
Abstract
Individualized treatment regimes (ITRs) represent decision-making frameworks that tailor treatment assignments to individual patient characteristics. The value function of an ITR quantifies the expected outcome under a counterfactual scenario in which such a treatment rule is applied. However, estimating optimal ITRs for survival data remains a significant challenge when outcomes are right-censored and only a subset of patients has complete outcome information due to time and cost constraints. To overcome this challenge, we formulate the problem within a semi-supervised learning framework and adopt an induced missingness perspective to model partially observed survival outcomes. We propose an imputation-based semi-supervised approach that is robust and adaptable to various imputation models. Specifically, we employ a flexible single-index kernel smoothing imputation technique to effectively utilize unlabeled data in multidimensional covariate settings. The proposed estimators for the parameters indexing the optimal ITRs are shown to be consistent and asymptotically normal. Moreover, semi-supervised estimation enhances efficiency by reducing asymptotic variance relative to supervised estimation. Numerical experiments on both simulated and real datasets demonstrate the superior performance of our proposed semi-supervised approach.
Keywords
Introduction
Precision medicine addresses a fundamental challenge in healthcare: patients respond differently to the same treatment due to individual differences in genetics, physiology, and medical history. Traditional “one-size-fits-all” approaches fail to capture this heterogeneity, limiting treatment effectiveness.1–4 A promising solution involves developing individualized treatment regimes (ITRs), which assign treatments based on individual characteristics to optimize some functional of the counterfactual outcome distribution in the target population, commonly referred to as the value function. The objective is to learn a decision rule that maximizes this value function, thereby selecting the best treatment among available options for each patient. The optimal ITR is the rule that attains the maximal value, defined as the supremum of the value function over a specified class of decision rules. This methodology relies on causal identification assumptions (see Section 2 for details) and has transformed healthcare decision-making,5–9 with applications in economics10–13 and computer science.14,15
Statistical methods for estimating optimal treatment decisions are commonly categorized into two classes: model-based methods and direct search methods. Model-based approaches for estimating optimal ITRs encompass several well-established strategies that rely on modeling the outcome or treatment effect. Among them, Q-learning is a widely used method16–18 that estimates the so-called Q-function, which represents the expected outcome as a function of patient characteristics and treatment, and then derives the treatment rule that yields the highest expected outcome. Another example is A-learning, which focuses on modeling treatment contrasts directly and constructs optimal rules based on estimated treatment effects.19–21 On the other hand, direct search methods aim to directly maximize the value function to obtain the optimal ITR. Early work in this direction includes 22 and, 23 who applied inverse probability weighting (IPW) to estimate the value function and then leveraged classification techniques to learn the optimal ITR. To address potential model misspecification, augmented IPW (AIPW) methods have been developed to achieve double robustness.24–27 More recently, cross-fitting techniques borrowed from semiparametric statistics 28 have been incorporated into ITR learning,11,29 enabling the use of flexible machine learning methods for estimating nuisance functions without sacrificing the efficiency of the resulting ITR estimator. A comprehensive review of ITR learning methods can be found in Kosorok and Laber 3 and references therein.
While these methods have demonstrated success in conventional outcome settings, estimating optimal ITRs with survival data presents substantial challenges. Early works in survival-based ITR estimation include Goldberg and Kosorok 30 and Zhao et al., 9 who extended Q-learning and doubly robust methods to accommodate censored survival outcomes. Subsequent developments have further advanced this research frontier, including Jiang et al. 31 and Díaz et al., 32 followed by more recent innovations such as dynamic treatment regime estimation, 33 imputation-based Q-learning methods, 34 multi-stage regimes with dependent censoring, 35 and transfer learning approaches for censored survival data. 36 However, these existing approaches typically assume complete survival outcome information for all subjects, which is often unrealistic in practice where large amounts of covariate data may be available but survival outcome ascertainment is limited by cost and time constraints. While semi-supervised learning has shown promise in various statistical applications, only a limited number of studies have considered such data structures in optimal ITR estimation,37–39 and these are primarily designed for non-survival outcomes. The intersection of semi-supervised learning and survival-based ITR estimation remains largely unexplored, motivating the development of methods that can effectively leverage both labeled and unlabeled data in the presence of survival data.
To address the challenges outlined above, we propose a novel semi-supervised framework for estimating optimal ITRs in the presence of censored survival outcomes and partially labeled data. We begin by establishing a supervised baseline using inverse probability weighting to estimate the value function under censoring. Building on this, we introduce a semi-supervised estimation strategy that leverages robust imputation to safely incorporate unlabeled data, thereby enhancing statistical efficiency through variance reduction. To overcome the non-smoothness introduced by the indicator function in treatment rule estimation, we employ a kernel smoothing approach, which improves both numerical stability and the convergence rate of the ITR estimator. This smoothing yields substantial computational gains compared to traditional methods such as genetic algorithms, while also enabling theoretical guarantees. Specifically, we show that the proposed smoothed estimators are asymptotically normal, and that the convergence rate of the parameters indexing the optimal ITR can be improved from
The remainder of this article is organized as follows. We first develop supervised and semi-supervised estimators for the optimal ITR with survival data and construct the corresponding kernel-smoothed estimators. We then establish the theoretical properties of the proposed estimators, demonstrating the superiority of our semi-supervised approach over the supervised method. The numerical studies section presents Monte Carlo simulation studies and an application to the METABRIC dataset. We conclude with a discussion of the strengths and limitations of the proposed methodology. Proofs of asymptotic properties and additional numerical results are provided in the Appendix.
Methodology
Let
We then use the potential outcomes framework,40,41 denoting Consistency: If Positivity: Strong ignorability : Conditionally independent censoring:
Our primary objective is to identify and estimate an ITR




