
Abstract
Background
Systemic lupus erythematosus (SLE) is an autoimmune condition showing persistent profiling of inflammation and damage of organs and immune system. Amongst many biomarkers for such autoimmune diseases, Galectin-3 (Gal-3) a β-galactoside-binding lectin responsible for regulation, inflammation, and fibrosis of immune repsonses, has engrossed researchers for further investigations as a potential biomarker. However, correlation has been studied between circulating Galectin-3 levels and SLE but outcomes still remain inconsistent. Therefore, this systematic review and meta-analysis evaluated the association between circulating galectin-3 levels and SLE.
Materials and Methods
PubMed, Scopus, ScienceDirect, Web of Science, and Embase databases are extensively used for literature search. The last database search was conducted on September 6, 2025. Eligible studies included case control studies reporting circulating galectin-3 levels in individuals with SLE and healthy controls. Two independent reviewers performed study selection and data extraction. Study quality was evaluated using the Newcastle-Ottawa Scale. Comprehensive Meta-Analysis software was used for statistical analysis. Pooled effect sizes were calculated as mean differences with 95% confidence intervals. Heterogeneity was assessed using the Cochrane Q test and I2 statistics, and publication bias was evaluated using Begg’s funnel plot and Egger’s regression analysis.
Results
Seven eligible studies were included in the meta-analysis. The pooled results showed that patients with SLE had significantly higher circulating Galectin-3 levels than healthy controls (mean difference = 8.48; 95% CI: 3.84–13.12; p < 0.0001). Substantial heterogeneity was observed across studies (Tau square: 32.57, Q = 196.03; p < 0.0001, I2 = 96.93%). Sensitivity analysis confirmed the stability of the overall findings. Begg’s funnel plot and Egger’s regression analysis indicated no publication bias among studies. Subgroup analysis supports the results of the overall analysis.
Conclusion
This meta-analysis depicts that galectin-3 may serve as a biomarker associated with SLE pathogenesis and inflammatory activity due to significantly elevated levels of circulating galectin-3 levels in patients with systemic lupus erythematosus.
Keywords
Introduction
Characterization of Systemic lupus erythematosus (SLE) as a chronic autoimmune disorder is due to the targeted damage of multiple organ systems by numerous autoantibodies production in renal, dermatological, neuropsychiatric, and cardiovascular organ systems. Even advancements in therapeutic strategies are not ameliorative as SLE remains associated with substantial morbidity and mortality worldwide. 1 Factors like genetic, environmental, and immune dysregulation are majorly responsible for multifactorial and complex pathogenesis of SLE. Lupus nephritis and cardiovascular disease are amongst the most severe complications which significantly impact prolonged organ damage and mortality.2,3 Therefore, identifying reliable biomarkers linked to the pathogenesis of SLE can be a breakthrough for improving disease monitoring and therapeutic interventions.
Key role of Galectin-3, a β-galactoside–binding lectin, in regulating immune responses, inflammation, and cell apoptosis has been reported.4,5 In the context of autoimmune disorders, galectin-3 also accelerates inflammatory signaling and autoantibody production by facilitating the activation and survival of immune cells, including macrophages, dendritic cells, and T lymphocytes.6,7 Additionally, galectin-3 can influence B-cell activation and antibody secretion, further contributing to the development of autoimmunity. 8 In SLE, elevated levels of galectin-3 have been linked to increased immune complex formation, heightened cytokine production, and impaired clearance of apoptotic cells, which are key mechanisms in lupus pathogenesis.9–11
Recent investigations suggested that galectin-3 and its binding protein contribute to the immunopathogenesis of SLE.9,10,12 Lupus nephritis and higher disease activity scores have been found associated with elevated levels of galectin-3. 9 Additionally, proliferated levels of circulating galectin-3 levels in patients with SLE compared with healthy controls were reported in several studies.10,13 However, contradictory observation has also been mentioned in a Chinese cohort, recording no significant change in Gal-3 levels between SLE patients and controls. 14 Given these inconsistencies and inquisitiveness for galectin-3 as a potential biomarker, a comprehensive systematic review and meta-analysis are warranted to quantitatively generate the available evidence and clarify the association between circulating galectin-3 levels and SLE.
Materials and methods
Literature search for meta-analysis
The recent guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020, were followed to conduct the present systematic review and meta-analysis.15,16 An inclusive literature search was conducted using PubMed, Scopus, ScienceDirect, Web of Science, and Embase to identify relevant reports for inclusion in the current investigation. The subsequent keywords and Medical Subject Headings (MeSH) terms were used to ascertain appropriate publications in different databases, such as “galectin-3,” “galectin 3,” “LGALS3,” “Mac-2 antigen,” “systemic lupus erythematosus,” and “SLE,” combined using Boolean operators (AND/OR). Manual screening of the reference lists from relevant articles and meta-analyses were also executed to decipher more eligible studies. The detailed search strategy is provided in Supplemental Table 1. The last database search was conducted on September 6, 2025.
