
Abstract
By its nature, scientific understanding is subject to change, as methods to study a phenomenon become more refined. How can scientific findings be conveyed to the general public when segments of the public may hold on to beliefs unsupported by science? We examined this problem by considering how individuals correct health misconceptions in response to differently phrased explanations of scientific knowledge. The results from two experiments showed that while explanations containing more tentative phrases characteristic of scientific communication (e.g., evidence suggests) were effective, those containing more assertive phrases (e.g., this is proven) were the most effective for updating lay knowledge. Furthermore, relative to the more tentative phrasing, the more assertive phrasing was judged as more convincing and conveying higher confidence. These findings demonstrate the need to determine more effective methods of communicating and conveying confidence in scientific findings.
Introduction
Communicating scientific knowledge to the general public is particularly difficult in circumstances in which information is novel or requires updating. In such cases, officials often make use of cautious phrasing (Cozby and Bates, 2014; Nesselroade and Grimm, 2018). This practice of using cautious phrasing is critical for accurately representing the evolving and sometimes incomplete nature of scientific findings. For example, to refute a lay misconception that the COVID-19 vaccine causes infertility, health officials may state that, “There is no evidence to suggest that COVID-19 vaccines cause infertility.” Such a statement, however accurate, may also come across as ambiguous. For example, it may mean that studies have examined this topic and found no relationship between the vaccine and infertility, or that the relationship has not been studied. Furthermore, which interpretation they favor may reflect individuals’ preexisting beliefs, consistent with the confirmation bias (Klayman, 1995). To help prevent the spread of erroneous and potentially dangerous health information, it is important to examine effective ways to correct health misconceptions. The central aim of the present research was to empirically test the hypothesis that the public is sensitive to the type of phrasing used in refutations of health misconceptions. We examined whether feedback containing tentatively worded phrases would be more or less effective than feedback containing assertively worded phrases in leading people to update their health knowledge.
The effects of communicating scientific uncertainty are mixed, and the consequences are not always obvious. Some research suggests that people find certain types of scientific uncertainty confusing, potentially leading to lower trust and a reduced likelihood of changing their behavior (e.g., Gustafson and Rice, 2020). However, other research suggests that transparently communicating uncertainty, particularly when it reflects the nuance of the evidence, can increase trust and improve the public’s understanding of science under some conditions (Batteux et al., 2022; Dries et al., 2025; Jensen, 2008; Mayweg-Paus and Jucks, 2015). Given these conflicting findings, it is critical to investigate how different types of language used to convey uncertainty influence belief updating.
Health misinformation
Health misinformation has rapidly increased in recent years largely because of proliferation through social media and the internet (Swire-Thompson and Lazer, 2020). Some misinformation may be disseminated with malicious intent, such as when untested health remedies are sold for financial gain. Other times, unverified (or incorrect) health information is perpetuated with good intent, such as when one recommends an untested home remedy. Regardless of the reason for its spread, unsubstantiated health practices have become integrated into our daily lives, often with adverse effects. For example, despite extensive research suggesting that most dietary supplements are ineffective for the general public (e.g., Jenkins et al., 2018), they are frequently marketed with promises of improving health. In addition to financial costs of engaging in ineffective health behaviors, there may be health repercussions, such as medication interactions (Jalloh et al., 2017) and organ damage (Radha Krishna et al., 2011). Furthermore, using ineffective health remedies can lead to delayed care and improper diagnosis (Wardle and Adams, 2014).
Correcting misconceptions
With the potential for negative consequences of misconceptions, it is important for officials to convey accurate scientific findings clearly and effectively with the public. While some research has focused on mobilizing people to correct misinformation on social media (Bautista et al., 2021; Tully et al., 2020) or on specific health topics, such as e-cigarette use (Huang and Wang, 2020) and measles vaccinations (Gesser-Edelsburg et al., 2018), very little work has examined how to effectively correct health misconceptions in general.
In a recent study, Sitzman et al. (2021) examined methods of correcting general health misconceptions in younger and older adults. After indicating whether health statements were true or false, participants received direct feedback about their judgments (e.g., “You are correct! This statement is false”) followed by a brief explanation about the statement’s accuracy. Results showed that direct feedback helped people correct their knowledge, an effect that was sustained after a week’s delay. The results are consistent with other research, suggesting that simple and direct refutations (i.e., “This statement is false”) are effective in correcting various types of misconceptions, including misconceptions about learning and memory (Lithander et al., 2021; Van Loon et al., 2015) or climate change (Danielson et al., 2016).
Despite these promising laboratory findings, scientists and healthcare officials may not use these kinds of simple and straightforward refutations (i.e., This is false). Instead, their training in research methods and statistics encourages a more nuanced, probabilistic language to capture the nature and strength of the existing evidence, as well as the evolving nature of science itself (Cozby and Bates, 2014; Nesselroade and Grimm, 2018). In turn, health organizations often adopt this cautious language when communicating information to the public (CDC, 2019; NHS, 2022; NIH, 2020; WHO, 2020). For example, instead of definitively stating that masks are effective against COVID, the Centers for Disease Control and Prevention (CDC) stated: “Experimental and epidemiologic data support community masking to reduce the spread of SARS-CoV-2” (CDC, 2021). Use of the more nuanced and cautious scientific language by healthcare professionals may come across to lay people as tentative or uncertain. Whereas both a direct (“Masks are effective against COVID”) and scientifically phrased statement (“Data support community masking to reduce the spread of SARS-CoV-2”) would support mask-wearing, it is possible that the type of phrasing used by the CDC and other scientific organizations might come across to the public as weak and unconvincing, potentially signaling that future data may alter or modify these recommendations.
Scientific phrases that were used during the COVID-19 pandemic have also been used in communication to counter misconception that the measles, mumps, and rubella (MMR) vaccine causes autism. In a statement, the Global Advisory Committee on Vaccine Safety (GACVS), concluded that “no evidence exists of a causal association between MMR vaccine and autism or autistic disorders” (WHO, 2020). This statement was intended to convey that the MMR vaccine is safe and does not cause autism in children. But it could be taken either as providing reassurance about the safety of the vaccine or as expressing uncertainty about the relationship between the vaccine and autism (World Health Organization [WHO], 2020).
The present research
Because health officials and scientists are commonly taught to use certain types of phrasing in their communication, we felt it was important to empirically test how these phrases are perceived by the general public and the extent to which such phrasing is effective for helping people to revise their health beliefs. Thus, the aim of the current experiments was to directly evaluate the effectiveness of various common phrases used by scientists for correcting health misinformation, and to compare their effectiveness to more assertive phrases (e.g., this is absolutely true, Epstein, 2015; e.g., this is completely false, Fields, 2023).
Participants were given statements containing true statements or health misconceptions and had to decide whether the statements were true or false. They were then given different types of feedback or a no-feedback control condition. Across both experiments, we examined the effectiveness of feedback containing common scientific phrases (e.g., evidence suggests) compared with feedback containing more assertive phrases (e.g., it is proven).