In the supervised learning setting, we observe


Let

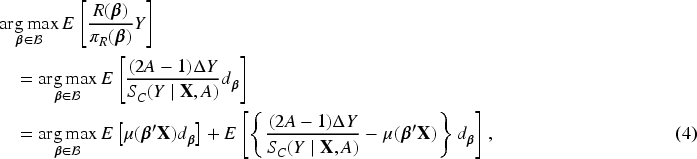
Based on the inverse probability weighting principle, the value function under a treatment rule

When the propensity score


To facilitate computation, we focus on the terms in (2) that depend on

In the semi-supervised (SS) setting, we have access to an additional unlabeled dataset

To fully leverage the auxiliary dataset

It is worth noting that this framework does not require the model to be correctly specified or even to exactly match the conditional expectation
Constructing the imputation function with the conditional expectation
Due to the sharp-edge effect
57
caused by the indicator function
The proposed SS estimator is closely related to, yet fundamentally different from, existing doubly robust (DR) methods for optimal ITR learning with censored data (e.g., Zhao et al.
9
). Both approaches augment the inverse probability weighting (IPW) term with a survival outcome regression component. However, their roles and objectives differ. In classical DR methods, the outcome model is introduced to protect against misspecification of the censoring model, whereas in our SS framework it serves as an imputation function whose primary purpose is to leverage abundant unlabeled data to stabilize estimation and reduce variance. Moreover, standard DR estimators rely exclusively on labeled data, while our method incorporates unlabeled data through the leading term
In this section, the smoothed estimations are proposed. Specifically, the decision indicator function

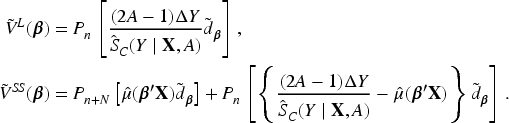
In the practical implementation, it is difficult to optimize


A natural choice of the initial value of
For the above non-convex optimization problem, we use the proximal gradient descent algorithm proposed by Nesterov,
61
which was also adopted in Wu and Wang.
47
Some notes on the convergence of this algorithms can be found in Appendix B. Let


Asymptotic properties
Let For every The density function of The censoring variable The kernel function The bandwidth
Conditions C1-C2 are assumed to ensure the consistency of estimators for