Inclusion and exclusion criteria
Subsequent criteria were considered for the eligibility of studies: (1) study design: only case-control studies; (2) participants: patients diagnosed with SLE according to established classification criteria, including those of the American College of Rheumatology (ACR) or the European League Against Rheumatism (EULAR); (3) outcome measures: studies reporting circulating Galectin-3 levels in both SLE patients and healthy controls, expressed as mean ± standard deviation (SD) or as median with interquartile range (IQR); and (4) publication characteristics: full-length articles published in English in peer-reviewed journals.
The exclusion criteria were as follows: (1) review articles, case reports, editorials, or conference abstracts. (2) Studies lacking sufficient data for extraction on either SLE patients or healthy controls; (3) reports with incomplete information or not including an appropriate healthy control group; and (4) animal studies or investigations involving SLE patients who were pregnant, had infections, had juvenile SLE, or had overlap syndromes.
Study screening
Two independent authors screened the retrieved records. Preliminarily, titles and abstracts were evaluated to eliminate irrelevant articles. The full-text versions of potentially appropriate studies were then assessed for inclusion. Discussion and necessary consultation between the authors and with a third author, whenever required was carried out to resolve any disagreements regarding the screening of articles were resolved to achieve consensus.
Data extraction
Independent data extraction was done by two investigators. The following information was collected: (1) first author and year of publication; (2) country or region of the study; (3) sample size and mean age ± standard deviation of both SLE patients and healthy controls; (4) circulating galectin-3 levels (mean ± SD or median and interquartile range); (5) assay methods used for galectin-3 measurement; and (6) SLE classification criteria applied. Galectin-3 levels were reported as medians with IQRs and were further converted into means and standard deviations using established statistical methods 17 for uniform quantitative synthesis.
