
Abstract
Background
Lupus nephritis (LN) predominantly affects women of reproductive age and carries substantial risks during pregnancy, including disease flare, preeclampsia, acute kidney injury, and adverse fetal outcomes. The therapeutic armamentarium for LN has expanded considerably with the approval of voclosporin, belimumab, and obinutuzumab, yet pregnancy safety data for these agents remain conspicuously absent. Concurrently, the 2024 EULAR recommendations for antirheumatic drugs in reproduction, the 2025 EULAR lupus nephritis update, and the 2024 KDIGO guidelines have reset the landscape of management guidance. This review critically appraises the evidence on the safety and clinical use of all current LN-relevant immunosuppressive and biologic therapies during pregnancy, lactation, and the periconceptional period.
Methods
A comprehensive narrative review of literature published between January 2000 and May 2025 was conducted using PubMed, MEDLINE, EMBASE, and Cochrane databases. Key guidelines, pregnancy registries, and landmark clinical trial data were incorporated.
Results
Hydroxychloroquine and azathioprine remain the cornerstones of pregnancy-compatible LN management. Tacrolimus is an acceptable calcineurin inhibitor with appropriate therapeutic drug monitoring. Low-dose aspirin is recommended universally to reduce preeclampsia risk. Mycophenolate mofetil is teratogenic and absolutely contraindicated in the first trimester. Voclosporin and obinutuzumab lack any pregnancy safety data and should be avoided. Belimumab data from the pregnancy registry have not raised major signals; selective use may be considered in refractory cases. Rituximab may be used cautiously for life-threatening disease, avoiding the third trimester due to neonatal B-cell depletion. Anifrolumab has no pregnancy data and should be reserved for situations where no compatible alternative exists.
Conclusion
The growing number of effective LN therapies creates both opportunities and new dilemmas in pregnancy management. A structured, phase-based approach to drug selection — anchored in preconception counselling, timely medication switches, and multidisciplinary surveillance — is essential to optimise maternal and fetal outcomes. Dedicated pregnancy registries for novel biologics are urgently needed.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease that disproportionately affects women during their reproductive years, with a peak incidence between ages 15 and 45 and a female-to-male ratio of approximately 9:1.1,2 Lupus nephritis (LN) — defined by renal immune complex deposition and inflammatory injury — develops in 40–70% of SLE patients and represents one of the most severe disease manifestations. 3
The intersection of LN and pregnancy constitutes one of the most challenging clinical scenarios in nephrology and rheumatology. LN in pregnancy substantially elevates the risk of preeclampsia (7–35%), disease flare (25–65%), acute kidney injury, intrauterine growth restriction (IUGR), preterm delivery, and fetal loss.4,5 Conversely, uncontrolled maternal disease carries its own considerable fetal risks — a therapeutic dilemma demanding precise, evidence-based management.
The LN therapeutic landscape has been transformed over the past 5 years. Voclosporin, belimumab, and obinutuzumab have received regulatory approval and are now incorporated into the 2025 EULAR lupus nephritis update, the 2024 KDIGO Glomerular Diseases guideline, and the 2024 ACR guideline as induction and/or maintenance options.6,7,8 Yet each was studied in trials that systematically excluded pregnant women, and dedicated pregnancy safety data remain virtually absent. The 2024 EULAR recommendations for antirheumatic drugs in reproduction consolidate guidance for older agents but candidly acknowledge the paucity of evidence for newer biologics. 9 This evidence gap is of direct clinical relevance: a woman achieving LN remission on voclosporin-based triple therapy faces a situation in which no approved pregnancy-compatible equivalent exists.
This narrative review provides a comprehensive, clinician-oriented synthesis of immunosuppressive and biologic drug safety in LN pregnancies, from preconception counselling through the postpartum period, addressing mechanism, teratogenicity data, guideline recommendations, and practical substitution strategies.