Under conditions C1-C5, as
This theorem gives the consistency of the indexing parameter
Under conditions C1-C5, as
Under conditions C1-C5, as
Under conditions C1-C5, as
Corollary 1, Corollary 2 and Corollary 3 illustrate the consistency of smoothed value functions, estimated parameters and corresponding value functions without smoothing respectively. These corollaries are immediate conclusions from the proof of Theorem 1.
To simplify the technical proof for asymptotic distributions of estimators, we adopt an equivalent identification condition for parameter that ‘there exists a covariate with a nonzero coefficient whose conditional distribution given the other covariates is continuous and its coefficient is normalized to have absolute value one’.
47
Throughout this section, we assume that Let Let
Following the consistency derived in Theorem 1 and the identification condition
Let
where
This theorem establishes the asymptotic normality of the estimators for the index parameters with a convergence rate
To further illustrate the advantages of the smoothing technique in terms of convergence rate, we provide the following theorem.
Under conditions C1–C5 and C8, we have
Theorem 3 states that the convergence rate of the estimated parameters without smoothing is
We utilize a straightforward resampling technique
65
by repeatedly perturbing the objective function to estimate the variance of supervised and semi-supervised estimators. This method has been widely used in the literature for inference.45,47,48,66 Let

It is worth noting that the estimator
Then we follow the proximal gradient descent algorithm as discussed in Section 2.3 and repeat the procedure for B times to get a sequence of estimators
Numerical studies
Monte Carlo simulations
In this section, a series of simulation studies are conducted to evaluate the performance of our proposed smoothed semi-supervised estimation, comparing it to the corresponding smoothed supervised estimation. In case 1, we generate the covariates
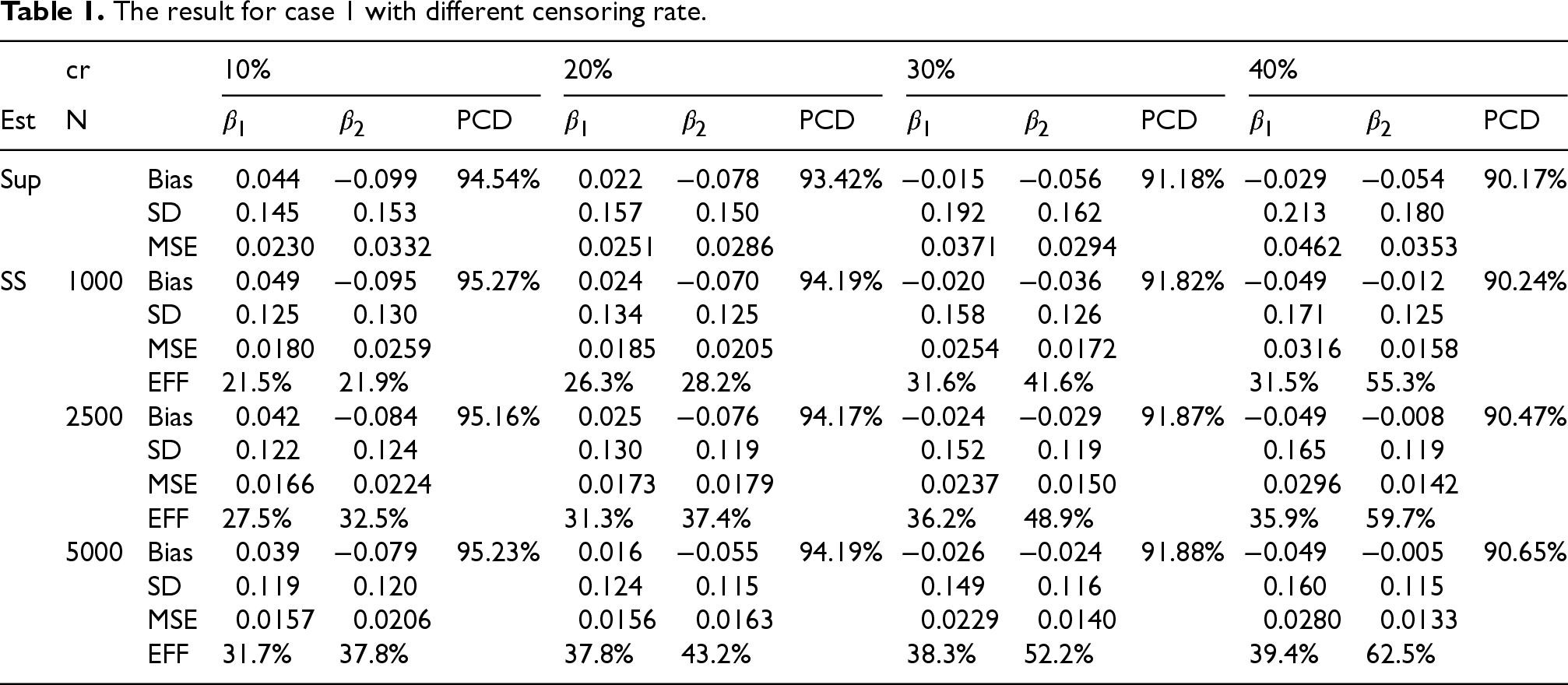
Table 1 reports the bias (Bias) of the estimator, the standard deviation (SD) of the estimator, the mean squared error (MSE) of the estimator, and the percentages of making correct decisions (PCDs) which is defined as


