
Abstract
Ordinal responses are common in clinical studies. Although the proportional odds model is a popular option for analyzing ordered-categorical data, it cannot control the type I error rate when the proportional odds assumption fails to hold. The latent Weibull model was recently shown to be a superior candidate for modeling ordinal data, with remarkably better performance than the latent normal model when the data are highly skewed. In clinical trials with ordinal responses, a balanced design is common, with equal sample allocation for each treatment. However, a more ethical approach is to adopt a response-adaptive allocation scheme in which more patients receive the better treatment. In this paper, we propose the use of the doubly adaptive biased coin design to generate treatment allocations that benefit the trial participants. The proposed treatment allocation scheme not only allows more patients to receive the better treatment, it also maintains compatible test power for the comparison of treatment efficiencies. A clinical example is used to illustrate the proposed procedure.
Keywords
1 Introduction
In clinical trials, ordered categorical response is a familiar type of patient outcome. For example, a study of various anti-malarial drugs by Youdom et al. 1 used the classification of clinical outcomes suggested by the World Health Organization. 2 The measure is an ordinal scale, including adequate clinical and parasitological response, late parasitological failure, late clinical failure, and early treatment failure. Another study that assessed various treatments for depression distinguished patients according to the severity of their depression based on a patient health questionnaire. 3 The possible categories are mild depression, moderate depression, moderately severe depression, and severe depression.
For comparisons of treatments with ordinal outcomes, the proportional odds model has long been a popular choice for testing the equality of treatment efficacy.4,5 However, as demonstrated by Lu et al., 6 the proportional odds model fails to control the type I error rate when the proportional odds assumption is invalid. A better alternative is to use the latent variable model, which conceptualizes ordinal responses as manifestations of underlying continuous variables. The latent variable model has long been an attractive technique for analyzing ordinal responses.7–9 Poon 10 proposed the use of the latent normal model to compare two treatments. Her method was extended to pairwise comparisons 11 and multiple comparisons with a control6,12 when more than two treatments are available. Although the latent normal model shows satisfactory performance and can control the type I error rate in ordinary cases, it also suffers from the type I error rate inflation problem when the degree of skewness differs greatly for data from various treatments. Lu et al.13,14 recently found that the latent Weibull model is a superb candidate to compare treatments with highly skewed ordinal outcomes. Testing procedures have been developed with very competitive test power even when the data are not skewed. The latent Weibull model appears to be superior to the aforementioned procedures in comparing treatments with ordered categorical outcomes.
In clinical studies, the traditional option for treatment allocation is a balanced design by which equal numbers of patients are assigned to each treatment, and trials with ordinal outcomes are no exception.15,16 However, during the patient recruitment period, incoming patients almost always arrive sequentially, which permits the use of a response-adaptive treatment allocation scheme. Response-adaptive treatment allocation procedures are able to incorporate information about the responses of previous patients amassed during the trial thus far and skew the probability of treatment assignment to favor the better treatment. 17 Hence, a response-adaptive design provides a desirable alternative to the popular balanced-design norm by reducing the number of patients who undergo the less effective treatment in clinical trials. 18
The primary objective of this paper is to introduce a response-adaptive treatment allocation scheme that can be applied to compare treatments with ordinal responses. Of the various types of available response-adaptive designs, the doubly adaptive biased coin design (DBCD) proposed by Hu and Zhang 19 has two important features. First, it enables the inclusion of pre-specified targets, such as the treatment of fewer patients with the inferior treatment. Second, the allocation scheme yields very competitive test power.
The layout of this paper is as follows. In Section 2, the latent Weibull model is outlined and the testing procedure to compare treatment efficacy is explained. In Section 3, the basic framework of response-adaptive design is given, including a discussion of the DBCD design. Under the DBCD framework, various allocation rules are given based on different objectives. In Section 4, a simulation study is used to demonstrate the benefits of the suggested design compared with the balanced design. In Section 5, a clinical study is redesigned to demonstrate the advantage of the DBCD design in practice. Finally, a few concluding remarks are given in Section 6.
