
Abstract
Craniomaxillofacial (CMF) bone defects pose significant regenerative challenges due to complex anatomy and physiological demands. While autologous bone grafting remains the gold standard, it is limited by donor-site morbidity and supply constraints. Mesoporous bioactive glass (MBG), characterized by its ordered nanoporous structure and superior bioactivity, offers a promising alternative. This review systematically analyzes the integration of MBG with 3D printing technologies, including direct ink writing, stereolithography, selective laser sintering, and fused deposition modeling. We critically evaluate physicochemical challenges such as rheological optimization and thermal devitrification while elucidating the “osteo-immune-vascular” axis orchestrated by these scaffolds. Specifically, we discuss how ionic dissolution products modulate macrophage polarization, stabilize hypoxia-inducible factor-1α (HIF-1α) to induce CD31ʰⁱEmcnʰⁱ vessel formation, and activate Wnt/β-catenin signaling. Despite promising preclinical data, clinical translation faces hurdles regarding regulatory approval and manufacturing standardization. Future developments in 4D printing, AI-driven inverse topology design, and organ-on-a-chip validation represent a paradigm shift from passive substitution to active regeneration, paving the way for the tissue-engineered reconstruction of complex CMF defects.
Keywords
Introduction
The clinical burden of craniomaxillofacial bone defects
The craniomaxillofacial (CMF) skeleton is a complex anatomical structure that not only dictates facial esthetics and identity but also serves critical physiological functions, including mastication, deglutition, phonation, and the protection of vital sensory organs 1 . However, the integrity of this system is frequently compromised by a myriad of pathological conditions. Epidemiologically, the burden of bone defects is staggering 2 . It is estimated that over 20 million patients worldwide suffer from devastating defects caused by trauma, tumor resection, infection, or congenital anomalies annually, with a global market for bone graft substitutes valued at approximately USD 3.1 billion in 2022 and projected to reach USD 4.6 billion by 20303,4.
Trauma remains a primary etiology. With the rising incidence of traffic accidents and sports-related injuries, facial fractures account for a significant proportion of emergency hospitalizations 3 . Furthermore, alveolar bone atrophy resulting from severe periodontitis—a condition affecting nearly 10–15% of the global adult population 5 —presents a ubiquitous challenge in restorative dentistry. Following tooth extraction, the alveolar ridge undergoes irreversible resorption, with vertical and horizontal bone loss reaching up to 40–60% within the first 2 years if left untreated 6 . This volumetric deficiency severely compromises the feasibility of dental implant placement, necessitating complex augmentation procedures 7 . In addition, congenital deformities such as cleft lip and palate, which occur in approximately 1 in 700 live births globally, require longitudinal, multi-stage bone grafting interventions throughout the patient’s growth and development 8 . These conditions not only impose a heavy economic burden on healthcare systems but also inflict profound psychological distress and quality-of-life deterioration on patients due to facial disfigurement and functional impairment.
The “gold standard” and its intrinsic limitations
To address these defects, the reconstruction of bone tissue requires a therapeutic strategy that provides mechanical stability while inducing osteogenesis. Historically and currently, autologous bone grafting (autografting) is widely regarded as the “gold standard” in clinical practice 9 . Harvested typically from the patient’s own iliac crest, fibula, rib, or calvarium, autografts possess the unique “triad” of essential properties: osteoconductivity (providing a scaffold), osteoinductivity (containing growth factors such as bone morphogenetic proteins [BMPs]), and osteogenicity (containing viable osteogenic cells) 10 .
Despite its superior biological performance, the clinical application of autografts is plagued by significant drawbacks. The most prominent limitation is donor-site morbidity, which is a direct consequence of the harvesting procedure. Clinical studies have reported complication rates at the iliac crest donor site ranging from 19.4% to 31% 11 . These complications include chronic pain, deep infection, hematoma, nerve injury (e.g., paresthesia of the lateral femoral cutaneous nerve), and cosmetic defects. Furthermore, the quantity of harvestable bone is finite, creating a supply-demand mismatch for massive defects (e.g., subtotal maxillectomy). Even when successfully implanted, autografts face the risk of unpredictable resorption, with volume loss reported as high as 50% in the long term, potentially leading to graft failure and the need for revision surgeries 12 .
