
Abstract
Randomized clinical trials in critically ill populations often use mortality at the end of follow-up as the primary outcome. When mortality is rare, composite outcomes that capture disease severity over time are frequently employed to improve efficiency. Motivated by the Crystalloid Liberal or Vasopressor Early Resuscitation in Sepsis (CLOVERS) trial—a randomized study comparing two fluid resuscitation strategies in hospitalized patients with sepsis—we evaluate multiple modeling approaches for estimating covariate-adjusted treatment effects on absorbing outcomes such as mortality. While analyses of binary end-of-follow-up outcomes (alive vs. dead) are natural, efficiency can be gained by incorporating low-cost longitudinal and ordinal severity data routinely collected in trials and by imposing reasonable modeling restrictions (constraints). We develop methods that leverage these data within the marginalized model framework, focusing on first-order marginalized transition models, which allows direct estimation of outcome-marginal (population-averaged) treatment effects. We highlight a key property of the marginalized transition model in the presence of absorbing states: the marginal and conditional sub-models correspond to cumulative incidence and discrete hazard models, respectively. Through simulation studies and an application to the CLOVERS data, we compare the validity and efficiency of competing approaches, including standard survival analyses.
Keywords
Introduction
We seek to summarize the treatment effect on disease outcomes in critically ill participants in a randomized clinical trial. A relevant outcome for such studies is mortality at the end of a follow-up period. However, mortality is often sufficiently rare that standard analyses would require excessively large sample sizes or would otherwise lack power. To address concerns about power and efficiency, composite outcomes, such as ventilator-free or oxygen-free days, are often used. These outcomes summarize disease severity over the course of follow-up and have been implemented in multiple studies.1,2 They are often modeled with ordinal regression methods with mortality being the worst/most severe outcome category. While composite outcomes can improve power to detect associations3,4 and are pragmatic for studies of critically ill participants, they have limitations. For example, when the treatment effect on mortality is different from the treatment effect on non-fatal severity, interpreting the model’s estimates can be difficult, and power can be reduced even when compared to standard cross-sectional analyses of mortality. 5
Historically, analyses of baseline covariate-adjusted treatment effects in randomized clinical trials have been conducted with binary logistic regression or with survival analysis models. Binary logistic regression has low power if the prevalence of mortality is low, and a survival analysis can improve power in the presence of dropout. However, a covariate-adjusted hazard ratio may not be of interest because it is based on analyses of a risk set that changes over time and there is an implicit conditioning on a post-randomization, ‘intermediate’ outcome (i.e. mortality has not yet occurred).6–9 Our approach to improve efficiency over a cross-sectional, binary logistic regression analysis does so by exploiting data that are commonly collected in randomized clinical trials or that could be collected at relatively low costs. Rather than modeling a cross-sectional, end of study, binary response, we can enrich analyses by leveraging daily (longitudinal), severity (ordinal) response data.10–13 We may then impose constraints or restrictions on the regression model to directly improve efficiency. From an ordinal response model perspective, we may impose proportional odds or partial proportional odds restrictions to improve precision over a more highly parameterized, general cumulative logit regression model. From a longitudinal data perspective, we may impose restrictions on the treatment effect over time to improve estimation efficiency. Notably, like the Cox proportional hazard model, 14 longitudinal data analysis can improve efficiency and robustness of a treatment effect estimator by using the timing of events and the partial information contained in participants who drop out or are lost to follow-up.15,16 Cross-sectional, binary logistic regression and ordinal regression analyses discard participant’s data prior to dropout.
In this paper, we compare approaches for estimating baseline covariate-adjusted treatment effects on mortality at the end of follow-up. In particular, we focus on longitudinal outcome-marginal models, which estimate covariate-adjusted treatment effects without conditioning on past or future outcome values as in done in standard transition models or mixed effects models.17–20 Within the broad class of outcome-marginal models, we appeal to marginalized models. Marginalized models were developed for longitudinal binary21–23 and ordinal outcomes10,11,13 as likelihood-based alternatives to semiparametric generalized estimating equations 24 and as outcome-marginal model alternatives to generalized linear mixed models and transition models.25,26 Briefly, marginalized models consists of two components: the outcome-marginal model linking the longitudinal outcome to the exposure and covariates and the conditional response, dependence model that captures the outcome dependence or correlation over-time. We will show that when the target outcome state is mortality, these two models correspond to other, more familiar models. Specifically, the outcome-marginal model corresponds to a cumulative incidence model while the conditional, response dependence model corresponds to a discrete hazard model. Thus, unlike in standard survival analysis, marginalized transition models estimate the covariate-adjusted, treatment effect on cumulative incidence of mortality directly. Similar to standard survival models, one can then obtain an end-of-study fully marginal (with respect to both outcome and baseline covariates) treatment effect by integrating over the covariates distribution.
Organization of the paper
Motivated by the Crystalloid Liberal or Vasopressor Early Resuscitation in Sepsis (CLOVERS) randomized clinical trial, we demonstrate the potential benefit of exploiting longitudinal (daily) and ordinal (health state) data to improve estimation efficiency when interest is in an end-of-follow-up treatment effect on an absorbing outcome state (e.g. death). We extend our previous work 13 to show that marginalized transition models are well-suited for this setting. We show that the two components of a marginalized transition model naturally correspond to a cumulative incidence model and a discrete hazards model, allowing direct estimation of outcome-marginal, covariate-adjusted treatment effects. Via simulation, we also show the extent to which precision and robustness to missing data can be improved compared to common analyses (e.g. cross-sectional logistic regression) when the models are correctly specified, and the extent of bias incurred when assumption choices are overly restrictive.
In the next section, we describe the CLOVERS trial. 2 In Section 3, we (i) review the first-order marginalized transition model (MTM) for longitudinal binary response data, (ii) describe its outcome-marginal and conditional, response-dependence components, (iii) discuss restrictions imposed when one of the outcome states is absorbing (e.g. death), and (iv) explore the connection between the MTM components and the more familiar cumulative incidence and discrete hazard models. In Section 4, we show an MTM extension to longitudinal, ordinal outcomes and describe how the ordinal MTM can exploit both the longitudinal and ordinal dimensions of response data to increase efficiency of the outcome-marginal, covariate-adjusted treatment effect estimate on mortality at the end of follow-up. We then conduct a comparative simulation study to examine efficiency and robustness of the estimation strategies in Section 5. In Section 6, we turn back to the CLOVERS trial and conduct analyses using the described methods. We wrap up the paper with a discussion in Section 7.
