gift card as an incentive via email through Tango Rewards.
Survey distribution
An electronic invitation with a link to complete the survey was sent via the patient portal (MyHealth) by the patient care team, which included the primary rheumatologist and patient care coordinator, on July 29, 2024. A reminder to complete the survey was sent 4 weeks later and remained available to complete until September 23, 2024. The first page of the survey explained the research objectives, with participants providing electronic consent before proceeding to the survey questions.
Study variables and data categorization
Data collected included demographics, disease history, reproductive history, and patient-reported discussions on reproductive health with their rheumatologist as recommended by the ACR Reproductive Health guidelines. 12 Demographic data included age (in years) and categorical variables such as race, ethnicity, educational status, employment status, marital status, nativity (U.S. born vs foreign-born), and preferred language for receiving medical care. Race and ethnicity categories were based on predefined survey response options. Due to very small sample size in certain subgroups, participants who selected Native Hawaiian or Other Pacific Islander were combined with participants who reported Asian race and categorized as Asian/Pacific Islander for purpose of analysis. Demographic data was classified based on predefined survey choices and then categorized based on survey responses (Online Appendix).
Disease-related covariates included disease duration (<5 years, 5–10 years, >10 years) as well as history of lupus-related hospitalizations in the past year (yes/no). Participants were also asked whether they were currently taking one or more medications, which were categorized into the following groups: (1) (2) (3) (4)
Of note, voclosporin was neither classified as a teratogenic nor pregnancy-compatible medication given the limited data. Two participants reported taking voclosporin, one of whom was also taking mycophenolate mofetil.
For each participant, we calculated the total number of current medications. We similarly calculated the total number of lupus-related medications, including azathioprine, belimumab, abatacept, tocilizumab, cyclophosphamide (past 3 months), HCQ, leflunomide, methotrexate, mycophenolate mofetil, rituximab (past 6 months), steroids (prednisone, methylprednisolone), tacrolimus, and voclosporin.
Reproductive history included reported sexual activity, contraception use, and pregnancy history. Sexual activity was assessed by asking participants to report prior and current sexual activity with male partners. For those currently sexually active with a male partner, participants were also asked about their current pregnancy intention status, specifically whether they were trying to conceive, trying to avoid pregnancy, or neither.
Participants reported current contraceptive method use, with the option to select multiple methods if applicable. Contraceptive methods were categorized based on efficacy per ACR Reproductive Health guidelines and included: (1) abstinence; (2) less effective methods (i.e., withdrawal, fertility awareness, and barrier or spermicidal methods); (3) effective methods (i.e., short-acting hormonal contraception such as oral contraceptive pills, patch, vaginal ring, or injection); (4) highly effective methods (i.e., LARC including intrauterine devices (IUDs) and hormonal implants); and (5) sterilization methods (i.e., tubal ligation, hysterectomy, or postmenopausal status). 12
Participant reproductive history also included number of pregnancies, miscarriages, and induced (medical or surgical) abortions, which were recorded as continuous variables and further dichotomized as history of at least one abortion or history of at least one miscarriage.
Finally, participants were asked whether they had ever discussed reproductive health topics with their rheumatologist, including contraception, pregnancy planning (i.e., disease remission, medications compatible or incompatible with pregnancy), and management of SLE during pregnancy. Many of these were used to define the outcomes, as described below.
Outcomes of interest
The primary outcomes evaluated patient-reported experiences with reproductive health counseling aligned with ACR guidelines. These outcomes were organized into three domains: 1 contraceptive use and counseling, 2 pregnancy planning, including medication compatibility and disease remission, and 3 HCQ use prior to or during pregnancy.
The first domain, contraceptive use and counseling, assessed the use of EHEC and whether patients received contraceptive counseling by their rheumatologists. Use of EHEC was coded as a binary variable – effective or highly effective methods of contraception per ACR Reproductive Health guidelines. 12 Contraceptive counseling (yes/no) was defined as either (a) discussion of contraception or (b) explanation of contraception in consideration of SLE by the patient’s rheumatologist within the past year.