2 Latent Weibull model
2.1 Clinical example
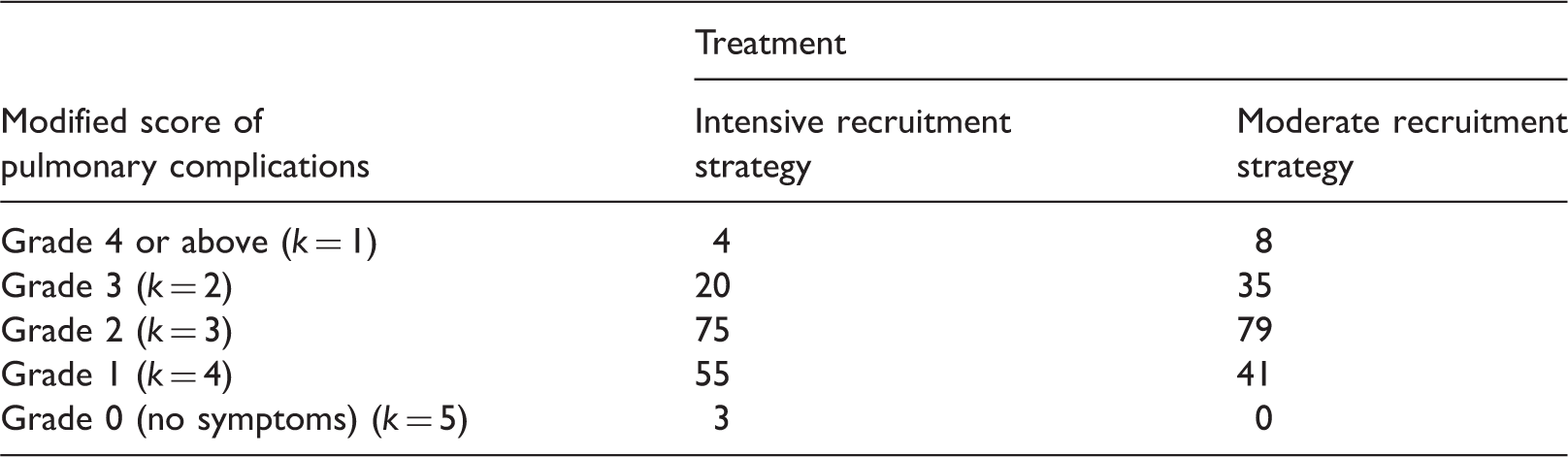
Severity of postoperative pulmonary complications with two recruitment strategies.
2.2 Model and parameter estimation
Assume the existence of two treatments in a clinical study with ordinal outcomes, similar to the aforementioned example. Let Y
i
be the ordinal response of treatment i, i = 1, 2, with possible values k, 
To provide a better model to cope with the problem of the inflated type I error rate for a wider spectrum of data environments, Lu et al.13,14 suggested the latent Weibull model. The Weibull distribution is a member of the log-location-scale distribution family, and its corresponding distribution in the location-scale family is the extreme value distribution.
23
Hence, the estimation procedures can easily be obtained by generalizing the estimation procedures that were previously derived from a model using the corresponding location-scale distribution.
13
Unlike the normal distribution, which is symmetric, the Weibull distribution has a very flexible distribution that can be applied to model data that are highly skewed. With the latent Weibull model, the distribution function of Z
i
is

Let n
i
patients undergo treatment i, i = 1, 2, and the total sample size, n, is therefore 

Let 
The entries
2.3 Comparison of treatments
For the latent Weibull model, the median of the latent Weibull distribution is a reasonable measure of the mean treatment efficacy because the Weibull distribution could be highly skewed. Let M
i
be the median of the underlying Weibull distribution 

To compare these two treatments, we test the null hypothesis

3 Response-adaptive design
3.1 Response-adaptive treatment allocation versus balanced design
Balanced design has turned out to be the most popular option to avoid subjective judgment and possible bias in treatment allocation in clinical studies, that is, an equal number of patients are assigned to each treatment regardless of differences in efficacy among the treatments. For trials with ordinal outcomes, balanced treatment allocation schemes also predominate in design protocols.20,24
Even though treatment randomization using the balanced design is widely adopted in clinical trials, response-adaptive randomization is becoming more acceptable. 25 The attractive feature of response-adaptive randomization is that the probabilities of treatment assignment can be shifted according to pre-determined objectives, such as lowering the number of patients who undergo the inferior treatment. In a response-adaptive randomization scheme, the patients are required to accrue sequentially, which enables the assessment of treatment efficacies with the data amassed at any given point in the trial. The usefulness of response-adaptive designs has recently been recognized by clinical researchers. For example, Berry et al. 26 proposed the use of response-adaptive randomization in a study of the Ebola virus, and Das and Lo 27 discussed the advantages of adaptive randomization in breast cancer trials.