The result for case 1 with different censoring rate.
The result for case 1 with different censoring rate.
The result for case 1 shows the obvious superiority of the semi-supervised approach over the supervised approach. It can be seen that SS estimator has nearly the same bias but significantly smaller SD compared to Sup estimator. Therefore, the MSE of SS estimator is smaller than that of Sup estimator and thus SS estimator has improved efficiency compared to Sup estimator. The proper use of unlabeled data makes the parameter estimation much more accurate, which is also reflected by the improvement of PCD. Furthermore, as shown in Table 1, there exists a direct correlation between the magnitude of the unlabeled sample size and the reduction in standard deviation of SS estimation. Consequently, while maintaining a fixed labeled sample size and the same censoring rate, this reduction results in a corresponding improvement in efficiency. Furthermore, the accuracy of the optimal ITR derived from SS estimation consistently exceeds the PCD of the optimal ITR derived from labeled data only. In addition, the increase of the censoring rate is accompanied by the decrease in the PCD of the optimal ITR. Nonetheless, it is worth noting that the SS estimation still has a significant advantage over the Sup estimation even when the censoring rate increases. It has an efficiency improvement of greater than 20% and maintains a higher PCD compared to Sup estimation. From the above discussion, it can be seen that although the supervised approach yields a good estimate of the optimal ITR, the semi-supervised approach can make this estimate more satisfactory by utilizing auxiliary information, which is very important in practical applications. This further demonstrates the validity of our approach.
In the following, we show that our results are insensitive to the model for treatment-free effects. The true survival times without censoring are generated by
Because our imputation-based conditional expectation model utilizes single index projection for dimension reduction, we can consider higher-dimensional covariates when estimating optimal ITR, which is not feasible in Zhou et al.
48
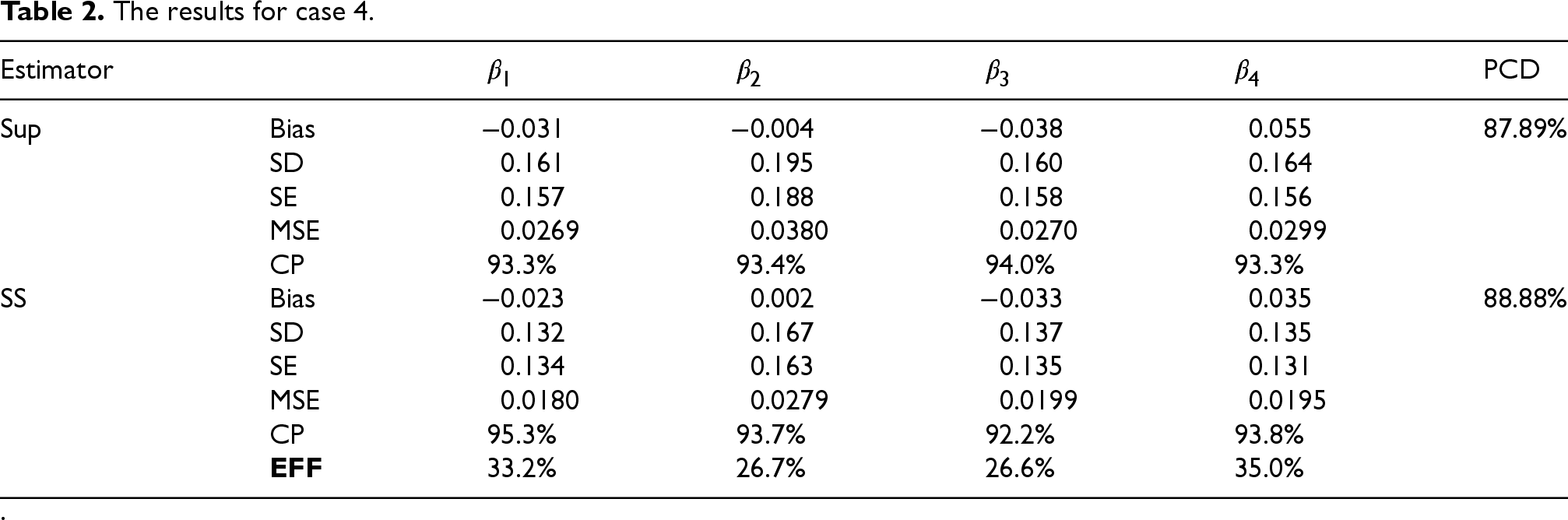
