
Abstract
Objective
To determine factors associated with hydroxychloroquine (HCQ)-induced retinopathy in Puerto Ricans with systemic lupus erythematosus (SLE) and to evaluate determinants of early HCQ-induced retinopathy.
Methods
We conducted a retrospective study of adult Puerto Ricans with SLE. Patients with ophthalmologist-confirmed HCQ-induced retinopathy were compared with those without retinopathy. A subgroup analysis comparing patients with early-onset (≤5 years) versus late-onset (>5 years) retinopathy was also performed. Demographic factors, clinical manifestations, and pharmacologic treatments were analyzed using bivariate methods and logistic regression models adjusted for SLE duration.
Results
A total of 279 patients were included; 41 had HCQ-induced retinopathy, while 238 did not. Among patients with HCQ-induced retinopathy, the mean age (SD) was 45.2 (13.2) years, and 90.2% were women. The mean (SD) SLE duration and HCQ treatment duration were 10.3 (7.7) years and 9.1 (5.8) years, respectively. Patients with HCQ-induced retinopathy were more likely to have higher daily and weight-adjusted HCQ doses and greater damage accrual, but were less likely to have proteinuria, lymphopenia, anti-dsDNA positivity, low complement levels or exposure to mycophenolate mofetil. Among patients with HCQ-induced retinopathy, 13 (31.7%) discontinued HCQ within 5 years of treatment initiation. In multivariable analysis, early-onset toxicity was associated with corticosteroid exposure.
Conclusions
In this cohort of Puerto Rican Hispanics with SLE, HCQ-induced retinopathy occurred in 14.7% of patients, and nearly 32% of those affected developed early-onset retinopathy. Retinopathy was primarily associated with higher daily and weight-adjusted HCQ doses, while early-onset retinopathy was associated with corticosteroid exposure. These findings provide population-specific data that may help optimize HCQ dosing and underscore the importance of regular ophthalmologic screening, even during the early years of therapy.
Keywords
Introduction
Hydroxychloroquine (HCQ) is an antimalarial drug with known immunomodulatory effects that is widely regarded as one of the most crucial therapeutic agents in the treatment of systemic lupus erythematosus (SLE). 1 Despite its efficacy, the prolonged HCQ use is associated with a risk of retinopathy, a potentially irreversible condition that can lead to permanent vision loss. 2 The American Academy of Ophthalmology (AAO) both 2016 and 2025 guidelines recommend a maximum daily HCQ dose of ≤5.0 mg/kg of actual body weight to reduce the risk of developing HCQ-induced retinopathy.3,4 In addition, the AAO advises a baseline fundus examination to exclude preexisting maculopathy and annual retinopathy screening starting after 5 years of treatment in patients without significant risk factors and on appropriate dosages. 3 Although these guidelines recommend performing the first ophthalmologic evaluation 5 years after starting HCQ, some studies have shown that HCQ-induced retinopathy can occur within the first 5 years of therapy.5,6
HCQ-induced retinopathy in SLE patients shows ethnic variability, yet Hispanic patients remain underrepresented in research. 7 Also, limited data exist on risk factors and on early-onset retinopathy. Therefore, we sought to determine the association of demographic factors, lupus manifestations, comorbidities, and medication exposure in Hispanics from Puerto Rico with HCQ-induced retinopathy, and identify factors linked to early-onset retinopathy.
Methods
Study design and population
A retrospective observational study was conducted in a cohort of Puerto Ricans with SLE followed at the lupus clinics of the University of Puerto Rico Medical Sciences Campus (UPR-MSC). The study period spanned from December 1987 to July 2024. Eligible participants were adults (≥21 years old), of Puerto Rican ethnicity (self and all four grandparents), and diagnosed with SLE according to the 1997 revised American College of Rheumatology (ACR) classification criteria. 8 Patients attended routine clinic visits every 3–4 months, with additional visits scheduled as needed based on disease activity or complications. At each routine visit, a structured questionnaire was completed to collect information on demographic characteristics, clinical manifestations, laboratory tests (complete blood count, comprehensive metabolic panel, urinalysis, erythrocyte sedimentation rate, C-reactive protein, lipid panel, anti-double-stranded DNA [anti-dsDNA] antibodies, and C3 and C4 complement levels), disease activity, disease damage, and pharmacologic treatment. A lupus autoantibody panel was performed for all patients at the time of SLE diagnosis, including antinuclear antibodies, anti-dsDNA antibodies, anti-Ro antibodies, anti-La antibodies, anti-Smith antibodies, anti-ribonucleoprotein (RNP) antibodies, anticardiolipin antibodies, lupus anticoagulant test, and C3 and C4 complement levels. Autoantibody testing was subsequently repeated as clinically indicated. This study was approved by the Institutional Review Board of the UPR-MSC (protocol# 2290033247).
