
Abstract
Background and Objective
Autonomic dysfunction may arise in chronic systemic diseases, including autoimmune connective tissue disorders. This study aimed to quantify autonomic symptom burden in patients with systemic lupus erythematosus (SLE) and systemic sclerosis (SSc), examine clinical correlates, and compare results with controls without autoimmune disease.
Methods
This cross-sectional study included 50 SLE patients, 50 SSc patients, and 35 controls. Clinical and demographic characteristics were collected during visits. Autonomic symptom burden was assessed using the Composite Autonomic Symptom Score-31 (COMPASS-31). COMPASS-31 total and subdomain scores were examined across groups and within disease groups according to clinical and serological variables. A post-hoc COMPASS-31 score >32.5 was used to define high autonomic symptom burden.
Results
Median total COMPASS-31 scores differed across groups and were higher in both SLE and SSc than in controls (15.43 and 20.53 vs 9.03; p = 0.001). Compared with SLE, SSc had higher orthostatic and vasomotor symptom burden. Using COMPASS-31 > 32.5, high autonomic symptom burden was present in 7/50 (14%) SLE and 13/50 (26%) SSc patients, while none of the controls exceeded the cut-off. In multivariable models, serositis and joint involvement predicted high symptom burden in SLE, whereas clinically significant gastrointestinal involvement and musculoskeletal involvement were independent predictors in SSc. After adjustment for age, sex, and comorbidity, total COMPASS-31 remained higher than in controls in both SLE (β = 7.01; p = 0.013) and SSc (β = 11.24; p < 0.001).
Conclusion
Autonomic symptom burden appears to be higher in patients with SLE and SSc than in controls. The subgroup differences suggest that autonomic symptoms may cluster with specific organ involvement. COMPASS-31 may be a practical screening tool to identify patients who could benefit from further objective autonomic evaluation. Routine, structured assessment may support timely recognition and management of autonomic symptoms in clinical practice.
Introduction
Systemic lupus erythematosus (SLE) and systemic sclerosis (SSc) are chronic autoimmune connective tissue disorders characterized by multisystem involvement. Neurological manifestations associated with these diseases may involve the central nervous system (CNS), peripheral nervous system (PNS), and the autonomic nervous system (ANS).1,2 In the literature, the reported prevalence of neuropsychiatric involvement in SLE ranges from 6% to 91%; in SSc, PNS involvement has also been described, and meta-analytic data suggest that the prevalence of peripheral neuropathy is approximately 27%.3,4
The ANS regulates involuntary bodily functions and consists of sympathetic and parasympathetic branches that act in a complementary manner. 5 Accordingly, autonomic involvement may contribute to non-specific but clinically frequent complaints in these diseases, such as fatigue, orthostatic symptoms, and gastrointestinal manifestations. Existing studies remain limited and heterogeneous, and reported prevalence varies by patient population and assessment method (symptom questionnaires, cardiovascular reflex testing, heart rate variability, tilt testing, or sudomotor testing); across autoimmune rheumatic disorders, parasympathetic and/or sympathetic dysfunction has been reported in 24% to 100% of patients. 6 Autonomic symptoms and abnormalities on objective autonomic testing have been described in both SLE and SSc, and the limited head-to-head data suggest that autonomic involvement may differ in pattern across these diseases.7,8,9,10,11 Autonomic dysfunction has also been reported in other systemic autoimmune disorders, including antiphospholipid syndrome and Sjögren’s syndrome, suggesting that autonomic involvement may represent a broader but under-recognized feature across immune-mediated rheumatic diseases.12,13
Recognizing autonomic symptoms suggestive of dysautonomia in clinical practice is often challenging because symptoms are typically non-specific and may be overlooked by patients or attributed to other disease manifestations. Therefore, practical and validated tools that allow systematic assessment of autonomic symptoms are important. The Composite Autonomic Symptom Score-31 (COMPASS-31) is a validated patient-reported questionnaire used to quantify autonomic symptom burden and has been applied across different conditions, including fibromyalgia and diabetes, to explore clinical correlates of dysautonomia.14,15,16,17 In rheumatology, COMPASS-31 has also been used to characterize autonomic symptom burden in systemic sclerosis cohorts.18,19 The availability of validated language versions, including German and Turkish, supports its use across diverse settings.20,21
In this study, we evaluated autonomic symptom burden in patients with SLE and SSc using COMPASS-31 and compared findings with controls without autoimmune disease. We also investigated associations between autonomic symptom burden and clinical parameters, including disease duration, disease activity, organ involvement, and autoantibody status.