Literature search strategy
A comprehensive narrative review was conducted in PubMed/MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews, covering publications from January 2000 to May 2025. The following MeSH terms and free-text keywords were combined using Boolean operators (AND/OR): “lupus nephritis” OR “systemic lupus erythematosus” AND “pregnancy” OR “periconceptional” OR “lactation” OR “breastfeeding” AND “immunosuppressive therapy” OR “biologics” OR “belimumab” OR “rituximab” OR “obinutuzumab” OR “voclosporin” OR “anifrolumab” OR “hydroxychloroquine” OR “azathioprine” OR “mycophenolate mofetil” OR “tacrolimus” OR “cyclophosphamide” OR “corticosteroids”. Supplementary searches were performed for individual drug names combined with “pregnancy safety,” “teratogenicity,” “fetal outcomes,” and “pregnancy registry.”
The following inclusion criteria were applied: (1) original research articles, systematic reviews, meta-analyses, and narrative reviews addressing the use of immunosuppressive or biologic agents in SLE or LN during pregnancy or the periconceptional period; (2) clinical guidelines and consensus statements from major professional societies (EULAR, ACR, KDIGO, ERA); (3) prospective pregnancy registries and pharmacovigilance reports for agents approved in LN (belimumab, voclosporin, obinutuzumab, anifrolumab); and (4) case series with a minimum of five reported pregnancies, provided they offered mechanistic or safety data not available elsewhere. Exclusion criteria included: (1) single case reports without systematic data synthesis; (2) studies focused exclusively on non-renal SLE manifestations without extractable nephritis subgroup data; (3) animal studies, unless no human data existed for a specific agent; and (4) publications available only as conference abstracts without accompanying peer-reviewed full text. Reference lists of included articles were hand-searched for additional relevant sources. All included evidence was narratively synthesised, with guideline recommendations and registry data prioritised over retrospective observational data where applicable.
Pathophysiological and risk considerations
The immunological adaptations of normal pregnancy — dominated by a Th2/regulatory T-cell shift promoting tolerance of the fetal allograft — are in inherent tension with the Th1/Th17-dominant pathophysiology of SLE and LN. 10 The net effect is unpredictable: some patients experience suppression of lupus activity during pregnancy; others flare, particularly in the postpartum period when immune suppression withdraws. 11
The overlap between active LN flare and preeclampsia is diagnostically challenging: both manifest with new or worsening hypertension, proteinuria, and renal impairment after 20 weeks. LN flare is typically accompanied by rising anti-dsDNA titres, falling complement (C3/C4), active urinary sediment (haematuria, cellular casts), and extra-renal SLE features — absent in pure preeclampsia.12,13 Accurate differentiation determines whether the clinical response is escalated immunosuppression versus delivery.
Risk stratification at conception is the critical determinant of outcomes. Active nephritis, eGFR <40 mL/min, proteinuria >1 g/day, hypertension, antiphospholipid antibodies, and prior nephritis flare independently predict adverse outcomes. 14 The 2024 Lancet Rheumatology systematic review confirmed previous LN, chronic hypertension, active SLE at conception, and secondary antiphospholipid syndrome as the four strongest predictors of adverse pregnancy outcomes. 15 Achieving complete or partial renal remission for at least 6 months before conception remains the primary objective of preconception counselling.