Assessment of HCQ-induced retinopathy
SLE patients were evaluated at baseline and annually by an ophthalmologist or retinologist using fundus examination, spectral-domain optical coherence tomography (SD-OCT), and automated visual field testing. Hydroxychloroquine (HCQ) retinopathy was diagnosed if fundoscopy revealed parafoveal depigmentation or classic bull’s-eye maculopathy, or if optical coherence tomography (OCT) demonstrated thinning of the photoreceptor layer or disruption of the outer retina, particularly in the parafoveal region. 3 Patients were classified as cases if they had received HCQ and subsequently discontinued it due to HCQ-induced retinopathy confirmed by an ophthalmologist. Patients who continued HCQ therapy without developing HCQ-induced retinopathy were included as controls. Patients with HCQ-induced retinopathy were further classified as having early-onset (≤5 years) or late-onset (>5 years) retinopathy. Participants were excluded from the study if HCQ was discontinued for reasons other than retinopathy (e.g., non-adherence, allergic reactions, or other adverse effects), if there was no documented history of HCQ use, or if medical records were incomplete and precluded accurate assessment.
Variables
Variables from demographic, clinical, and pharmacologic domains were ascertained. Demographic factors included age, sex, and SLE duration. Cumulative (at any time during follow-up) clinical manifestations according to the American College of Rheumatology (ACR) classification criteria and serologic markers were determined. 8 Disease activity and damage at last study visit were assessed using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI).9,10 Comorbidities included tobacco use, overweight/obesity (body mass index ≥25 kg/m2), dyslipidemia, arterial hypertension, diabetes mellitus, coronary artery disease, congestive heart failure, stroke, chronic kidney disease, cataracts, diabetic retinopathy, and hypothyroidism. Current (at the last study visit) and cumulative pharmacologic treatments were evaluated. These included SLE therapies (HCQ, corticosteroids, mycophenolate mofetil (MMF), azathioprine, tacrolimus, methotrexate, cyclophosphamide, belimumab, and rituximab), as well as nonsteroidal anti-inflammatory drugs (NSAIDs), statins, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), low-dose aspirin, and tamoxifen. For HCQ, current and cumulative doses and weight-adjusted dosing (mg/kg/day) were also calculated.
Statistical analyses
First, demographic characteristics, SLE clinical manifestations, comorbidities, disease activity, disease damage, and pharmacologic treatments were compared between patients with and without HCQ-induced retinopathy using bivariate analyses. For patients with HCQ-induced retinopathy, the last study visit (current visit) corresponded to the date on which HCQ was discontinued. Student’s t tests were used for continuous variables and chi-square tests for categorical variables. Variables demonstrating statistical significance in bivariate analyses were subsequently evaluated in logistic regression models adjusted for SLE duration, with odds ratios (ORs) and 95% confidence intervals (CIs) reported.