Quality assessment
Newcastle–Ottawa Scale (NOS) was used for assessment of the methodological quality of the included case-control studies independently by two investigators. 18 The Three domains evaluated by NOS are Selection (0–4 stars), Comparability (0–2 stars), and Exposure (0–3 stars). Methodological quality of studies can be estimated as moderate to high when scored five or more stars. Disparities were validated through discussion and risk-of-bias visualisation was performed using the robvis tool. 19
Statistical analysis
Statistical analyses were pereformed using Comprehensive Meta-Analysis (CMA) version 4 software. Effect sizes were calculated as mean differences with corresponding 95% confidence intervals (CIs). For statistical significance, a two-tailed p-value < 0.05 was considered. Assessment of between-study heterogeneity was done by using the Cochrane Q test, Tau, 2 and I2 statistics. Significant heterogeneity was defined as p < 0.05 and I2 > 50%. 20 As the data for the meta-analysis were obtained from different populations, the meta-analysis was completed using a random-effects model. Begg’s funnel plot and Egger’s regression was performed to evaluate publication bias. 21 Sensitivity analyses for assessing the robustness of the pooled estimates were performed by sequentially excluding each study. 22 Additionally, determination of whether sufficient studies had been conducted to reach a definitive conclusion regarding the association between galectin-3 levels and SLE, or further research was warranted was done by trial sequential analysis (TSA). 23
Results
Literature findings and suitable studies for meta-analysis
Collectively, 1,047 publications were initially identified through systematic searches of PubMed (n = 44), Scopus (n = 771), ScienceDirect (n = 159), Web of Science (n = 48), and Embase (n = 25). Exclusion of duplicate records (n = 276) was followed by screening titles and abstracts, and then evaluating potentially relevant articles through full-text assessment. This resulted in inclusion of seven studies that met the eligibility criteria for meta-analysis.
