
Abstract
Objective
To develop a standardized nursing protocol for pediatric hypoprothrombinemia-lupus anticoagulant syndrome (HLAS), a rare condition lacking unified clinical nursing guidelines worldwide, aiming to improve nurses’ predictive, precise and whole-course care capabilities and optimize long-term clinical outcomes in affected children.
Methods
Evidence-based nursing principles were integrated with clinical practice. After the admission and standardized management of a typical index case in March 2025, a multidisciplinary team composed of pediatric nephrology, rheumatology, laboratory medicine and nursing specialists conducted retrospective case analysis and collaborative protocol formulation, with its core innovation being the integration of thromboelastography (TEG) parameters to establish a quantitative bleeding risk stratification model. The systematic literature search covered all mainstream Chinese and English databases from database establishment to March 2025, consistent with the timeline of case admission and protocol development.
Results
Application of this protocol in the index case enabled early identification of high bleeding risk, effectively avoiding severe bleeding events and nosocomial infections. The standardized health education and targeted psychological intervention significantly improved the disease cognition and family self-management ability of caregivers. It also transformed nurses from passive caregivers to proactive care managers.
Conclusion
This protocol fills the gap in specialized nursing guidelines for pediatric HLAS, standardizes clinical nursing practices, and provides a replicable methodological reference for the development of standardized nursing protocols for other rare pediatric diseases.
Keywords
Introduction
Childhood-onset systemic lupus erythematosus (cSLE) is a chronic, heterogeneous autoimmune disease involving multiple organ systems, presenting significant clinical challenges in pediatrics. Hematological abnormalities are common manifestations of cSLE, among which hypoprothrombinemia-lupus anticoagulant syndrome (HLAS) is a rare but life-threatening complication that has garnered increasing clinical attention in recent years. The unique pathophysiological mechanism of HLAS involves the coexistence of lupus anticoagulant (LA) (exhibiting in vitro anticoagulant activity) and significantly reduced activity of multiple coagulation factors—most notably prothrombin (FII)—due to antibody-mediated clearance. 1
Laboratory result interpretation in pediatric HLAS is further complicated by developmental hemostasis—the age-dependent maturation of the hemostatic system that results in significantly different normal ranges for coagulation assays in children compared with adults. This age-specific physiological difference is a critical and non-negligible consideration when evaluating pediatric coagulation parameters and designing children-targeted nursing protocols, which has been emphasized in previous studies on childhood antiphospholipid syndrome. 2
Three sets of core conceptual paradoxes clinically specific to pediatric HLAS severely restrict standardized nursing and clinical management, which are systematically sorted out in this study.
First, the classic antiphospholipid syndrome (APS) paradox: APS itself predisposes patients to thrombosis, yet the test for antiphospholipid antibodies (aPL) is named “lupus anticoagulant” because it prolongs clotting times in vitro.
Second, the adult HLAS duality: adult patients with SLE and HLAS carry both aPL antibodies (lupus anticoagulant positivity) and low prothrombin levels secondary to anti-prothrombin antibodies, creating concurrent risks of thrombosis and bleeding.
Third, the unique pediatric HLAS paradox distinguished from adult cases: due to physiological developmental hemostasis, pre-pubertal children have inherently lower baseline concentrations of multiple coagulation cascade factors. This physiological characteristic reduces the thrombotic risk of childhood APS but significantly exacerbates the bleeding tendency of pediatric HLAS, making children more vulnerable to life-threatening hemorrhagic complications than adult patients. Existing studies on pediatric HLAS remain limited to case reports and small-sample reviews, such as the recent single-center retrospective analysis of 70 Chinese children with HLAS by Tian et al., 3 highlighting the urgent need for targeted clinical management and nursing frameworks.
Current clinical nursing for children with HLAS faces a prominent dual dilemma of balancing bleeding and infection risks. Clinically, nurses must take precise and hierarchical interventions to prevent fatal hemorrhage under severe coagulation dysfunction, strictly implement whole-process infection prevention and control during long-term intensive immunosuppressive therapy, and relieve the persistent psychological stress of children and their families caused by chronic disease and acute recurrent complications. Regrettably, no systematic, standardized specialized nursing protocol exists for clinical practice, forcing staff to rely on fragmented experience and reactive strategies, which compromises care consistency and safety.
Based on the March 2025 admission of an index case of cSLE complicated by HLAS, we adopted evidence-based methods, integrated clinical experience from this case, and leveraged MDT collaboration to retrospectively construct a scientific, practical, and generalizable specialized nursing protocol for HLAS. This protocol aims to provide operational guidance for clinical nurses, standardize practices, and improve the prognosis of affected children.