General principles of drug management
The overarching framework is guided by three principles: (1) maintain the lowest disease activity with the fewest potentially harmful medications; (2) never leave LN untreated in pregnancy, as uncontrolled maternal disease carries greater fetal risk than most compatible medications; and (3) plan medication transitions proactively, ideally six to twelvemonths before conception.6,9
The 2024 EULAR recommendations affirm that hydroxychloroquine, azathioprine, tacrolimus, low-dose prednisone, and low-dose aspirin are compatible with pregnancy and should not be discontinued. 9 Belimumab data do not currently raise major concerns but are limited; rituximab should be reserved for severe or refractory disease with avoidance in the third trimester; and voclosporin, obinutuzumab, and anifrolumab lack sufficient data for routine use. 9 Multidisciplinary management — nephrology, rheumatology, maternal-fetal medicine, and neonatology — is universally recommended; all LN pregnancies should be managed in specialised centres.6,8,9
Pregnancy-compatible agents: Evidence and practical guidance
Hydroxychloroquine
Hydroxychloroquine (HCQ) is the single most important drug in LN pregnancy management and is strongly recommended as foundational therapy throughout pregnancy and the periconceptional period by all major guidelines.6,8,9 Its benefits are multifaceted: HCQ reduces flare risk during pregnancy, lowers preeclampsia incidence, decreases congenital heart block risk in anti-Ro/La-positive women, and provides long-term cardiovascular and renal protection.16,17 Multiple prospective cohort studies and registry analyses have found no increased risk of major congenital malformations attributable to HCQ.18,19
Pharmacokinetic studies have demonstrated that apparent HCQ clearance increases by approximately 60% during pregnancy, with a corresponding reduction in half-life of roughly 10 days compared with the postpartum period. 20 Critically, average HCQ concentrations ≤100 ng/mL have been associated with a significantly elevated odds of preterm birth (OR 11.2; 95% CI 2.3–54.2; p = 0.003) in pharmacokinetic modelling, 20 raising the clinical consideration of therapeutic drug monitoring during pregnancy in high-risk patients. HCQ is compatible with breastfeeding; infant exposure through breast milk is minimal. 9 Discontinuation postpartum should be strongly discouraged given the elevated flare risk.
Azathioprine
Azathioprine (AZA) is the preferred immunosuppressant for LN maintenance during pregnancy, serving as the standard substitute for mycophenolate mofetil. The fetal liver lacks inosinate pyrophosphorylase — the enzyme required to convert AZA to its active metabolites — which partially explains its relative fetal safety compared with MMF. 21 Evidence from SLE cohorts and inflammatory bowel disease registries consistently supports AZA safety at doses ≤2 mg/kg/day.21,22 A key LN-specific study confirmed that switching from MMF to AZA at least 6 weeks before conception was associated with low LN flare rates and no significant increase in adverse fetal outcomes. 23 The switch must be planned preconceptionally; MMF-to-AZA transition initiated after confirmation of pregnancy eliminates the window of protection during the highest-risk teratogenic period.
Low-dose corticosteroids
Prednisone ≤10 mg/day is compatible with pregnancy throughout all trimesters. Prednisone and prednisolone are preferentially inactivated by placental 11β-hydroxysteroid dehydrogenase, limiting fetal exposure to approximately 10% of maternal concentrations. 24 Prolonged use above 20 mg/day increases the risks of gestational diabetes, premature rupture of membranes, IUGR, and maternal hypertension; doses should be tapered to the lowest effective level. 24 Short courses of intravenous methylprednisolone for acute moderate-to-severe flare are acceptable in all trimesters. Peripartum stress dosing is indicated for women on prednisone ≥7.5 mg/day for more than 3 weeks.
Tacrolimus
Tacrolimus has decades of safety data from solid organ transplantation pregnancies. Available data from transplant registries and LN cohorts indicate no direct teratogenicity; the primary fetal risks — IUGR and prematurity — appear dose-dependent and mediated by placental vasoconstriction. 25 Therapeutic drug monitoring is essential, with trough levels maintained at 4–8 ng/mL throughout pregnancy. Tacrolimus is the calcineurin inhibitor of choice as a substitute for voclosporin in patients planning pregnancy, and the substitution should be planned preconceptionally.
Low-dose aspirin
Low-dose aspirin (75–150 mg/day) is universally recommended for all LN pregnancies, initiated between 12 and 16 weeks of gestation, as prophylaxis against preeclampsia.6,8,9,26 LN confers a baseline preeclampsia risk of 7–35% depending on disease activity and antibody profile. Aspirin should be ceased at 36 weeks to avoid premature closure of the ductus arteriosus and neonatal bleeding complications.
Agents requiring cessation, bridging, or exceptional use
Mycophenolate mofetil
Mycophenolate mofetil (MMF) — the most widely prescribed LN maintenance immunosuppressant globally — is a well-established human teratogen, absolutely contraindicated throughout the first trimester. 27 MMF embryopathy is a recognisable pattern of malformations encompassing cleft lip and palate, microtia, external auditory canal atresia, chorioretinal coloboma, and cardiac defects.27,28 The risk of congenital malformation with first-trimester MMF exposure in non-transplant populations is estimated at approximately 25%, compared with 4–5% in the general population. 27 Women who conceive unexpectedly on MMF must discontinue it immediately; detailed anatomical fetal ultrasound is mandatory.