The study identification process followed the PRISMA 2020 guidelines, and a detailed description of the screening procedure is presented in Figure 1 as a PRISMA flow diagram. Newcastle-Ottawa Scale for case-control studies
18
was used to evaluate the methodological quality of the included studies, and both study-level and item-level results of the quality assessment are illustrated in Supplemental Figure 1. The NOS exploration indicated that all included eligible studies had more than five stars. PRISMA 2020 study flow chart showing the number of included and excluded articles for the present meta-analysis.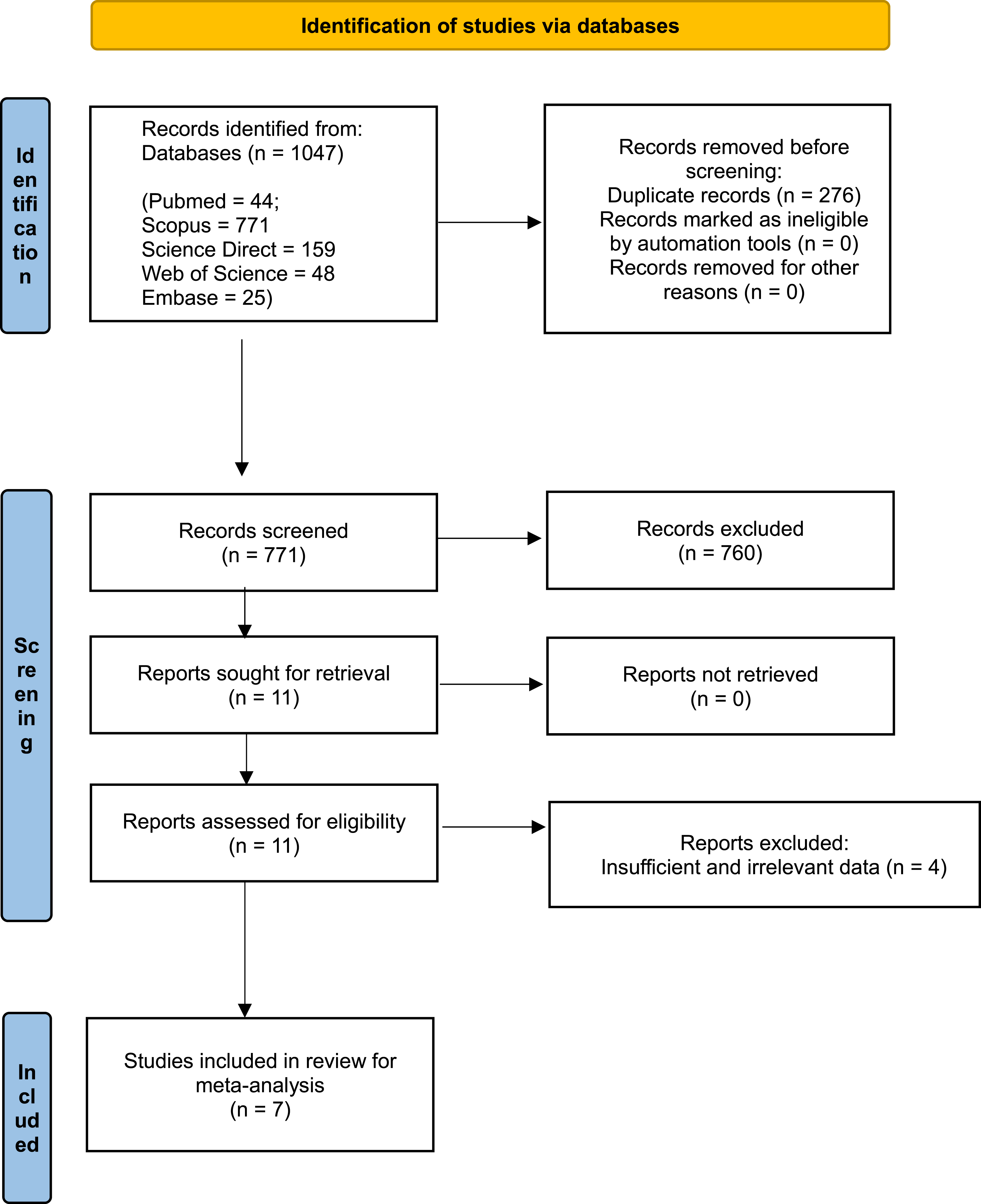
Baseline data of all studies included in the present meta-analysis.
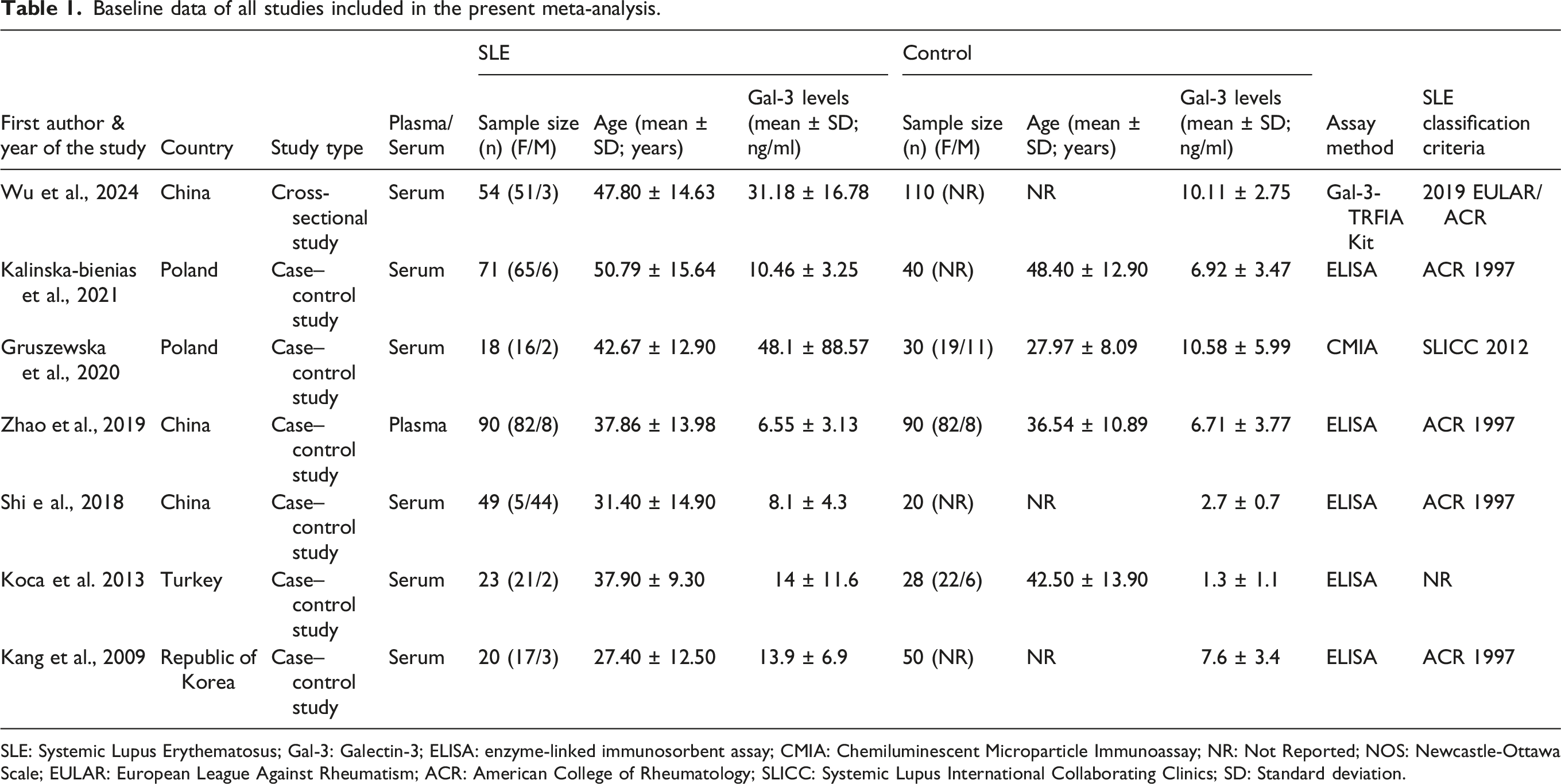
SLE: Systemic Lupus Erythematosus; Gal-3: Galectin-3; ELISA: enzyme-linked immunosorbent assay; CMIA: Chemiluminescent Microparticle Immunoassay; NR: Not Reported; NOS: Newcastle-Ottawa Scale; EULAR: European League Against Rheumatism; ACR: American College of Rheumatology; SLICC: Systemic Lupus International Collaborating Clinics; SD: Standard deviation.
Publication bias
Key challenge in meta-analyses is publication bias, as it can distort the pooled effect estimate by excluding unpublished or missing studies, thereby influencing the reliability and validity of the pooled estimates. To evaluate potential publication bias among the included studies, Begg’s funnel plot and Egger’s regression test were applied. 21 Visual inspection of Begg’s funnel plots did not reveal significant asymmetry in the overall comparison of serum galectin-3 levels between SLE patients and healthy controls. Similarly, no substantial publication bias was observed in subgroup analyses stratified by ethnicity, patient sample size, and study quality (NOS score) (Supplemental Figures 2–6).
Egger’s regression (publication bias) and heterogeneity test analysis for the association between galectin-3 and SLE.
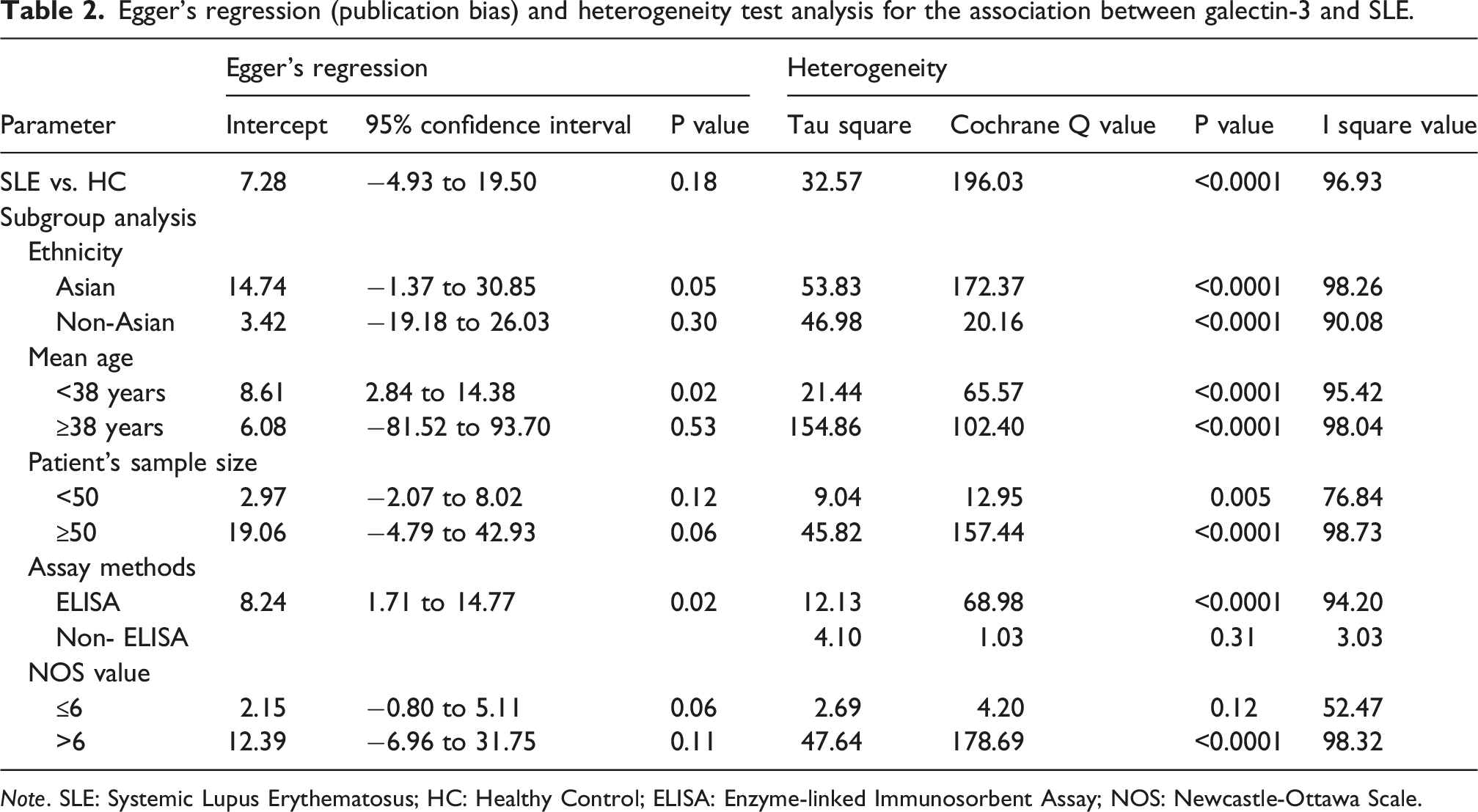