The second domain, pregnancy planning, which includes medication compatibility and disease remission, evaluated discussions on screening for pregnancy plans, medication safety related to pregnancy, and disease remission prior to pregnancy. Patient-reported variables included whether pregnancy plans were screened (yes/no) using a question that was informed by the One Key Question framework. 13 Additionally, patients reported their primary sources of reproductive health information and any barriers to reproductive health discussions with their rheumatologists.
Participants with a history of pregnancy after their SLE diagnosis were specifically asked about discussions with their rheumatologists on medications compatible or incompatible with pregnancy, the importance of achieving disease remission prior to pregnancy, and the monitoring of lupus disease activity through SLE-related laboratory tests during pregnancy. These were all coded as binary outcomes (yes/no).
The third domain focused on HCQ use and counseling during preconception and pregnancy. Patients reported whether their rheumatologist discussed HCQ use prior to or during pregnancy (yes/no). Additionally, participants indicated whether they took HCQ during these periods (yes/no/unable to recall).
Statistical analysis
Descriptive statistics summarized baseline characteristics of all survey participants. We then summarized survey responses to the three domains of outcome variables to quantify the prevalence of each type of outcome. Categorical variables including missing data were presented as frequencies and percentages; continuous variables were reported as means with standard deviations.
Exploratory bivariate analyses were conducted to identify factors associated with EHEC use, contraception counseling, and screening for pregnancy plans. These analyses were restricted to females of reproductive potential, defined as childbearing age without history of sterilization (n = 91). These secondary analyses were intended to generate hypotheses rather than establish causal relationships. Variables were selected based on clinical relevance, and appropriate statistical tests were applied (Chi-square or Fisher’s exact tests for categorical variables, two-sample t-tests for continuous variables). A sensitivity analysis was subsequently performed among females at risk for pregnancy, defined as the subset of females of reproductive potential and sexually active with a male partner (n = 86). This was intended to account for clinical applicability of contraceptive counseling across subgroups.
Ethical approval and participant consent
The study protocol was approved by the Stanford Institutional Review Board (IRB: 69064).
Results
Patients demographics and characteristics, presented as n (%) unless otherwise specified.
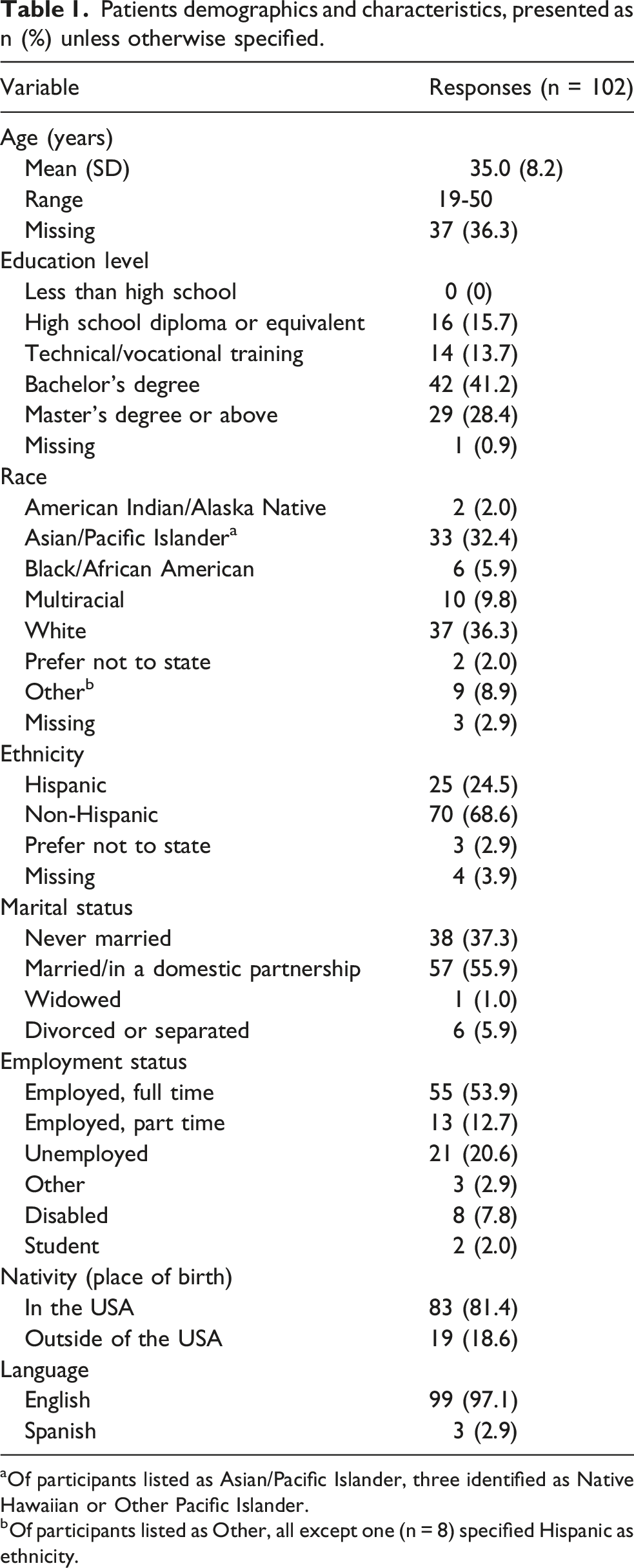
aOf participants listed as Asian/Pacific Islander, three identified as Native Hawaiian or Other Pacific Islander.