Alternatives: Allografts and xenografts
To circumvent the morbidity associated with autografts, allogenic grafts (from human donors) and xenogenic grafts (derived from species such as bovine or porcine sources) have been extensively utilized10,13. While these alternatives eliminate the need for a secondary surgical site and offer unlimited supply, they are not without shortcomings. Allografts carry a risk, albeit low, of disease transmission (e.g., HIV, hepatitis) and may elicit an immune response leading to graft rejection or encapsulation 10 . Moreover, the rigorous sterilization processes (e.g., gamma irradiation, freeze-drying) required to ensure safety inevitably devitalize the tissue, destroying osteogenic cells and denaturing osteoinductive proteins, thereby reducing the graft to a primarily osteoconductive scaffold with reduced mechanical strength10,14.
Similarly, xenografts (e.g., deproteinized bovine bone mineral, DBBM) are widely used in dentistry due to their structural similarity to human bone mineral 15 . However, their high crystallinity often leads to an extremely slow degradation rate 16 . Clinical observations indicate that xenograft particles can remain encapsulated in the host tissue for years without being replaced by new bone, potentially interfering with the osseointegration of dental implants and altering the biomechanics of the regenerated region 17 . Consequently, there is an urgent and unmet clinical demand for synthetic, “off-the-shelf” biomaterials that are biocompatible, biodegradable, bioactive, and mechanically tailored to specific defects.
The evolution of bioactive glass
From 45S5 to mesoporous variants among synthetic bone substitutes, bioactive glasses (BGs) have garnered immense attention since the pioneering discovery of the 45S5 Bioglass® by Larry Hench in 1969 18 . Unlike inert bioceramics (e.g., alumina/zirconia) that trigger fibrous encapsulation, BGs are capable of forming a strong, interfacial bond with host bone 19 . This integration is mediated by a rapid sequence of surface reactions: ion exchange (Na+/Ca2+ with H+), formation of a silica-gel layer, and subsequent precipitation of an amorphous calcium phosphate layer that crystallizes into hydroxyapatite (HA), mimicking the mineral phase of natural bone 20 . Furthermore, the dissolution products of BGs (e.g., Si4+, Ca2+ ions) have been proven to biologically stimulate osteoblast (OB) gene expression 21 .
However, traditional melt-derived BGs suffer from inherent limitations, including low porosity, low specific surface area (<10 m2/g), and a tendency to crystallize during thermal processing, which diminishes bioactivity 22 . To overcome these hurdles, mesoporous bioactive glasses (MBGs) were developed in the early 2000s using supramolecular surfactant templates (e.g., P123, F127) via sol-gel chemistry 23 . MBGs are characterized by a highly ordered nanoporous channel structure (pore size 2–50 nm) and an exceptionally high specific surface area (300–1000 m2/g) 24 . This unique texture significantly enhances in vitro apatite-forming ability (often within hours) and provides a versatile platform for the loading and controlled delivery of therapeutic drugs, growth factors, or antibacterial agents, representing a quantum leap in bone tissue engineering materials 25 . Figure 1 illustrates the structural evolution from traditional BG to 3D-printed mesoporous scaffolds.