A subgroup analysis was then performed among patients with HCQ-induced retinopathy to compare early (≤5 years) versus late (>5 years) onset of toxicity. Predictors showing statistical significance in the initial subgroup comparisons were entered into penalized logistic regression models adjusted for SLE duration. Firth’s penalized likelihood method was applied to address small-sample bias and separation. Odds ratios with 95% confidence intervals were reported.
In multivariable analyses across all study groups, models were adjusted for disease duration to account for potential differences in follow-up time between groups and to mitigate bias arising from longer exposure periods among patients who remained on therapy without developing HCQ-induced retinopathy compared with those who experienced earlier events.
A two-sided p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 13 (IBM Corp., Armonk, NY, USA), except for logistic regression analyses, which were conducted using StataNow/SE version 19.5 (StataCorp LLC, College Station, TX, USA).
Results
From the total cohort of 414 SLE patients, 135 did not meet the eligibility criteria and were excluded. Of the remaining 279 patients, 41 developed HCQ-induced retinopathy, while 238 continued HCQ therapy without evidence of retinopathy. Among patients with HCQ-induced retinopathy, the mean age (SD) was 45.2 (13.2) years, and 90.2% were women. The mean (SD) SLE duration was 10.3 (7.7) years, and the mean (SD) HCQ treatment duration was 9.1 (5.8) years. Figure 1 shows the distribution of HCQ treatment duration prior to discontinuation due to HCQ-induced retinopathy. HCQ exposure ranged from 1 to 23 years. The most frequent time to HCQ discontinuation occurred at 5 years (6 patients), followed by 6 years (5 patients). Overall, 13 patients (31.7%) discontinued HCQ within 5 years of treatment initiation. The mean HCQ dose based on actual body weight was 5.4 mg/kg/day. Of the 41 patients, 26 had a mean HCQ dose greater than 5 mg/kg/day, while 15 had a mean dose ≤5 mg/kg/day. 15 patients were diagnosed by fundus examination and 26 by OCT. It is important to note that some patients in this cohort initiated HCQ therapy prior to the 2016 revision of the American AAO guidelines, which recommended a maximum daily dose of ≤6.5 mg/kg based on ideal body weight. Distribution of hydroxychloroquine (HCQ) treatment duration among systemic lupus erythematous patients who developed HCQ-induced retinopathy.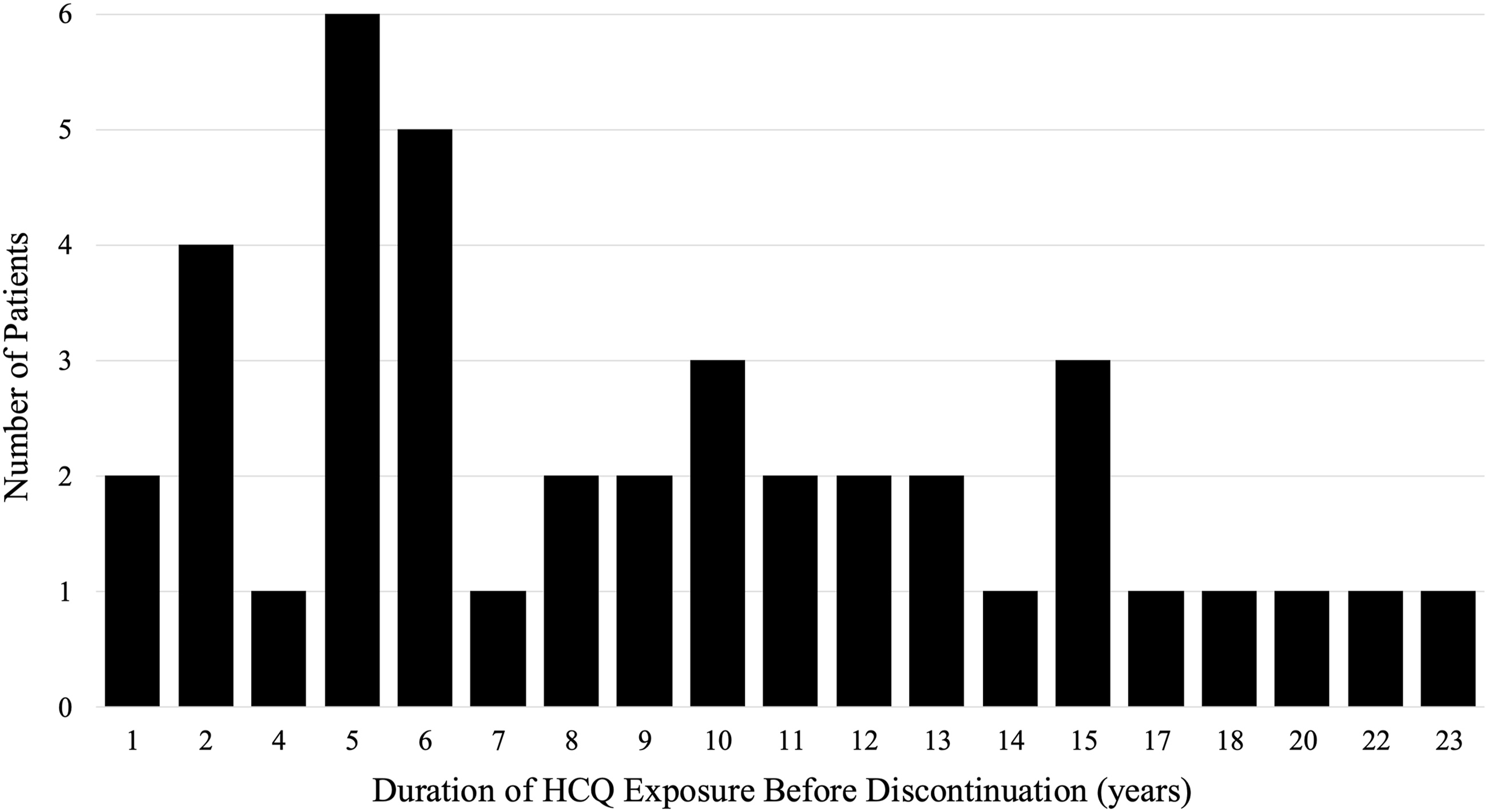
Demographic factors, HCQ dosages, lupus manifestations, comorbidities, disease activity, disease damage and current (last visit) and cumulative (at any time) pharmacologic therapy in SLE patients with and without HCQ-induced retinopathy.