Among the various classes of response-adaptive design, DBCD, which was first proposed by Eisele, 28 is considered to be superior to many other procedures.19,29,30 Desirable optimal criteria can be incorporated into the DBCD, and treatment allocations converge to the pre-specified targets. The mechanism to implement treatment randomization with DBCD is given in the following subsection. Note that the use of a response-adaptive design with ordinal responses is more difficult than its counterpart with continuous outcomes. This mainly happens because the response-adaptive design requires continuous estimation of the parameters, even during the early stages of a clinical study when the number of individuals recruited for the trial is still small and, therefore, the ordinal data may be quite skewed. Traditional estimation procedures do not work satisfactorily, but the latent Weibull model performs much better in terms of estimation and testing, even when the data are very skewed. Hence, with the use of the latent Weibull model, response-adaptive treatment randomization is a feasible treatment allocation scheme.
3.2 Treatment allocation scheme of DBCD
Assume that n patients are to be assigned to two treatments in a clinical study. At time t, q
DBCD treatment randomization scheme
The first n0 patients are allocated to the two treatments using restricted randomization to obtain an initial estimate of the parameters, For
In Stage 1, the parameters
Using the treatment allocation procedure in Hu and Zhang,
19
the allocation function for treatment 1 in the second step is

3.3 Allocation rules