Pilot study: Perceptions of assertive and tentative phrasing
Before comparing the corrective effects of assertively worded feedback with those of more tentatively worded feedback, we conducted a pilot study of the materials to determine how participants interpreted refutations that include the tentative phrases common in scientific communication versus the more assertive phrases. Participants were asked to rate the phrases in terms of ease of understanding, strength of argument, and confidence conveyed.
Methods
Participants
Ninety-one participants (51.65% female, 48.35% male; 43.10% white, 20.69% Black, 15.52% Latino/Latina, 13.79% Asian-American, 3.45% Middle Eastern, all other categories <2%; 18–26 years old, Mage = 19.02, SD = 1.42) were asked to evaluate the enhanced tentatively worded and assertively worded feedback used in the experiments. No participants were excluded from the analysis. Participants were undergraduate students recruited from the University of Massachusetts Lowell’s Sona system, a web-based participant recruitment and management platform. Participants were compensated with course credit. All experimental procedures were approved by the university institutional review board, and all participants provided informed consent.
Materials and procedure
Stimuli consisted of 28 true and 28 false statements about health and nutrition. True statements included items such as “Eating smaller meals can help reduce acid reflux” and “A warm compress can help relieve dry eyes.” False statements included items such as “Eating carrots can improve your vision” and “Eating local honey can fight off allergies.” A total of 23 statements were taken from a recent study on health misconceptions (Sitzman et al., 2021); the remaining 33 were compiled from internet sources detailing health information. These health statements were selected and categorized as a misconception if the statement had no evidence supporting it or had been refuted in the peer-reviewed literature, whereas statements were categorized as true if the majority of peer-reviewed literature supported the information.
To create statements that people would pay attention to and be motivated to answer correctly, we selected health statements that could result in an associated behavior. Based on published data (Sitzman et al., 2021) and another pilot study we conducted (with 34 subjects), we selected items that were endorsed by between 10% and 90% of the participants based on their responses to a dichotomous (true or false) question. To avoid floor and ceiling effects, we excluded statements that fell outside of this endorsement range.
The pilot study evaluated two feedback conditions that were later incorporated into the main study: an enhanced tentatively phrased feedback condition and an enhanced more assertively phrased feedback condition. For consistency, we refer to these conditions as “enhanced” because both use best practices outlined in the literature and are similar to the enhanced conditions used in the following experiments that are compared with a basic refutation condition that does not incorporate best practices. In both conditions of the pilot study, each statement was followed by a brief explanatory refutation or affirmation written in a conversational style. The enhanced tentative condition used cautious scientific language (e.g., “data do not support this statement”), whereas the enhanced assertive condition used more definitive language (e.g., “this statement is undeniably false”). Both conditions also incorporated several evidence-based misinformation correction strategies, including acknowledging why the misconception may seem plausible, providing corrective information, and referencing expert consensus (MacFarlane et al., 2021). The assertive versions contained the same substantive information as the tentative versions but differed in wording style and degree of certainty conveyed.
Participants read and made judgments about 28 enhanced tentatively worded and 28 more assertively worded refutations in a randomized order (where statements were also randomly assigned to be more tentatively worded or more assertively worded). After reading each refutation, participants rated it on ease of understanding (How easy to understand is the explanation above?), strength of argument (How strong and convincing is the explanation above?), and confidence conveyed (How confident does the above explanation sound?) using a sliding scale from 0 to 100.
Analytic plan
To examine how more tentatively worded and more assertively worded feedback differed on the three metrics—ease of understanding, strength of argument, and confidence conveyed—we conducted a series of three multilevel models. Multilevel modeling was chosen over paired t-tests or standard regression to account for the interdependent nature of the data, as indicated by high intraclass correlation (ICC) values for each metric. For each model, the outcome variable was the respective metric, the fixed effect was feedback type (more tentatively worded vs. more assertively worded), and nested random intercepts were included for participants within feedback type to account for variability in responses by condition within participants. Each model also included statement type (true vs. false), which improved model fit as assessed by Akaike information criterion (AIC), Bayesian information criterion (BIC), and likelihood ratio tests; however, moderation effects of statement type were tested and did not further improve model fit.
Results and discussion
For ease of understanding, there was no significant difference between enhanced tentatively worded refutations and assertively worded refutations (estimate = −0.93, SE = 0.62, z = −1.49, p = 0.136, d = −0.04). However, feedback addressing true statements was rated as easier to understand than feedback addressing false statements (estimate = 1.52, SE = 0.49, z = 3.10, p = 0.002, d = 0.07).
In contrast, refutation wording had a significant effect on perceived confidence. Enhanced tentatively worded refutations were rated as conveying less confidence than assertively worded refutations (estimate = −2.41, SE = 0.62, z = −3.91, p < 0.001, d = −0.11). Feedback for true statements was also perceived as conveying greater confidence than feedback for false statements (estimate = 3.07, SE = 0.46, z = 6.67, p < 0.001, d = 0.15).
A similar pattern emerged for perceived strength of argument. Type of refutation significantly influenced strength ratings, with enhanced tentatively worded feedback rated as less strong than assertively worded feedback (estimate = −1.84, SE = 0.63, z = −2.91, p = 0.004, d = −0.09). Feedback for true statements was again rated as stronger than feedback for false statements (estimate = 4.54, SE = 0.49, z = 9.23, p < 0.001, d = 0.21). Taken together, the results from this pilot study indicate that feedback containing more tentative phrasing common in scientific communication was perceived as conveying less confidence and as being less convincing than more assertive feedback containing more assertive phrasing, while not differing in perceived ease of understanding.
Experiment 1: Effectiveness of tentative phrasing in updating lay health misconceptions
In experiment 1, we compared the effectiveness of feedback containing common tentative phrases often used in scientific communication to feedback containing more assertive phrases. Given the results from the pilot study, we reasoned that more tentative phrases commonly used in scientific communication may come across as ambiguous or weak, compared with feedback containing more assertively worded phrases, commonly used by political figures or by general news outlets, which often uses definitive or exaggerated statements (e.g., “this is absolutely false”). Thus, we compared the effectiveness of feedback containing more tentative phrasing to feedback containing more assertive phrasing for updating health knowledge. We also assessed participants’ initial confidence about the accuracy of a health-related belief and their general health-related anxiety as potential moderators of their updating of their beliefs.
Methods
Transparency and openness
Materials and analysis codes for all experiments are available on the open science framework: https://osf.io/b54rn/?view_only=4dd4424226ea4093be687b0d9acdd2a6. Data were analyzed using R, version 4.3.1 (R Core Team, 2023) and the lme4, version 1.1.34 (Kuznetsova et al., 2017), and lmerTest, version 3.1.3 (Bates et al., 2015) packages. The experiments were not preregistered.