Note. SLE: Systemic Lupus Erythematosus; HC: Healthy Control; ELISA: Enzyme-linked Immunosorbent Assay; NOS: Newcastle-Ottawa Scale.
Heterogeneity investigation
The assessment of Between-study heterogeneity was performed using the Cochrane Q test, Tau square and the I2 statistic, which are commonly used measures in meta-analytical studies.20,22 The analysis revealed considerable heterogeneity among the included studies. For the primary comparison between SLE patients and healthy controls, the heterogeneity statistics were as follows: Q = 196.03, Tau square = 32.57, Pheterogeneity < 0.0001, and I2 = 96.93%, indicating a high level of variability across studies (Table 2).
Additionally, substantial heterogeneity was recorded in subgroup analyses evaluating the association between Galectin-3 levels and SLE, stratified by ethnicity, mean age of participants, and sample size (Table 2). Given the considerable heterogeneity, a random-effects model was employed to calculate the pooled estimates in this meta-analysis, as recommended in methodological guidelines for meta-analyses with heterogeneous data. 22
Elevated galectin-3 levels observed in SLE patients than healthy controls
A pooled analysis verified that individuals with SLE had extensively elevated serum Galectin-3 levels than healthy controls. The overall pooled mean difference (MD) in Galectin-3 levels between the two groups was 8.484, with a standard error of 2.367, 95% CI: 3.84 to 13.12 and a p-value of < 0.0001 (Figure 2(B)), suggesting a vital role of galectin-3 in the onset of SLE. However, significant heterogeneity was observed (Tau Square: 32.57, Q: 196.03, Pheterogeneity: < 0.0001, and I Square: 96.93). Combined analysis for the association of galectin-3 with SLE. Mean galectin 3 levels in SLE cases, as reported in various publications, was compared through a meta-analysis. (a) A funnel plot is utilized to evaluate the presence of publication bias. (b) A forest plot illustrates the association between Galectin 3 and SLE. (c) A sensitivity plot is employed to assess the robustness of the meta-analysis.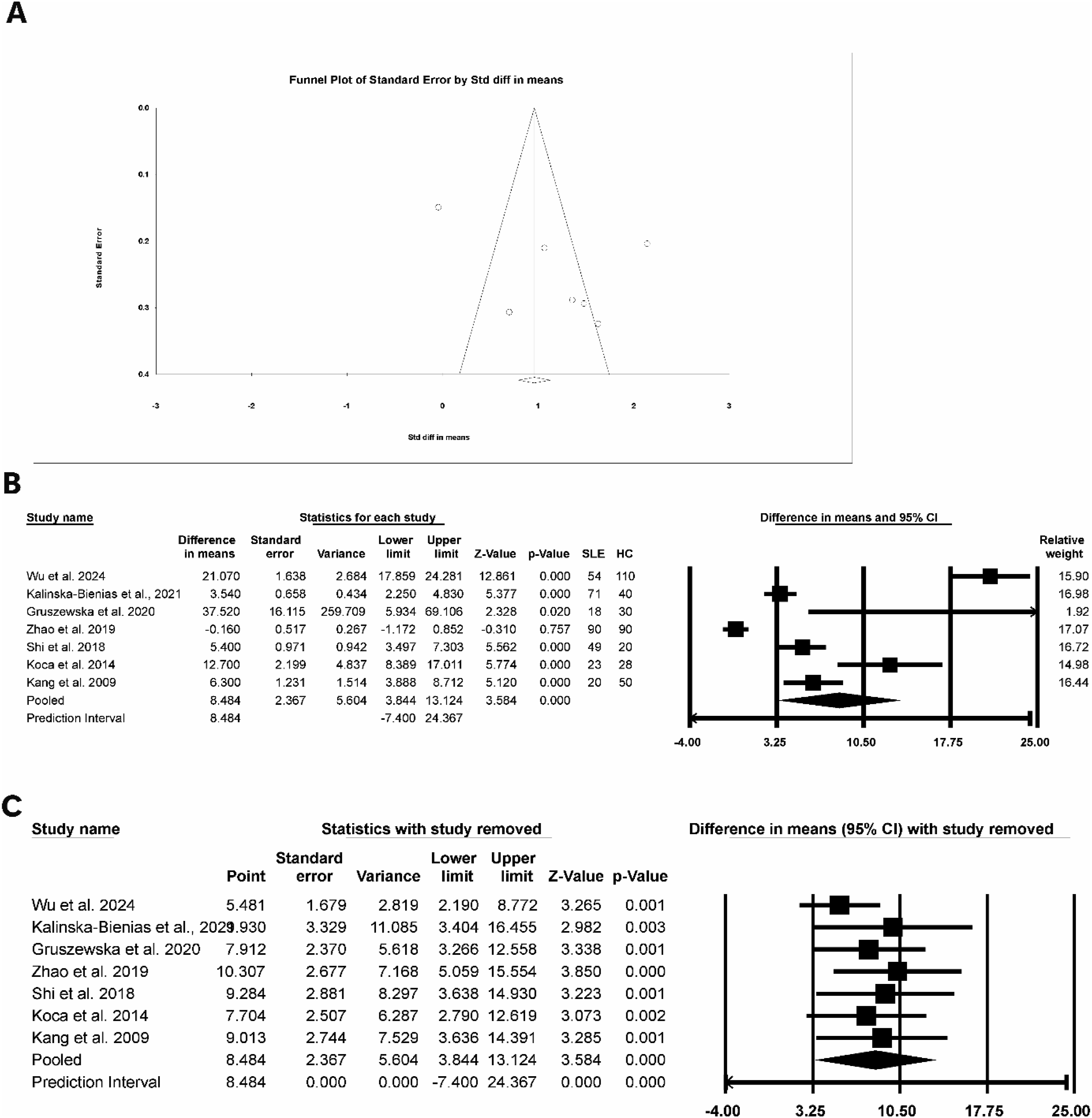
Subgroup analysis