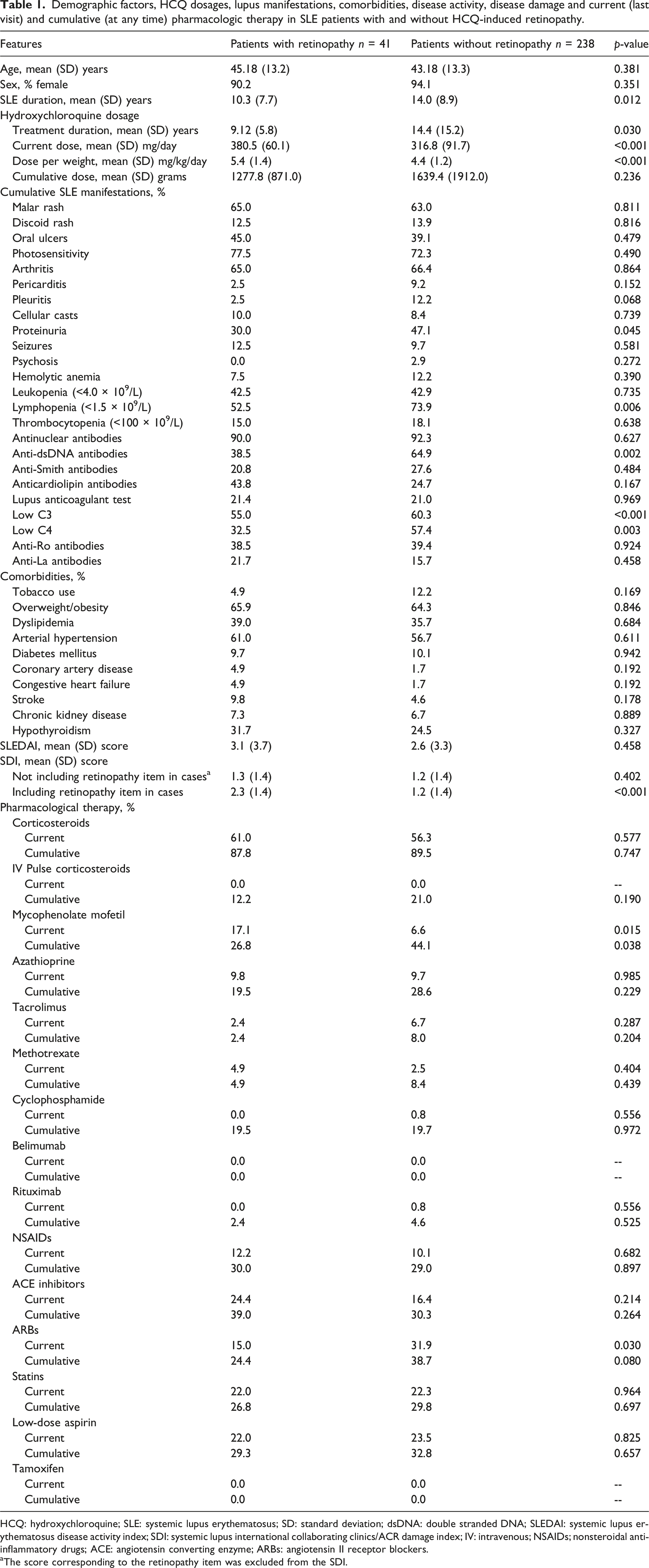
HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus; SD: standard deviation; dsDNA: double stranded DNA; SLEDAI: systemic lupus erythematosus disease activity index; SDI: systemic lupus international collaborating clinics/ACR damage index; IV: intravenous; NSAIDs; nonsteroidal anti-inflammatory drugs; ACE: angiotensin converting enzyme; ARBs: angiotensin II receptor blockers.
aThe score corresponding to the retinopathy item was excluded from the SDI.
Logistic regression analysis of factors associated with HCQ-induced retinopathy in SLE patients.
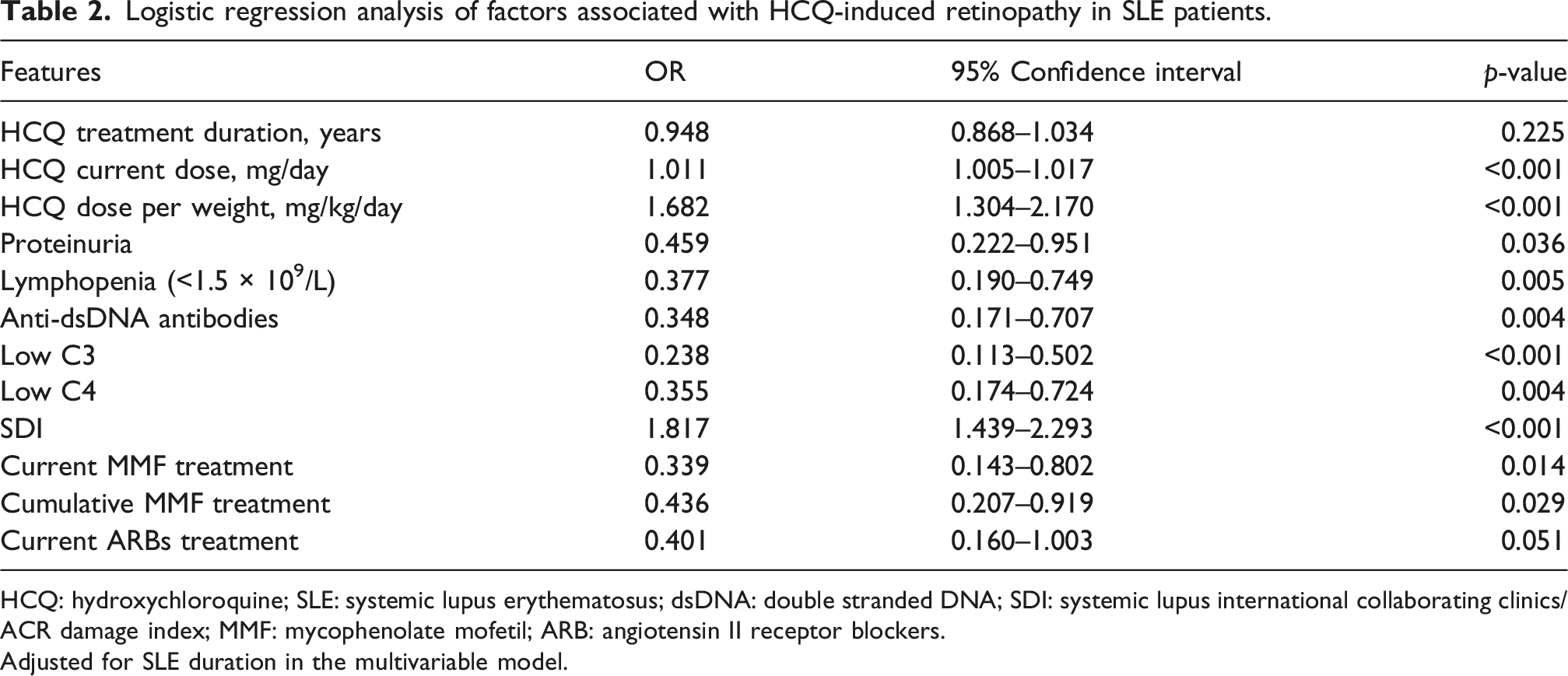
HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus; dsDNA: double stranded DNA; SDI: systemic lupus international collaborating clinics/ACR damage index; MMF: mycophenolate mofetil; ARB: angiotensin II receptor blockers.