Methods
Participants
Based on prior work using a similar design (brief vs. detailed explanations; Swire et al., 2017), we selected F = 14.91 (ηp² = 0.12), 1–β = 0.80, and α = 0.05 to estimate the required sample size for detecting differences between the no-feedback and tentatively worded feedback conditions. The within-subjects binary outcome was modeled with a GLMM (logit link) including random intercepts for participants and items. Power analysis focused on the contrast between enhanced assertively worded and enhanced tentative-worded conditions. Using BUCSS in R (Anderson & Kelley, 2017) with 80% assurance and α = 0.05, this indicated a minimum sample of 116 participants.
A total of 138 undergraduate students from a large northeastern U.S. university initiated the study. Most were in their first or second year and had limited scientific training. As such, this sample represents a segment of the general public with a limited amount of scientific training. After excluding participants who did not complete the full study, the final dataset contained 117 participants (46.61% female, 50% male, 1.69% non-binary, <1% other; 53.39% white, 10.17% Asian-American, 7.78% Black, 4.23% South-East Asian, 4.23% Latino/Latina, 3.39% Middle Eastern, 2.54% East Asian, all other categories <2%; 18–43 years old, Mage = 20.42, SD = 4.04). Participants who completed both sessions were compensated with course credit. All experimental procedures were approved by the university’s institutional review board, and all participants provided informed consent.
Design and materials
The study used a within-subjects design with four conditions. Two conditions contained feedback using more tentatively phrased statements written to mimic how public health officials and scientists might present information; they included a basic tentative feedback condition and an enhanced tentative feedback condition (which used best practices, described further below). A third condition contained enhanced feedback presented in more assertively phrased statements. Finally, there was a no-feedback condition. For true statements, the feedback affirmed that the statement was true. For false statements, the feedback refuted the statement.
Stimuli consisted of 28 true and 28 false statements about health and nutrition used in the pilot study. For all feedback conditions, the statement was followed by a brief explanation written in a conversational tone that either affirmed the true statement or refuted the false statement, following procedures used in prior work (Lithander et al., 2021; Rich et al., 2017; Sitzman et al., 2021). The explanation was the same across the tentatively phrased feedback conditions for a given statement and contained two to three sentences and varied in length from 20 to 72 words (M = 36.11).
For example, for the statement, The flu shot can give you the flu, the feedback explanation was as follows: The injectable form of the flu vaccine cannot cause the flu because it does not contain a whole live flu virus. The vaccine has two basic types, one that contains a dead virus, and one that contains only a single gene from the virus. In both cases, virus replication is not possible. People may feel mildly ill after the shot; however, this is the body’s normal immune response to the injection. The dependent measure was accuracy when re-evaluating the veracity of the true and false statements after a 2-day delay. We selected the 2-day delay because this delay has been shown to be generally effective (e.g., Rich and Zaragoza, 2020) while limiting demand characteristics and short-term effects. By allowing time for memory consolidation before providing a correction, it is possible to assess whether misconceptions continue to influence beliefs despite correction (e.g., Ecker et al., 2020; Johnson and Seifert, 1994) and mimic real-world conditions in which misinformation is often corrected after some time has passed.
Basic tentative feedback
The basic tentatively phrased feedback condition included the phrases “data support this statement” (or “data do not support this statement”) or “there is substantial evidence to support this statement” (or “there is no evidence to support this statement”).
Enhanced tentative feedback
The enhanced tentatively phrased feedback condition contained the same phrases as in the basic condition but incorporated some best practices for correcting false information, including statements designed to disarm participants, discredit the misconception, provide correct information, and reference an expert source (for review, see MacFarlane et al., 2021).
For example, to refute the misconception that the flu shot can give you the flu, one of the enhanced tentatively phrased conditions stated: Data do not support this statement. This is easy to assume when you have mild symptoms after a vaccine. This response is your body starting to recognize components of the flu and developing antibodies against it. Virologists agree, though, that the flu shot cannot give you the actual flu. The injectable form of the flu vaccine cannot cause the flu because it does not contain a whole live flu virus. The vaccine comes in one of two forms, one that contains a dead virus, and one that contains only a single gene from the virus. In both cases, virus replication is not possible. The soreness you feel is just your body getting prepared in case you are exposed to the flu.
Enhanced more assertive feedback
The third feedback condition was the enhanced more assertive feedback condition. This condition contained the same components and information as the enhanced tentatively phrased condition but contained exaggerated and definitive language such as: “this is completely false,” “this is undeniably true,” and “this has been proven.”
For example, to refute the misconception that the flu shot can give you the flu, the enhanced assertively phrased feedback condition stated: This statement is undeniably false. But it’s understandable that some people assume this after having mild symptoms from a vaccine. This response is your body starting to recognize components of the flu and developing antibodies against it. All virologists know for certain that it is impossible for the flu shot to give you the actual flu. The injectable form of the flu vaccine cannot cause the flu because it does not contain a whole, live flu virus. The vaccine comes in one of two forms, one that contains a dead virus, and one that contains only a single gene from the virus. In both cases, virus replication is impossible. It is proven that the soreness you feel is just your body getting prepared in case you are exposed to the flu. This condition was developed based on phrases and communication styles used in common media and news sources.
Both enhanced feedback conditions also included an image along with the text to enhance learning (Brunyé et al., 2007; Clark and Paivio, 1991; Weinstein et al., 2018 but see Lithander et al., 2021). Selected images were related to the health topic described in each statement (such as a picture of a needle and a vial for the statement The flu shot can give you the flu) but did not include any graphs depicting scientific results. We refer to the feedback conditions aimed to test the effects of common tentative phrases used in scientific discourse as the more tentative conditions, and the condition with more absolute language as the more assertive condition.
Procedure
During the first session, statements were presented one at a time with true and false statements randomly intermixed. After reading each statement, participants indicated whether the statement was true or false, and indicated their level of confidence in their response on a scale from 0 (not at all confident) to 100 (absolutely confident). Because people may be more willing to update their knowledge if the health topic is particularly important to them, they were asked to rate the personal importance of the health topic on a scale from 0 (not at all important) to 100 (extremely important).
After evaluating all 56 statements, participants completed a distractor task. Immediately following the distractor task, all 56 statements were presented again in a random order, followed by one of the four within-subject feedback conditions; there were seven true statements and seven false statements in each condition. In the control (no-feedback) condition, the health statement was simply re-presented. In the feedback conditions, the false statement was re-presented followed by feedback and an explanation displayed for a minimum of 12 seconds before an arrow appeared at the bottom of the screen allowing participants to advance to the next screen. After statements and corrections (or statements alone in the control condition) had been presented, participants were reminded to return for the second session.
Two days later, participants completed the second session. Participants again evaluated the truth of the true and false statements from the first session, which were presented in a new random order. At the conclusion of the session, participants completed the 18-item Short Health Anxiety Inventory (Salkovskis et al., 2002) and a brief demographics questionnaire. All study questions were forced-choice to prevent missing data.