As the combined analysis revealed the presence of significant heterogeneity, we explored various subgroup analyses and broadly subgrouped based on (i) ethnicity (Asian and non-Asian), (ii) mean age (<38 years and ≥38 years), (iii) patient sample size (<50 and ≥50), (iv) assay method (ELISA and non-ELISA), and (v) NOS value of the enrolled study (≤6 and >6).
Similar to the overall assessment, considerably greater level of galectin-3 was examined in SLE patients in both the Asian (MD: 8.03, SE: 3.71, 95% CI: 0.75 to 15.31, p = 0.031) and non-Asian groups (MD: 10.12, SE: 4.78, 95% CI: 0.74 to 19.51, p = 0.034) (Supplemental Figure 2). Interestingly, for all subgroup analysis similar observations were observed [mean age <38 years (MD: 5.75, SE: 2.40, 95% CI: 1.03 to 10.47, p = 0.01), mean age ≥38 years (MD: 16.25, SE: 8.11, 95% CI: 0.35 to 32.15, p = 0.04) (Supplemental Figure 3); Number of patients enrolled < 50 (MD: 8.10, SE: 1.92, 95% CI: 4.33 to 11.86, p < 0.0001), number of patients enrolled ≥50 (MD: 7.93, SE: 3.95, 95% CI: 0.18 to 15.88, p < 0.0001) (Supplemental Figure 4); ELISA (MD: 5.12, SE: 1.64, 95% CI: 1.90 to 8.35, p = 0.002), Non-ELISA (MD: 21.48, SE: 2.57, 95% CI: 16.44 to 26.52, p < 0.0001) (Supplemental Figure 5); NOS ≤6 (MD: 6.05, SE: 1.39, 95% CI: 3.32 to 8.77, p < 0.0001), NOS >6 (MD: 9.06, SE: 3.52, 95% CI: 2.16 to 15.97, p = 0.01) (Supplemental Figure 6)].
Sensitivity analysis
To verify the robustness of the pooled estimates, a leave-one-out sensitivity analysis was performed by consecutively excluding one study at a time and recomputing the pooled effect size. 24 The results demonstrated that excluding any one of the study did not significantly modify the overall pooled estimate for the association between galectin-3 levels and SLE, signifying that the findings of the primary meta-analysis were statistically robust (Figure 2). However, some variability was observed in subgroup analyses stratified by ethnicity, mean participant age, sample size, assay methods, and study quality (NOS score) (Supplemental Figures 2–6). These variations could be the resultant of the lower number of studies in subgroups.