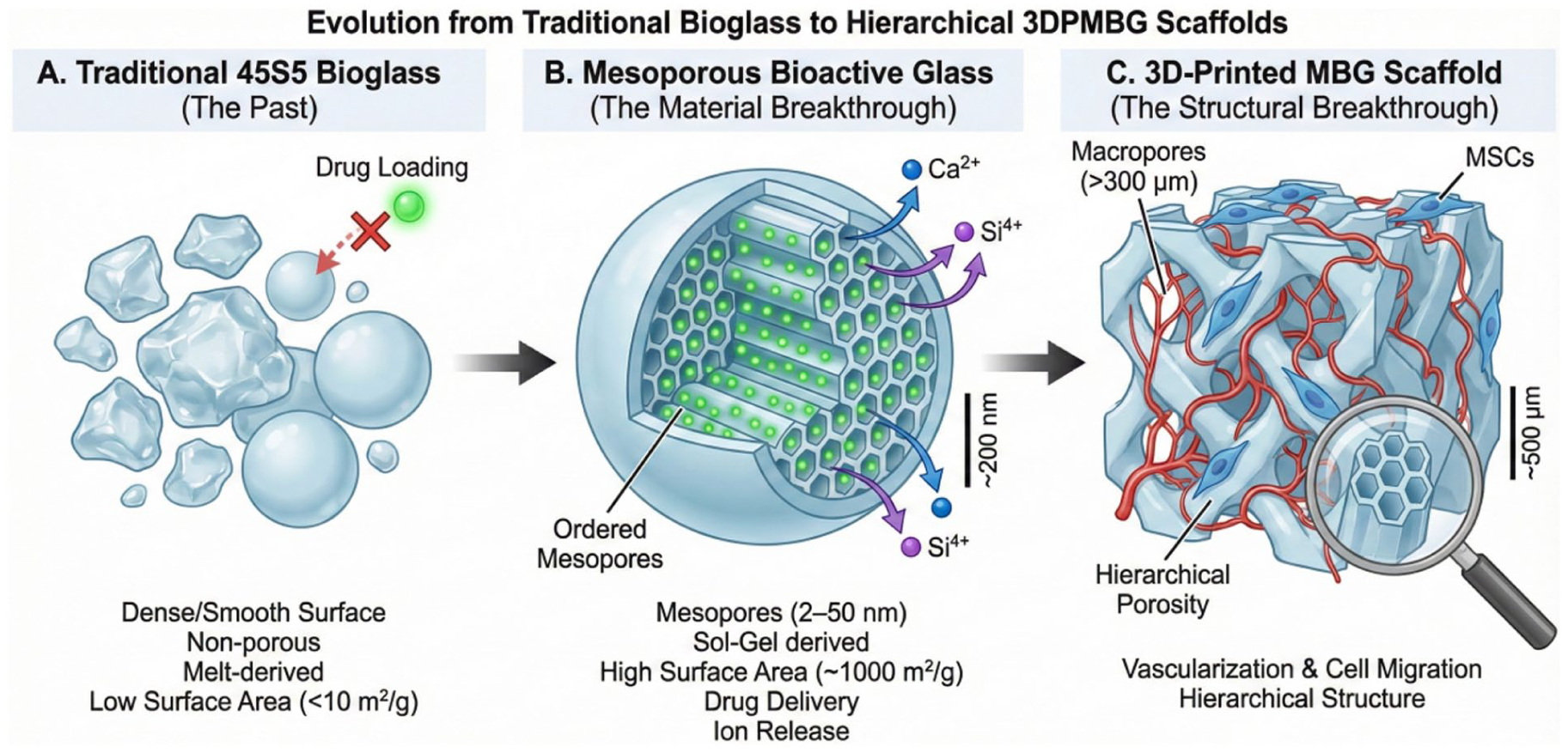
Schematic illustration of the structural evolution from traditional bioactive glass to 3D-printed mesoporous scaffolds. (a) Traditional 45S5 bioglass: characterized by a dense, non-porous surface with limited specific surface area, restricting its drug-loading capacity. (b) Mesoporous bioactive glass (MBG): synthesized via sol-gel templates, featuring highly ordered mesoporous channels (2–50 nm). This nanotexture significantly increases surface area, enabling the encapsulation and controlled release of therapeutic molecules. (c) Three-dimensionally printed MBG scaffold: by processing MBG into a 3D construct, a hierarchical pore architecture is achieved. The macroscopic pores (>300 μm) facilitate cell migration and vascular network formation (angiogenesis), while the intrinsic mesopores regulate drug delivery and ion release, realizing the synergy of structural support and biological functionalization.
The intersection of MBG and 3D printing
While MBG powders demonstrate excellent bioactivity, their translation into clinically usable 3D scaffolds has been hindered by the material’s inherent brittleness and the difficulty of shaping them into complex, patient-specific geometries required for CMF reconstruction 26 . Traditional fabrication methods (e.g., polyurethane foam replication) often yield scaffolds with poor mechanical reliability and uncontrolled pore architecture27,28.