Materials and methods
Study design and participants
This cross-sectional study included patients aged 18–65 years who were followed at the Rheumatology Division, Department of Internal Medicine, Marmara University School of Medicine, and diagnosed with SLE or SSc. SLE patients fulfilled the 2019 EULAR/ACR Classification Criteria for SLE, 22 and SSc patients fulfilled the 2013 ACR/EULAR Classification Criteria for SSc. 23 In total, 50 patients with SLE, 50 patients with SSc, and 35 controls without autoimmune disease were enrolled. Controls were recruited from hospital staff and patients’ relatives, and the same exclusion criteria were applied.
Exclusion criteria included uncontrolled diabetes mellitus or hypertension, congestive heart failure, cardiac arrhythmias, severe neurological or psychiatric disorders, pregnancy, active malignancy, and severe anemia. Ethical approval was obtained from the Ethics Committee of Marmara University School of Medicine (approval no. 09.2021.1376).
Data collection and clinical assessment
Demographic data (age, sex, smoking status, comorbidities) and clinical parameters (age at diagnosis, disease duration, organ/system involvement, and current treatments) were recorded during routine clinical visits using standardized follow-up forms.
In SLE, disease activity was assessed using the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K), 24 and cumulative organ damage was evaluated using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SLICC/ACR DI). 25 In SSc, disease activity was assessed using the revised European Scleroderma Trials and Research (EUSTAR) activity index. 26 Skin involvement was evaluated by a trained researcher using the modified Rodnan Skin Score (mRSS). 27
In SSc, gastrointestinal (GI) involvement was classified according to the Medsger Severity Score criteria. 28 Scores of 0–1 were considered mild/clinically insignificant; higher scores indicate increasing severity. In this study, Medsger GI subscore ≥2 was defined as clinically significant GI involvement and used for subgroup analyses. Musculoskeletal involvement in SSc encompassed physician-documented arthritis/synovitis, tenosynovitis, tendon friction rubs, and/or clinically relevant joint contractures.
Assessment of autonomic symptom burden (COMPASS-31)
Autonomic symptoms were assessed using the COMPASS-31 questionnaire. 14 COMPASS-31 evaluates six domains—orthostatic intolerance, vasomotor, secretomotor, gastrointestinal, urinary, and pupillomotor—and yields a total score ranging from 0 to 100; higher scores indicate greater autonomic symptom burden. Total and domain scores were analyzed in both patient groups. Associations between COMPASS-31 scores and clinical/laboratory parameters (disease duration, disease activity, organ involvement, and autoantibody positivity) were evaluated.
A post-hoc threshold of COMPASS-31 > 32.5 was used to define high autonomic symptom burden, as previously applied in other disease cohorts. 29
Statistical analysis
Statistical analyses were performed using SPSS v28.0 (IBM Corp., Armonk, NY, USA). Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were compared using Student’s t-test/Mann–Whitney U (two groups) and ANOVA/Kruskal–Wallis (three groups), as appropriate; correlations were assessed with Pearson or Spearman tests. When overall three-group comparisons were significant, post-hoc pairwise testing used Bonferroni adjustment (ANOVA) or Dunn–Bonferroni (Kruskal–Wallis). Two-sided p < 0.05 was considered significant.