bOf participants listed as Other, all except one (n = 8) specified Hispanic as ethnicity.
Contraceptive use and contraceptive counseling
Reproductive and sexual history among females with lupus of childbearing years (n = 102) n, %.
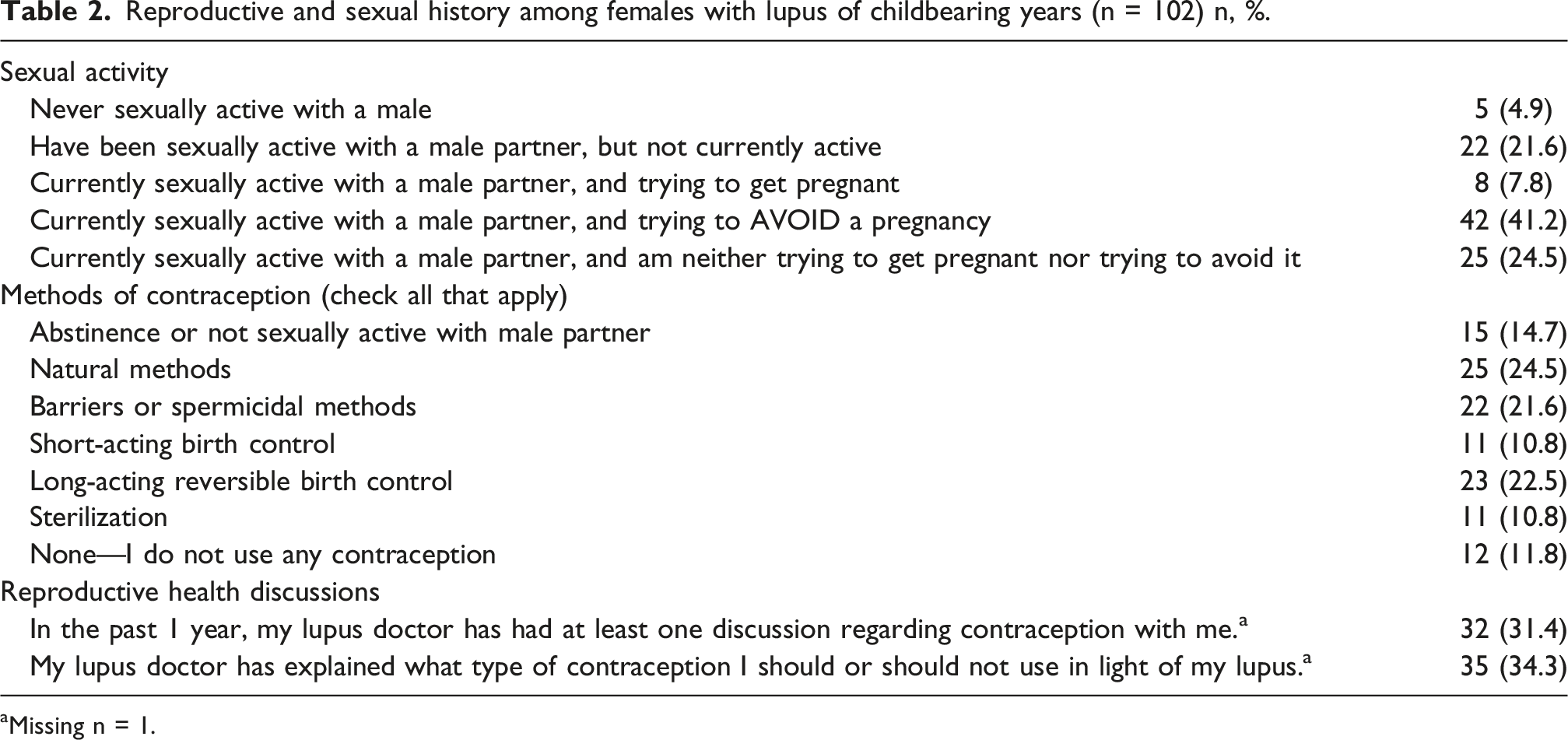
aMissing n = 1.