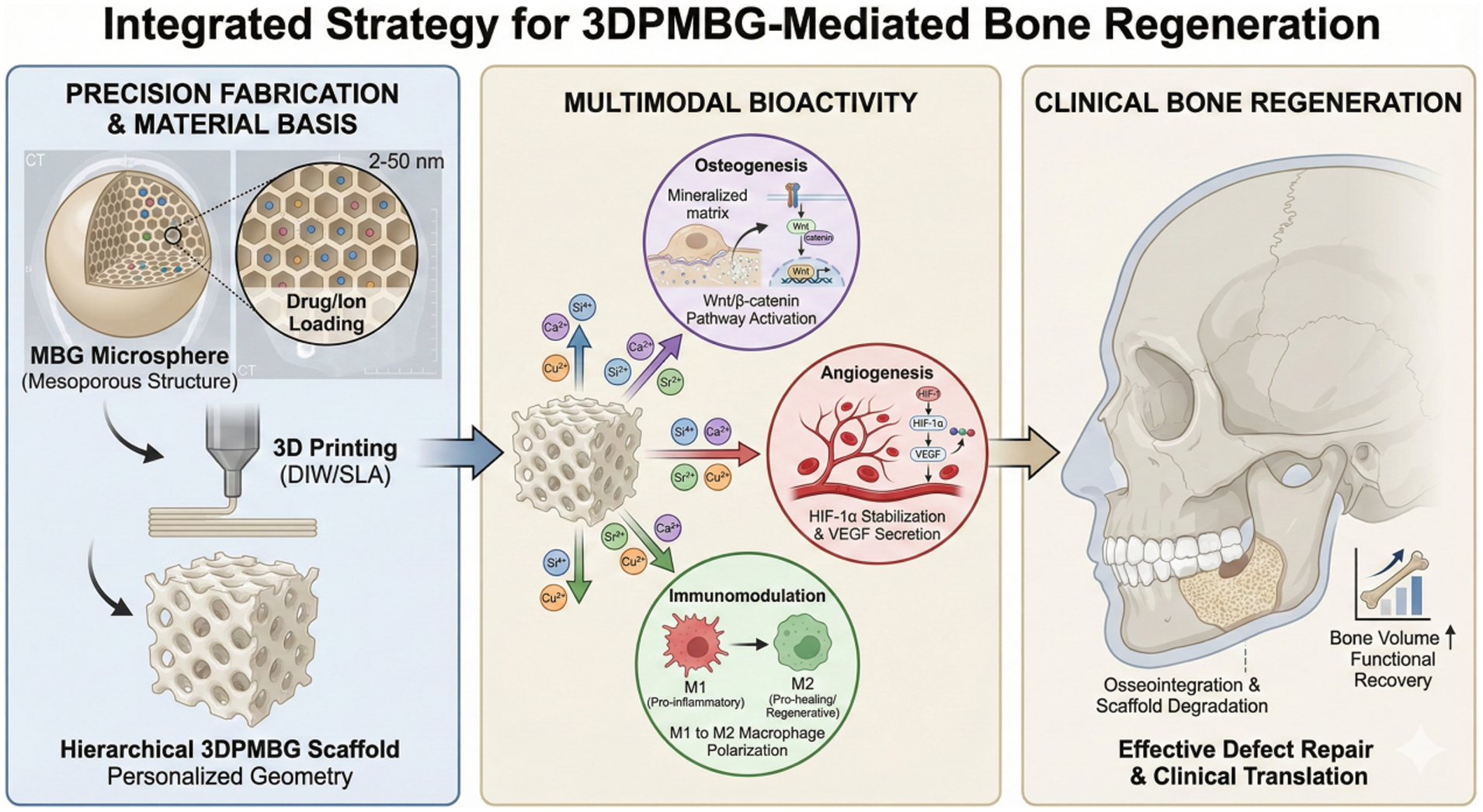
The advent of additive manufacturing (AM), or 3D printing, has revolutionized this landscape 29 . By integrating patient imaging data (computed tomography (CT)/magnetic resonance imaging (MRI)) with computer-aided design (CAD), 3D printing enables the fabrication of patient-specific implants (PSIs) that precisely fit irregular defects 29 . More importantly, 3D printing allows for the construction of scaffolds with hierarchical porosity: macroscopic pores (>300 μm) to facilitate vascular ingrowth and cell migration, and mesoscopic pores (2–50 nm) to enhance surface bioactivity and drug delivery22,27,30–32. When coupled with functional ion-doping (e.g., Sr2+, Cu2+, Ag+), 3D-printed MBG (3DPMBG) scaffolds emerge as a multifunctional platform capable of osteoinduction, angiogenesis, and immunomodulation33–36.