’s study. To investigate whether the semi-supervised method remains more efficient as the covariate dimension increases, we next consider case 4 and case 5 with
The results for case 4.
.
Comparing the simulation results in Table 1 with those in Table 2 and Table C.5, it is found that when the sample size and censoring rate are fixed, the computational complexity of parameter estimation increases significantly with the increase of the covariates dimension
To illustrate our kernel-smoothed semi-supervised method for optimal ITR estimating, we analyze the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) dataset69–71 which is available at cbioportal website. This dataset contains clinical records of primary breast tumors from 2509 patients with long-term follow-up, including the patient’s age at diagnosis, cellularity, estrogen receptor (ER) status, progesterone receptor (PR) status, human epidermal growth factor receptor 2 (HER2) status, neoplasm histologic grade, tumor size, Nottingham prognostic index, non-synonymous tumor mutational burden (TMB), chemotherapy, hormone therapy, type of breast surgery, radio therapy, overall and relapse free survival time (in months) with corresponding status, etc. In order to study the effect of radio therapy (
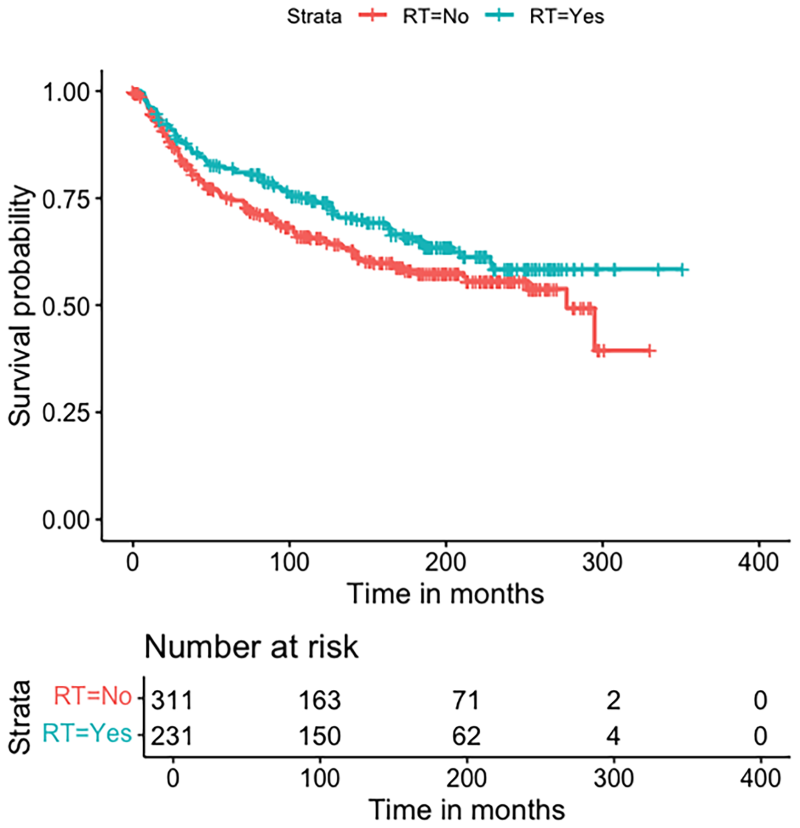
Plot of the Kaplan–Meier estimator of survival functions of relapse free survival time in months for patients who received radio therapy (RT) or not, respectively.
However, we can not take a ‘‘one-size-fits-all’’ treatment regime for all patients because treatment decisions also depend on costs, side effects and other factors that affect an individual’s quality of life. 77 Therefore we need to suggest appropriate treatment decisions for patients based on their individual characteristics.
Numerical simulation results in Section 4.1 show that the increase in the dimension of covariates will lead to a decrease in the PCD of the optimal ITR, so the rational selection of covariates is very important. According to the conclusion of medical studies78,79 that receptors mainly respond to hormone therapy and HER2 targeted therapy, ER, PR and HER2 status are not included in the covariate set for studying the impact of radio therapy prognosis. Inspired by the extensive research in the medical literature on the effects of radio therapy on breast cancer patients,80–82 we select the following covariates