Adjusted for SLE duration in the multivariable model.
Demographic factors, HCQ dosages, lupus manifestations, comorbidities, disease activity, and disease damage and current (last visit) and cumulative (at any time) pharmacologic therapy in SLE patients with early-onset (≤5 years) and late-onset (>5 years) HCQ-induced retinopathy.
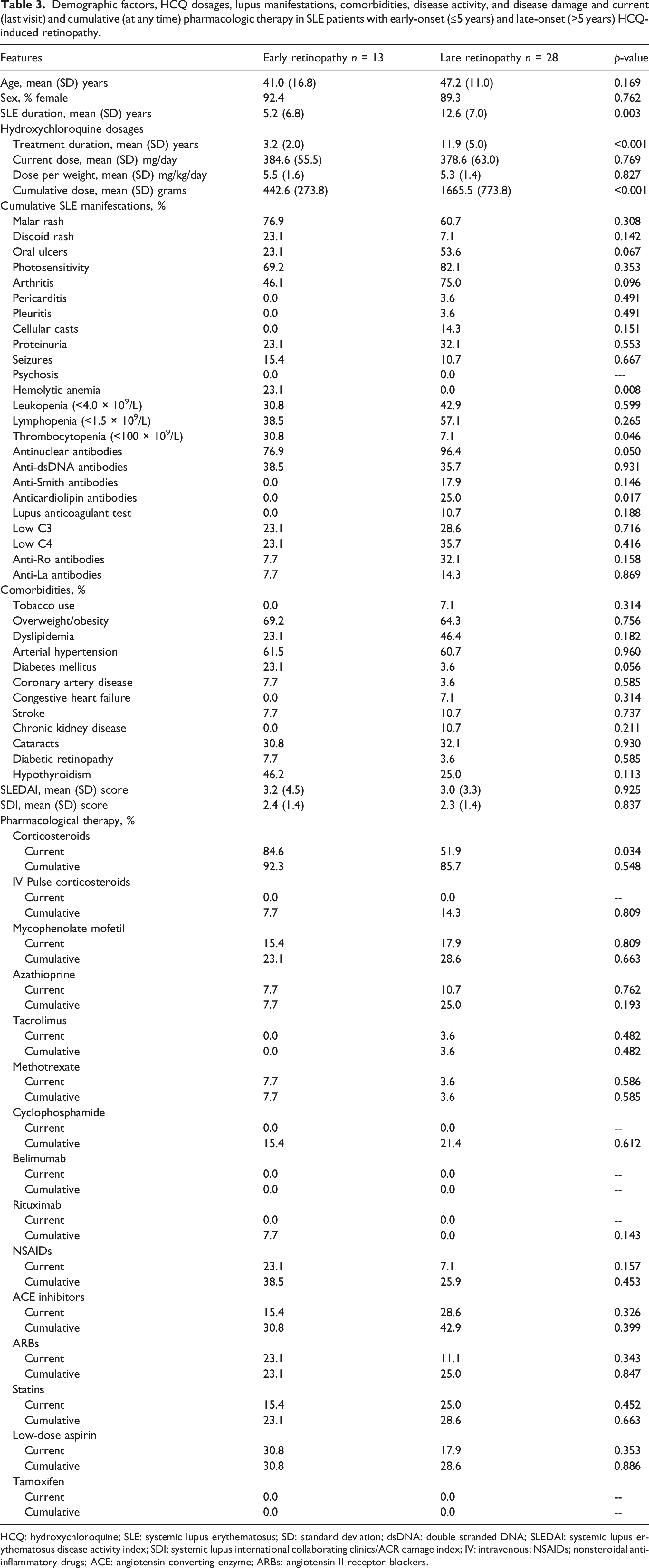
HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus; SD: standard deviation; dsDNA: double stranded DNA; SLEDAI: systemic lupus erythematosus disease activity index; SDI: systemic lupus international collaborating clinics/ACR damage index; IV: intravenous; NSAIDs; nonsteroidal anti-inflammatory drugs; ACE: angiotensin converting enzyme; ARBs: angiotensin II receptor blockers.