High autonomic symptom burden was defined post-hoc as COMPASS-31 > 32.5. Independent predictors were evaluated within each disease group using parsimonious multivariable logistic regression (candidate variables prespecified based on clinical relevance and screened in univariable analyses; variables with p < 0.10 entered). Adjusted group differences in total COMPASS-31 were examined using multivariable linear regression with study group as the main predictor, adjusting for age, sex, and comorbidity (DM/HT/CAD/CVD; present/absent).
Results
Participant characteristics
Demographics and disease characteristics of patients with SLE (n = 50).
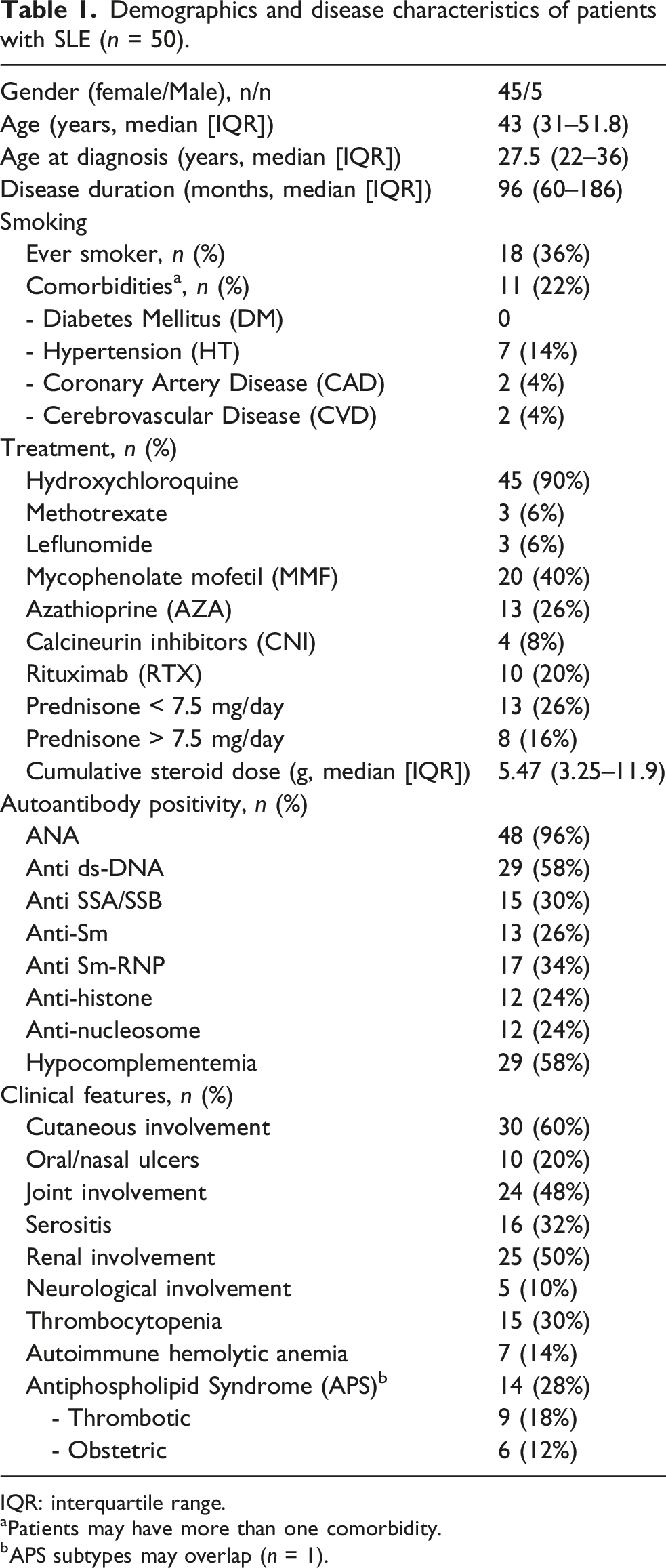
IQR: interquartile range.
aPatients may have more than one comorbidity.
bAPS subtypes may overlap (n = 1).