CLOVERS study: data
The CLOVERS study was a multi-center randomized clinical trial on the efficacy of two fluid resuscitation strategies in patients with sepsis. 2 The trial randomly assigned 1,563 patients to restrictive or liberal fluid resuscitation strategies, and the primary analysis was a survival analysis on mortality before discharge within 90 days after randomization. CLOVERS also conducted numerous secondary analyses that included composite outcomes such as hospital-free days and ICU-free days through 28 days post-randomization. 2 To calculate hospital-free days and ICU-free days, the study collected daily patient state data during the 28 days post-randomization and summarized them to create the outcomes. We study the setting where interest is in a cross-sectional, outcome-marginal, covariate-adjusted treatment effect on mortality at day 28. To improve precision and power over commonly used analysis approaches, we use the available daily state data to estimate this quantity. Specifically, participants were observed daily to be in one of four ordered states from randomization to day 28: discharged/home, hospital, hospital/ICU, and death. We compare treatment effect estimation strategies using cross-sectional (at day 28) and longitudinal data analysis procedures for binary and ordinal outcomes. The binary outcome combines the states discharged/home, hospital and hospital/ICU into a single alive state while the ordinal outcome considers the four states separately.
We include 1,529 of the 1,563 participants in the CLOVERS study with available daily data. Briefly, the mean age was 59.4 years (standard deviation 15.9 years) and mean sequential organ failure assessment (SOFA) score, indicating level of organ dysfunction, was 3.39 (standard deviation 2.67). Figure 1 shows the proportion of participants in each outcome state from day 0 (randomization) to day 28. As is common in studies of critically ill participants, the proportion of participants who die and/or are discharged/at home increases with time, while the proportions of participants in the hospital and hospital/ICU states decreases. While we are interested in the outcome-marginal, baseline covariate-adjusted, cross-sectional treatment effect on day 28 mortality (yellow vs not yellow on day 28), we want to use all intermediate follow-up days and outcome severity states to improve precision.
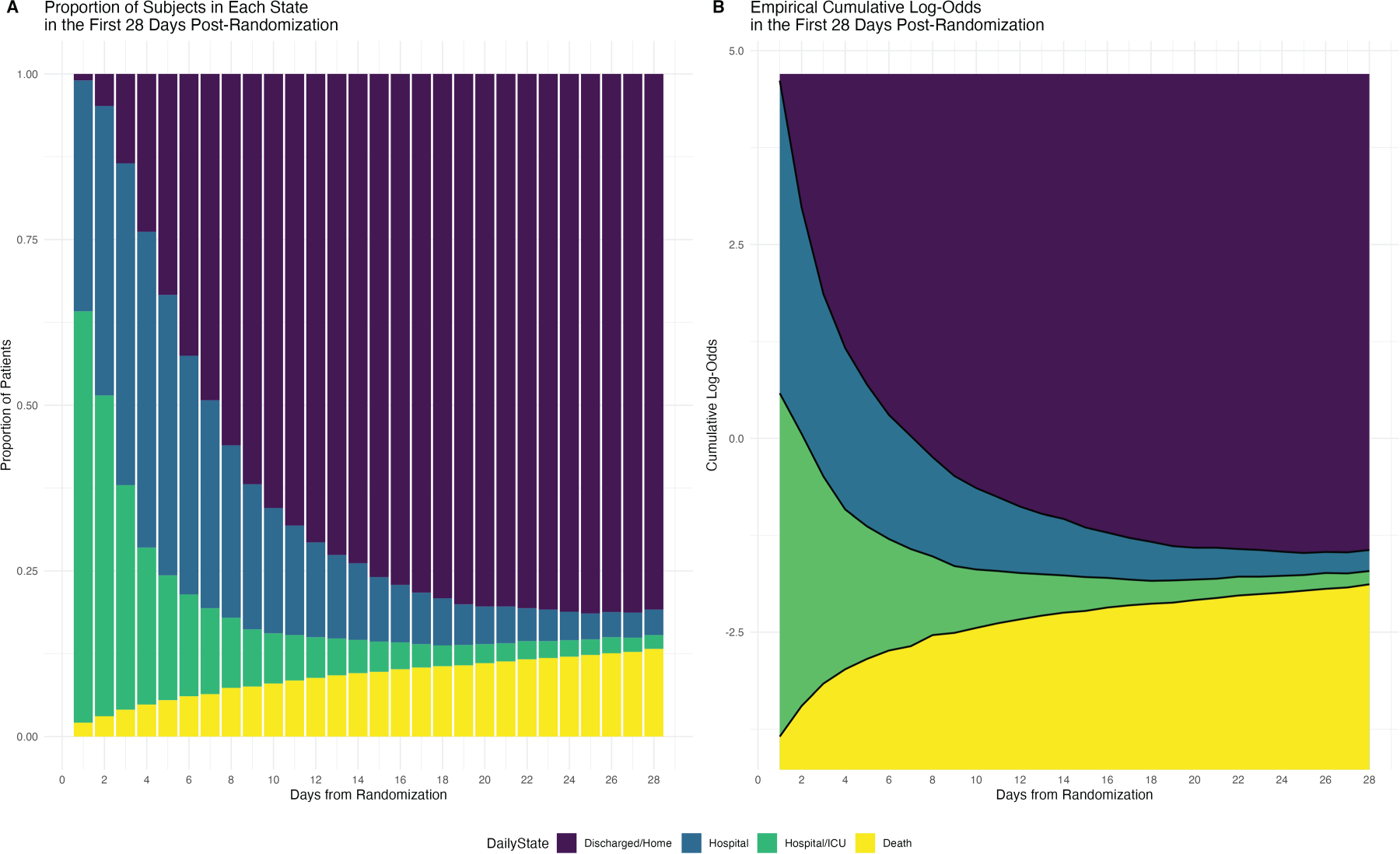
Proportion of patients in each of the four outcome states for the first 28 days of follow-up. Day 0 refers to the day of randomization.