With reference to the DBCD treatment randomization scheme, we must construct the target allocation rule ρ, proportion allocated to treatment 1, according to certain desired allocation objectives. Here, we examine several viable candidates.
Rule 1: Balanced design (ρ1). This is the most popular allocation rule in clinical studies. Under the DBCD framework
Rule 2: Maximize power (ρ2). As explained by Hu and Rosenberger,
29
the DBCD allocation rule to maximize test power for comparison of treatments 1 and 2 is equivalent to searching for a ρ function such that the variance Rule 3: Minimize failure (ρ3). An ethical allocation target is to reduce the number of patients who undergo the inferior intervention. Hence, with fixed test power, or equivalently with fixed Rule 4: Modified Rule 3 (ρ4). Rule 4 is a modification of Rule 3, with the median replaced by the standardized median to reduce the effects of extreme heterogeneity between the two treatments. Hence, the required minimization function is

4 Simulation study
4.1 Comparisons of allocation rules under the latent Weibull model
A simulation study was conducted to study the performance of the allocation rules given in Section 3. Data were generated from a Weibull distribution and classified into five ordered categories (K = 5). Other values of K were also used, although these results are not presented here because the major findings are similar.
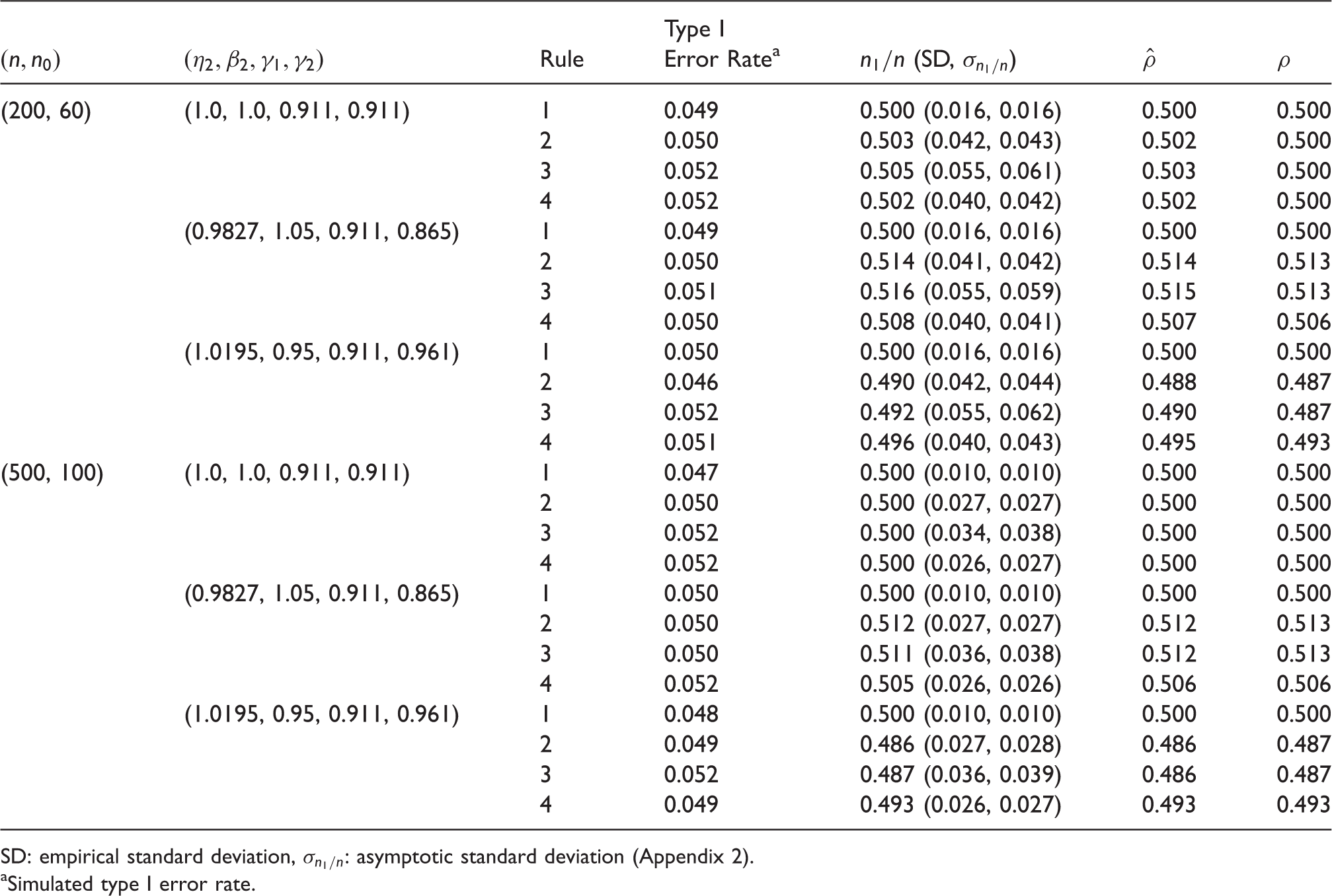