Demographics and disease characteristics of patients with systemic sclerosis (n = 50).
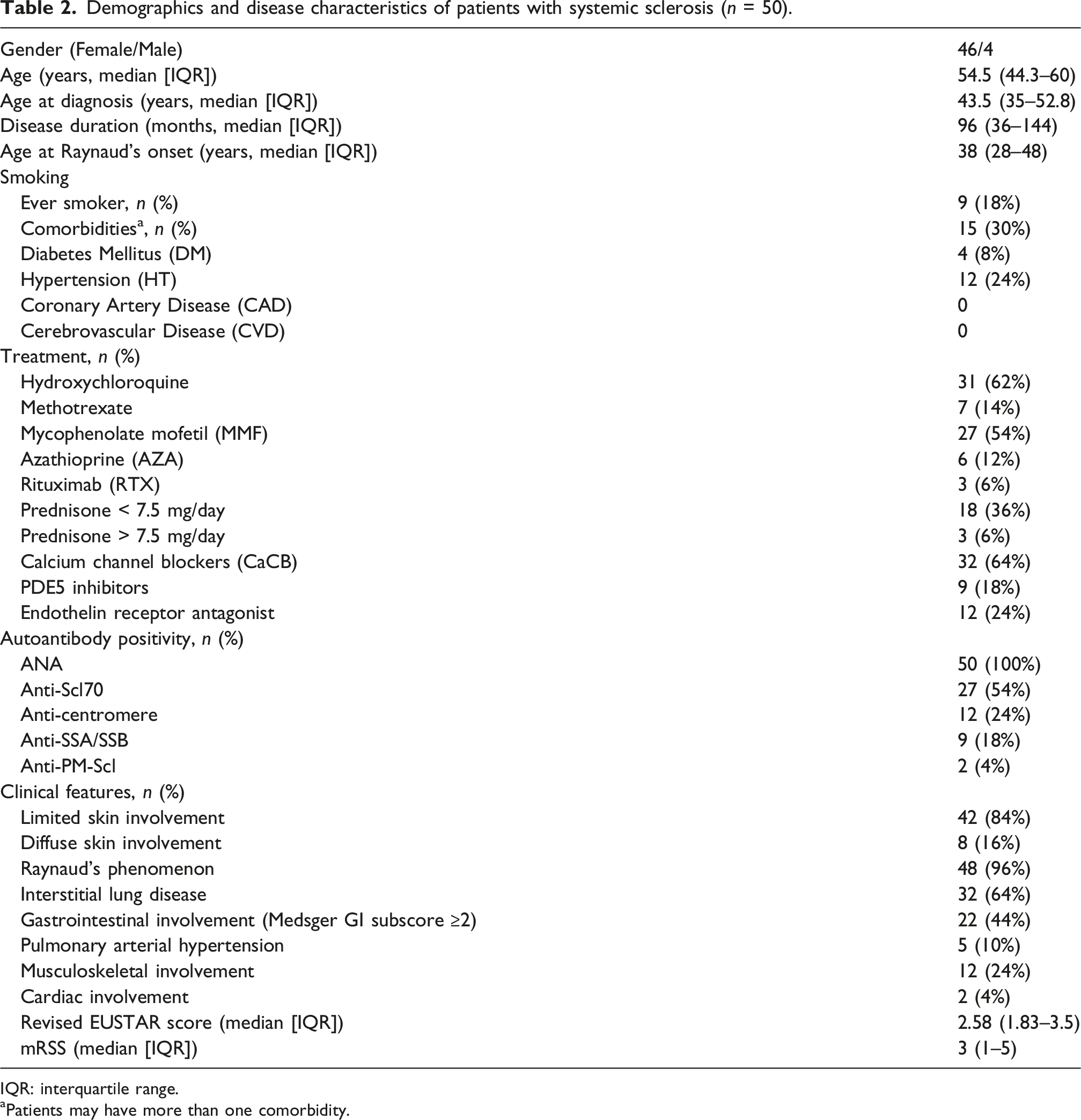
IQR: interquartile range.
aPatients may have more than one comorbidity.