Logistic regression analysis of factors associated with early-onset HCQ-induced retinopathy in SLE patients.
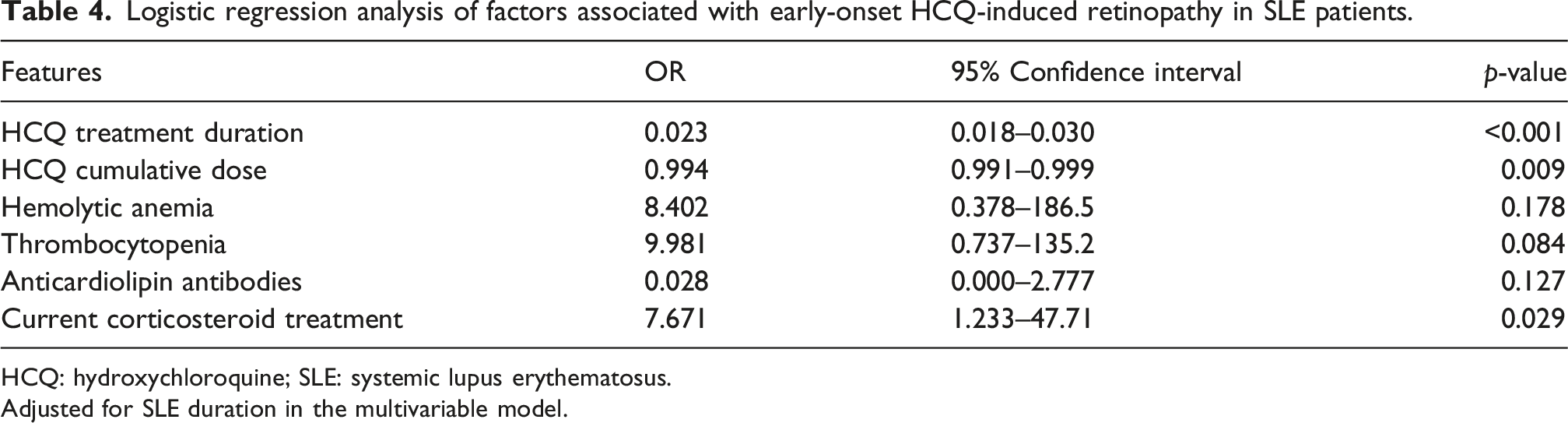
HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus.
Adjusted for SLE duration in the multivariable model.
Discussion
This study provides important insights into HCQ–induced retinopathy in a Puerto Rican population of patients with SLE, demonstrating both a relatively high overall prevalence and a notable frequency of early-onset HCQ-induced retinopathy. In our cohort of 279 patients treated with HCQ, nearly 15% developed HCQ-associated retinopathy. The prevalence observed in our population is higher than that reported in several previous studies. For example, in a Canadian case–control study by Mukwikwi et al., which included 326 patients exposed to antimalarial drugs, 5.5% developed HCQ-induced retinopathy over a mean follow-up of 12.8 years. 11 This study included patients treated with both HCQ and chloroquine (CQ), although approximately 90% were receiving HCQ. Similarly, in a large cohort study conducted within the Kaiser Permanente Northern California system by Melles et al., HCQ retinopathy was identified in 2.4% of 3325 patients. 12 However, several methodological differences may partly explain the higher prevalence observed in our cohort. In the Kaiser Permanente study, retinopathy may have been underestimated among patients who initiated HCQ before the implementation of screening with OCT, a more sensitive modality for detecting early HCQ-induced retinopathy than fundoscopy. 3 In addition, that cohort included patients with a variety of rheumatologic diseases rather than exclusively patients with SLE, which may further contribute to differences in the observed prevalence rates.