Exploratory analysis among females with SLE of reproductive potential (n = 91) identified several variables with significant differences in the distribution of contraceptive outcomes (Supplemental Tables 1 – 2). Regarding EHEC use, significant differences were observed across racial groups (p = 0.021), with numerically higher use reported among White (19/33, 59.4%) compared to Asian/Pacific Islander participants (7/31, 22.6%). Regarding contraceptive discussion, significant differences in the distribution were observed across employment status (p = 0.019), teratogenic medication use (p = 0.007), disease duration (p = 0.0075), and who was most likely to initiate reproductive health conversation (p = 0.013) (Supplemental Table 2). Contraceptive discussion was associated with younger mean age (p = 0.03) and higher mean number of medications (p = 0.04) (Supplemental Table 2). Regarding contraceptive explanation, significant differences in the overall distribution were observed across teratogenic medication use (p = 0.016), disease duration (p = 0.01), and who was most likely to initiate reproductive health conversation (p = 0.04) (Supplemental Table 2). Sensitivity analyses among females at risk for pregnancy (n = 86) revealed similar patterns (Supplemental Tables 3 – 4).
Pregnancy planning including medication compatibility and disease remission
Among all participants (n = 102), 51% reported being asked about being screened for pregnancy plans in the past year. Exploratory bivariate analysis among females of reproductive potential (n = 91) revealed screening for pregnancy plans differed in distribution of frequencies by race (p = 0.009), educational status (p = 0.03), nativity (p = 0.05), teratogenic medication use (p = 0.02), and who was most likely to initiate reproductive health conversation (p < 0.001) (Supplemental Table 5). Younger mean age (p < 0.01) and higher mean number of medications (p = 0.04) including lupus-specific medications (p = 0.03) were significantly associated with being asked about pregnancy plans in the past year (Supplemental Table 6). Sensitivity analysis among females at risk for pregnancy (n = 86) revealed similar findings (Supplemental Tables 3 – 4).
