
Abstract
Parallel design and crossover design are two of the most frequently used designs for studying drug-gene interactions. Due to the concerns of statistical power and ethics, it is often more prudent to use the crossover design while allowing the patients to have choices of not switching the treatment if the first stage treatment is effective. This complicates the calculation of the required sample size to achieve pre-specified statistical power. We propose a method to determine the required sample size with a closed-form formula. The proposed approach is applied to determine the sample size of an adaptive crossover trial in studying gene-drug interaction in treating atrial fibrillation, the most common cardiac arrhythmia in clinical practice. Our simulation study confirms the power achieved by the sample size determined using the proposed approach. Issues related to the adaptive crossover trial are also discussed and practical guidelines are provided.
Introduction
The study of gene-drug interactions is important for the development of personalized medicine.1,2 The clinic Pharmacogenomic approach has been increasingly implemented3–5 in cancer treatment, 6 in heart health,7,8 and in treating and managing chronic diseases. 9 Randomized trials to determine gene-drug interactions clinically manifested have been frequently performed to generate knowledge on the interactions. To guide the success of such clinical trials, an important consideration is the sample size required for detecting the interactions with good statistical power. The sample size and power can be substantially affected by the study designs in addition to the genetic variation among the patient population.
A simple design for studying the interactions is the parallel design where patients are randomized to receive different treatments. 10 This design is simple both in implementation and in statistical analysis of the treatment effects. However, it is not as efficient as the crossover design11–13 where patients are randomized to receive one treatment and later switch to another treatment. The crossover design is more powerful in detecting the interactions with the same sample size as the parallel design. The former is however limited by the possible carry-over effect that may confound the treatment effect evaluation. When such effects can be well controlled in a trial, it is often favored over the parallel design. A second issue is the ethical concern of switching from a treatment that is efficacious to one that may not be effective. To address such issues, an adaptive crossover design that leaves the option to not switch when the first treatment is deemed effective may be more attractive. 14 The adaptive crossover design can be more powerful than the parallel design and addresses the ethical concern. However, it is less powerful than the crossover design and requires a sample size calculation adjusting for the adaptive nature of the trial to maintain the same statistical power for detecting gene-drug interactions.
The sample size determination for the parallel design and the crossover design have been well documented respectively in the literature, e.g., Jones and Kenward, 12 Chow et al., 10 Siyasinghe and Sooriyarachchi. 13 As far as we are aware, the sample size requirement for detecting the gene-drug interaction for the adaptive crossover design has not been systematically examined. A related but different design termed the dynamic treatment regime15–17 has been proposed in the literature. The sample size calculation for the dynamic treatment regime has been studied by many authors in different scenarios.16,18,19 However, as pointed out by Murphy, 16 the dynamic treatment regime serves a different purpose and the sample size calculation is different from the adaptive design.
In this article, we examine in detail the adaptive crossover design for studying gene-drug interactions and propose a sample size determination approach to achieve the require power. We compare the efficiency of the adaptive crossover design with the parallel design and the crossover design in terms of their power achieved with the same sample sizes. We also discuss analytical issues that may be encountered in such a design and provide guidelines on when such a design may be used.
Designs for studying gene-drug interaction
Parallel design for studying gene-drug interaction
The parallel design is the simplest one where subjects are randomized to receive the treatment drug A or drug B for the two genotypes: Risk allele (R) and wild type (W). Table 1 lists the design and outcome model for the parallel randomized trial. The objective of the study is to test the gene-drug interactions. The hypothesis to be tested is