Analytic plan
The dependent variable was the accuracy of participants’ true or false responses to the health statements after the 2-day delay. Because we were interested in the effectiveness of the feedback on the correction of erroneous beliefs, the main analysis included responses to statements that were initially answered incorrectly (Lithander et al., 2021; Rich et al., 2017). Both true statements that participants believed were false, and false statements that participants believed were true were included in the analysis, all referred to as incorrect beliefs or misconceptions.
A multilevel logit regression model with binomial distribution was fitted to the data to investigate whether initial confidence, feedback condition, and rated importance predicted accuracy at posttest, as done by previous research (e.g., Lithander et al., 2021). Parameters were estimated using restricted maximum likelihood (REML). The resulting subset included a varying number of items for each participant, depending on participants’ accuracy on the initial test. A model with random effects for both item and participant were used to predict accuracy in statement judgments (Bates et al., 2015; Judd et al., 2017). Using this model allowed us to control for non-independent data points (each item was presented to every participant, but random effects correct for these within item dependencies). By doing so, the model accounts for variations across items, and trends that occur within each item. Our model was also conditioned on initial confidence (standardized), health anxiety (standardized), and whether the statement was true or false, as these predictors significantly improved model fit (assessed via AIC, BIC, and likelihood ratio tests). We also explored potential moderation effects of health anxiety, importance, and initial confidence. The health anxiety and importance moderation terms did not improve model fit, and the interaction with confidence was primarily driven by the control condition. To maintain parsimony and prioritize predictive performance, we retained these variables as covariates. Full moderation analyses are available on OSF. Importantly, the main study findings remain consistent across both approaches.
Results and discussion
Descriptive statistics
Students’ health anxiety scores ranged from 0 to 37, with higher numbers indicating higher health anxiety. Participants’ average health anxiety score was 13.55 (SD = 7.24). Average confidence in judgments across all health statements at the initial test was 61.26 (SD = 28.44). For items that were initially incorrect, initial confidence across all conditions was 60.05 (SD = 29.14), whereas confidence for statements that were initially correct was 62.26 (SD = 27.81). Prior to the study manipulation, students rated the statements as having an average importance of 53.17 (SD = 28.46), with importance ratings ranging from 0 to 100.
Initial beliefs
At the initial test, participants accurately indicated the truth of slightly over half of the statements (M = 54.66%, SD = 49.79%). Tukey pairwise comparisons showed no differences in initial accuracy across any of the four conditions (Control, M = 55.49%, SD = 49.71%; Basic more tentative, M = 54.58%, SD = 49.81%; Enhanced more tentative, M = 54.15%, SD = 49.84%; Enhanced more assertive, M = 54.40%, SD = 49.82%), ps > 0.56.
Effect of feedback condition
A multilevel logit regression model predicting accuracy at posttest yielded significant main effects of the feedback condition, initial confidence, and health anxiety (see Table 1).
Coefficients of logit multilevel model predicting accuracy at posttest for experiment 1.
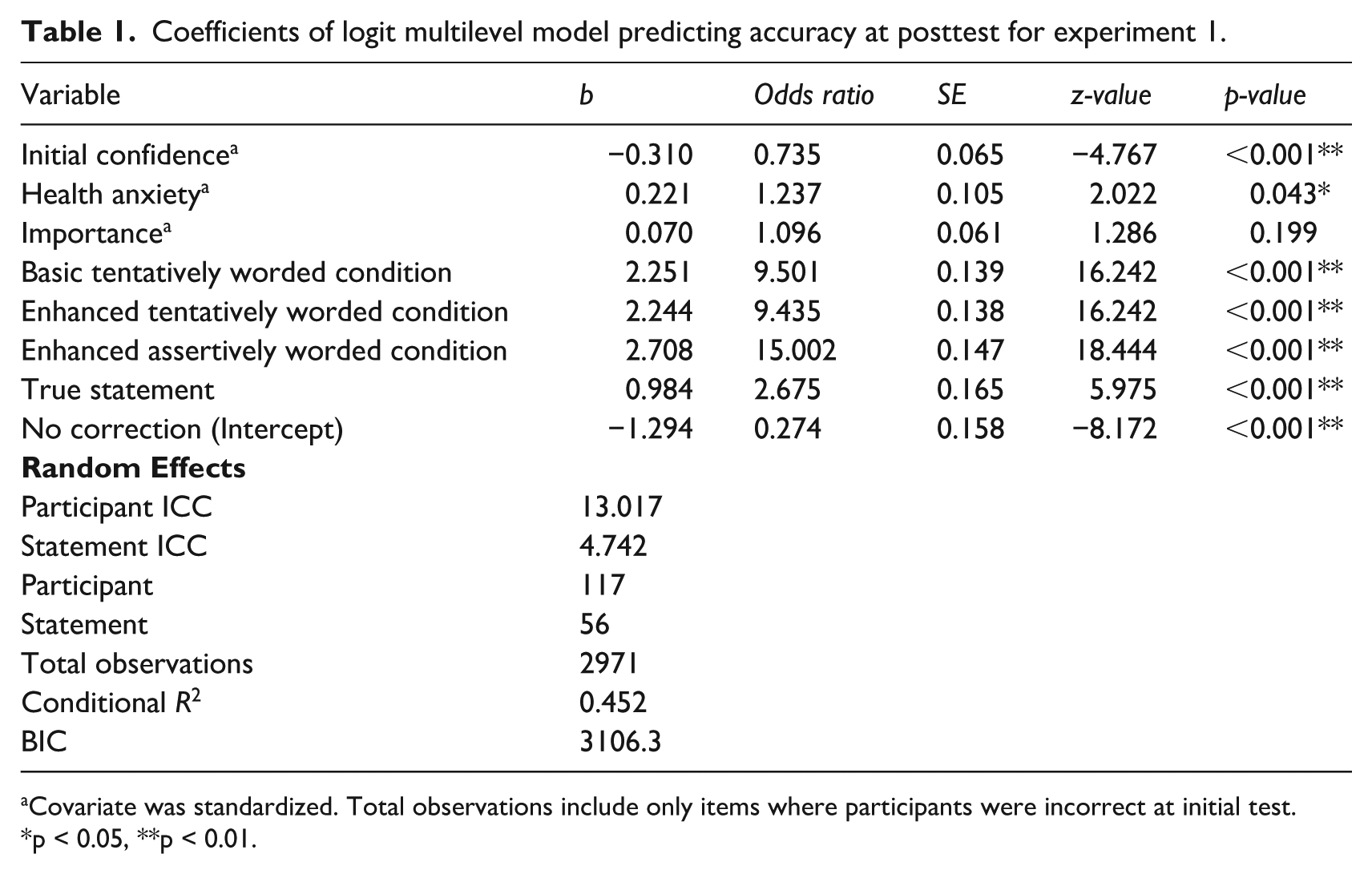
Covariate was standardized. Total observations include only items where participants were incorrect at initial test.
p < 0.05, **p < 0.01.