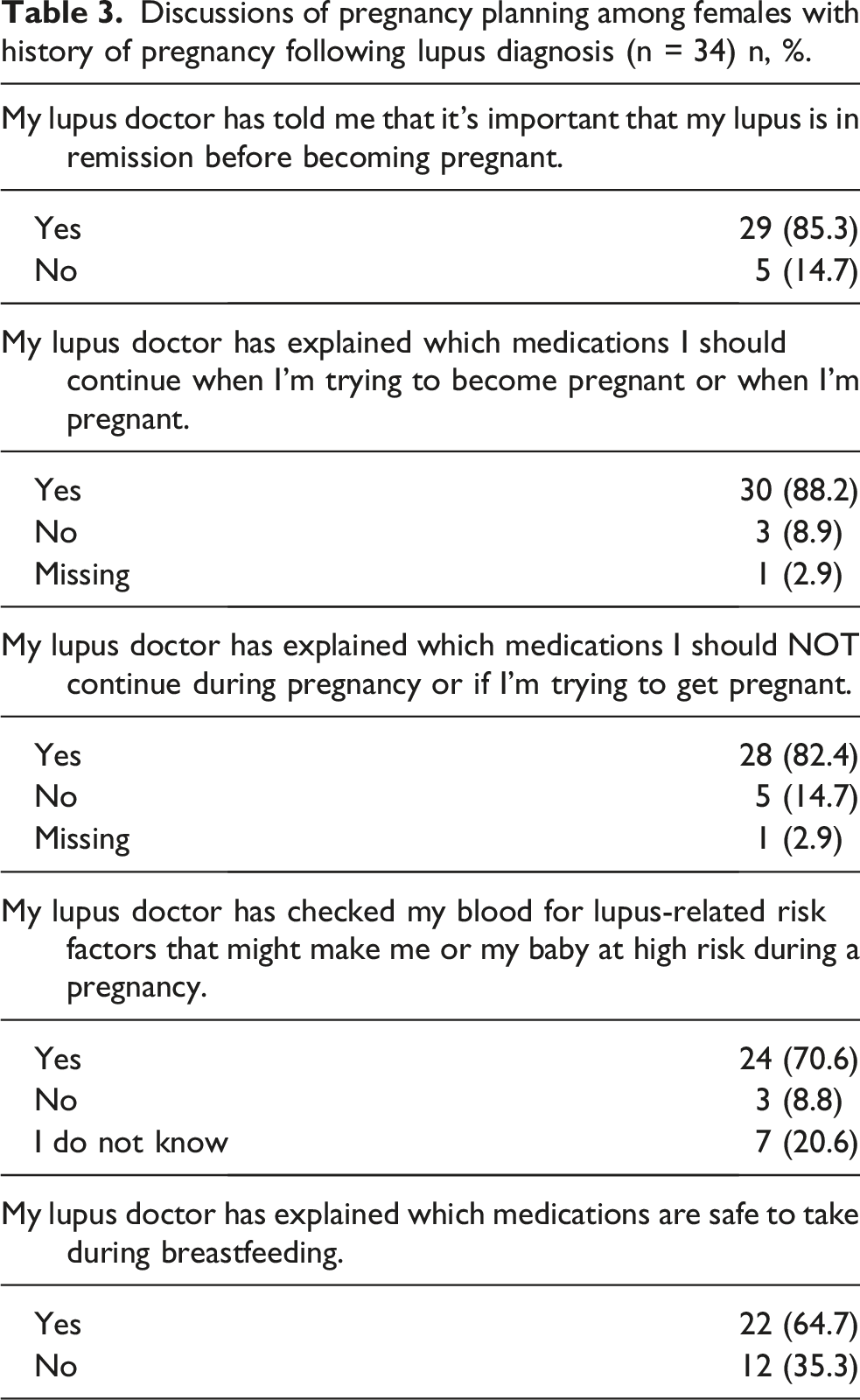
Discussions of pregnancy planning among females with history of pregnancy following lupus diagnosis (n = 34) n, %.
Hydroxychloroquine use and counseling during preconception and pregnancy
Hydroxychloroquine (HCQ) counseling and use during pregnancy (n= 34) n, %.