Methods and process for retrospective construction of the specialized nursing practice protocol
Systematic acquisition and rigorous appraisal of evidence
To ensure scientific rigor and timeliness, an evidence-building team was established. The team used the PIPOST model (Population, Intervention, Professional, Outcome, Setting, Time) to formulate research questions and systematically searched Chinese and English databases from inception to March 2025 (corresponding to the time of the index patient’s admission and protocol development initiation). Two trained researchers independently conducted quality assessment and content extraction. Evidence was graded and synthesized to form the protocol basis.
In-depth analysis of clinical practice foundation and case insights
Theoretical evidence was integrated with practical experience. The index case—a 10-years 6-month-old pre-pubertal female (Tanner stage 1) diagnosed with cSLE complicated by HLAS admitted in March 2025—was tracked for full clinical course analysis. On admission, key laboratory findings were: PT >2 × upper normal limit, APTT >2 × upper normal limit, FII activity 17.5 %, lupus anticoagulant positive, WBC 3.2 × 109/L, Neut 1.1 × 109/L, Hb 102 g/L, Plt 215 × 109/L. Real-world clinical data ensured protocol applicability.
Collaborative integration of the multidisciplinary team (MDT) and consensus building
Protocol development was embedded in the MDT care model. Through retrospective analysis of MDT discussions for the enrolled patient, nurses proposed professional nursing diagnoses and draft care plans. The final protocol framework and core content were confirmed via consensus meetings after patient discharge.
Core content and connotation of the HLAS specialized nursing practice protocol
Module 1: Refined bleeding protection system based on dynamic risk assessment
Multi-level, three-dimensional dynamic bleeding risk assessment
HLAS patient bleeding risk dynamic assessment and corresponding nursing measures.
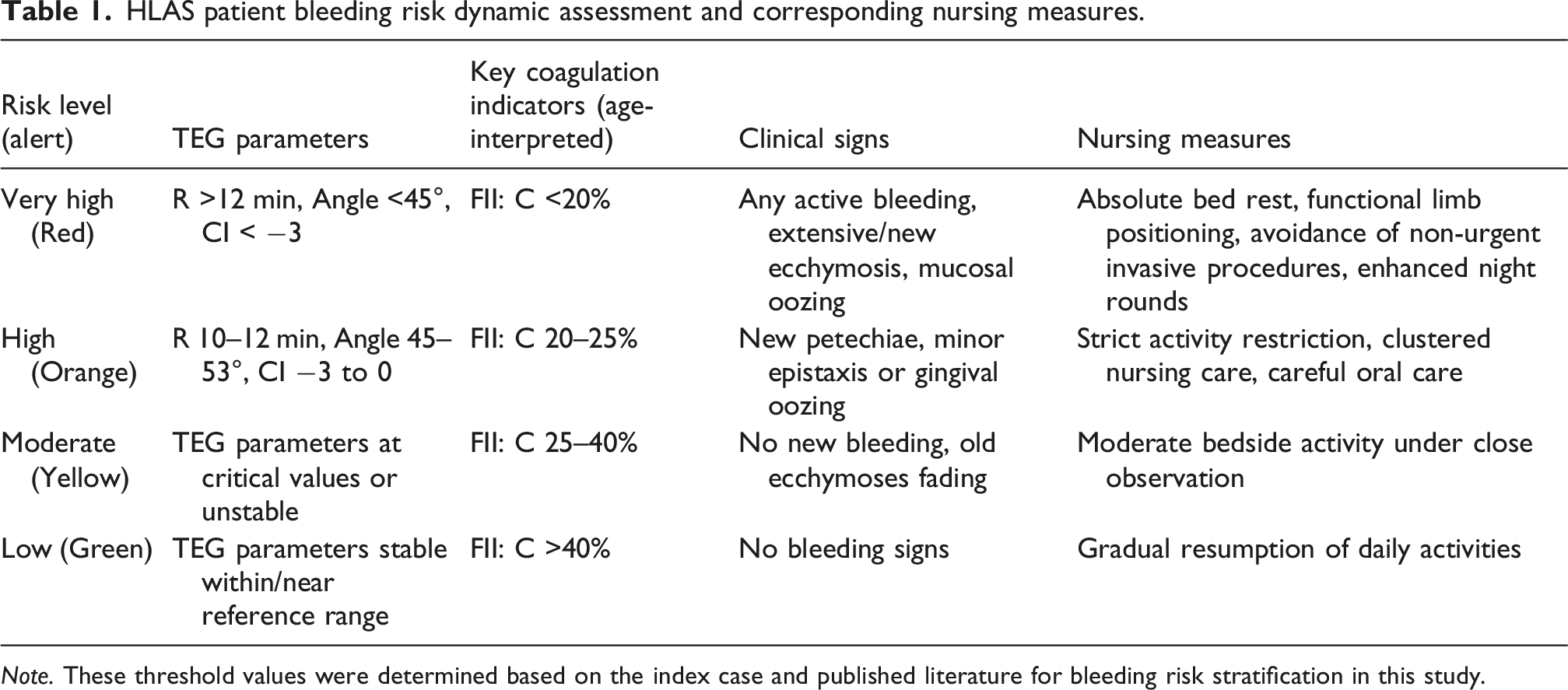
Note. These threshold values were determined based on the index case and published literature for bleeding risk stratification in this study.