There was no significant effect of reported health topic importance on accuracy at posttest. Compared with the control condition, each of the three feedback conditions increased the logit probability of accuracy at posttest. Helmert-coded contrasts were used to compare feedback conditions at posttest. First, accuracy did not differ between the basic (M = 71.81) and enhanced tentative-phrase (M = 71.50) conditions (estimate = −0.01 log-odds, p = .96), indicating that adding enhanced phrasing provided no benefit beyond the basic version. Second, collapsing across these two conditions, feedback with more assertive phrasing (M = 77.91) yielded significantly greater posttest accuracy than feedback with more tentative phrasing (basic + enhanced, estimate = 0.92 log-odds, p < 0.001), corresponding to roughly 2.5 times higher odds of a correct response. Finally, all feedback treatments (basic, enhanced, and more assertive) substantially outperformed the control condition, (estimate = 7.20 log-odds, p < 0.001), corresponding to more than 1300 times higher odds of posttest accuracy. These findings suggest that enhanced tentative and basic tentative phrasing perform similarly. The more assertive phrasing led to higher accuracy than the more tentative versions, and all forms of feedback were highly effective relative to the control condition (see Figure 1). True statements increased the logit probability of accuracy at posttest by 0.984.
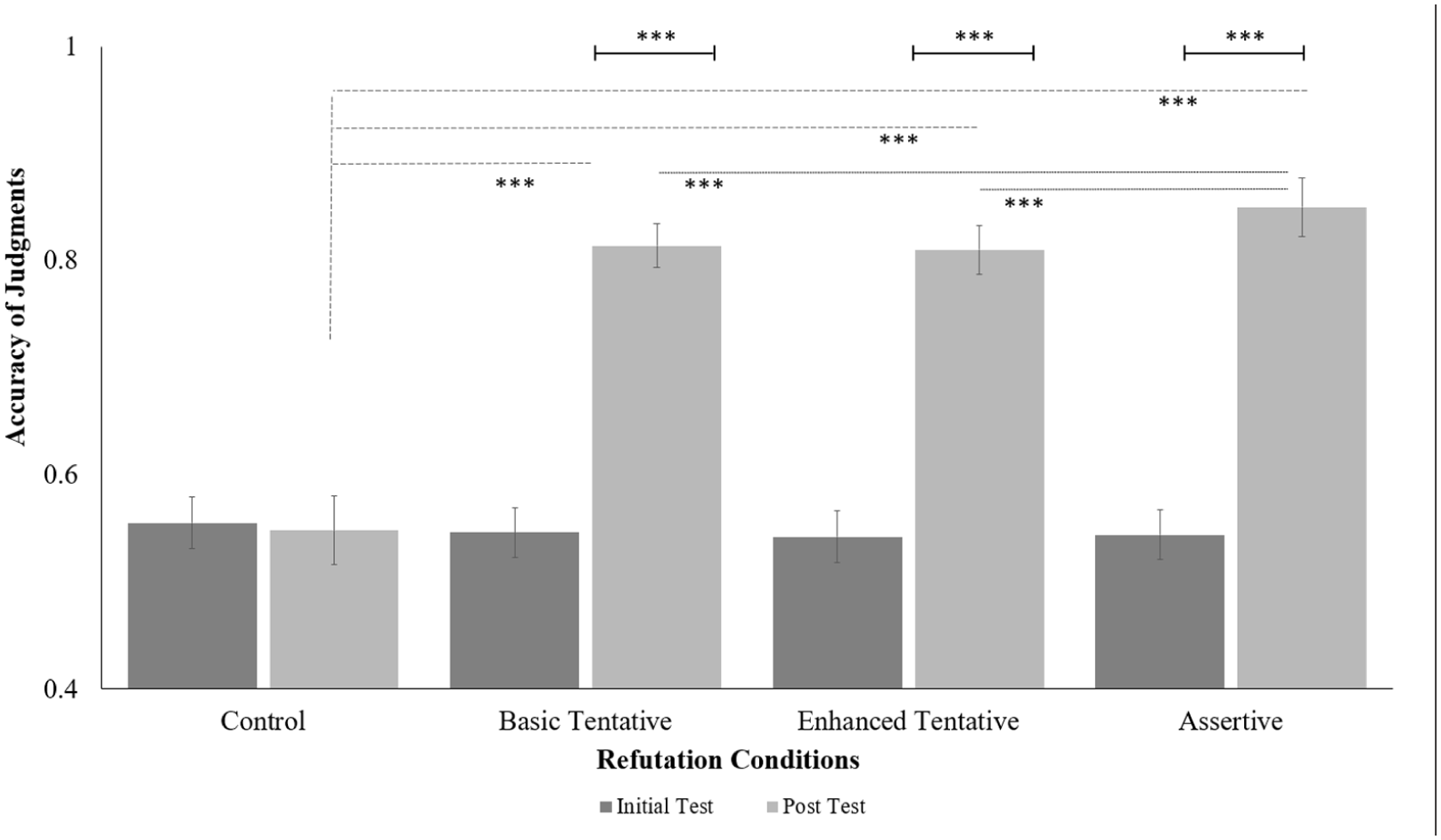
Average accuracy of judgments by condition at initial and posttest evaluations for experiment 1.
Higher initial confidence ratings during the initial test decreased the logit probability of accuracy at posttest. For each standard deviation increase in initial confidence rating, the logit probability of accuracy at posttest decreased by 0.378. We found a significant effect of health anxiety on accuracy at posttest. For each standard deviation increase in health anxiety, the logit probability of accuracy at posttest increased by 0.223.
Experiment 2: Replicating effect of phrasing on correcting lay health misconceptions
Results showed that more assertively worded feedback was more effective at correcting erroneous beliefs than more tentatively worded feedback (experiment 1), likely because more tentatively worded feedback is perceived as conveying less confidence and as being less convincing than more assertively worded feedback (pilot study). Experiment 2 was conducted to determine if the results from experiment 1 would replicate under conditions of greater initial misconceptions and would generalize to a more diverse online sample.
Methods
Participants
Based on the results of experiment 1 (t = −3.38, enhanced tentatively worded vs. enhanced assertively worded, 0.80 power, α = 0.05), a power analysis showed that 90 participants would be needed in experiment 2 to detect a difference between the more tentatively worded and more assertively worded feedback conditions using and assurance of 50% to account for uncertainty.
A total of 142 participants living in the United States were recruited from Amazon’s Mechanical Turk (Mturk) to test a broader demographic in terms of age and education relative to the Sona sample of undergraduate students. These participants were previously vetted by CloudResearch for high-quality work (Hauser et al., 2022; Rivera et al., 2022). Excluding those who did not complete the full study, the final dataset contained 119 participants (62.18% female, 36.97% male, <1% non-binary; 76.47% white, 8.40% Black, 5.04% Asian-American, all other categories <2%; 25–73 years old, Mage = 41.37, SD = 10.48). Participants who completed both sessions were financially compensated. All experimental procedures were approved by the local institutional review board, and all participants provided informed consent.