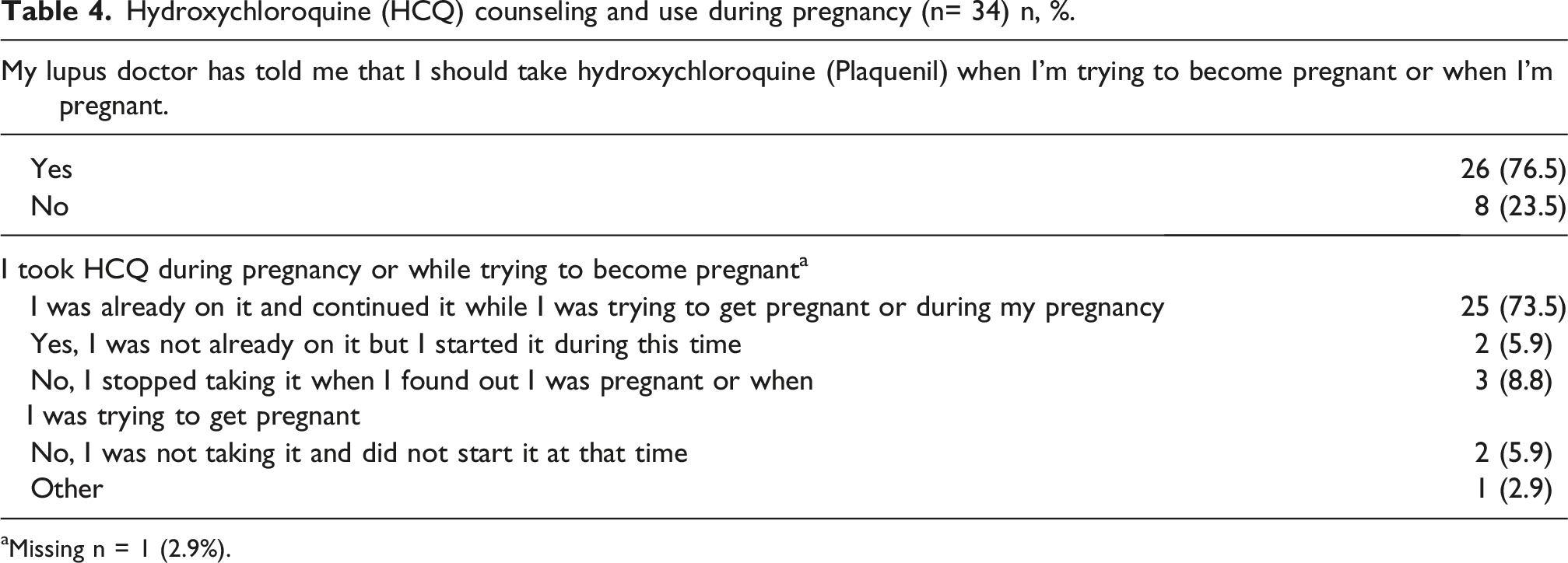
aMissing n = 1 (2.9%).
In the full cohort of female patients with SLE of childbearing age (n = 102), the most frequently reported source of reproductive health information was their rheumatologist (62.7%). Information on the internet (36.3%) and lupus support groups (12.7%) were less commonly reported sources of reproductive health information. Less than one-third of all participants reported having no barriers to discussing reproductive health with their rheumatologists (30.4%). The most reported barrier to having reproductive health discussions with their rheumatologist was being told to discuss with an obstetrician/gynecologist (OB/GYN) instead (30%). This was followed by patient-level factors, including the belief that the topics were not relevant (18.6%) and concerns about the safety of pregnancy in relation to SLE (16.7%).
Discussion
Our cross-sectional survey study of females of childbearing age with SLE at a large academic center highlights gaps in reproductive health counseling and guideline uptake, as well as areas where counseling frequency and uptake were high. Results from our main analyses highlight that less than one-third of participants reported receiving contraceptive counseling by their rheumatologist in the past year. The use of effective or highly effective contraception (EHEC) was similarly low, reported by fewer than one-third of participants in this high-risk group. Among females with a history of pregnancy following diagnosis of SLE, a significant majority reported having discussions about the importance of disease remission, medication compatibility, and disease monitoring during pregnancy. Further, most females in this group reported having discussions about HCQ and an even higher proportion reported taking it when trying to conceive as well as during pregnancy. Reported barriers to reproductive health discussions with a rheumatologist included being advised to defer discussions to OB/GYN and patients’ perception that reproductive health was less important, thereby highlighting opportunities for targeted intervention.
The most clinically notable findings associated with differences in contraceptive use and counseling included differences by race, teratogenic medication use, and perceived initiation of reproductive health discussions. A population-based cohort study among Medicaid beneficiaries found that Black and Asian females with SLE had lower odds of prescription of contraception compared to White females; the use of highly effective forms of contraception was also lower among Black females compared to White females. 14 Differences in contraceptive use including method may be driven by social and cultural factors. A qualitative study found that Black and Hispanic women were likely to choose non-hormonal methods of contraception and report fatalistic beliefs about pregnancy compared to Whites, 15 highlighting discrepancies between evidence-based guidelines and real-world uptake.