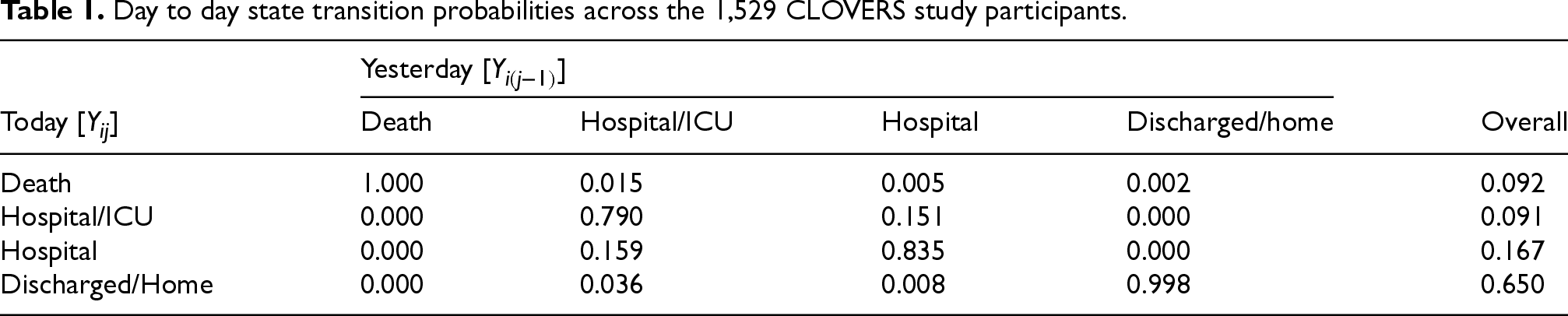
Table 1 shows day-to-day transition probabilities. Death is an absorbing state which is central to our analytical considerations. Discharged/home is nearly absorbing in that several participants died after being in the discharged/home state, although no one was observed to transition from discharged/home to hospital or hospital/ICU. The lack of transitions from discharged/home to hospital or hospital/ICU was part of the study design, that is, study coordinators did not follow hospitalizations after discharge; however, for the purposes of our analyses, we will assume that none of those transitions occurred. While participants transitioned regularly between the hospital and hospital/ICU states, the overall probability of remaining in the same state from day to day was high.
Day to day state transition probabilities across the 1,529 CLOVERS study participants.
In studies like CLOVERS, the simplest way to estimate the treatment effect on mortality at the end of follow-up is to fit a binary logistic regression model with the outcome being mortality status (yes/no) at day 28. However, we may gain efficiency by considering alternative strategies that incorporate richer outcome information into the estimation procedure. For example, we may focus analyses exclusively on day 28 but replace the binary mortality status with a four-level ordinal severity outcome (death, hospital/ICU, hospital, discharged/home); alternatively, we may exploit the complete daily trajectory from baseline to day 28 of the binary mortality status (yes/no); finally, we may use daily, severity information to fit a longitudinal, ordinal MTM. One would expect that incorporating richer outcome information into the estimation model could result in efficiency gains. However, to realize the efficiency gains, parameter constraints are likely to be required. For instance, prior work has shown that constraining the treatment effect at baseline to be equal to zero in a randomized clinical trial can improve efficiency.27,28 This paper aims to explore the potential for efficiency gains from these alternative modeling strategies compared to binary logistic regression.
Let 


The marginalized transition model can be used for the analysis of longitudinal binary outcome data even when outcome state 

Additionally, because when
When severity is available: Cumulative probability models
We now incorporate severity into the analysis. That is, we expand state 2 (i.e. alive) into health states with higher values denoting better health. Our interest is still in the outcome 





As in the binary outcome setting, the CPMs in equations (4) and (5) only describe a portion of the multivariate distribution 
Aims and data generating mechanism
Our simulation study aims to (i) characterize the validity, efficiency, type I error and power of the described models for estimating an end-of-study treatment effect when one outcome state is absorbing; (ii) highlight the potential benefit of using longitudinal data under various dropout mechanisms; (iii) study robustness of the estimation procedures to model misspecification; and (iv) compare the efficiency of marginalized transition models and Cox proportional hazard models in estimating an end-of-study treatment effect.
We begin by simulating data from a randomized clinical trial where 
To evaluate and compare power across analysis procedures, we increase the absolute magnitude of the treatment effect from
To characterize robustness of the estimation procedures to model misspecification, we consider the complete follow-up setting described above and then modify coefficient values to simulate two additional scenarios: one where the PO assumption for the treatment effect does not hold, and one where the PO assumption holds for the treatment effect but not for the covariate parameter. Misspecification of the PO assumption for the treatment effect was simulated by setting
Finally, because the Cox proportional hazards model is a popular choice in settings like those considered here, we sought to compare marginalized transition models and Cox proportional hazards models. To do so we generated and fit data under 1) the marginalized transition model described at the beginning of the section and 2) a Cox proportional hazard model with a Weibull baseline hazard. Corresponding to 2), survival times were generated from
Estimation target and methods
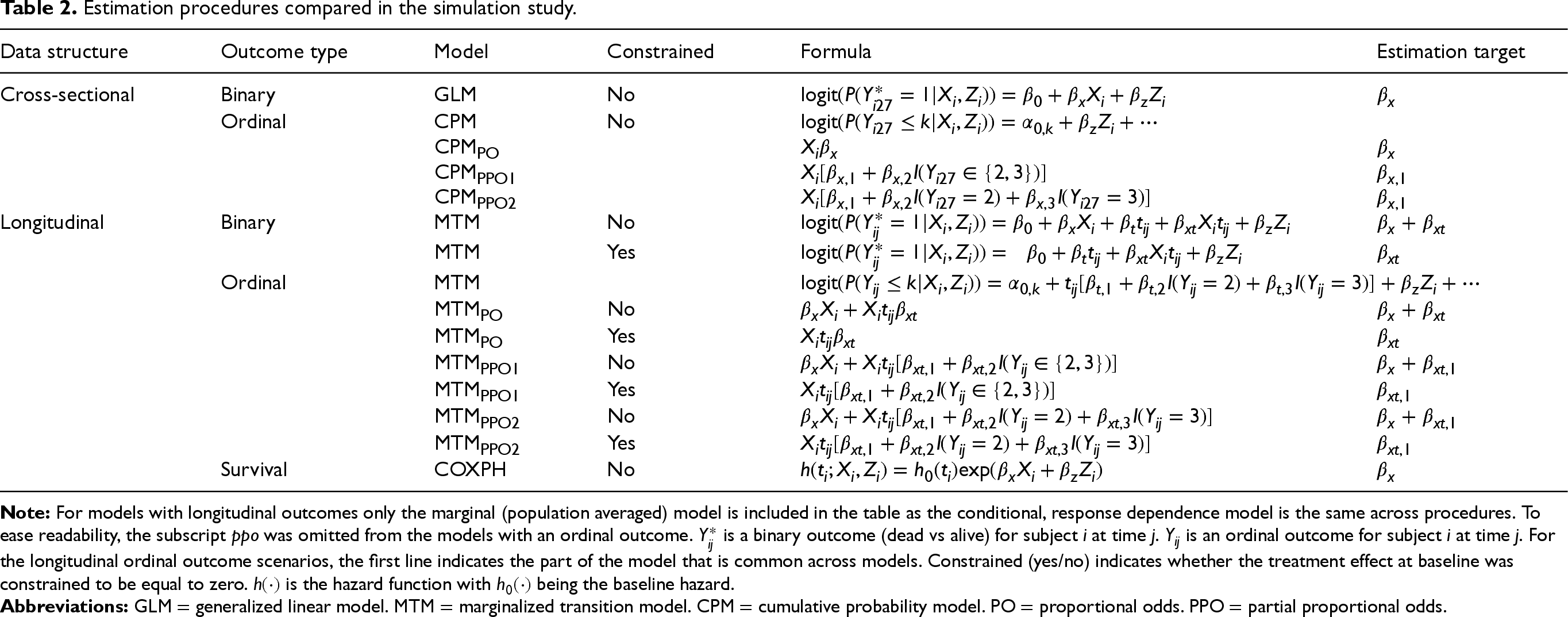
Across all simulations, we are interested in estimating an end of follow-up treatment effect on an absorbing state. For a comprehensive comparison, we estimate the treatment effect with the procedures described above and summarized in Table 2. Each procedure is identified by a distinct combination of data structure (cross-sectional or longitudinal), outcome type (binary or ordinal), model (GLM, CPM, MTM, or Cox proportional hazard models), and, when applicable, a baseline treatment effect constraint (i.e. is the treatment effect constrained to be zero at baseline?). Within the CPM and MTM models we further explore each procedure under different PO assumptions for the treatment effect. Based on these possible combinations, we obtain 13 different modeling approaches.