Design and materials
We selected the 41 most difficult items from experiment 1 and added 39 new items not used in the prior experiments. The final set of stimuli consisted of 40 true and 40 false statements about health and nutrition. Statements were compiled from internet sources detailing health information. By including a greater number of items and more difficult items, we aimed to increase the number of initial errors, leaving more room for corrections.
Procedure
The procedure was identical to that used in experiment 1.
Analytic plan
Analyses paralleled those in experiment 1. Mixed-effects logistic regression models predicted posttest accuracy from feedback condition, with random intercepts for participants and items. Health anxiety, importance, and initial confidence were examined as potential moderators. As in experiment 1, importance did not significantly moderate performance, and the health anxiety interaction was primarily driven by the control condition. In contrast to experiment 1, initial confidence moderated the effect of feedback in a condition-specific manner: higher initial confidence predicted lower accuracy in the enhanced more assertive-worded condition, but not in the tentative feedback conditions. Health anxiety and importance were retained as covariates to preserve model parsimony.
Results and discussion
Descriptive statistics
Participants’ health anxiety scores ranged from 1 to 39, with an average score of 14.81 (SD = 8.03). Average confidence in judgments across all health statements at the initial test was 65.66 (SD = 29.68). For items that were initially incorrect, initial confidence across all conditions was 60.75 (SD = 29.51), and average initial confidence for items that were initially correct was 70.32 (SD = 29.09). Prior to the study manipulation, students rated the statements as having an average importance of 57.30 (SD = 30.47), with a range of 0 to 100.
Initial beliefs
We compared initial accuracy across the four conditions (Control, M = 52.44%, SD = 49.95%; Basic more tentatively worded, M = 51.51%, SD = 49.99%; Enhanced more tentatively worded, M = 50.97%, SD = 50.00%; Enhanced more assertively worded, M = 50.21%, SD = 50.01%) using Tukey pairwise comparisons. There were no significant differences in accuracy across any of the conditions, ps > 0.12.
Effect of feedback condition
We used a mixed-effects logistic regression model predicting posttest accuracy with random intercepts for participants and items. The model included feedback condition, initial confidence, health anxiety, importance, and statement type as covariates. As in experiment 1, importance did not significantly predict posttest accuracy. Full estimates are reported in Table 2.
Coefficients of logit multilevel model predicting accuracy at posttest for experiment 2 (main effects model).
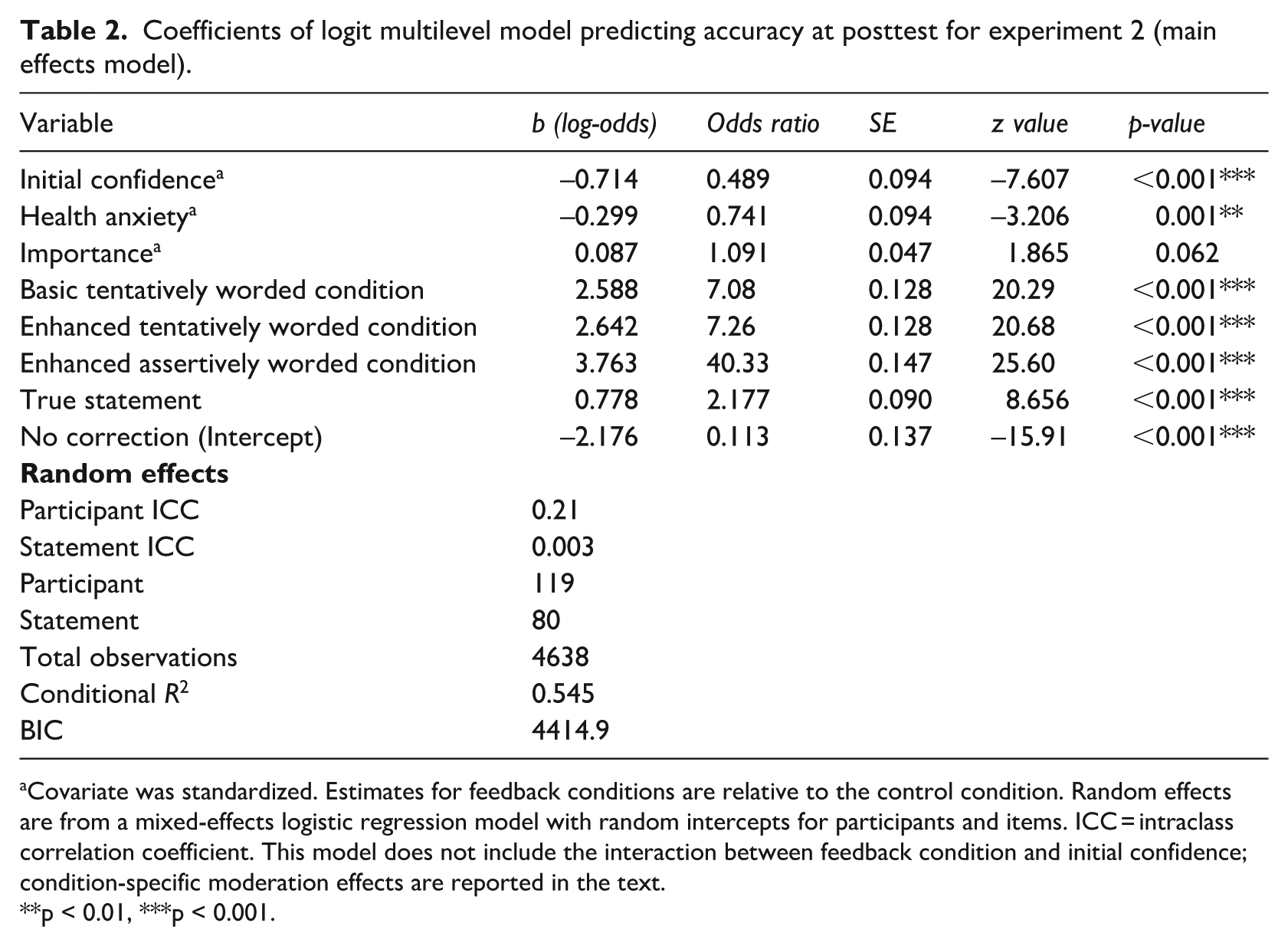
Covariate was standardized. Estimates for feedback conditions are relative to the control condition. Random effects are from a mixed-effects logistic regression model with random intercepts for participants and items. ICC = intraclass correlation coefficient. This model does not include the interaction between feedback condition and initial confidence; condition-specific moderation effects are reported in the text.
p < 0.01, ***p < 0.001.
Compared with the control condition (M = 19.3%), all feedback conditions significantly increased posttest accuracy. Participants who received basic tentatively worded feedback had a mean accuracy of 61.9%, corresponding to ~7.1 times higher odds of a correct response than control. Accuracy in the enhanced tentatively worded condition was 63.7%, corresponding to ~7.3 times higher odds relative to control. Participants who received enhanced assertively worded feedback had the highest accuracy (M = 77.9%), with ~40.3 times higher odds of a correct response compared with control (see Figure 2).