Parallel design and the outcome model.
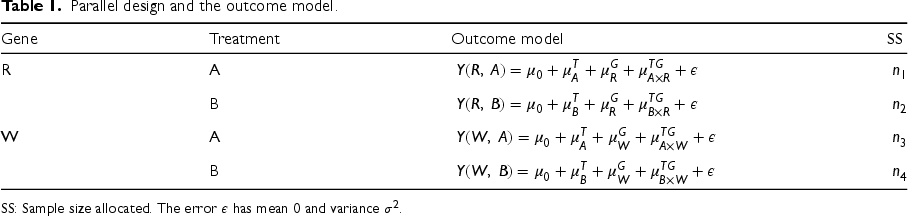
SS: Sample size allocated. The error
The crossover design randomly assigns patients to treatment drug A for a period of time and then switches to treatment drug B possibly after a washout period, or alternatively to treatment drug B for a period of time and then switches to treatment drug A after a washout period. Table 2 lists the design and outcome models for the two outcomes for each patient. The objective of the study is again to test the gene-drug interaction, i.e., to test the hypothesis in (1).
Adaptive design for studying gene-drug interaction
The parallel randomized design is simple and gives rise to straightforward treatment effects estimates. On the other hand, the crossover design is more efficient in general. In practice, however, if the first stage treatment is effective, patients or doctors may choose to not switch the treatment. In this case, the crossover design is not completely executed. Table 3 lists the possible treatment scenarios under such a situation.
Crossover design and the outcome models.
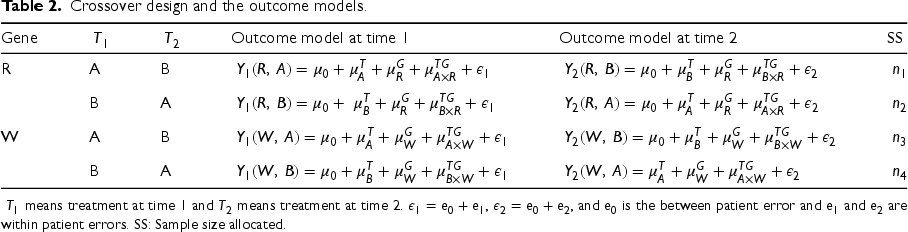
Crossover design and the outcome models.
Adaptive design and decision rule.
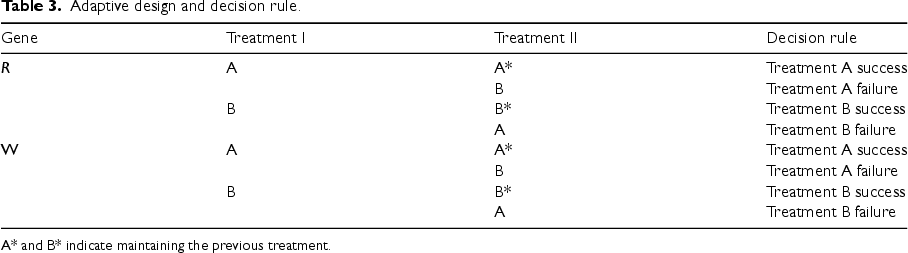
A* and B* indicate maintaining the previous treatment.
If we ignored the second stage trials, i.e., the crossover, the trial can still be analyzed as a parallel trial. One issue is that the trial may be substantially under-powered. For ethical consideration, we may design a study that allow patients to not switch if the first stage treatment is effective. The altered trial is often termed the adaptive crossover trial. We may use the second-stage data under reasonable conditions to increase the power, especially when the patients are difficult to recruit. Our main objective is to provide sample size and power calculation under the adaptive trial design for testing the gene-drug interaction.
Sample size requirement in the parallel design
In the parallel design, let the sample size be allocated as shown in Table 1. The mean difference for the risk allele genotype carriers under two different treatments,
















In the cross-over design, let the sample size allocation be as given in Table 2. Assume no residual effects nor treatment order effects. The mean difference for the risk allele genotype carriers under two different treatments,










Parallel part of the adaptive crossover design and the outcome model.
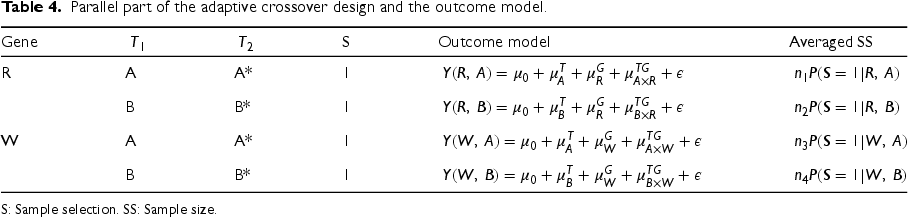
S: Sample selection. SS: Sample size.
For the adaptive design, the analysis ignoring the possible crossover part is simple for analysis. It can yield a causal effect under general conditions. However, the power can be low and the required sample size is large. Under stronger conditions, power can be gained by including all the data in the crossover part of the analysis. In the following, we use
The two-stage analysis approach poses substantial difficulty for the variance estimate due to the overlap sample issue of the two-stage analysis. We take the following alternative approach to simplify the analysis. The alternative approach separates patients without crossover from patients with crossover. The patients without crossover form a parallel design and patients with crossover form a crossover design, and the adaptive design is a mixture of the parallel design and the crossover design. Note that both the parallel design sample and the crossover design sample are biased samples with known sampling probability depending on the first-stage outcomes.
For the parallel design part shown in Table 4, the mean difference 





Crossover part of the adaptive crossover design and the outcome models.