Estimation procedures compared in the simulation study.
Estimation procedures compared in the simulation study.
First, we consider the binary outcome
For each of the 5,000 replications, we estimated regression coefficients for the treatment effect, their standard error and the percent bias in the treatment effect estimate empirical standard error (SE) of the treatment effect estimate average standard error estimate (SEE) root mean square error (RMSE) coverage probability (CP) of the relative efficiency of each estimation procedure to the cross-sectional generalized linear model for binary outcome (GLM) (i.e. the empirical variance of GLM divided by empirical variances of all other estimation procedures).
Results
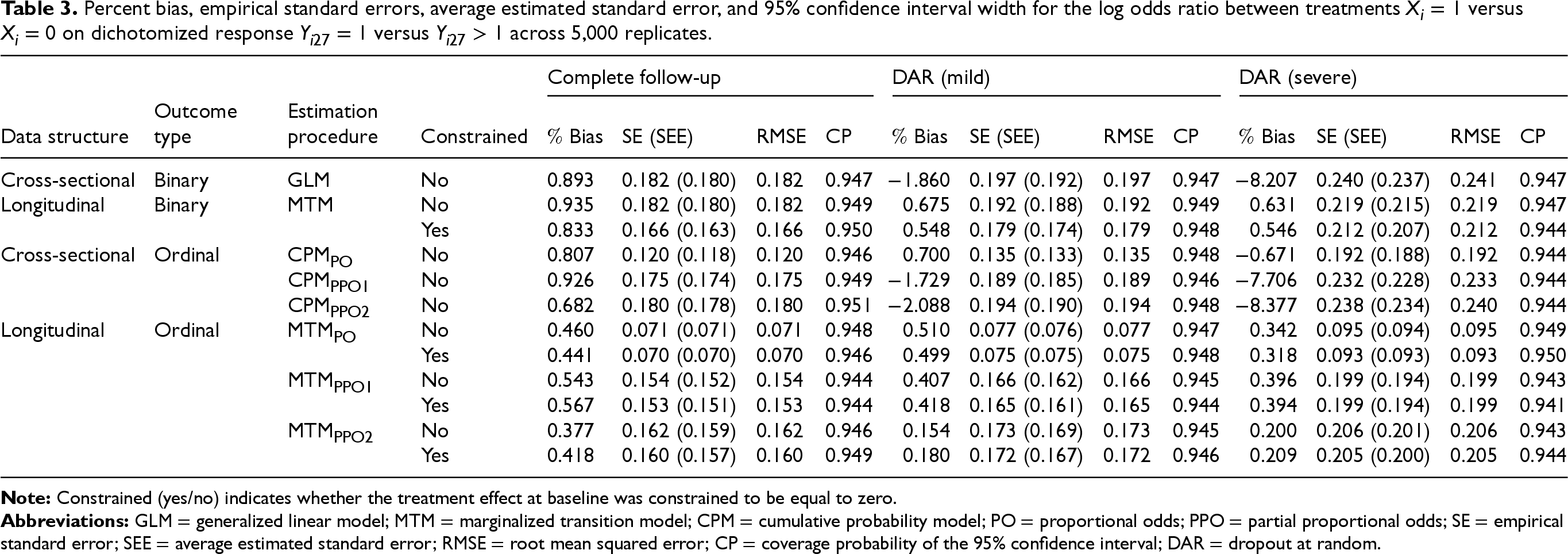
Results on validity of the marginalized transition models are presented in Table 3. Under complete follow-up and mild DAR, all estimation procedures yielded approximately unbiased treatment effect estimates and standard errors, and confidence intervals had appropriate coverage. Under severe DAR, estimates of the association between the treatment and the dichotomized response value
Percent bias, empirical standard errors, average estimated standard error, and 95% confidence interval width for the log odds ratio between treatments
versus
on dichotomized response
versus
across 5,000 replicates.
Percent bias, empirical standard errors, average estimated standard error, and 95% confidence interval width for the log odds ratio between treatments
Figure 2 shows the treatment effect relative efficiency of each estimation procedure to the cross-sectional generalized linear model with a binary outcome (GLM). Under complete follow-up, considering a longitudinal binary outcome rather than a cross-sectional binary outcome did not result in any precision gain. However, to the extent that dropout occurs, gains were realized (e.g.