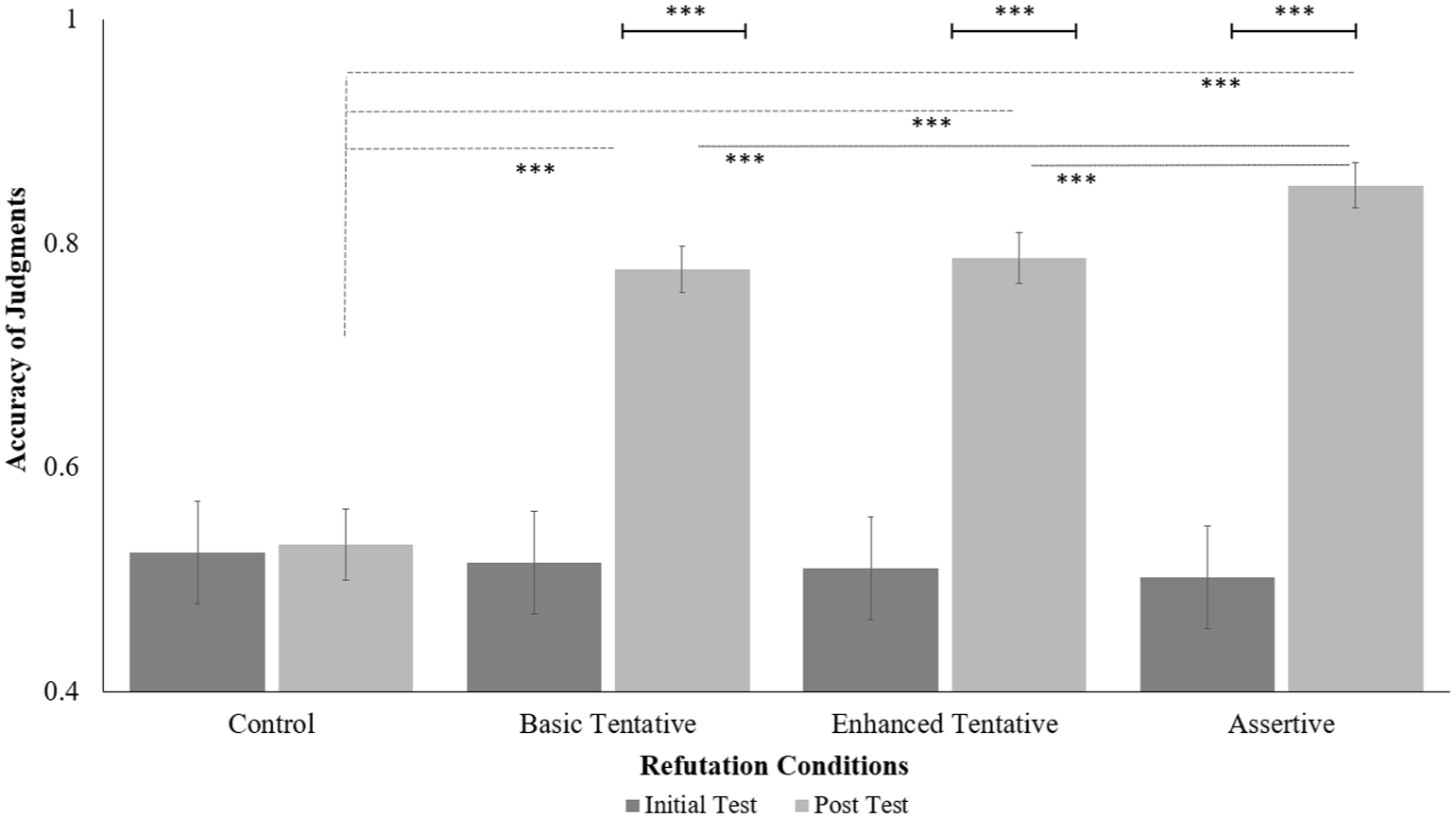
Average accuracy of judgments by condition at initial and posttest evaluations for experiment 2.
Helmert-coded contrasts indicated that accuracy did not differ between the basic and enhanced tentatively worded conditions (estimate = 0.06 log-odds, p = 0.55), suggesting no advantage of enhanced tentative phrasing. Collapsing across the two tentative conditions, enhanced assertively worded feedback produced significantly higher accuracy than tentative feedback (estimate = 2.03 log-odds, p < 0.001), corresponding to ~7.6 times higher odds of a correct response. Overall, all feedback conditions substantially outperformed the control condition (estimate = 9.06 log-odds, p < 0.001). These findings replicate the pattern observed in experiment 1.
Participants were more likely to correct erroneous responses to true statements than to false statements, with the logit probability increasing by 0.778 for true statements. Posttest accuracy was slightly lower across experimental conditions compared with experiment 1, likely due to differences in population, baseline accuracy, or the addition of more items; nevertheless, the main effect of enhanced assertively worded feedback was replicated.
Moderation by initial confidence
Unlike experiment 1, initial confidence moderated the effect of feedback in a condition-specific manner. Higher initial confidence was associated with lower posttest accuracy in the enhanced more assertively worded condition (b = −0.50, SE = 0.16, z = −3.18, p = 0.001), whereas the basic tentatively worded (b = −0.13, SE = 0.13, z = −1.08, p = 0.28) and enhanced tentatively worded (b = −0.02, SE = 0.12, z = −0.19, p = 0.85) conditions showed no significant moderation. Pairwise comparisons of slopes indicated that the moderation effect was significantly stronger in the enhanced more assertively worded condition than in the other two experimental feedback conditions (all p < 0.01). This finding suggests that participants with higher initial confidence were less likely to update their beliefs when receiving assertive feedback.
Effects of covariates
Across conditions, higher initial confidence predicted lower posttest accuracy overall (b = −0.71 log-odds per SD increase). Health anxiety also negatively predicted posttest accuracy (b = −0.30 per SD increase), whereas importance did not. The effect of health anxiety differed in direction from experiment 1, indicating that its influence should be interpreted with caution.
General discussion
Official health organizations and scientists often use certain scientific phrases to communicate health information and correct health misconceptions. This type of language is necessary to convey the nature of the available evidence, but it may be vulnerable to misinterpretation and exploitation (Oreskes and Conway, 2010). Despite frequent use, there has been little systematic research investigating how the use of tentatively worded scientific phrases (e.g., there is no evidence to suggest) might be interpreted and influence the likelihood that people will update their health knowledge. The current studies aimed to answer these questions.
Our results showed that the public is sensitive to uncertainty cues in health communication and that the language used to refute misconceptions can significantly influence the likelihood that people will update their beliefs. Specifically, we found that feedback using more tentative phrases common in scientific communication was effective for updating erroneous beliefs relative to no feedback but not as effective as feedback containing more assertively worded phrases. Providing basic feedback was sufficient for people to update their beliefs. In fact, more complex explanations (including statements designed to disarm participants, discredit the misconception, provide correct information, and reference an expert source) were not more effective than providing simple feedback, aligning with recent work demonstrating that simple corrections are sometimes sufficient to correct erroneous beliefs (e.g., Lithander et al., 2021; Walter and Tukachinsky, 2020).