S: Sample selection. SS: Sample size.
For the crossover design part shown in Table 5, the mean difference 


















Items 5–9 allow us to compute
Basic assumption for the trial
Atrial fibrillation (AF), the most common sustained cardiac arrhythmia in clinical practice, is associated with significant morbidity and increased mortality. Antiarrhythmic drugs (AADs) are commonly used to treat symptomatic AF. However, response in an individual patient is highly variable and AADs can be associated with adverse events. The limited success of AADs is related to heterogeneity of the electrical substrate, limited understanding of the underlying mechanisms, and our inability to predict responses to therapy in individual patients. Nonetheless, recent advances in our understanding of the genetic mechanisms of AF support the hypothesis that variability in response to antiarrhythmic therapy is modulated by common genetic variants associated with AF. Genetic approaches to AF have revealed that susceptibility to and response to therapy is modulated in part by the underlying genetic substrate. We showed that a common chromosome (chr) 4q25 single nucleotide polymorphism (SNP) (rs10033464) not only predicted successful control of AF symptoms but that patients who carried the risk allele responded better to Na + -channel (class I) than K + -channel blocker (class III) AADs. Our ongoing study is testing the hypothesis that a common chr4q25 SNP modulates response to AADs in patients with frequent symptomatic AF assessing burden as a measure of therapeutic efficacy. We propose a prospective randomized pharmacogenomic cross-over study that will determine if there is an interaction between a chr4q25 SNP and reduction in AF burden when patients are treated with flecainide (class I) versus sotalol (class III) AADs for 6-months each across race-ethnicities. The class III drug serves as a baseline and the class I drug is more effective for patients carrying the risk allele. Based on the pilot study, 20 the mean AF burden on flecainide (class I) was 20 ± 14% (SD). A mean reduction in AF burden of 10% in chr4q25 AF risk allele versus wild-type allele carriers may be clinically meaningful assuming that half of the patients will receive flecainide first and the other half sotalol first. As the minor allele frequency of rs10033464 is 12%, the ratio of carriers to non-carriers of the risk allele is 1:8. The variation of the AF burden over time within a patient is assumed to be 50% of the inter-patient variation.
Based on the assumptions, we can derive the following quantities for the sample size calculation.
Equal sample size is assumed for each treatment group, i.e., Intra-patient correlation is assumed to be
The formula for the total sample size is


When the intra-patient correlation is 

We need to obtain the success probability of each drug under different genotypes. This is estimated from the preliminary data on the treatment response rates. Table 6 lists the hypothetical response rates for different treatment and genotype combinations.



Response rates of treatment-gene combinations.