We confirmed that higher current daily and weight-adjusted HCQ doses are associated with an increased risk of HCQ-induced retinopathy. 2 However, in our cohort, 36.5% of retinopathy cases occurred in patients receiving an HCQ dose of ≤5 mg/kg/day based on actual body weight. This finding is particularly noteworthy, also considering that the mean daily dose in our population was 5.4 mg/kg/day, which closely approximates the 2016 recommendations of the American Academy of Ophthalmology (AAO) that advise a maximum daily dose of ≤5.0 mg/kg/day based on actual body weight to reduce the risk of retinopathy. 3 It is important to note that some patients in our cohort initiated HCQ therapy under earlier AAO guidelines that recommended dosing up to 6.5 mg/kg/day based on ideal body weight, which may have contributed to higher cumulative exposure over time. In a cohort study by Melles et al., a progressively higher risk of retinopathy was observed across increasing hydroxychloroquine dose categories after 15 years of therapy, ranging from approximately 3% among patients receiving ≤5 mg/kg/day, to 11% among those receiving >5–6 mg/kg/day, and up to 22% among those receiving >6 mg/kg/day. 12 Similarly, in the case-control study by Mukwikwi et al., 12 of the 18 patients who developed retinopathy had average daily doses exceeding recommended limits. 11 In an Indian cohort study by Manoj et al., which included patients with various rheumatologic diseases including SLE, the mean daily HCQ dose among those who developed retinopathy was 5.7 ± 0.9 mg/kg/day based on actual body weight. 13 In contrast, the substantial proportion of retinopathy cases occurring within guideline-recommended dosing in our cohort suggests that dosing considered acceptable by current standards may not fully mitigate retinopathy risk in this population. This finding highlights the potential contribution of additional patient-specific or disease-related factors influencing susceptibility to HCQ-induced retinopathy.
The potential for confounding by indication may explain our finding of a higher prevalence of MMF use among patients without HCQ-induced retinopathy. This association likely reflects a greater burden of lupus nephritis within this subgroup, as MMF is a cornerstone therapy for renal involvement in SLE. 14 This interpretation is supported by the increased frequency of proteinuria, hypocomplementemia, and anti-dsDNA positivity, hallmarks of active nephritis. 1 These patterns suggest differences in disease phenotype and management rather than a protective effect of inflammatory activity itself. Patients with renal involvement typically undergo intensified immunosuppressive therapy, closer clinical monitoring, and more frequent HCQ dose adjustments, which may limit sustained high-dose exposure and enhance early toxicity detection. 15 In contrast, patients without major organ involvement may remain on higher HCQ doses for longer periods, increasing cumulative retinal exposure. Together, these findings suggest that treatment strategies and disease severity, particularly in the context of lupus nephritis, may indirectly influence the risk of HCQ-induced retinopathy rather than any pharmacologic interaction between MMF and HCQ. Consequently, the observed difference in MMF use should not be interpreted as evidence of a protective effect against HCQ-induced retinal toxicity, but rather as a reflection of underlying differences in disease manifestations and treatment indications between groups. Finally, the higher proportion of lymphopenia observed in our patients who did not develop HCQ-induced retinopathy probably reflects the bidirectional relationship between hematologic disease activity and immunosuppressive management in SLE. Lymphopenia is a common manifestation of active immune-mediated disease and often serves as an indication for intensified immunosuppressive therapy, particularly in patients with concurrent lupus nephritis and serologic activity. 16
Our study found that 31.7% of HCQ-induced retinopathy cases occurred in patients with a hydroxychloroquine exposure duration of ≤5 years. This higher proportion is notably greater than that reported in most previous studies. One possible explanation for this difference is the more intensive ophthalmologic surveillance in our cohort, as patients underwent annual ophthalmologic screening beginning immediately after initiation of HCQ therapy. This approach may have increased the detection of early or subclinical retinal abnormalities that could have been missed in cohorts following less frequent screening protocols. Another potential explanation is the higher cumulative exposure to HCQ doses in earlier treatment eras, as a significant proportion of our patients were treated under previous AAO guidelines that recommended dosing up to 6.5 mg/kg/day and different baseline and follow-up screening practices, in contrast to current recommendations. Furthermore, the earliest retinopathy in our population occurred less than a year after starting HCQ therapy. In contrast, the Canadian study by Mukwikwi et al. had no cases detected in the first 5 years of therapy, and the minimum number of years of exposure to HCQ before retinopathy developed was 8 years. 11 A shorter duration of treatment before toxicity was detected in the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort by Almeida-Brasil et al., with the earliest case being detected after 4 years of HCQ initiation. 17 Our findings challenge the AAO guideline recommending annual screening for retinopathy to begin after 5 years of HCQ use for patients on acceptable doses and without significant risk factors, like renal disease. However, in our study, the prevalence of chronic kidney disease did not differ significantly between patients with early-onset and those with late-onset HCQ-induced retinopathy. Our data suggest that a significant proportion of retinopathy can manifest earlier, underscoring the potential for early-onset toxicity in this population. The contrasts between our results and those seen in other studies highlight the need to consider ethnic variations, particularly the possibility that genetic predispositions or unique metabolic profiles in Puerto Ricans may contribute to the earlier onset of HCQ toxicity.
A higher proportion of patients with early HCQ-induced retinopathy had greater current corticosteroid exposure at the time of HCQ discontinuation. This observation was further supported by adjusted analyses, in which corticosteroid use was identified as an independent factor associated with early-onset retinopathy. This association may reflect the higher disease activity and greater corticosteroid requirements typically observed during the early years of SLE, rather than a direct effect of corticosteroid therapy itself. 18 Although a higher proportion of hemolytic anemia and thrombocytopenia was observed among patients with early HCQ-induced retinopathy in the bivariate analyses, these associations did not reach statistical significance in the regression models.