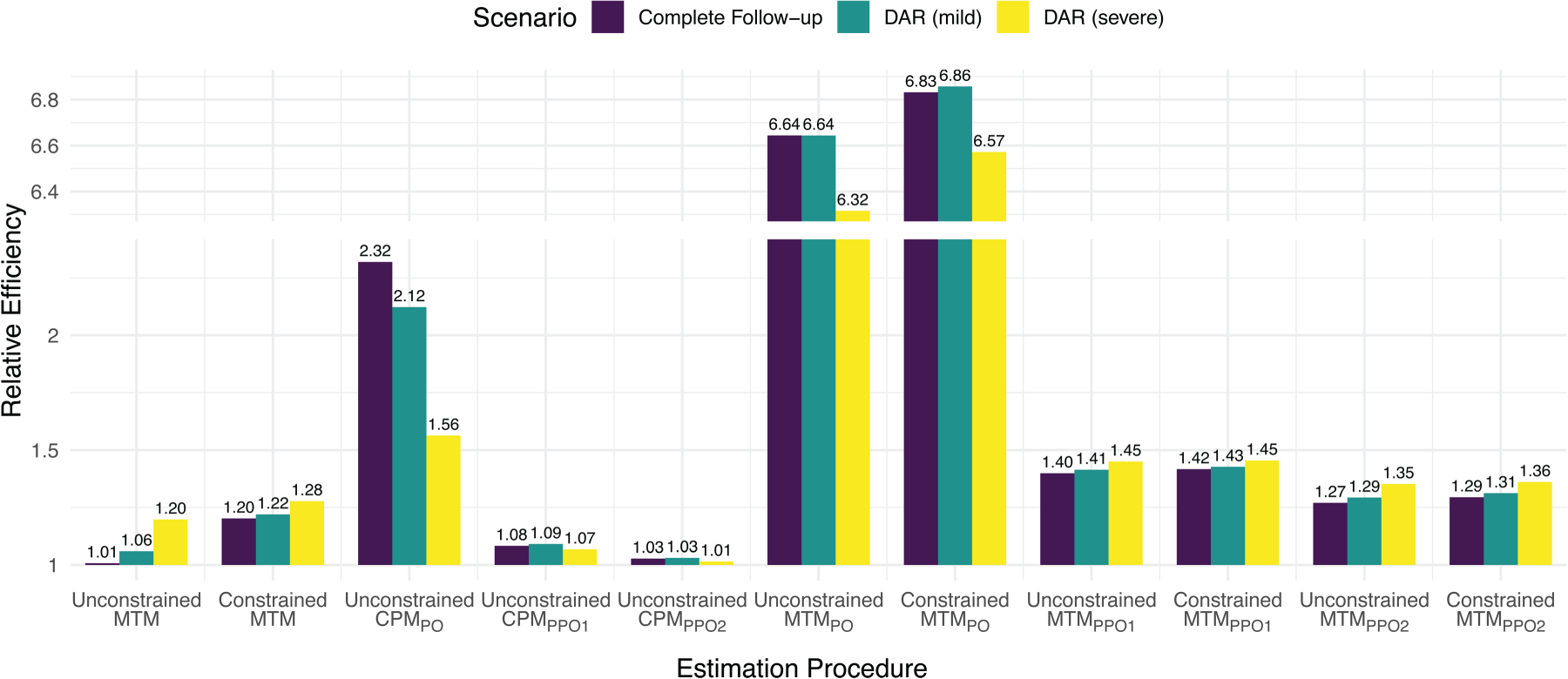
Relative efficiency of different estimation procedures to a cross-sectional binary logistic regression (GLM) in estimating the association between the treatment
Consistent with the observed validity when the above models are properly specified, we observed that type 1 error rates maintained their nominal 0.05 levels (see Supplementary Table S3), and consistent with the efficiency gains observed above, we observed power improvements associated with the use of longitudinal and ordinal response models and with the placement of constraints on the treatment effect overall and at baseline (for the longitudinal binary response setting; see Table 4).
Percent bias, empirical standard errors, average estimated standard error, coverage probability of the 95% confidence interval and power for the odds ratio between treatments
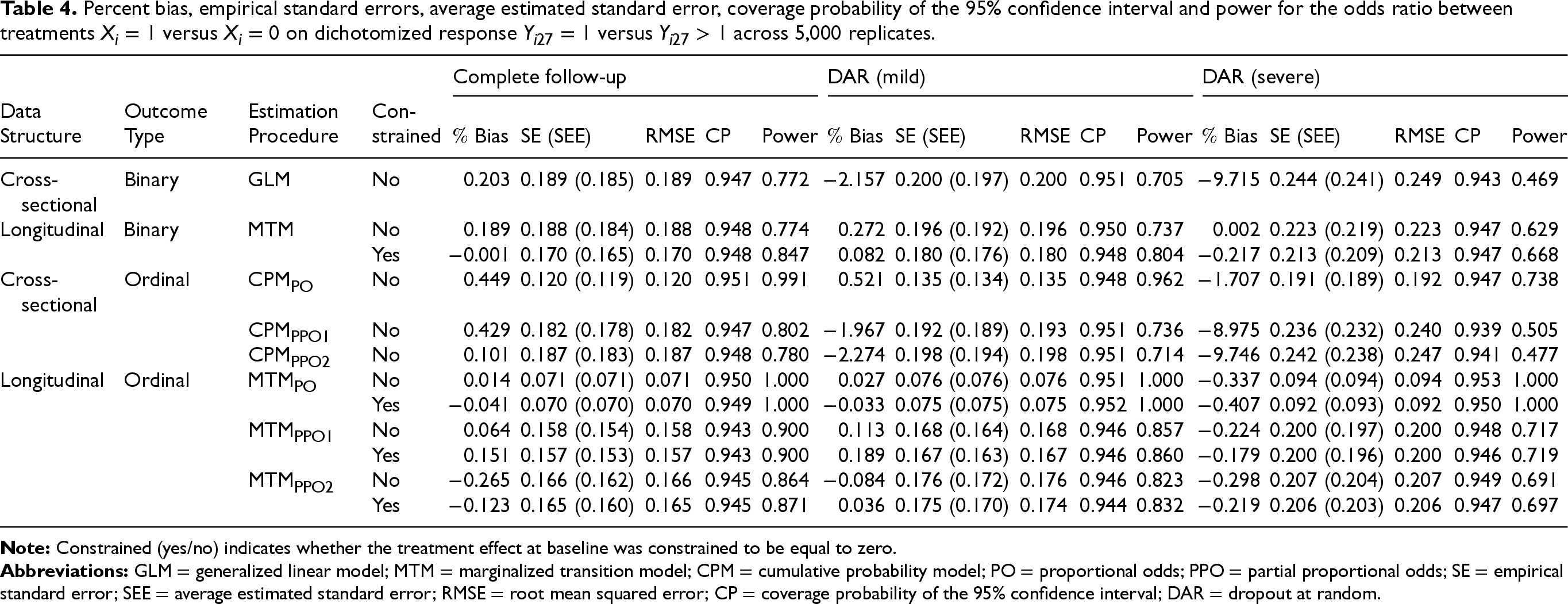
Table 5 summarizes the results when the model is misspecified. When the PO assumption for the treatment effect is misspecified, models that assume a common odds ratio across the three log cumulative odds dichotomizations (CPM
Percent bias, empirical standard errors, average estimated standard error, and 95% confidence interval width for the log odds ratio between treatments
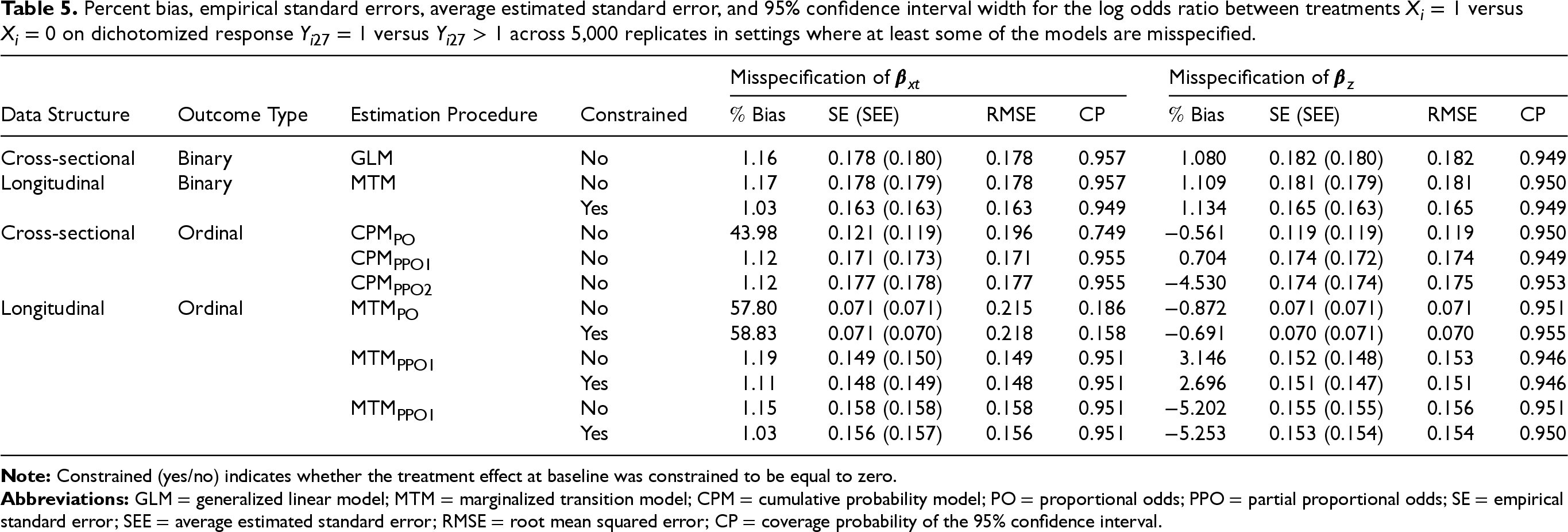