A 2025 French case series reported eight pregnancies in which MMF was deliberately reintroduced after completion of organogenesis (i.e., after the first trimester) for highly refractory LN; seven resulted in successful live births with no cases of MMF-induced embryopathy at delivery. 29 Long-term follow-up at a mean of 6.5 years showed normal physical and neurological development in all living children. 29 This represents an exceptional measure outside standard guidelines, applicable only in specialist centres with extensive multidisciplinary counselling, documented informed consent, and no viable alternative immunosuppressant.
Cyclophosphamide
Cyclophosphamide (CYC) is among the most potent teratogens in clinical use. First-trimester exposure during weeks 5–12 is associated with fetal loss and cyclophosphamide embryopathy (IUGR, microcephaly, abnormal digits). 30 CYC is absolutely contraindicated in the first trimester. In the second and third trimesters, IUGR, bone marrow suppression, and premature delivery remain concerns, and CYC is reserved exclusively for life-threatening or organ-threatening LN. 30 With the advent of rituximab as an alternative for severe refractory disease, the threshold for CYC use in pregnancy has risen; rituximab may be preferred in the second trimester given its less severe direct fetal toxicity profile.
Voclosporin
Voclosporin (Lupkynis®), a novel calcineurin inhibitor approved in 2021, demonstrated superior proteinuria reduction versus standard of care in the AURORA-1 trial. 31 However, it carries a complete absence of human pregnancy safety data. The 2024 EULAR recommendations state explicitly that voclosporin has insufficient safety data and should be avoided. 9 The formulation additionally contains ethanol as an excipient — a recognised fetal neurotoxin — adding to the case for avoidance in pregnancy. 32 Women achieving LN remission on voclosporin-based triple therapy who plan pregnancy require preconception transition to tacrolimus at least 3 months before conception, with close LN monitoring during the switch.
Biologic therapies: Evidence review and practical guidance
Belimumab
Belimumab (Benlysta®), a fully human monoclonal antibody targeting BLyS/BAFF, is approved for active LN and consolidated by the BLISS-LN trial and 2024–2025 guideline updates as part of triple therapy with MMF and glucocorticoids.6,7,8 Pregnancy data derive primarily from the Belimumab Pregnancy Registry (BPR, GSK study BEL114256), a prospective observational registry established at drug approval. Interim data through March 2021 did not identify an excess of major birth defects compared with disease-matched controls. 33 In reproductive toxicology studies in cynomolgus monkeys, belimumab crossed the placental barrier and was detected in fetal cord blood without evidence of fetal harm at 9–20-fold the maximum recommended human dose. 33
The 2024 EULAR reproductive health recommendations concluded that limited data on belimumab in pregnancy do not raise concerns about in utero exposure, positioning it as conditionally acceptable — not routinely recommended but not absolutely contraindicated. 9 A practical approach for women who conceive while on maintenance belimumab or who require it for refractory LN involves selective continuation in the first and early second trimester, with cessation before the third trimester if clinically feasible. Anti-B-cell effects in the neonate are theoretically possible but have not been formally reported. 9 The Belimumab Pregnancy Registry remains open and further data accrual is essential.