Trial sequential analysis
TSA is a powerful statistical analysis employed in meta-analyses to enhance the reliability of conclusions by mitigating statistical errors, such as type I and type II errors, that frequently occur when combining data from multiple investigations. The TSA evaluates whether the considered sample size and evidence are adequate to support a definitive conclusion, or whether further investigation is necessary, thereby reducing the risk of false positives and false negatives.23,25
The cumulative Z-curve crosses the alpha spending boundary, reaches the required information size, or crosses the futility boundary, indicating inclusion of enough investigations in the meta-analysis. In the present study, as illustrated in Supplemental Figure 7, the cumulative z-curve for galectin-3 levels in SLE against healthy controls surpassed the monitoring boundary and attained the Required Information Size (RIS) line. The RIS of 685 represents the combined number of participants (SLE patients and healthy controls) required to achieve adequate statistical power. The cumulative sample size included in the present meta-analysis exceeded this threshold, indicating that the available evidence is sufficient according to TSA criteria, and consequently, no further studies are warranted.
Discussion
Galectin-3 is a multifunctional lectin that participates in a variety of biological processes, such as the regulation of immune responses, inflammation, apoptosis, and tissue remodeling. 7 Various cells, such as macrophages, dendritic cells, and T and B lymphocytes, as well as structural cells such as endothelial and epithelial cells, are involved in these activities.7,26 As galectin-3 mediates these biological processes, it is often considered to be linked to the development of autoimmune diseases. Therefore, it has become of interest to many researchers as a potential biomarker and mediator of autoimmune diseases, including SLE.
In this study, a systematic review and meta-analysis were performed to evaluate the association between circulating Galectin-3 levels and SLE. Our results showed that seven eligible case-control studies included in this analysis demonstrated that patients with SLE have significantly elevated levels of circulating Galectin-3 compared to healthy controls. These findings suggest that possible involvement of Galectin-3 in the underlying mechanisms of SLE. These findings are in agreement with previous investigations, which have also demonstrated that patients with SLE have significantly increased levels of circulating Galectin-3 than healthy individuals.10,13 Therefore, the potential findings of this meta-analysis reinforce that Galectin-3 may be associated with SLE.
Galectin-3 is known to participate in multiple biological functions that may contribute to SLE development. For instance, galectin-3 regulates the adhesion, migration, and activation of immune cells.27,28 Additionally, dysregulated immune responses in SLE lead to the generation of autoantibodies and immune complexes that can damage various tissues. Experimental studies have shown that galectin-3 can activate macrophages, dendritic cells, and T and B cells.7,12 Galectin-3 is also regulating cytokine activity. For instance, galectin-3 can bind to the IFN-γ receptor, a cytokine that plays a fundamental role in the pathogenesis of SLE. 29
Further support for the role of galectin-3 in the pathogenesis of SLE comes from experimental studies using galectin-3-deficient mice. For example, galectin-3-deficient mice have lupus-like manifestations, including increased IFN-γ levels and the formation of germinal centers, both of which are associated with SLE activity. 30 Conversely, other experimental studies using galectin-3 knockout mice have revealed reduced development of lupus-like manifestations, such as diffuse alveolar hemorrhage, lupus nephritis, and autoantibody production. 9 These contrasting findings suggest that galectin-3 may play a complex role in regulating immune responses and the progression of autoimmune inflammatory diseases, such as SLE. However, these proposed mechanisms for galectin-3’s role in SLE may explain the elevated galectin-3 levels observed in patients with SLE.
Another aspect of galectin-3 linked to SLE is its potential role in tissue damage. Lupus nephritis is a severe and often life-threatening manifestation of SLE. Galectin-3 plays a role in fibrogenesis and extracellular matrix remodeling, processes associated with tissue damage in lupus nephritis. Studies of patients with SLE have established that galectin-3 levels correlate with the presence of lupus nephritis and the development of renal fibrosis. 9 In addition, galectin-3-binding protein (G3BP) has also been studied as a potential biomarker for SLE and lupus nephritis. For instance, G3BP levels in the urine of patients with SLE have been shown to correlate with the activity of lupus nephritis.31,32 These observations support that galectin-3 may mediate tissue damage associated with SLE.
Another interesting aspect of galectin-3 in the context of SLE is its potential as an autoantigen. Antibodies to galectin-3 have been identified in the sera of patients with SLE.33,34 These anti-Galectin-3 antibodies have been found to promote the production of inflammatory cytokines and vascular inflammation. 35 The detection of anti-Galectin-3 antibodies in the sera of patients with SLE and the demonstrated pathogenic effects of galectin-3 suggest that galectin-3 may contribute to disease progression of SLE. Thus, galectin-3 has the potential to be both a biomarker and a mediator of SLE.