Table 6 summarizes results of the comparison between the marginalized transition models and the Cox proportional hazard model. When generating the data under a marginalized transition model with an ordinal outcome and a treatment effect assumed to be the same across all dichotomization of
Percent bias, empirical standard errors, average estimated standard error, and 95% confidence interval width for the fully marginal (with respect to
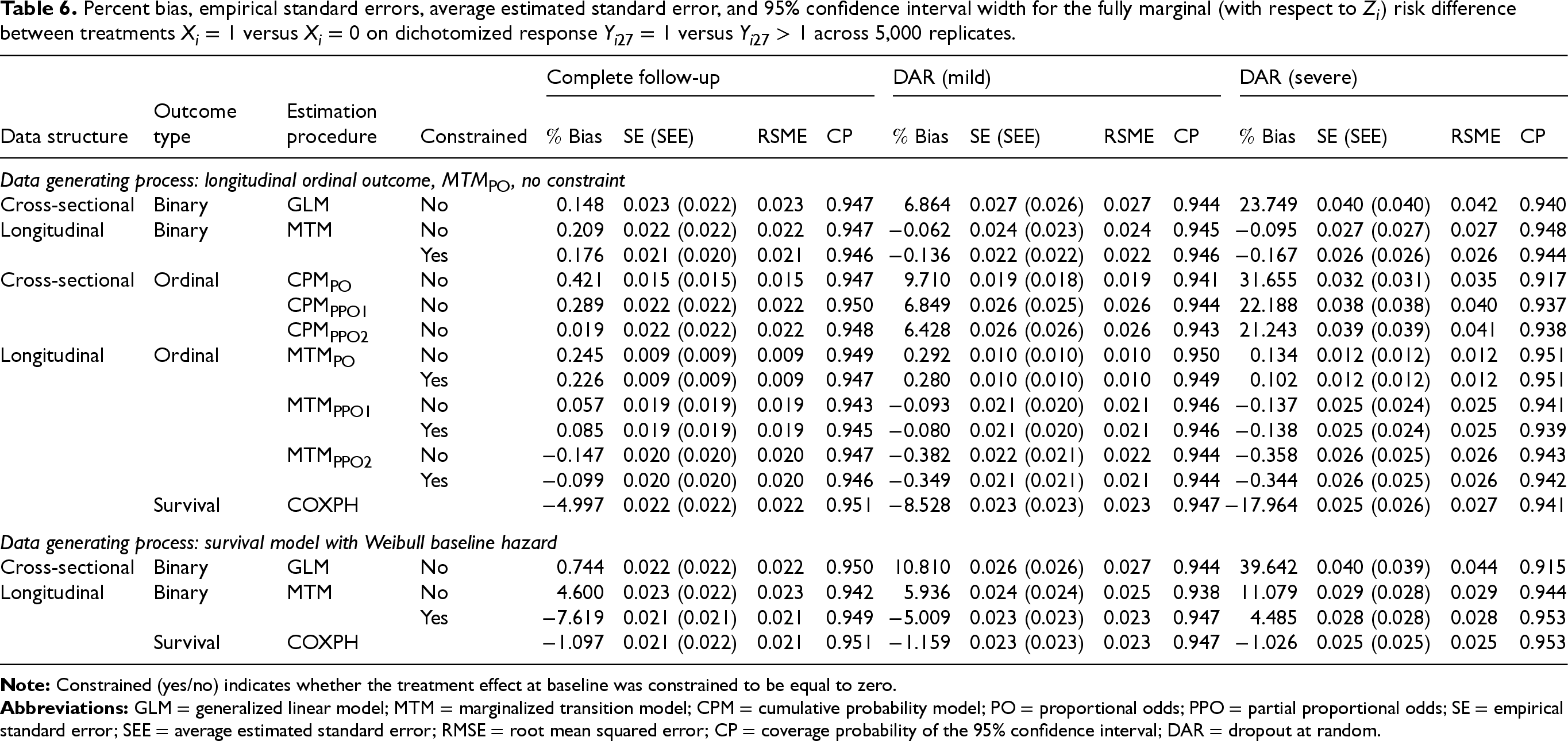
One interesting observation occurred under mild and severe DAR with the cross-sectional modeling procedures (CPM
We note that when severity is available, the treatment effect on mortality can be estimated using a discrete time multi-state survival model. 31 While we did not include the multi-state survival model in the simulations due to its heavy computational burden, we fit it to estimate the treatment effect on mortality in the CLOVERS data in the next section. A detailed summary of runtime for the currently implemented MTM models is provided in Table A4. Under complete follow-up, average runtime per replicate were 1−2 minutes for longitudinal binary outcomes and 6−8 minutes for longitudinal ordinal outcomes. These runtimes are expected to improve with updates to the software. Computation time was negligible for the GLM, CPM, and Cox proportional hazards models (<0.01 minutes on average).