The results from experiments 1 and 2 are consistent with previous research suggesting that there may be drawbacks to using tentative phrasing when communicating information to the public (MacFarlane et al., 2021). The pilot study illustrated one potential reason why feedback using tentative phrases common in scientific communication was less effective than feedback using more assertively worded phrases—because the commonly used tentative phrases are perceived as being weaker and conveying less confidence than more assertively worded feedback. This finding aligns with the literature suggesting that these common phrases are perceived as communicating uncertainty (Ma and Ma, 2022) and as less credible (Flemming et al., 2015). In addition, the finding is consistent with research showing that hedging increases uncertainty in a corrective message, thus reducing its efficacy (see Rashkin et al., 2017), whereas more confidently worded arguments increase persuasion (Petty et al., 2002).
The elaboration-likelihood model of Petty and Cacioppo (1986) also offers a way to interpret our findings. According to this model, how individuals make decisions (in this case, decisions about whether to update their health-related beliefs in response to different types of messages) depends on whether they carefully consider the relevant information (central route to persuasion) or whether they are influenced by incidental aspects of the communication, such as source characteristics or phrasing (peripheral route). Factors such as motivation (the personal relevance of the communicated topic) and the ability to evaluate and interpret the message without distractions make it more likely that an individual will engage in elaboration, and effortful thinking and base their evaluation of the topic on the quality of the content, resulting in a more durable belief that will be resistant to future counter-arguments. However, individuals may also be susceptible to incidental aspects of the message being communicated, such as, in the present study, the relative certainty or uncertainty with which the claim is couched. In the latter instance, participants are likely not processing the message on its merits but being overly influenced by how the message is phrased.
Although it is important for scientists to use language that accurately reflects the evolving and sometimes incomplete nature of evidence, our findings suggest that this practice may have unintended consequences when communicating with the public. Therefore, scientists might consider ways to emphasize a high level of confidence in scientific results whenever possible. Another option may be to reduce potential ambiguity in conveying results either by avoiding phrases such as “there is no evidence that . . .” or adding a disambiguating phrase, such as “despite several studies that have been done to look at X, there is no evidence that Y.” Explicitly educating the public, through interactive museum exhibits, for example, about how conclusions are arrived at by scientists, and beginning this education early on (i.e., with children in primary school) may help the public better appreciate that a nuanced characterization is often a more accurate one.
In addition to educating the public, it is important for scientists to consider how they communicate with the public. Many scientists endorse the deficit model when communicating with the public (Davies, 2008; Wallerstein and Duran, 2010). In the context of correcting misinformation, the deficit model suggests that a lack of knowledge can be resolved by merely conveying information (Choi et al., 2023; Houtman et al., 2021). However, research suggests that this is not the case and that it is important to provide an alternative explanation for the correction and to do so using simple language (for a review, see Ecker et al., 2022).
The current research indicates that these best practices should address the type of language used with an eye toward explaining what various scientific terms mean and clearly conveying the nature and strength of the evidence when attempting to update information. Future research should examine additional linguistic characteristics of the corrections, including the length of the feedback provided, or the type of framing—narrative versus statistical—or even the modality of the feedback (written or spoken). Our results clearly show that, considered as a whole, feedback about health misconceptions that is conveyed in a direct and assertive manner has a greater impact on knowledge updating than feedback that comes across as uncertain and tentative.
Initial confidence in beliefs played a role in predicting accuracy at posttest. In experiment 1, greater confidence in one’s incorrect health beliefs was associated with reduced belief updating across conditions, consistent with work showing that strongly held beliefs are resistant to change, although prior research on confidence and belief updating has yielded mixed results (Ecker et al., 2010; Lewandowsky et al., 2012). The results from experiment 2 both replicated this overall pattern and identified a boundary condition: confidence undermined belief updating primarily when feedback was assertively worded, but not when feedback was tentative-worded. These findings suggest that confidence does not uniformly impede belief revision, but instead interacts with features of corrective feedback. Assertive feedback may provoke resistance among individuals who already feel certain in their beliefs, whereas tentative feedback may allow confident individuals to consider corrective information without directly threatening prior beliefs. Many of the health statements reflected folk remedies, which may be well integrated into participants’ worldviews, further contributing to resistance under assertive feedback.
There are potential limitations to the current study. Although we think it highly unlikely that our findings can be attributed to the within-subjects design, it is possible that it may have made participants more sensitive to the manipulation. In future research, a between-subjects design would eliminate potential artifacts introduced by participants being aware of the semantic differences across conditions. In addition, the use of first- and second-year university students in experiment 1 limits generalizability to the general public. Although this is arguably a better sample than PhD students or more advanced academics for representing the general population, it is possible that even first-year students are likely to be more open to scientific reasoning and argumentation than non-academic segments of the population. Experiment 2, which used a more wide-ranging sample of participants recruited from Mturk, does not have this limitation. Another limitation is that we examined somewhat uncontroversial health misconceptions, so future research might examine how the type of feedback influences knowledge updating of more politicized or controversial health topics. In addition, future research might examine how long these corrective effects last. It is also possible that, though we found that participants were more likely to correctly answer statements about the truth of various misconceptions following assertive corrections than tentative ones, or no correction, changes in these responses could partly reflect demand characteristics rather than true changes to beliefs, a topic that future studies might attempt to decipher. Finally, we did not examine how the source of the health correction might influence belief revision, but other research has examined this topic in other domains and documented the importance of source trustworthiness on knowledge updating (see Guillory & Geraci, 2013).
For now, our findings offer some hope that, at least in the short term, misinformation can be corrected using tentatively phrased feedback that is commonly used in scientific communication. However, the results also show that feedback containing tentative phrases is less effective than feedback containing more assertive phrases. Therefore, it is important to assess ways to make scientific communication more effective and to communicate confidence in research findings whenever possible.
Footnotes
Authors’ note
Portions of these data were presented at the 2022 Annual Meeting of the Psychonomic Society and at the 2023 Annual Meeting of the Eastern Psychology Association.
Ethical considerations
This study received ethical approval from the University of Massachusetts Lowell IRB (Approval #21-184-GER-EXM) on November 2, 2021.
Consent to participate
All participants provided written informed consent prior to participating.
Author contributions
Renee Hunsberger was responsible for data curation, formal analysis, investigation, visualization, and writing-original draft and contributed to the conceptualization, methodology, validation, and support for writing, reviewing, and editing. Lisa Geraci was responsible for project administration, resources, and supervision and contributed to the conceptualization, methodology, validation, and writing-review & editing and support for writing the original draft. Jyotsna Vaid contributed to writing, reviewing, and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.