The relatively elevated frequency of HCQ-induced retinopathy, including early-onset retinopathy, in our population could reflect underlying pharmacogenomic and pharmacokinetic variability. HCQ-induced retinopathy is characterized by progressive damage to the outer retina, particularly the photoreceptors and retinal pigment epithelium (RPE). 4 The pathophysiology involves the accumulation of HCQ in the RPE, likely due to its binding to melanin, which may concentrate the drug and prolong its toxic effects. 4 Pharmacogenomic and pharmacokinetic genetic variants, particularly in CYP2D6, CYP2C8, and CYP3A4/5, can influence HCQ metabolism and systemic exposure, potentially affecting toxicity risk. 19 Poor metabolizer phenotypes may result in higher drug concentrations and increased risk of retinopathy, while ultra-rapid metabolizers may have lower exposure and reduced efficacy. 20 Ethnic differences in the frequency of these alleles are well documented. For example, CYP2D6*10 is more common in East Asians, while CYP2D6*4 is prevalent in Europeans. Latin American populations, including Puerto Ricans, are highly admixed, with variable frequencies of CYP2D6, CYP2C8, and CYP3A4/5 alleles depending on the proportions of European, African, and Amerindian ancestry.21,22 CYP2D6*31 is a nonfunctional allelic variant that results in a poor metabolizer phenotype for CYP2D6 substrates, including HCQ. In Puerto Rican populations, the CYP2D6*31 allele is present at a frequency of approximately 2%, which is higher than in other major ancestral groups such as North American Caucasians and African Americans, where it is absent. 23 This allele has been directly associated with poor metabolism of CYP2D6 substrates in vivo, as demonstrated by increased parent drug concentrations and reduced metabolite formation. 23 On the other hand, the CYP3A5*3 allele (rs776746), which results in a nonfunctional enzyme due to aberrant splicing, has a high minor allele frequency (MAF ≈76.4%) in the Puerto Rican population, which was similar to frequencies in the general Hispanic group of undetermined ethnicities. 24 Comprehensive, population-specific data on the Puerto Rican population’s pharmacogenomic and pharmacokinetic genetic variants remain scarce. Puerto Ricans’ diverse genetic ancestry significantly affects allele frequencies and drug responses; neglecting this may lead to misestimation of pharmacogenetic effects.
This study has some limitations that should be acknowledged. First, its retrospective observational design introduces inherent constraints. Second, the relatively small sample size and limited number of outcome events in the subgroup analyses comparing patients with early versus late HCQ-induced retinopathy may have increased the risk of overfitting in the multivariable models, potentially affecting the stability, precision, and generalizability of the observed associations. Consequently, these findings should be interpreted with caution and warrant confirmation in larger, adequately powered studies. Third, we assumed adherence to prescribed HCQ dosing; however, medication compliance could not be objectively verified, which may have affected estimates of cumulative exposure. Fourth, genetic susceptibility and pharmacogenomic variability were not assessed and may contribute to individual differences in the risk of HCQ-induced retinal toxicity. Finally, because the study period spanned from December 1987 to July 2024, our study may have introduced selection bias, as patients with HCQ-induced retinopathy during the earlier years of the study were diagnosed primarily by fundus examination. Therefore, changes and advances in screening modalities over time may have influenced detection rates. For example, subclinical or early retinal changes in patients who did not discontinue treatment may not have been detected. In fact, 15 patients were diagnosed by fundus examination and 26 by OCT. Although stratification by treatment era would have been valuable, the number of patients within each subgroup was too small to allow meaningful comparisons or adequately powered statistical analyses. Despite this limitation, standardized AAO criteria were consistently applied, and ophthalmologic follow-up was even more rigorous than current AAO recommendations, as all patients underwent baseline examination and annual follow-up after initiating HCQ therapy, rather than baseline examination followed by the first screening at 5 years, as recommended by the AAO guidelines.
In conclusion, the findings of this study have important implications for clinical practice, particularly regarding the monitoring of HCQ-induced retinopathy in the Puerto Rican population. Nearly 30% of HCQ-induced retinopathy cases occurred in patients treated for ≤5 years, suggesting that earlier and more frequent retinal screening, potentially beginning at the initiation of therapy, may be warranted. Additionally, 36.5% of patients who developed retinopathy were receiving HCQ at or below the AAO-recommended maximum daily dose of ≤5.0 mg/kg/day, indicating that even guideline-recommended dosing may not fully lessen the risk of HCQ-induced retinopathy in this population. Although higher daily and weight-adjusted doses were associated with increased risk, a substantial proportion of cases occurred within AAO guideline-recommended dosing ranges. This observation should be interpreted cautiously, as it likely reflects the interplay of multiple factors, including cumulative exposure, disease characteristics, and individual susceptibility, rather than limitations of current recommendations alone. Further studies are needed to better define risk stratification across diverse populations and to optimize screening strategies within existing guideline frameworks.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.