Rituximab
Rituximab, a chimeric type I anti-CD20 monoclonal antibody, is used off-label in refractory or relapsing LN and in the rituximab-belimumab sequential combination strategy. 34 Its role is recognised in EULAR 2025, ACR 2024, and KDIGO 2024 guidelines as a rescue option.6,7,8 IgG antibodies are actively transported across the placenta via the neonatal Fc receptor, with transfer increasing substantially in the second and third trimesters. The primary concern is neonatal B-cell depletion: infants born to mothers receiving rituximab in the second or third trimester may develop transient peripheral B-cell depletion and occasional cytopenias. 35 Available case series confirm this depletion is generally transient, with B-cell counts recovering within 6 months of birth, and without serious neonatal infections in published data.9,35
The 2024 EULAR recommendations conditionally support rituximab use when no compatible alternative can control organ-threatening or life-threatening disease, with explicit recommendation to avoid use in the third trimester. 9 Key practical considerations include: use as early as possible in gestation if required to minimise third-trimester placental transfer; full blood count and B-lymphocyte subset assessment in all in utero-exposed infants; and delay of live-attenuated vaccines in the infant for at least 6 months after birth.9,36
Obinutuzumab
Obinutuzumab (Gazyvaro®), a humanised type II anti-CD20 monoclonal antibody with superior B-cell depletion compared with rituximab, was studied in the pivotal REGENCY phase 3 trial — published in the New England Journal of Medicine in February 2025 — which demonstrated significantly higher complete renal response rates, leading to incorporation into the 2025 EULAR LN recommendations.7,37 No human pregnancy safety data exist. Given that obinutuzumab shares the anti-CD20 mechanism with rituximab but with substantially greater potency and more prolonged B-cell depletion (often 12–24 months following a single course), the expected neonatal risk profile is at least as concerning as that of rituximab, and potentially considerably greater. 38 No pregnancy registry exists. Obinutuzumab should not be used in pregnancy, and women must be counselled that conception should be deferred until B-cell counts have fully normalised following administration.
Anifrolumab
Anifrolumab (Saphnelo®), a fully human monoclonal antibody targeting IFNAR1, is approved for moderate-to-severe SLE; phase 2 data suggest potential LN benefit. 39 No pregnancy safety data exist. The 2024 EULAR recommendations state explicitly that anifrolumab should be used in pregnancy only if no pregnancy-compatible medication can effectively control maternal disease 9 — a statement that effectively represents a contraindication in routine LN management, given the availability of multiple compatible alternatives. Until prospective data from the Saphnelo® Pregnancy Registry are available, anifrolumab should not form part of LN management in pregnancy or in women actively planning conception.
Monitoring and multidisciplinary management framework
Preconception assessment
The preconception visit is the most important consultation in LN pregnancy management. Goals include: confirming disease remission (complete or partial renal remission for ≥6 months); establishing baseline eGFR, uPCR, blood pressure, and serological profile (anti-dsDNA, C3/C4, anti-Ro/La, antiphospholipid antibodies); reviewing all medications for pregnancy compatibility and implementing necessary substitutions; vaccinating against pneumococcus, influenza, and hepatitis B; ensuring adequate folate supplementation; and addressing contraception. Target blood pressure <130/80 mmHg before conception reduces superimposed preeclampsia risk.
General principles of vaccination before conception
Vaccination is a cornerstone of preconception preparation in women with LN, given the substantially increased susceptibility to vaccine-preventable infections associated with both the underlying immunological dysregulation of SLE and the prolonged immunosuppressive therapy required for disease control. 36 The periconceptional period — ideally six to 12 months before planned conception — represents the last opportunity to administer certain vaccines, since live-attenuated vaccines are contraindicated during pregnancy and immediately after biologic therapy.
The 2024 EULAR recommendations for antirheumatic drugs in reproduction, together with the 2019 EULAR recommendations on vaccination in adult patients with autoimmune inflammatory rheumatic diseases, provide the primary framework for vaccination guidance in this population.9,40 The following principles apply: (1) Inactivated vaccines — including influenza (annual), pneumococcal (PCV15/PCV20 or PPSV23), hepatitis B, hepatitis A, pertussis (Tdap), and COVID-19 — are safe and recommended before, during, and after pregnancy in women with LN, irrespective of immunosuppressive therapy. (2) Live-attenuated vaccines — including measles-mumps-rubella (MMR), varicella, herpes zoster (live formulation), and yellow fever — must be completed at least 4 weeks before conception, and are contraindicated during pregnancy and in women on biologic agents or high-dose immunosuppression. (3) Women receiving anti-CD20 therapy (rituximab, obinutuzumab) should be vaccinated at least 4 weeks before administration, as B-cell depletion substantially impairs vaccine immunogenicity; serological confirmation of adequate response is recommended where feasible. (4) Annual influenza vaccination is recommended throughout pregnancy as it reduces maternal and neonatal morbidity. (5) Pertussis (Tdap) vaccination is recommended during each pregnancy, preferably between 27 and 36 weeks of gestation, to provide passive neonatal immunity via transplacental antibody transfer. (6) Folate supplementation (5 mg/day given the risk of anti-folate effects of some immunosuppressants) should be initiated alongside vaccine review and continued through the first trimester. Vaccination status should be reviewed and updated at every preconception consultation, with documentation of immune status for hepatitis B and varicella where prior immunity is uncertain.