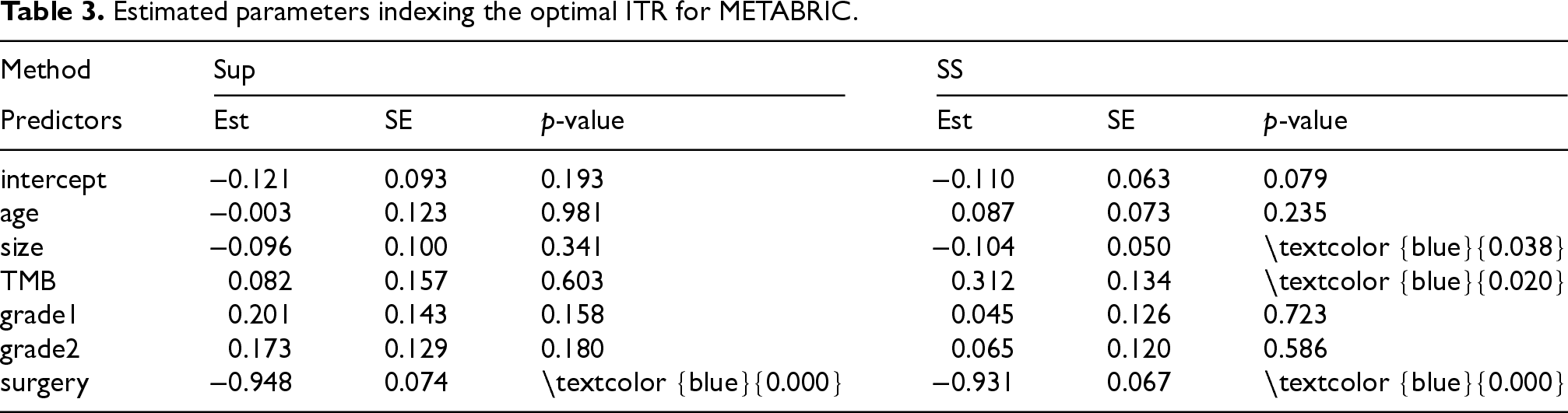
Table 3 shows that both the supervised and semi-supervised methods identify the covariate surgery as significant at the 0.05 level, suggesting that breast cancer patients who undergo breast-conserving surgery should receive radio therapy. This result is in line with existing medical studies. For example, Sedlmayer et al. 85 showed that radio therapy after breast-conserving surgery improved survival for most patients, 86 showed that elderly patients who received radiation therapy after breast-conserving surgery had a lower risk of locoregional recurrence and 87 mentioned that radiotherapy after breast-conserving surgery for early breast cancer has become an indispensable part of breast cancer treatment, which can significantly reduce breast tumor recurrence and improve survival rate. Additionally, the semi-supervised method identifies tow extra significant covariates ‘size’ and ‘TMB’. Thomas et al. 88 demonstrated that tumor size is a significant factor in predicting the recurrence risk in breast cancer patients after receiving radio therapy, with larger tumors indicating a higher risk of recurrence. In contrast, tumor grade is less critical than tumor size which does not show statistical significance in our analysis for this METABRIC dataset. ‘TMB’, which is often considered as an important biomarker in immunotherapy, 89 has an unclear relationship with radio therapy, despite existing research suggesting that local radio therapy can enhance anti-tumor immune responses. 90 Thus, our semi-supervised method offers a potentially viable direction for future research.
The semi-supervised method is more efficient than the supervised method, as also evidenced by the smaller estimation variance and a higher value function. The optimal individualized treatment recommendations derived from supervised and semi-supervised methods are presented in Table 4.
Estimated parameters indexing the optimal ITR for METABRIC.
Treatment recommendation for METABRIC study.