For the CLOVERS study analyses, we implemented the estimation procedures described in Section 5 to calculate the effect of a restrictive fluid strategy on mortality at the end of follow-up. The covariate vector
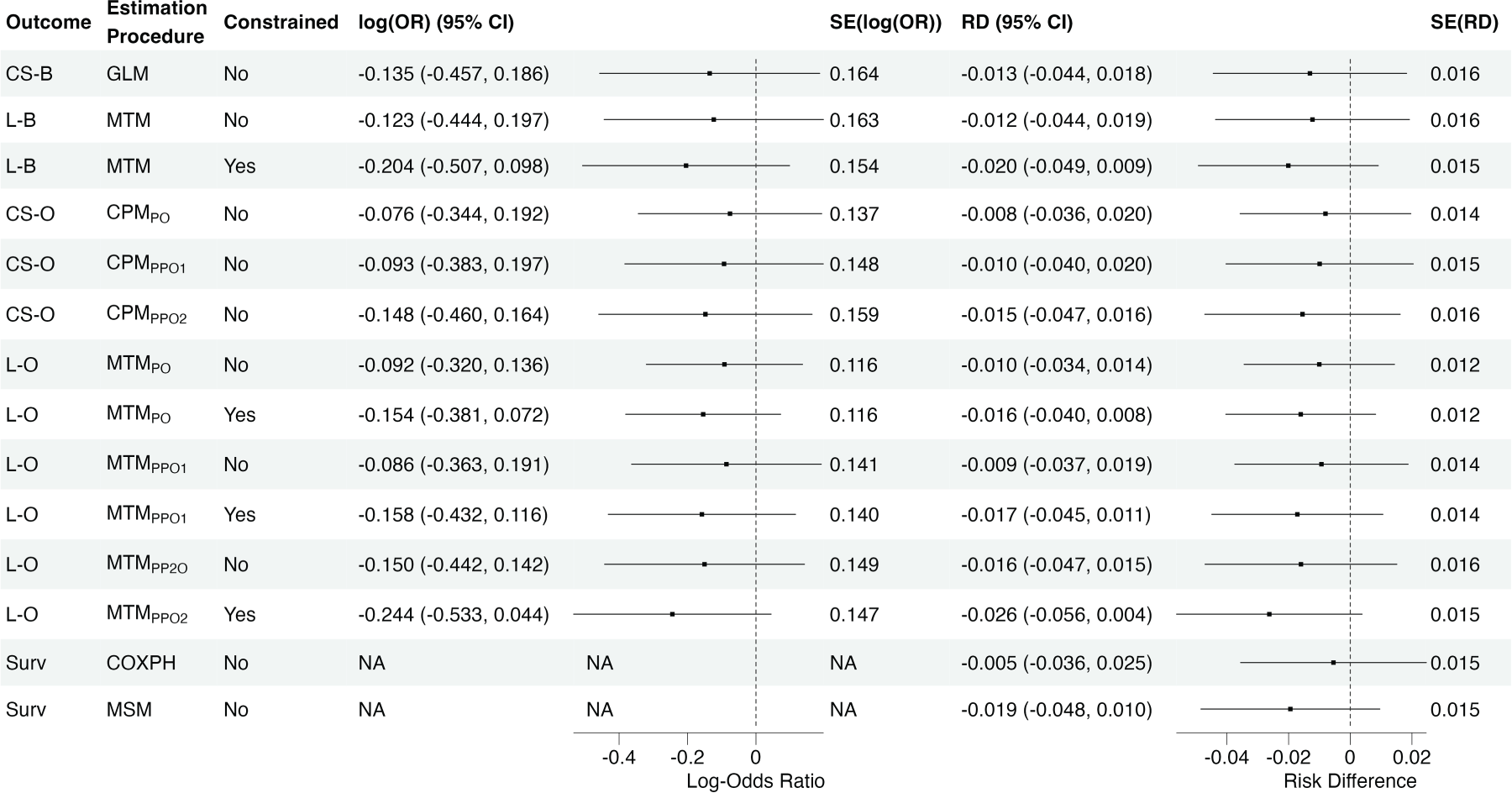
Estimated covariate-adjusted log-odds ratios and fully marginal (with respect to baseline covariate) risk differences (RD) describing the effect of restrictive fluid strategy on mortality at the end of follow-up with
Similar to the precision gains observed in the simulation studies for the log-odds ratio estimates, model uncertainty decreased when we used an ordinal outcome rather than a binary outcome: compared to the cross-sectional generalized linear model with a binary outcome, we observed a
When estimating risk differences, the estimated standard error for the treatment effect from the Cox proportional hazard model tracked with those of the marginalized regression models for longitudinal binary outcome. Similarly, the estimated standard error for the treatment effect from the multi-state survival model tracked with the less constrained MTMs for ordinal outcomes (e.g. estimated standard error was 0.015 in both the multi-state model and the longitudinal ordinal model where the treatment effect was assumed to differ across all outcome dichotomizations).