Simulation settings and results for
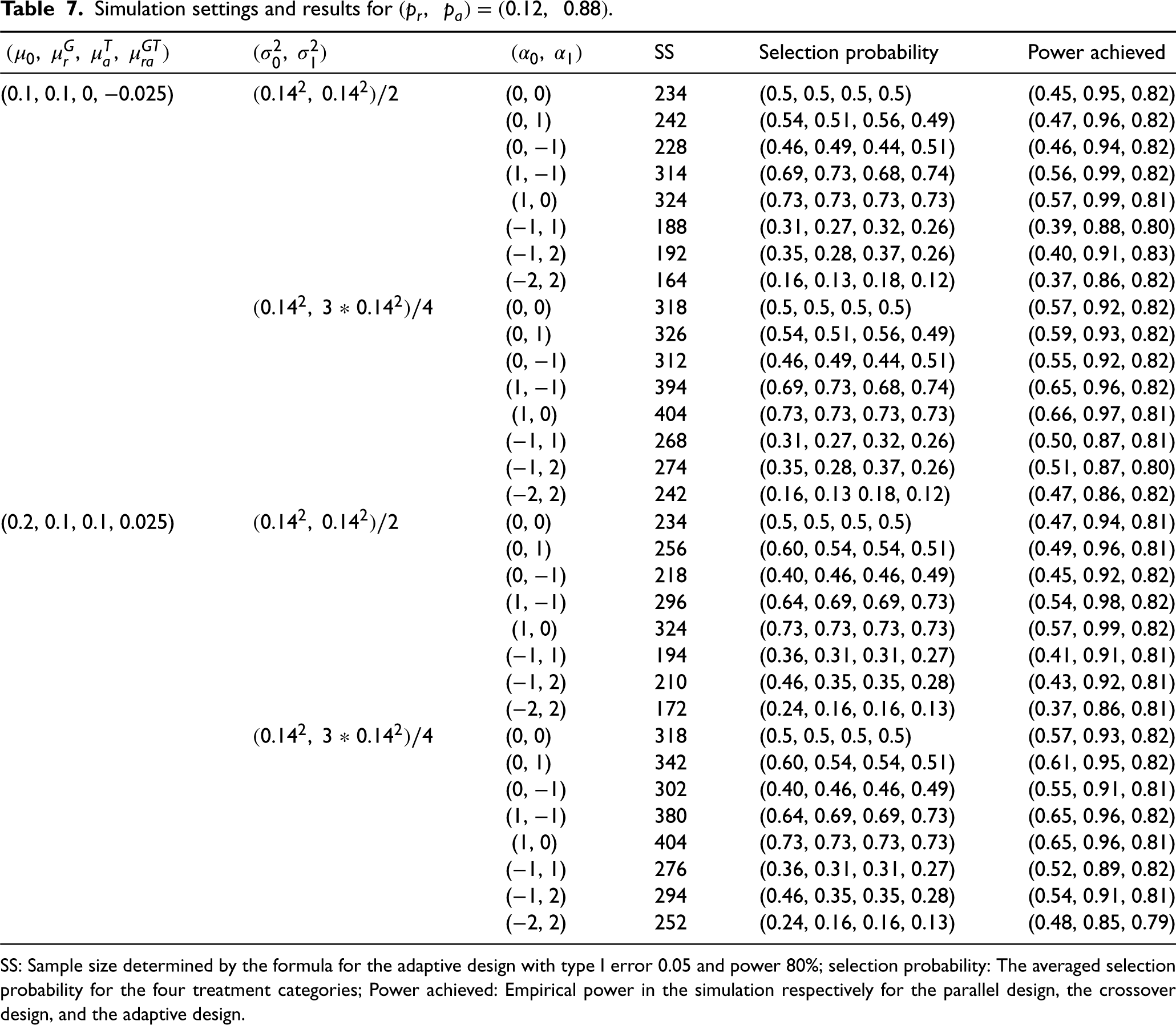
SS: Sample size determined by the formula for the adaptive design with type I error 0.05 and power 80%; selection probability: The averaged selection probability for the four treatment categories; Power achieved: Empirical power in the simulation respectively for the parallel design, the crossover design, and the adaptive design.
We perform a simulation study to examine the accuracy of the sample size determined by the approximate formula for practical use. The simulation generates data using the same models as given in Table 2 for the two outcomes. We assume that 
Assuming a two-sided test with type I error 0.05 and targeted power of 80%, the results of the simulation study are shown in Table 7. The simulation results are based on 5000 replicates of each scenario. From the table, we see that in almost all the cases, the actual power achieved based on the sample sizes determined by the formula is very close to the planned power for the adaptive design. The cross-over design is more powerful than the adaptive design, while the parallel design is less powerful than the adaptive design. The simulation results validate the reliability of the sample size determination formula.
The adaptive crossover trial provides patients the reassurance that should the initial AAD be efficacious in treating their AF, there is no necessity for the other class of ADD. While the design is less powerful than a crossover design, it is more powerful than the parallel trial in detecting a gene-drug interaction.
Depending on the success rate in the first stage trial, the sample size reduction can be substantial in comparison with that required by a parallel design. The adaptive design, however, requires stronger conditions to make the analysis valid. The primary reason is that patients making the treatment switch can be systematically different from patients who choose not to switch. For the analysis, we assume that the first-stage potential outcomes do not affect the potential outcomes in the second stage. The estimated interaction effect can be biased if the condition is violated.
The analysis of the trial can be fit into the longitudinal data framework through the likelihood estimation approach. Such an analysis framework can be more efficient than the multiple samples approach taken in this article. This means the required sample size can be smaller to achieve the same level of statistical power. However, the likelihood approach requires stronger modeling assumptions than those for the multiple-sample approach taken in this article. The latter is more robust against possible model misspecification.
The sample size formula is an approximation. When concerns about the impact of the approximation
Supplemental Material
sj-r-1-smm-10.1177_09622802231181704 - Supplemental material for Sample size determination for adaptive crossover trial in detecting gene-drug interactions
Supplemental material, sj-r-1-smm-10.1177_09622802231181704 for Sample size determination for adaptive crossover trial in detecting gene-drug interactions by Hua Yun Chen and Dawood Darbar in Statistical Methods in Medical Research
Supplemental Material
sj-r-2-smm-10.1177_09622802231181704 - Supplemental material for Sample size determination for adaptive crossover trial in detecting gene-drug interactions
Supplemental material, sj-r-2-smm-10.1177_09622802231181704 for Sample size determination for adaptive crossover trial in detecting gene-drug interactions by Hua Yun Chen and Dawood Darbar in Statistical Methods in Medical Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation for the National Institutes of Health (grant number 5R01HL148444).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.