Under the optimal ITR obtained by the supervised method, the average recurrence-free survival time for breast cancer patients is 122.95 months. In contrast, the optimal ITR obtained by our semi-supervised method increases this average to 123.75 months. Figures C.1 and C.2 in the Appendix C show density plot comparisons of the five covariates grouped by whether or not radio therapy was recommended by the supervised and semisupervised methods, respectively. As can be seen in these plots, the covariate of breast-conserving surgery or mastectomy is significantly heterogeneous in both groups, resulting in the covariate ‘surgery’ playing a dominant role in determining our optimal ITR. The Sup and SS estimators generally recommend similar treatments for most patients. Only ten patients who are recommended not to receive radio therapy under the supervised method are re-recommended to receive radiotherapy under the semi-supervised method. For instance, among these ten patients, four are classified as grade 3. Although the four patients are all over 45 years old, their tumor sizes are not less than 20 mm. According to the DEGRO Practical Guidelines for Radiotherapy of Breast Cancer IV, 91 patients with at least two risk factors (grade 3 and larger tumor size here) are strongly recommended to undergo radio therapy after mastectomy to reduce the long-term risk of recurrence. All these findings support that the proposed semi-supervised method is more efficient than the traditional supervised method in this real data application, which is attributed to the effective use of auxiliary unlabeled data.
To conclude, we propose a novel semi-supervised learning method for estimating optimal ITR in right-censored survival data framework. Our research demonstrates that while both the semi-supervised (SS) estimator and the traditional IPW-based supervised estimator are unbiased, the SS estimator may have relatively smaller variance. Consequently, the proposed SS method significantly improves efficiency in the sense of MSE. We establish that the estimated parameters indexing the optimal ITR follow an asymptotic normal distribution. Extensive simulation studies in Section 4 indicate that, with a fixed number of labeled samples
Our methodology is developed under the assumption that the unlabeled outcomes are MCAR, which is standard in the semi-supervised learning literature54,55,92,93 and often adopted when labeling is primarily determined by study design. Nevertheless, in clinical applications, outcome availability may depend on observed covariates due to time or cost constraints, making the MCAR assumption potentially restrictive. To address this concern, our framework can be naturally extended to the more general missing at random (MAR) setting.
94
Let 
Several extensions are also worth further investigation. First, our proposed method can be extended to estimate optimal ITRs under quantile criteria. While some existing studies have considered quantile-based criteria,48,95 none has explored such objectives under a semi-supervised survival data structure. Second, extending the current framework to multi-stage treatment problems for learning optimal dynamic treatment regimes (DTRs)21,96 under the semi-supervised setting is another promising direction. Finally, when treatments are multi-class or continuous rather than binary,97,98 semi-supervised learning of optimal ITRs presents an intriguing avenue for future research.
Supplemental Material
sj-zip-1-smm-10.1177_09622802261460255 - Supplemental material for Efficient semi-supervised estimation of optimal individualized treatment regimes with survival outcome
Supplemental material, sj-zip-1-smm-10.1177_09622802261460255 for Efficient semi-supervised estimation of optimal individualized treatment regimes with survival outcome by Xintong Li, Minghao Chen, Jialiang Li and Yong Zhou in Statistical Methods in Medical Research
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Y. Zhou's work is supported by Natural Science Foundation of Shanghai (No. 23JS1400500), Shanghai Municipal Education Commission (No. 2024AI01002). J. Li's work was supported by Academic Research Funds A-8003585-00-0 and A-8001947-00-00 in Singapore.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.