Controls and between-group comparisons
Between-group comparisons of COMPASS-31 domain scores (boxplots) are shown in Figure 1. Median total COMPASS-31 scores differed across groups (SLE: 15.43 [IQR 7.74–25.38], SSc: 20.53 [IQR 10.83–32.67], controls: 9.03 [IQR 3.62–16.83]; overall p = 0.001). Total COMPASS-31 scores were higher in both SLE and SSc compared with controls, while the difference between SSc and SLE was not statistically significant (p = 0.101). Compared with SLE, SSc had higher orthostatic (p = 0.017) and vasomotor scores (p < 0.001). COMPASS-31 domain scores across study groups. Boxplots show COMPASS-31 domain scores (Orthostatic intolerance, Vasomotor, Secretomotor, Gastrointestinal, Urinary, and Pupillomotor) in controls without autoimmune disease, systemic sclerosis (SSc), and systemic lupus erythematosus (SLE). The central line indicates the median; boxes represent the interquartile range (IQR, Q1–Q3). Whiskers extend to 1.5×IQR, and points indicate outliers. Higher scores indicate greater autonomic symptom burden.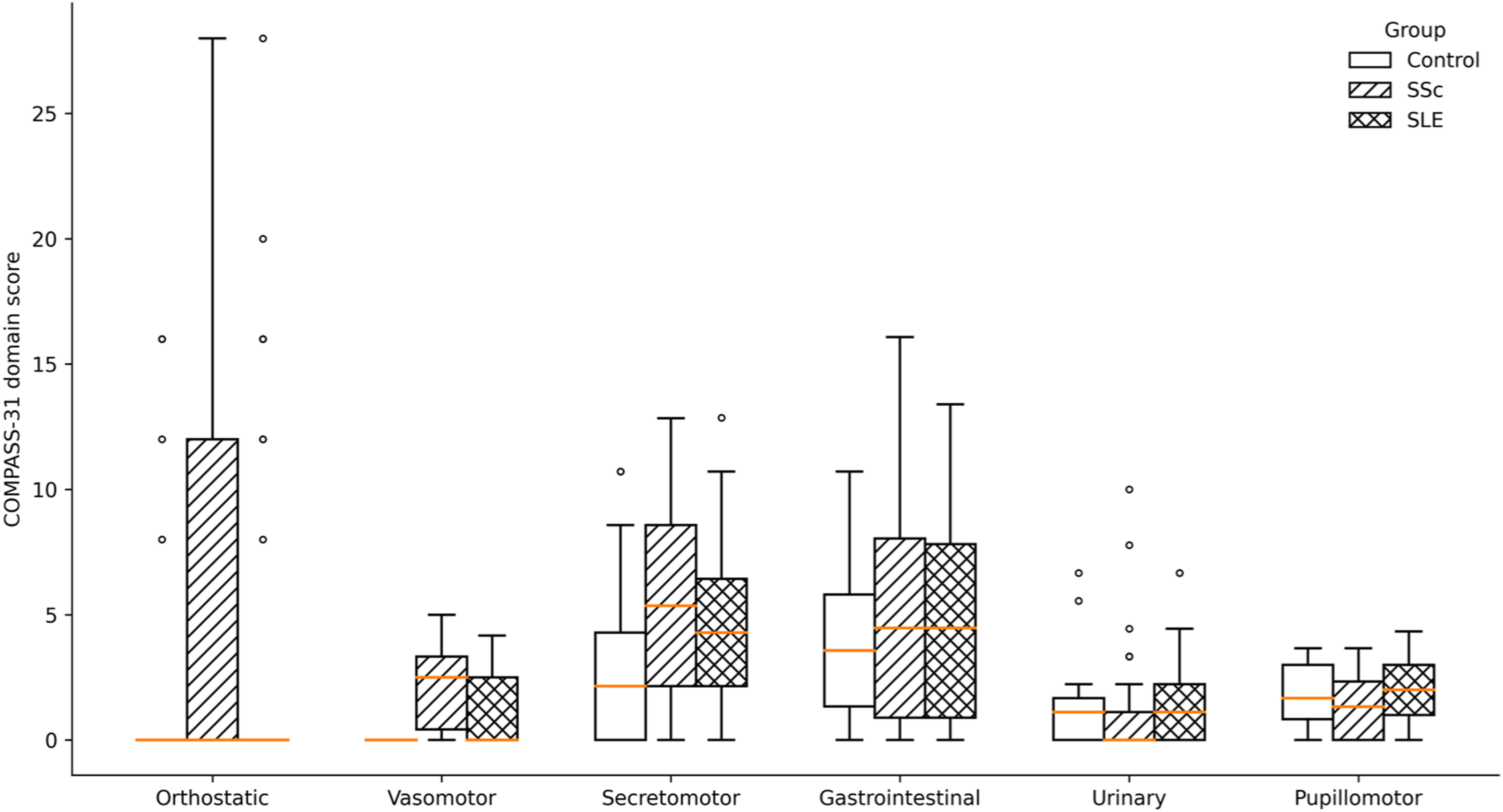
In adjusted analyses (multivariable linear regression controlling for age, sex, and comorbidity), total COMPASS-31 remained higher than in controls in both SLE (β = 7.01; 95% CI 1.53–12.48; p = 0.013) and SSc (β = 11.24; 95% CI 5.89–16.58; p < 0.001). The adjusted difference between SSc and SLE was not statistically significant (β = 4.23; 95% CI −0.81 to 9.27; p = 0.099). None of the controls exceeded the post-hoc threshold for high autonomic symptom burden (COMPASS-31 > 32.5).