Antenatal and postpartum monitoring
At minimum, monthly clinical review with assessment of blood pressure, urinalysis, uPCR, serum creatinine and eGFR, and complement levels (C3/C4) is recommended throughout pregnancy.6,8 Anti-dsDNA titres should be measured at least every trimester and more frequently when flare is suspected. In anti-Ro/La-positive women, fetal echocardiography should be performed between 16 and 26 weeks to screen for congenital heart block. Serial fetal growth scans from 20 weeks are recommended.
The postpartum period represents the highest-risk window for LN flare, with rates peaking between three and 6 months post-delivery. 11 Monitoring at monthly intervals for the first 6 months is recommended. Women who suspended effective regimens for pregnancy should be systematically re-evaluated; return to MMF is appropriate once breastfeeding is concluded, or immediately if not breastfeeding.
Distinguishing LN flare from preeclampsia
Features favouring LN flare include rising anti-dsDNA titres, falling C3/C4, active urinary sediment with cellular casts, haematuria, extra-renal SLE manifestations, and onset before 20 weeks. 13 Features favouring preeclampsia include onset after 20 weeks, serological quiescence, normal complement, elevated sFlt-1/PlGF ratio, and absent haematuria. Renal biopsy in pregnancy carries higher bleeding risk and is reserved for cases where diagnosis materially changes management (Tables 1 and 2).
Summary tables
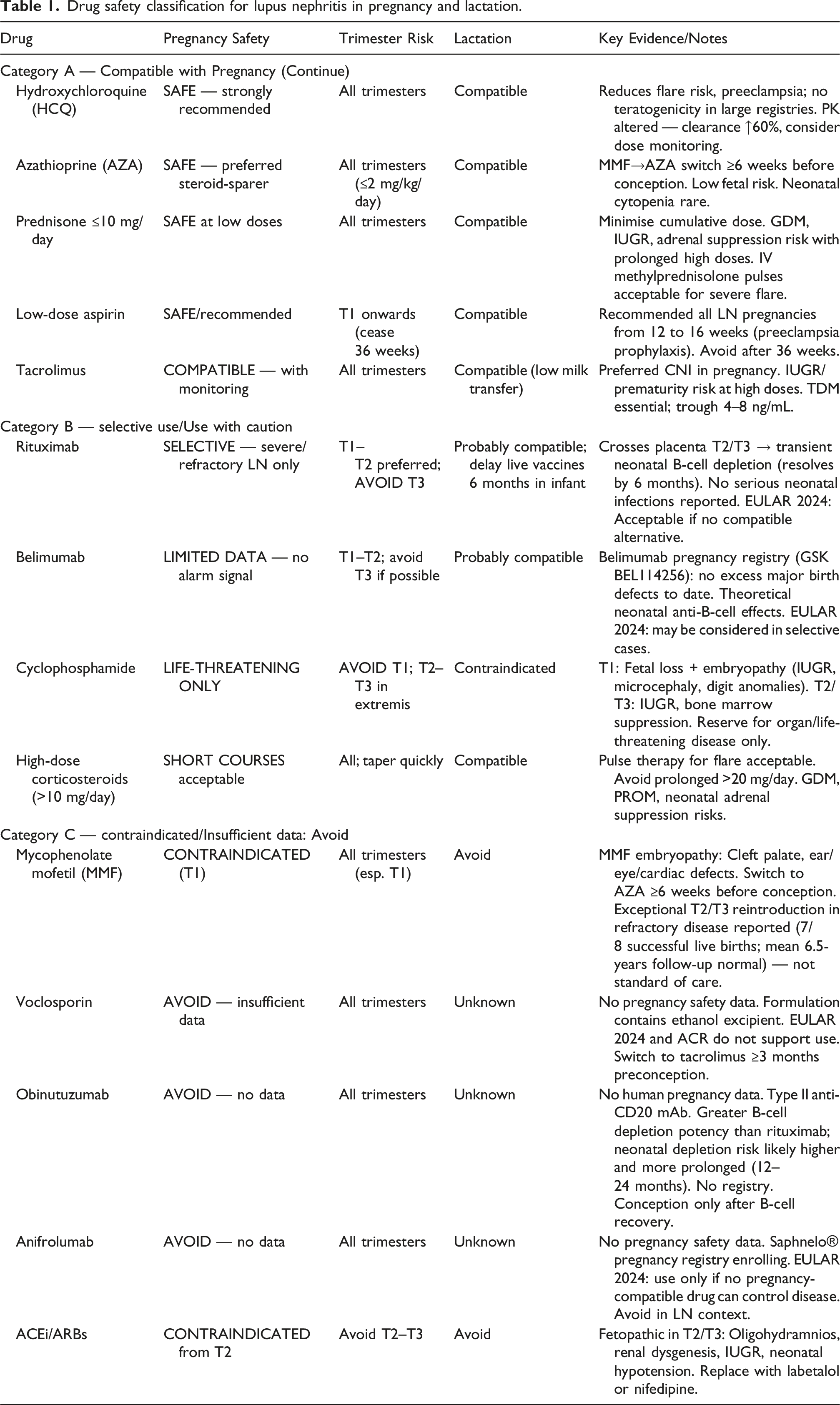
Drug safety classification for lupus nephritis in pregnancy and lactation.