Consistent with prior studies, significant differences in the distribution of contraceptive counseling were observed across teratogenic medication use. 16 However, approximately 40% of females of reproductive potential on teratogenic medications reported not receiving contraceptive counseling in the past year, a critical gap warranting further investigation. Furthermore, counseling alone may be insufficient to improve uptake of guideline-concordant methods. In the USC-LAGMC cohort, contraceptive counseling was associated with contraceptive use among those taking teratogenic medications. However, investigators found that counseling was not associated with highly effective methods of contraception in this high-risk subgroup. 17 The findings suggest that factors beyond counseling alone are critical to improve guideline-concordant uptake. It is possible that contraceptive counseling may be influenced by initiation of conversation by patient, rheumatologist, or both. Significant differences in the distribution of contraceptive counseling were observed across the covariate ‘who was most likely to initiate reproductive health conversation’ (i.e., patient, rheumatologist, both, or neither); however, the study was underpowered to draw meaningful conclusions about differences in counseling and initiation of reproductive health conversation. These findings are hypothesis-generating and warrant investigation in larger studies. Future studies should evaluate the role of discussion initiation and other strategies to facilitate reproductive health discussions and improve guideline-concordant contraceptive use in patients with SLE.
Barriers to contraceptive use may extend beyond patient-level factors and involve physician and system-level determinants. A focus group composed of rheumatologists cited various barriers to contraceptive counseling and uptake including limited time during visits, medical complexity, and reliance on obstetrics/gynecology (OB/GYN) and primary care providers for practical considerations (ie. insertion of IUD). 18 Coordination across specialties represents a promising strategy to improve contraceptive counseling and uptake. A single center study found that females with SLE seen by OB/GYN and primary care were more likely to receive prescription for contraceptives. 4 Future studies should investigate different care trajectories among females with SLE as they relate to reproductive health and identify targeted strategies to improve guideline-concordant uptake across health systems and communities.
It is important to note the limitations of this study. As with all survey-based studies, there is a potential for self-selection bias. Individuals with a particular interest or experience related to the topic of reproductive health may have been more likely to respond. Although anonymous, the sensitive nature of the topic of reproductive health may have contributed to the fact that less than 30% of all eligible participants responded to the survey. The cross-sectional design and timing of survey distribution introduce several important limitations that should be considered when interpreting study findings. First, while participants were asked to report experiences with reproductive health counseling in the past year, it is possible that some participants may not have had more recent clinical contact at the time of survey distribution. As noted, “no” responses may reflect either lack of reproductive health counseling during rheumatology visit or lack of follow-up with the rheumatologist in the past year. Regardless, reproductive health counseling is recommended as part of routine care for females with SLE. Gaps in reproductive health counseling within this high-risk population warrant further investigation. For the subset of participants with history of pregnancy following diagnosis of SLE, it is possible that pregnancies may have occurred prior to the release of 2020 ACR Reproductive Health guidelines. Given the eligibility window, period of survey distribution, and asking about pregnancy-related counseling (i.e. HCQ use, disease remission, medication compatibility, and disease monitoring) within the past year, measures were taken to capture patient-reported experiences following the release of the guidelines. Second, the survey captured current contraceptive method use, medication use, and sexual activity at the time of completion, which may not reflect circumstances at the time reproductive health counseling was or was not received. Linking current patient characteristics to care experiences that may have occurred more than 1 year prior limits the ability to draw causal inferences or establish meaningful associations between patient factors and counseling receipt. Third, recall bias is a valid concern. Participants were asked to recall clinical discussions in the past year when completing the survey. The cross-sectional nature and limited sample size preclude multivariable analyses to identify independent predictors of reproductive health counseling and uptake. Findings from exploratory bivariate analyses are therefore intended for hypothesis generation to inform future studies with adequate statistical power. Furthermore, self-reported data may be subject to misclassification, and in some cases potential response bias. The framing of certain survey questions may have also introduced response bias. Specifically, the question ‘What makes it hard to discuss contraception and pregnancy questions with your lupus doctor?’ assumes the existence of barriers, which may have biased respondents toward reporting perceived barriers even when none existed. Furthermore, framing one of the response options as “my lupus doctor has suggested that I talk with an OB/GYN instead” rather than “additionally” may have inadvertently missed capturing relevant discussions that occurred between the rheumatologist and the patient. Because of small sample sizes, the three participants who identified as Native Hawaiian or Other Pacific Islander were combined with those identifying as Asian, limiting our ability to examine these groups separately. Future studies should require more targeted recruitment to adequately assess potential heterogeneity across these populations. Additionally, administering the survey in English limits insights from non-English-speaking individuals. The findings from USC-LAGMC highlight gaps in reproductive counseling among Spanish-speaking individuals compared to English-speakers. 11 Factors related to disease activity and organ damage, including history of lupus nephritis, were not captured in this survey. This limits our ability to contextualize findings in relation to disease severity and clinical risk profile. Lastly, while the low response rate may limit generalizability of the study, this is an underestimate of the true response rate as it is unclear how many patients received the invitation to participate. Of those who did participate, most were English-speaking, college-educated, and identified as White or Asian, which may not reflect the broader SLE population, but does generally represent the patient mix at Stanford University. The electronic delivery of the survey may have limited participation to individuals with reliable internet access and proficiency with digital technology. Notably, our survey was modified from an instrument originally developed at USC-LAGMC, which serves a predominantly Hispanic population at an urban safety-net hospital. The identification of gaps in reproductive health counseling in both settings suggest these deficits may persist in different clinical contexts, underscoring the need for multi-site studies with broader demographic representation.