Systemic lupus erythematosus (SLE)
In the SLE group, total COMPASS-31 score showed a weak but statistically significant correlation with cumulative damage (SLICC/ACR DI; rho = 0.313, p = 0.034), whereas no association was observed with contemporaneous disease activity (SLEDAI-2K; rho = −0.077, p = 0.612). Total COMPASS-31 was not correlated with disease duration (rho = 0.224, p = 0.130), although longer disease duration was associated with higher secretomotor and urinary subscores (rho = 0.428, p = 0.003 and rho = 0.414, p = 0.004, respectively).
Serositis was associated with higher orthostatic symptom burden (p = 0.004) and higher total COMPASS-31 scores (p = 0.013). Using COMPASS-31 > 32.5, 7/50 (14%) SLE patients met the definition of high autonomic symptom burden. In multivariable logistic regression, joint involvement (OR 13.91, 95% CI 1.26–154.05; p = 0.032) and serositis (OR 11.90, 95% CI 1.61–88.11; p = 0.015) were independently associated with high autonomic symptom burden. Given the limited number of events (n = 7), these estimates should be interpreted cautiously and confidence intervals were wide.
Systemic sclerosis (SSc)
In the SSc group, total COMPASS-31 score was not significantly correlated with global disease activity (revised EUSTAR activity index; rho = −0.262, p = 0.069) or skin thickness (mRSS; rho = −0.157, p = 0.286). Total COMPASS-31 was not correlated with disease duration (rho = −0.042, p = 0.776) and did not differ by cutaneous subset (limited vs diffuse; p = 1.00; diffuse 8/50).