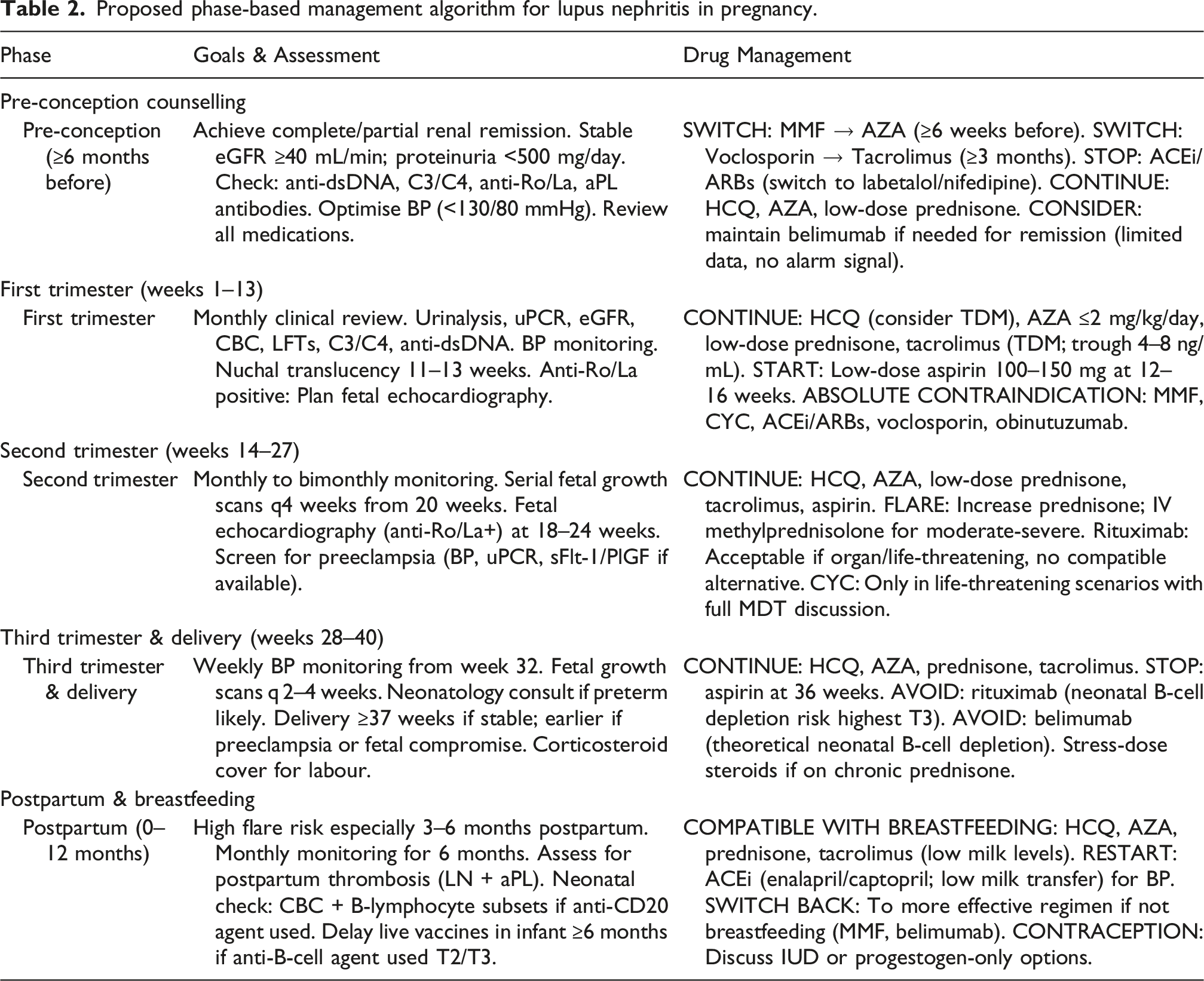
Proposed phase-based management algorithm for lupus nephritis in pregnancy.
Research gaps and future directions
Despite considerable progress in LN therapeutics, the evidence base for drug safety in LN pregnancy is characterised by fundamental limitations. All pivotal trials for voclosporin (AURORA-1/2), belimumab (BLISS-LN), and obinutuzumab (NOBILITY, REGENCY) systematically excluded pregnant women, creating an evidence void precisely in the population for which new drugs are most often prescribed. While the Belimumab Pregnancy Registry and Saphnelo® Pregnancy Registry exist, no comparable registries have been established for voclosporin or obinutuzumab — the latter an urgent priority now that obinutuzumab is a guideline-supported induction option.
Pharmacokinetic data in pregnant LN patients are almost entirely absent for newer agents, despite the substantial PK alterations of pregnancy (as exemplified by the HCQ clearance data). Long-term immunological, neurodevelopmental, and infectious outcomes in children exposed in utero to anti-CD20 agents require systematic study. Prospective validation of differential biomarkers for LN flare versus preeclampsia — including sFlt-1/PlGF, urinary TWEAK, and CXCL10 — in well-characterised LN pregnancy cohorts is lacking. Future research priorities include establishment of mandatory pharmacovigilance registries for all novel LN biologics, inclusion of women of reproductive age in post-marketing safety studies, and development of pregnancy-specific disease activity indices.
Conclusion