Without loss of generality, the parameters of the first treatment, η1 and β1, were fixed at 1. A variety of combinations of η2 and β2 were selected. The number of simulated replications was 10,000 for each parameter configuration. The total sample sizes n were selected to be 200 and 500. For Stage 1 of the DBCD procedure, we adopted restricted randomization, with the proportion of patients who undergo the better treatment (i.e. the treatment with a larger median), the simulated test power, and the average proportion of patients in the worst category, Simulated treatment allocation under H0 with SD: empirical standard deviation, Simulated type I error rate.
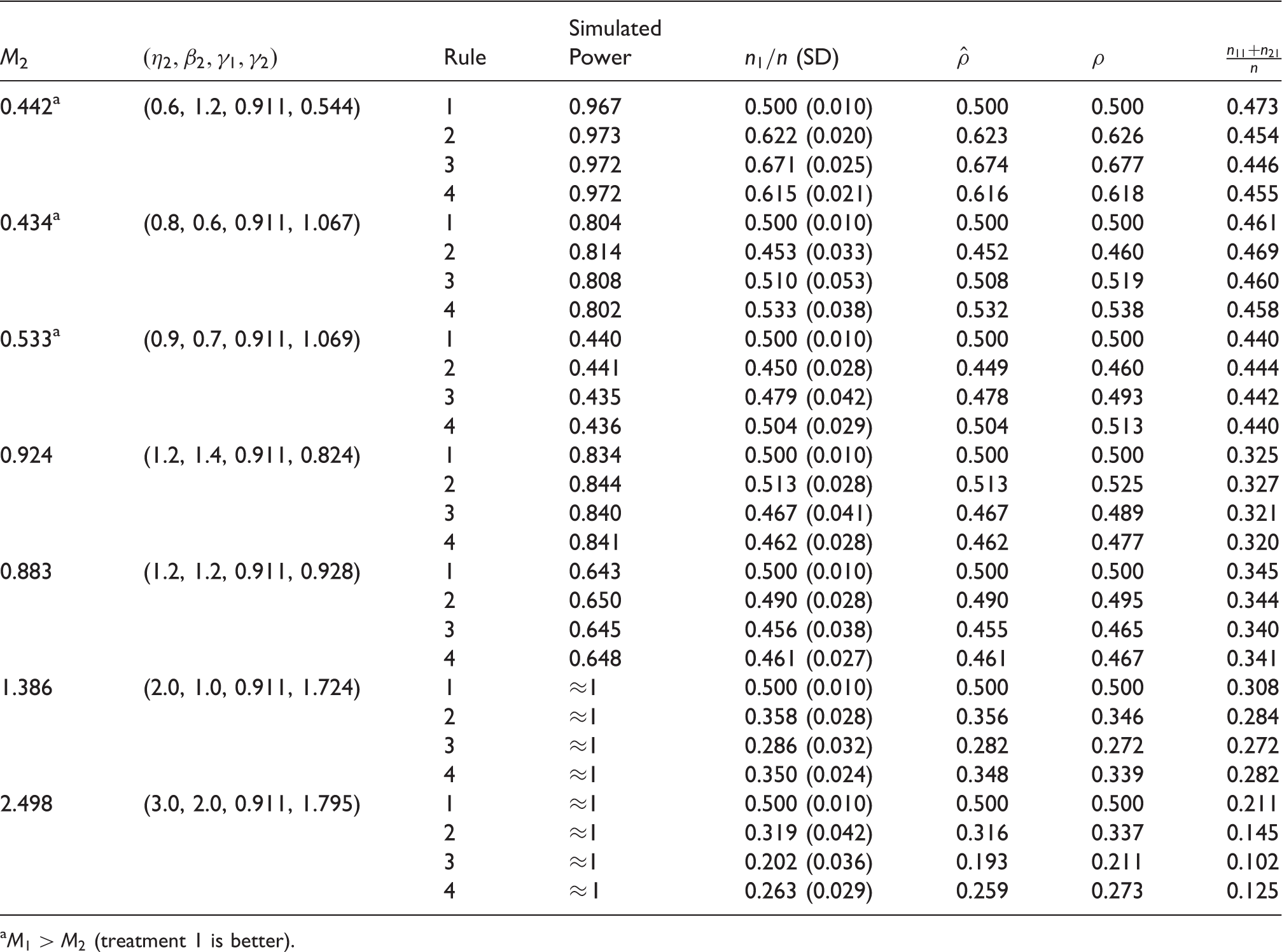
Proportion who underwent the better treatment. As demonstrated in Tables 3 and 4, Rules 3 and 4 are in general more capable of sending more patients to the better treatment, reflecting the inherent construction criteria of these two rules. Nevertheless, Rule 2, a function of γ, is constructed to maximize the test power. Hence, under Rule 2, it is possible that more patients receive the better or the worse treatment. For instance, in Table 3, when n = 200, Simulated treatment allocation under H1 (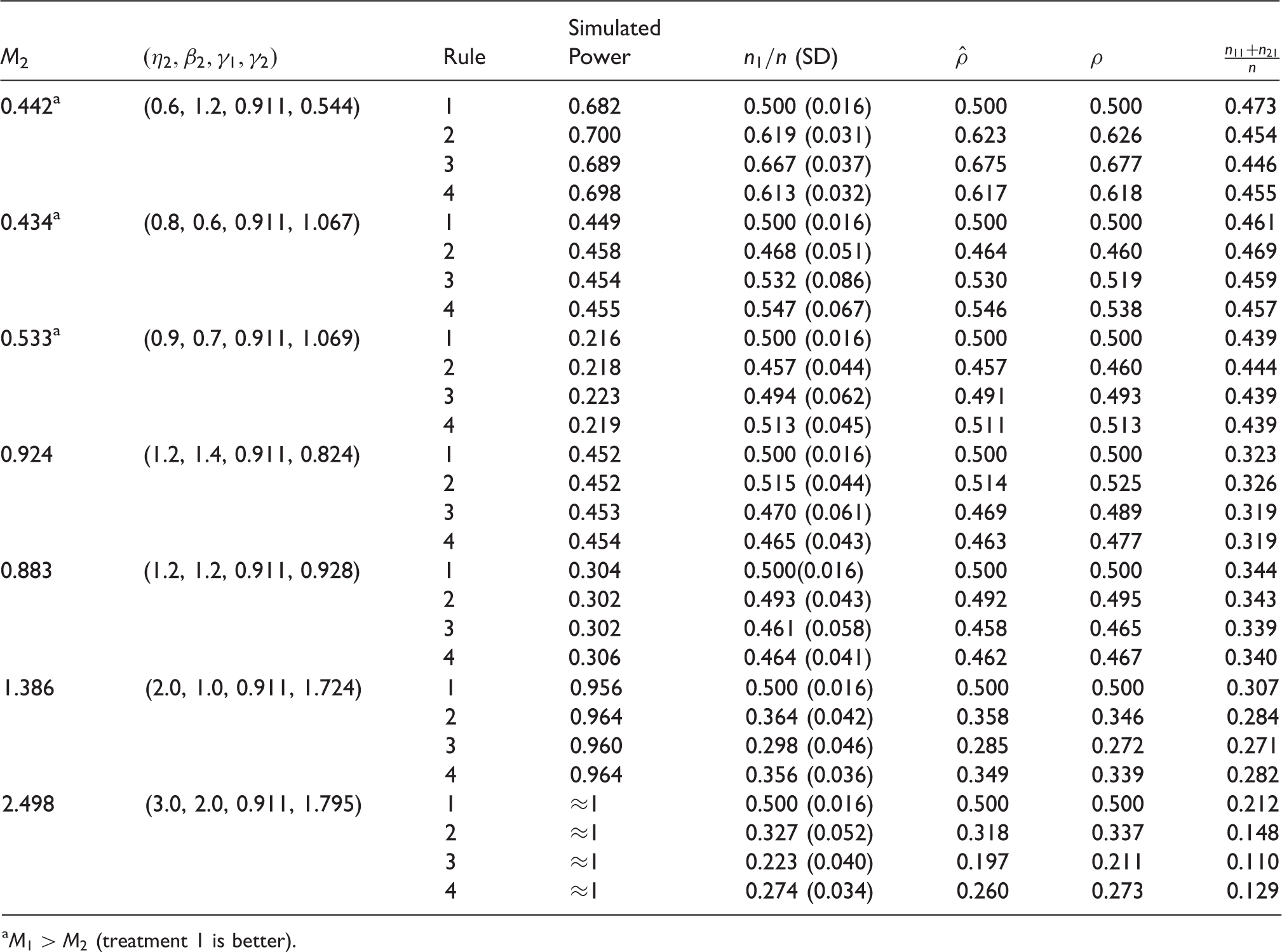
Test power. As mentioned previously, the DBCD allocation scheme yields very competitive test power and is consistent with our simulation results. As shown in Tables 3 and 4, the test powers of all four rules are very similar. Although Rule 2 always attains the greatest power, the test powers of Rules 3 and 4 are only slightly lower than that of Rule 2. There is no significant gain or loss among the various choices of allocation rules.