Module 2: “Standard precautions plus” layered infection prevention and control system
Infection prevention comprised three integrated layers: • Layer 1 (Basic Protection): Strict hand hygiene, environmental cleaning, appropriate isolation signage, and visitor restrictions when indicated. • Layer 2 (Enhanced Monitoring): Daily assessment for early infection signs, including temperature monitoring, oral mucosa examination (for thrush/herpes), respiratory/gastrointestinal symptom surveillance, and prompt identification of opportunistic infections. • Layer 3 (Immunosuppression Phase Intensified Protection): During high-dose corticosteroid or mycophenolate mofetil (MMF) therapy, additional measures included single-room isolation when feasible, limiting exposure to potentially infected individuals, meticulous oral care protocols, and aseptic technique for all medication administration.
Module 3: Medication and treatment monitoring
Precise and individualized monitoring of immunosuppressants
Index case medication regimens included: methylprednisolone 30 mg/kg/day pulse therapy (max 1 g); oral prednisone 2 mg/kg/day (max 60 mg/day); hydroxychloroquine 5 mg/kg/day once daily; MMF 600 mg/m2/dose twice daily (max 2 g/day).
Coagulation factor replacement monitoring
When coagulation factor replacement was administered, the protocol required: verifying product type and dosage per physician orders; administering via slow infusion following the “start slow, observe closely, adjust speed” principle; assigning dedicated staff to monitor the first 15 min of infusion for transfusion reactions (chills, fever, rash, dyspnea, back pain). Critically, nurses were required to recognize the HLAS paradox: while correcting bleeding with coagulation factors, they must remain vigilant for thrombotic risks (sudden limb swelling/pain, chest pain, dyspnea, altered consciousness) and be prepared for both scenarios.
Module 4: Personalized psychological support and structured health education
Comprehensive, individualized psychosocial assessment and intervention
cSLE combined with HLAS exerted significant psychological impact on children and families. Nurses used validated tools to regularly assess children’s anxiety, depression, and coping styles: non-verbal methods (play therapy, sandplay, drawing) for younger children; respectful, equal communication for school-age/adolescent children to address concerns about body image, education interruption, and social isolation. Family member psychological status was also assessed, with empathetic support provided; severe cases were referred to clinical psychology/psychiatry departments.
Structured, phased, multi-format health education system
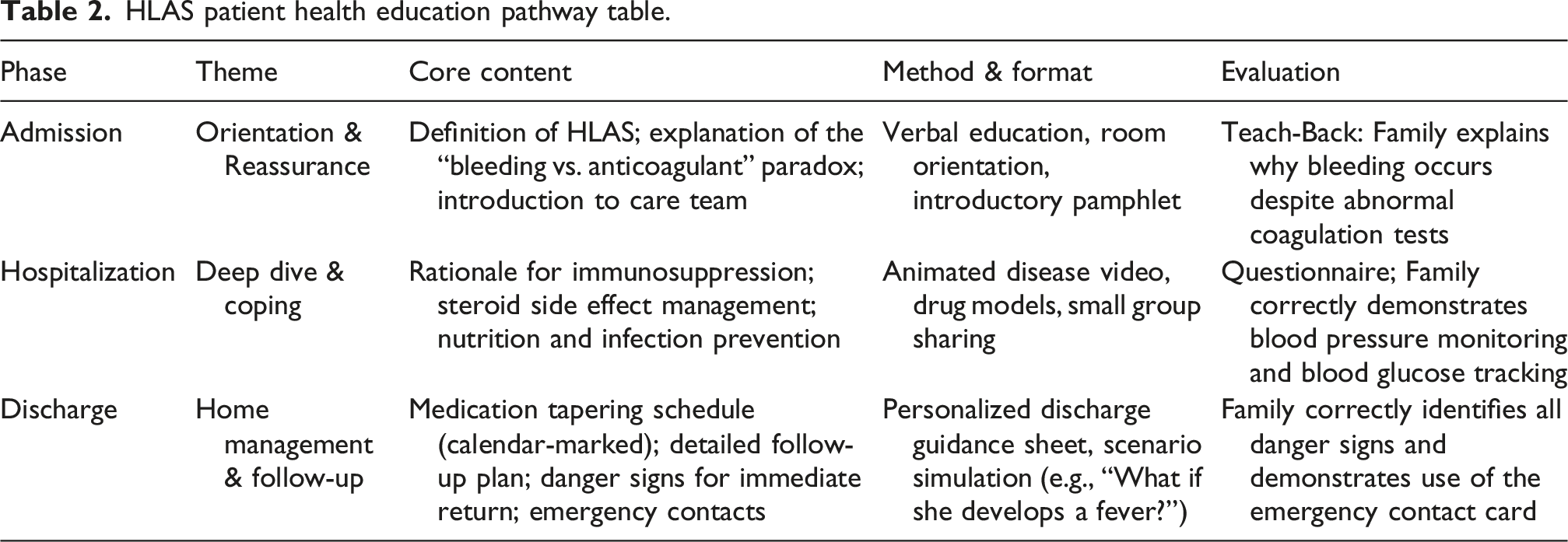
Module 5: Seamless transitional care and discharge guidance
A “Personalized Discharge Nursing Plan” was developed for each HLAS child. 1–3 days before discharge, the primary nurse held a discharge preparation meeting with the family to review the discharge guidance sheet item by item, covering: medication details (name, dosage, administration, duration, precautions); follow-up plan (timing, departments, required tests); home life guidance (activity resumption, diet, hygiene); self-monitoring checklist; emergency contact channels. A post-discharge follow-up system ensured seamless transition to home care.