Despite the significant results from the studies included in this systematic review and meta-analysis, a high degree of heterogeneity was observed across them. High heterogeneity is often present in biomarker-based meta-analyses. Subgroup analyses by several variables, including patients’ ethnicity, age, study sample size, assay method of Galectin-3 measurement, and study quality, were performed to assess whether these variables contributed to the heterogeneity of the results. However, the results of these subgroup analyses were similar to those of the analysis of all studies. These findings suggest the reliability of the conclusions of this meta-analysis.
Subgroup analysis also demonstrated that the mean difference was higher in studies that used non-ELISA methods to determine Galectin-3 levels (MD = 21.48) than those that used ELISA methods (MD = 5.12). Such differences in mean differences between the two types of assays is likely due to the differences in the methods used by each type of assay rather than the true biological differences in Galectin-3 levels. ELISA methods are generally performed in a similar way in each assay, while non-ELISA methods encompass a variety of different analytical techniques, each of which may be sensitive to different factors that contribute to variability in the measured Galectin-3 levels. Thus, the larger mean difference within the non-ELISA methods subgroup is likely due to this variability in the methods of measuring Galectin-3 levels. Therefore, these subgroup analysis results should be interpreted with caution, and suggest the need for standardizing the assays used to measure Galectin-3 levels among research studies.
Additionally, the results of the sensitivity analyses, publication bias analyses, and trial sequential analyses support the reliability of the present study’s results. The moderate publication bias observed in the subgroup with a mean age <38 years may reflect the small number of available studies, differences in disease severity among younger SLE patients, and selective publication of statistically significant findings. Because publication bias tests have limited power when only a few studies are included, this observation should be interpreted cautiously. Furthermore, the trial sequential analysis demonstrated that the cumulative sample size exceeded the RIS of 685 participants. Importantly, the RIS refers to the total number of participants included in the analysis (SLE patients plus healthy controls) rather than the number of SLE patients alone, indicating that the available evidence is statistically sufficient according to TSA criteria.
This study provides important implications for the management of patients with SLE. As mentioned earlier, there are difficulties in detecting and monitoring SLE. Various laboratory tests are often used to diagnose SLE, such as measuring serum anti-dsDNA antibody and complement component levels and inflammatory markers in the blood. However, these markers do not always provide a complete representation of SLE status in individual patients. Therefore, galectin-3 may be a useful biomarker for SLE. It has been reported in researches that the diagnostic value of galectin-3 in musculoskeletal and rheumatic diseases is similar to that of common inflammatory markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). 28 Therefore, galectin-3 levels may be useful for monitoring SLE activity and potentially for early detection of complications, such as lupus nephritis.
A key strength of this investigation is that it represents one of the earliest comprehensive attempts to systematically synthesize available evidence on circulating galectin-3 levels in patients with SLE. Additionally, various methods were employed in the study to ensure the credibility of the conclusions of the findings. Furthermore, subgroup analyses of the studies were done to find out the potential impact of different variables on galectin-3 levels in patients with SLE.
However, the current investigation has a few limitations. For instance, only a few number of studies were incorporated in the meta-analysis. Additionally, most studies lacked clinical information on the patients included. Finally, as previously stated, a high level of heterogeneity was recorded among the studies, possibly due to differences in the variables studied. Most of the researches covered in this meta-analysis were cross-sectional, making it unfeasible to draw conclusions about the causal relationship between galectin-3 and SLE. Another important limitation is the restricted geographical representation of the included studies. The available evidence was derived primarily from Asian and Eastern European populations (China, Republic of Korea, Turkey, and Poland), with no eligible studies identified from North American, South American, African, or other major populations. Consequently, caution should be exercised when extrapolating the present findings to ethnically and geographically diverse populations.
Future studies should address the limitations of the current investigation. For example, prospective and longitudinal studies using larger cohorts of patients with SLE may help investigate the relationship between galectin-3 levels and SLE activity, treatment response, and other disease manifestations. Furthermore, studying the role of galectin-3 in the pathogenic processes of SLE may provide new insights into this protein’s role in the development of lupus and its treatment.
Conclusion
In summary, the present systematic review and meta-analysis demonstrate that circulating galectin-3 levels are significantly elevated in SLE patients compared with healthy controls, suggesting a potential role of Galectin-3 in the immunopathogenesis of SLE. These findings highlight galectin-3 as a promising biomarker associated with inflammatory and immune-mediated processes in lupus. However, the presence of substantial heterogeneity and the limited number of available studies warrant cautious interpretation. Further large-scale prospective and mechanistic studies are needed to clarify the clinical utility of galectin-3 in disease diagnosis, monitoring, and prognosis in SLE.
Supplemental material
Supplemental material - Association of galectin-3 in systemic lupus erythematosus: A systematic review and meta- analysis
Supplemental material for Association of galectin-3 in systemic lupus erythematosus: A systematic review and meta-analysis by Shovit Ranjan, Madhavi Dubey and Aditya K. Panda in Lupus.
Footnotes
Acknowledgements
Aditya K Panda receives support from the Anusandhan National Research Foundation (ANRF), New Delhi, India, through the PAIR Network program (ANRF/PAIR/2025/000029/PAIR).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.