Equal efficacy (under the null). When the two treatments have equivalent medians (refer to Table 2), all allocation rules can send roughly half the patients to each treatment, as expected. Furthermore, the simulated type I error rates are all close to the pre-specified level, 0.05.
Sample size n. First, for the simulated power, when the sample size is 500 (Table 4), the simulated test power is much greater than that when sample size is 200 (Table 3). Furthermore, the allocation proportion
Standard deviation of allocation proportion (
Average proportion of patients in the worst category,
Tuning parameter τ. For the tabulated results, the value of τ is set to 2. However, other values of τ, such as 3 and 4, were also adopted. However, with no substantial differences in terms of the general features of the findings, the results are omitted.
In summary, although a balanced design is a popular approach in clinical studies, it is not a desirable treatment randomization scheme because it allows too many patients to undergo the inferior treatment when the efficacy of one of the treatments is much higher. Rule 4 is the better choice among the four allocation schemes because it has four advantages. First, it can allocate more patients to the better treatment and reduce the number of patients in the worst category. Second, the allocation of Rule 4 is more stable when the variances of two treatments differ substantially (i.e. very different values of γ1 and γ2). Third, as compared to Rule 3, Rule 4 consistently has a smaller standard deviation for the allocation proportion. Fourth, it attains a level of test power that is very competitive when compared to the other rules.