Our study has several strengths. First, the diagnosis of SLE was confirmed through clinician chart review. All participants were confirmed to receive care at a rheumatology clinic within a tertiary care center. We also used a modified survey developed by colleagues at USC-LAGMC, specifically designed to assess adherence to ACR guidelines. 11 Finally, by offering the survey electronically, we were able to engage participants through a commonly used method of communication; the majority of eligible participants in the study regularly use electronic messaging with their providers.
In conclusion, the study identifies specific gaps in reproductive health counseling among individuals with SLE while also revealing areas of concordance with current guidelines. Differences in counseling by race and medication exposure highlight opportunities for future research and the development of targeted interventions for this high-risk population. In addition, the physician experience of providing reproductive health counseling to patients with SLE warrants further exploration. Insights from both the patient and clinician perspectives will be essential for improving the overall consistency and quality of care.
Supplemental material
Supplemental Material - Diagnosis to dialogue: Reproductive health conversations and guideline adherence in women with lupus
Supplemental Material for Diagnosis to dialogue: Reproductive health conversations and guideline adherence in women with lupus by Akhil Sood, Leanna M. Wise, Sadaf Sediqi, Amanda Moyer, Ellie Diamond, Alyssa Howren, Yashaar Chaichian, Julia F. Simard in Lupus
Supplemental material
Supplemental Material - Diagnosis to dialogue: Reproductive health conversations and guideline adherence in women with lupus
Supplemental Material for Diagnosis to dialogue: Reproductive health conversations and guideline adherence in women with lupus by Akhil Sood, Leanna M. Wise, Sadaf Sediqi, Amanda Moyer, Ellie Diamond, Alyssa Howren, Yashaar Chaichian, Julia F. Simard in Lupus
Footnotes
Ethical considerations
The study protocol was approved by the Stanford Institutional Review Board.
Consent to participate
Participants provided electronic consent before proceeding to complete the survey.
Author contributions
AS was involved in study design, data collection, statistical analysis, and drafting of the manuscript. LW and AM provided clinical guidance and review of the manuscript. SS, ED, AH provided support in study design and data collection. JS and YC contributed to the study design and provided expert guidance and review of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Akhil Sood was a postdoctoral fellow in the Stanford Division of Immunology & Rheumatology, supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) T32 Training Program (5T32AR050942-19). This work was also partly supported by NIAMS R01 AR077103.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AS is a consultant for Third Rock Ventures. LW has received research support from Aurinia Pharmaceuticals (unrelated to this work) and has participated in speakers’ bureaus for AstraZeneca, Aurinia Pharmaceuticals, and GlaxoSmithKline, and served on an advisory board for AstraZeneca. YC receives research support from Lupus Therapeutics and the Lupus Research Alliance and has previously received research support from Eli Lilly and Company and Amgen Inc.; he has also served as a speaker providing non-branded SLE educational content through PeerDirect.
Data Availability Statement
The survey data was collected in REDCap. In accordance with IRB, the data are not publicly available and cannot be shared by request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.