Interstitial lung disease was associated with higher urinary symptom burden (p = 0.029). Clinically significant gastrointestinal involvement (Medsger GI subscore ≥2) was associated with higher orthostatic (p = 0.022), secretomotor (p < 0.001), pupillomotor (p = 0.001), and total COMPASS-31 scores (p = 0.002). Musculoskeletal involvement was associated with higher vasomotor (p = 0.036), orthostatic (p = 0.007), and total scores (p = 0.011). Vasoactive medications (calcium channel blockers, PDE5 inhibitors, endothelin receptor antagonists) were not associated with orthostatic (p = 0.961) or total COMPASS-31 scores (p = 0.467). Using COMPASS-31 > 32.5, 13/50 (26%) SSc patients met the definition of high autonomic symptom burden. In multivariable logistic regression, gastrointestinal involvement (OR 7.79, 95% CI 1.62–37.50; p = 0.011) and musculoskeletal involvement (OR 5.21, 95% CI 1.05–25.76; p = 0.043) were independently associated with high autonomic symptom burden.
Discussion
In the current study, autonomic symptom burden assessed by COMPASS-31 was higher in both SLE and SSc than in controls. While total COMPASS-31 scores were broadly comparable between SLE and SSc, domain-level differences and organ-defined subgroup associations pointed to distinct patterns of symptom distribution within each disease. These findings underscore autonomic symptoms as a patient-reported component of disease burden in systemic autoimmune diseases. 6 Given that COMPASS-31–based symptom data in SLE remain relatively limited, our results extend the symptom-focused literature by providing a direct, questionnaire-based comparison with SSc while also exploring clinically relevant within-disease associations.
Comparative data on autonomic involvement in SLE versus SSc remain limited and are derived mainly from objective assessments. In a comparative study using cardiovascular reflex tests and pupillometry (SLE, n = 31; SSc, n = 19), Straub et al. described broadly similar overall burden but different patterns, with relatively more prominent pupillary involvement in SLE and more marked cardiovascular autonomic involvement in SSc. 7 A larger Holter/heart rate variability–based comparison (SSc, n = 76; SLE, n = 70; controls, n = 45) also indicated disease-specific differences in cardiac autonomic tone and arrhythmia/conduction profiles. 30 Together, these studies support increased autonomic involvement in both diseases, with disease-related differences in pattern, which is broadly in keeping with the domain-level symptom distribution observed in our COMPASS-31 data.
In SSc, our findings can be interpreted in the context of the disease’s prominent vasculopathic phenotype. 31 In the vasculopathic spectrum in which Raynaud’s phenomenon is a hallmark, altered neural control of vascular tone and adrenergic signaling have been implicated, 32 and increased α2-adrenergic vasoconstrictor responses have been reported in isolated dermal arterioles from patients with diffuse SSc. 33 In line with this framework, we observed higher orthostatic intolerance and vasomotor symptom burden in SSc compared with SLE, suggesting that vascular dysregulation may contribute to the symptom profile captured by COMPASS-31 in SSc.
Among the clinical manifestations of SSc, gastrointestinal (GI) involvement has been repeatedly associated with greater autonomic symptom burden. This pattern has also been observed in prior symptom-based COMPASS-31 studies. Adler et al. evaluated COMPASS-31 in SSc (n = 104) and found higher dysautonomia symptom scores in patients with more severe GI disease, including elevations in orthostatic intolerance and secretomotor domains. 18 Hughes et al. studied autonomic and GI symptoms in SSc (SSc n = 17; controls n = 32) and likewise reported higher autonomic symptom burden in SSc than in controls. 19 In our cohort, clinically significant GI involvement was associated with higher COMPASS-31 burden across multiple domains and remained an independent predictor of high symptom burden. Musculoskeletal involvement was also linked to high symptom burden, further supporting substantial within-disease heterogeneity in autonomic symptom expression.