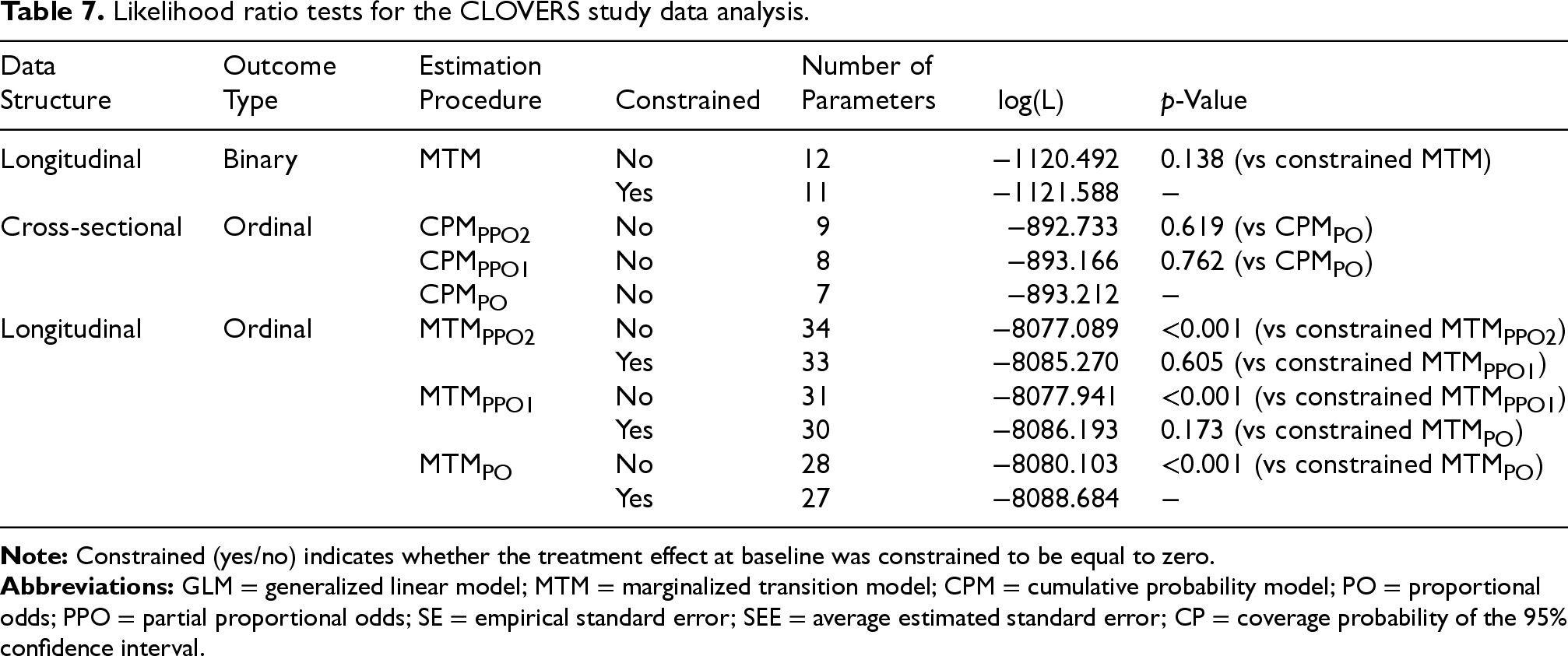
Likelihood ratio tests can be used to compare many of the model fits. Here, we focus on understanding whether relaxing the PO assumptions and/or the assumption of a null treatment effect at baseline improved model fit. Table 7 shows the maximized log-likelihood for the MTMs with longitudinal binary outcome, the CPMs with cross-sectional ordinal outcome, and the MTMs with longitudinal ordinal outcome. For the longitudinal binary outcome models, we observed insufficient evidence to suggest that relaxing the assumption of a null treatment effect at baseline improved model fit (
Likelihood ratio tests for the CLOVERS study data analysis.
We discussed and compared approaches to summarize the outcome-marginal baseline covariate-adjusted treatment effect on mortality at the end of a follow-up period in a randomized clinical trial when health state data are collected daily (i.e. longitudinally). We focused on how and when specific modeling choices, such as the use of longitudinal versus cross-sectional outcomes or of ordinal versus binary outcomes, can improve estimation efficiency compared to the commonly used cross-sectional binary logistic regression and survival analysis.
Together with the choice of outcome, we studied how estimation efficiency can be improved by imposing constraints on the form of regression model. In particular, we considered scenarios where the treatment effect at baseline was forced to be zero and, for the ordinal outcome, we examined scenarios where we imposed and/or relaxed PO assumptions. Constraining the treatment effect at baseline to zero improved estimation efficiency with longitudinal binary outcome models but not with longitudinal ordinal outcome models. This result could be explained by the number of parameters estimated in each procedure: there were 6 parameters in the MTM with a longitudinal binary outcome compared to the 18 to 20 parameters in the MTMs with a longitudinal ordinal outcomes. Hence, the removal of one parameter, known to have no effect on the outcome, may have a greater impact on the model that estimates fewer parameters overall. When we imposed the PO assumption on the treatment effect, we observed additional improvements in efficiency. However, we also note that the PO assumption could lead to invalid inference if misspecified. Thus, when deciding on the form of the regression model, one needs to strike a balance between robustness and efficiency. While we focused on treatment effect estimation in a randomized clinical trial, the proposed approach can be applied to non-randomized studies where one is interested in an end of follow-up exposure effect while adjusting for baseline covariates. However, in these settings, the inclusion of time-varying exposures and/or confounders would require careful consideration.
In the presence of at least one absorbing state, we showed how MTMs can directly model cumulative incidences without having to condition on any post-randomization outcomes. The outcome-marginal and conditional response-dependence components of an MTM correspond to cumulative incidence and discrete hazard models, respectively, and, when interest is in a fully-marginal (i.e. marginal with respect of both outcomes and covariates) treatment effect, the efficiency of MTMs tracks with Cox proportional hazard models and discrete-time multi-state survival models. In contrast to survival analysis methods, first-order MTMs provide a valid way to directly estimate covariate-adjusted treatment effects on cumulative incidence.
The design of CLOVERS did not allow us to observe transitions from the discharged/home state to either the hospital state and/or the hospital/ICU state. While, for the purpose of the analyses in this paper we assumed that none of unobserved transition occurred, this assumption might not be realistic in scenarios where the probability of remaining in the same state from day to day is lower. In future work, we will explore how marginalized transition models with longitudinal ordinal outcomes can be extended to cases where we have interval censored data, for example, when we know participants are alive, but we do not know in which state they are in. The MTMs presented in this paper can be fitted using the R package
Supplemental Material
sj-pdf-1-smm-10.1177_09622802261462925 - Supplemental material for Modeling treatment effects on absorbing outcomes in clinical trials: Leveraging longitudinal and ordinal data for efficiency gains
Supplemental material, sj-pdf-1-smm-10.1177_09622802261462925 for Modeling treatment effects on absorbing outcomes in clinical trials: Leveraging longitudinal and ordinal data for efficiency gains by Chiara Di Gravio, Ran Tao, Yunbi Nam, Eric P Schmidt, Nathan Shapiro and Jonathan S Schildcrout in Statistical Methods in Medical Research
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors have no conflicting interests to declare with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.