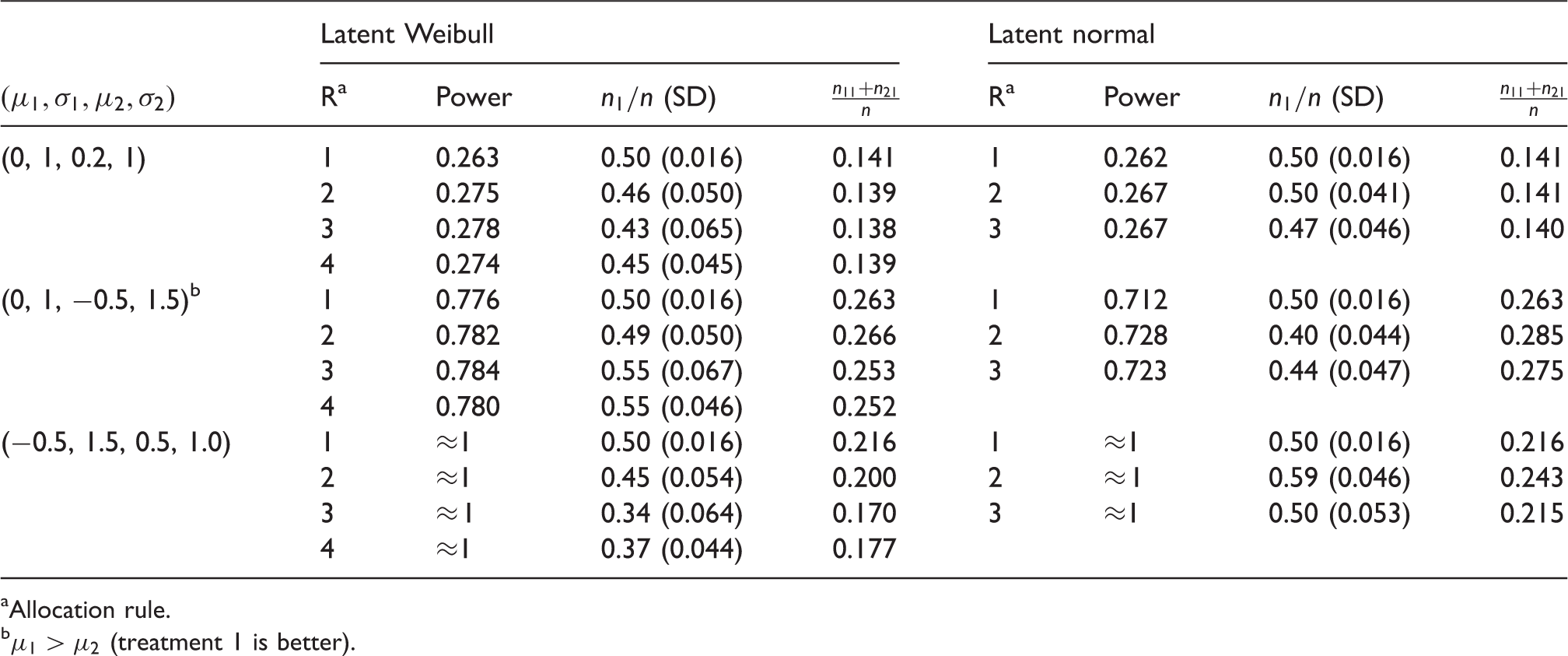
4.2 Comparisons of latent Weibull and latent normal models
In addition to the latent Weibull model, the latent normal model is a viable option for treatment comparisons when the responses are categorical. 6 As indicated by Lu et al., 13 the latent normal model is able to serve as an appropriate inference tool when the data are not highly skewed. Hence, the rest of this section is devoted to comparing the latent normal model and the latent Weibull model with reference to their comparative performance in treatment allocation.
According to Model (1), assume that Z
i
has a normal distribution with distribution function 
Parallel to the development of the allocation rules using the latent Weibull model, the allocation rules under the latent normal model are given in the following:
Rule 1: Balanced design ( Rule 2: Maximize power ( Rule 3: Minimize failure (

For the simulation study, data are generated from normal distributions with threshold fixed at
Simulated treatment allocation under H1 (
Comparison between latent normal and latent Weibull models in treatment allocation (
Allocation rule.