Protocol application and analysis of practical effects
The protocol was applied to the index case (10-years 6-month-old female, cSLE complicated by HLAS). Admission TEG showed R = 12.8 min, Angle = 43.9°, CI = −8.1; FII:C = 17.5 %; PT/APTT >2 × upper normal limit; WBC = 3.2 × 109/L, Neut = 1.1 × 109/L, Hb = 102 g/L, Plt = 215 × 109/L. Guided by the protocol, the nursing team classified her as Very High Risk (Red Alert) and initiated corresponding protections. Throughout hospitalization, only minor, controllable epistaxis and skin bruising occurred; no severe bleeding or nosocomial infection was observed. Structured health education and psychological support significantly improved the child’s emotional state and family disease management capability.
Discussion
Innovative value of TEG in HLAS nursing risk assessment
Traditional coagulation tests (PT, APTT, INR) provide isolated information, are susceptible to LA interference, and fail to reflect in vivo coagulation balance. 5 TEG dynamically visualizes the full process from fibrin formation to clot lysis. Integrating TEG into nursing risk assessment enables precision care, and partially mitigates developmental hemostasis confounding effects on pediatric traditional coagulation tests. 6
Essence of HLAS nursing: Dynamic balance between bleeding and infection risks
The core HLAS nursing contradiction is the inverse relationship between bleeding and infection risks. In the acute phase (FII:C <20 %, PT/APTT>2× ULN), priorities include absolute bed rest, clustered care, avoidance of invasive procedures, and environmental modification, alongside basic infection control. As immunosuppressive therapy takes effect and coagulation improves, bleeding risk decreases, but infection risk peaks due to immunosuppression. Nursing priorities then shift to refined infection prevention: protective isolation, fever monitoring, strict aseptic technique, and opportunistic infection identification. This dynamic priority adjustment operationalized by integrated risk tools (TEG, FII:C, clinical signs) is the core of HLAS specialized nursing.7,8
Evolution of the specialist nurse role
Nurses evolved from passive order executors to active assessors, planners, coordinators, educators, and researchers. 9 Through MDT participation, nurses translated medical decisions into personalized care plans, coordinated cross-department resources, and played an irreplaceable role in education, psychological support, and transitional care. 10 This role expansion enhances nursing professional value.11,12
Limitations and future perspectives
Limitations include: (1) single-case derivation requiring multi-center validation; (2) lack of robust pediatric age-specific TEG reference ranges, necessitating cautious threshold interpretation; (3) resource intensity potentially challenging implementation in general wards. Future plans include protocol digitalization, nationwide HLAS nursing collaborative research, and extension to other rare pediatric diseases.
Conclusion
Triggered by a March 2025 cSLE-HLAS index case, this study retrospectively constructed a standardized, scientific, and operable pediatric HLAS specialized nursing protocol via evidence-based methods and MDT collaboration. TEG partially overcomes developmental hemostasis interference to improve bleeding risk assessment accuracy. This protocol fills the gap in HLAS nursing guidelines and provides a replicable paradigm for rare pediatric disease nursing.
Footnotes
Acknowledgments
The authors thank all medical and nursing staff of the Department of Pediatric Nephrology, Rheumatology and Immunology for clinical support and data collection; the Medical Ethics Committee of Changzhou Children’s Hospital for ethical approval; the patient’s guardians for informed consent and support; and MDT members for protocol development contributions. No artificial intelligence-assisted technologies were used in manuscript preparation, and no third-party writing/editing assistance was received.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.