Beyond organ-specific associations, whether autonomic involvement in SSc tracks with disease duration or cutaneous phenotype remains uncertain. A report of two cases raised the possibility that cardiac autonomic dysfunction may occur early, even before overt fibrotic organ disease becomes clinically apparent. 34 Objective studies have produced mixed signals regarding duration: one cohort assessed with 24-h electrocardiography and heart rate variability (HRV) measures (n = 27) reported a relationship with disease duration, 35 whereas a Holter-based study using electrocardiography-derived autonomic metrics (n = 32) did not demonstrate a clear duration relationship. 36 Evidence regarding cutaneous phenotype is also inconsistent: a heart rate variability study (n = 17; 9 diffuse disease, 8 CREST) suggested differences in cardiac autonomic modulation between diffuse disease and CREST, with reduced parasympathetic control reported in the CREST subset. 37 In contrast, symptom-based COMPASS-31 cohorts have not reliably shown limited–diffuse differences. 18 In line with symptom-based data, total COMPASS-31 in our SSc cohort did not show a clear relationship with disease duration and did not differ between limited and diffuse subsets. Overall, dysautonomia may be present across the SSc spectrum and may not be confined to advanced disease; in established SSc, symptom burden may be influenced more by organ involvement than by duration or skin subset.
In our SLE cohort, autonomic symptom burden assessed by COMPASS-31 appeared to relate more closely to cumulative damage than to contemporaneous disease activity, indicating a more persistent, longer-term disease impact rather than short-term activity fluctuations. Higher COMPASS-31 scores in patients with serositis and joint involvement may reflect more prominent autonomic symptoms in specific inflammatory clinical phenotypes, which is biologically plausible given bidirectional links between immune activation and autonomic regulation.6,38 We also observed domain-specific signals indicating that longer disease duration may be accompanied by greater secretomotor and urinary symptom burden.
Objective autonomic testing studies in SLE provide complementary but heterogeneous context. In a prospective cohort using a standard cardiovascular reflex battery (SLE n = 51; controls n = 30), autonomic dysfunction did not correlate clearly with activity, damage, or duration, 8 whereas a comparative study combining cardiovascular reflex testing with pupillometry reported associations between disease activity and autonomic neuropathy measures in SLE. 7 This variability may reflect heterogeneity in patient populations, test batteries, and definitions of autonomic dysfunction. It may also reflect partial dissociation between patient-reported autonomic symptom burden and abnormalities detected by objective autonomic testing.
Clinically, the consistently higher COMPASS-31 scores in SLE and SSc compared with controls and the ease of administration support the potential use of COMPASS-31 as a structured symptom assessment tool
In conclusion, autonomic symptom burden was increased in both SLE and SSc compared with controls. Although total symptom burden was broadly similar between diseases, the distribution of symptoms across COMPASS-31 domains differed, with more prominent orthostatic and vasomotor symptoms in SSc and clinically meaningful within-disease variability in both disease groups. Together with previous reports in other systemic autoimmune disorders such as antiphospholipid syndrome and Sjögren’s syndrome, our findings support the need for greater awareness of autonomic dysfunction in autoimmune rheumatic diseases. Routine, structured assessment of autonomic symptoms may facilitate earlier recognition and more comprehensive management, while longitudinal studies incorporating objective autonomic testing are needed.
Footnotes
Acknowledgements
The authors thank all participants who were included in this study. AI-assisted language editing support (ChatGPT) was used solely to improve language, grammar, and readability during manuscript preparation. All AI-assisted edits were critically reviewed, revised, and verified by the authors, who take full responsibility for the accuracy, originality, and integrity of the manuscript.
Ethical considerations
This study was approved by the Ethics Committee of Marmara University School of Medicine (approval no. 09.2021.1376) and was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants prior to inclusion in the study.
Author contributions
Aysegul Avcu: Conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, writing—review and editing. Zeynep Hazal Baltaci: Investigation, data curation, formal analysis, writing—review and editing. Dilara Deniz Ergin: Investigation, data curation, writing—review and editing. Ebru Asicioglu: Methodology, supervision, writing—review and editing. Haner Direskeneli: Conceptualization, supervision, writing—review and editing. Fatma Alibaz-Oner: Conceptualization, methodology, supervision, formal analysis, writing—review and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available because they contain potentially identifiable clinical data but are available from the corresponding author on reasonable request.