The management of lupus nephritis in pregnancy has entered a pivotal and paradoxical era. The same therapeutic advances transforming LN outcomes — voclosporin, belimumab, obinutuzumab — have simultaneously created a new category of clinical uncertainty: a growing proportion of women achieving remission on regimens that cannot be safely continued into pregnancy, and for which no equivalent pregnancy-compatible alternative has been validated.
The foundational principles remain robust: hydroxychloroquine is indispensable and should never be discontinued; azathioprine is the preferred immunosuppressant backbone; tacrolimus is the acceptable calcineurin inhibitor; preconception medication review and transition are non-negotiable; and multidisciplinary care in experienced centres is essential. MMF remains absolutely contraindicated in the first trimester. Voclosporin, obinutuzumab, and anifrolumab should be avoided until evidence emerges.
Belimumab and rituximab occupy an evolving middle ground — their use is neither routine nor absolutely prohibited, but governed by carefully individualised risk-benefit judgement in severe, refractory disease. This nuanced position demands that clinicians managing LN in reproductive-age women maintain active familiarity with emerging registry data. Most critically, comprehensive mandatory pregnancy registries for all agents approved for LN management must be established as an urgent priority. Without this infrastructure, the evidence-practice gap will widen in direct proportion to the number of novel therapies reaching clinical use.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.