The major findings are summarized in the following:
When treatment means are similar, When the variances of the treatments are different, the findings reveal the superiority of the latent Weibull model, especially when the treatment means are very different. With reference to the latent normal model, the response-adaptive rules are highly influenced by the variance of the data and undesirably sending more patients to the inferior treatments in most cases. Furthermore, as compared to the allocation rules using the latent Weibull model, the proportion of patients in the worst category is much higher. For example,
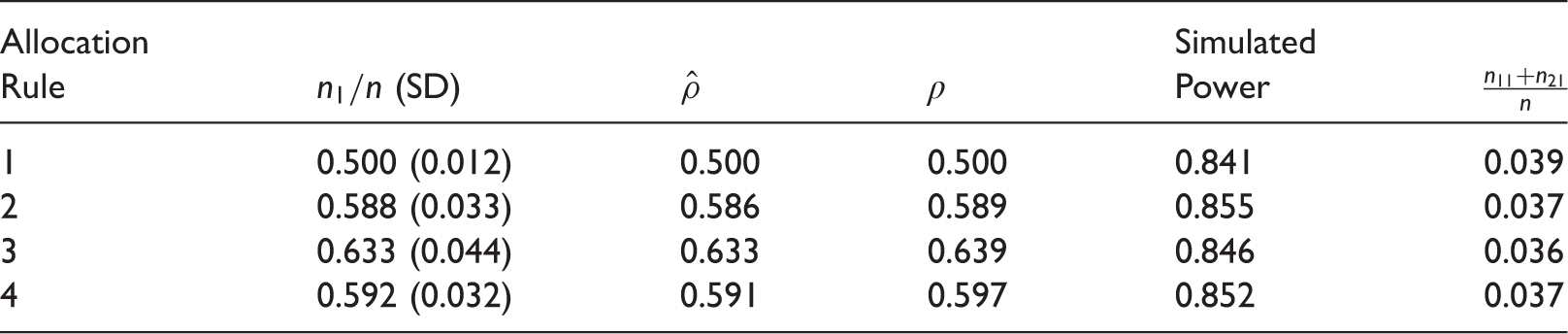
5 Clinical example
To demonstrate the advantages of response adaptive treatment allocation procedures, the clinical trial given in Section 2.1 has been redesigned to demonstrate the practical advantages of the proposed treatment randomization scheme. A simulation study is carried out using the response-adaptive treatment allocation scheme. The parameters for the simulation are estimated using the data collected in a clinical trial. In this example, the estimates of the parameters M1 and γ1 for treatment 1 (intensive recruitment strategy) are 0.857 and 1.031, respectively. For treatment 2 (moderate recruitment strategy), the estimates of the parameters M2 and γ2 are 0.562 and 0.778, respectively. The corresponding threshold estimates are 0.038, 0.235, 1.173, and 4.670, respectively. Moreover, the statistic for testing equal treatment efficacies is −2.960, and the corresponding p-value is 0.003, which is strong evidence against the null hypothesis, which indicates that intensive recruitment strategy can effectively reduce postoperative pulmonary complications.
Comparison of allocation rules for the clinical example (
6 Conclusions
The purpose of this study is to generate useful and pragmatic treatment allocation randomization schemes that outperform the conventional balanced design option for ordinal outcomes. For the comparison of the efficacies of two treatments, we show that a response-adaptive treatment allocation scheme is more ethical because it allows more patients to undergo the better treatment. In addition, each of the discussed allocation procedures has very similar test power. Among the various allocation rules introduced in this paper, Rule 4 appears to be the best candidate because it not only reduces the number of patients who receive the inferior treatment but it is also more robust to the differences between the standard errors of the median estimators of the two treatments. Hence, Rule 4 is the recommended treatment allocation scheme.
The latent Weibull model is an important component in the formulation of the proposed treatment allocation scheme. This is the first attempt in the literature to have applied the latent Weibull model for the derivation of response-adaptive treatment allocation schemes for ordinal responses. The allocation rules are derived using very general basic principles in DBCD. The asymptotic variance of the allocation proportion is also provided. The comparative study between the latent Weibull model and the latent normal model has illustrated the ethical advantage of the former with respect to proportion of patients being treated by the better treatment and the proportion of patients in the worst category. The latent Weibull model provides a much better estimation procedure than other comparable models, especially during the early stages of the treatment randomization process, when the number of observed outcomes is still small, thus increasing the likelihood of obtaining a very skewed distribution. In this paper, the randomization procedure is restricted to two treatments, and an exploration of response-adaptive randomization schemes for clinical trials with multiple treatments would be an interesting project.
Footnotes
Acknowledgements
We are grateful to the referees for many valuable suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lu’s research was supported by the project of the National Social Science Foundation of China (no. 15BTJ016). The research of Poon and Cheung was supported by the Research Grants Council of the Hong Kong Special Administrative Region (CUHK14301118) and a direct grant from The Chinese University of Hong Kong.