Scope of this review
This review aims to provide a comprehensive and critical analysis of the state-of-the-art in 3DPMBGs for CMF regeneration. We will systematically cover: (1) the material science evolution from traditional BG to MBG; (2) the adaptability and optimization of various 3D printing technologies (direct ink writing (DIW), stereolithography (SLA), digital light processing (DLP), selective laser sintering (SLS), fused deposition modeling (FDM)) for MBG; (3) the biological mechanisms underlying osteogenesis, angiogenesis, and immune regulation; and (4) the current status of preclinical validation and the roadmap for clinical translation. Particular emphasis will be placed on the challenges of regulatory approval and standardization, identifying the gaps that must be bridged to move this promising technology from the bench to the bedside.
Methodology and literature search strategy
To ensure a comprehensive and objective synthesis of the current literature, a structured literature search was conducted utilizing systematic review principles to support this comprehensive narrative review.
Search strategy
An extensive electronic literature search was performed across primary scientific databases, including PubMed, Web of Science, Scopus, and Google Scholar. The search timeframe encompassed articles published from inception up to February 2026, with a particular emphasis on publications from the last decade to capture the latest advancements in AM. The search strategy utilized Boolean operators (AND, OR) to combine the following key terms: (“Mesoporous bioactive glass” OR “MBG” OR “mesoporous glass”) AND (“3D printing” OR “additive manufacturing” OR “rapid prototyping” OR “bioprinting”) AND (“craniomaxillofacial” OR “maxillofacial” OR “oral” OR “dental” OR “alveolar” OR “bone regeneration” OR “osteogenesis” OR “angiogenesis” OR “macrophage polarization”).
Inclusion and exclusion criteria
To ensure the relevance and quality of the synthesized data, strict inclusion and exclusion criteria were applied.
Inclusion criteria: (1) Peer-reviewed original research articles (both in vitro and in vivo studies); (2) studies specifically utilizing 3DPMBG-based scaffolds (pure or composites); (3) studies reporting on bone tissue engineering, particularly in CMF or load-bearing applications; and (4) articles published in English.
Exclusion criteria: (1) non-English publications; (2) conference abstracts, editorials, or unpublished reports lacking peer review; (3) studies focusing solely on traditional melt-derived BGs (e.g., 45S5) without a mesoporous structure or 3D-printed architecture; and (4) studies exclusively investigating soft-tissue repair without a bone-regeneration component.
Quality assessment and data extraction
The quality of the included preclinical studies was critically evaluated based on experimental design, the presence of appropriate control groups (e.g., autografts, blank defects, or traditional bioceramics), and the reproducibility of the 3D printing parameters. Furthermore, the translational potential of the studies was assessed by prioritizing in vivo experiments that utilized critical-sized defect models (e.g., rat calvarial, rabbit femoral, or porcine models) and provided robust histomorphometric and radiological (micro-CT) quantitative data.
Material science and advanced AM strategies
The transition of MBG from laboratory powders to clinically viable implants is significantly facilitated by the evolution of AM. Understanding the fundamental materials science underlying these processes—specifically the rheological, photochemical, and thermodynamic interactions between the inorganic glass phase and the printing matrix—is crucial for optimizing scaffold performance.
Unlike traditional subtractive manufacturing or casting, AM builds scaffolds layer-by-layer based on computer-aided design/computer-aided manufacturing (CAD/CAM) digital models, enabling the fabrication of PSIs with complex geometries that perfectly match CMF defects27,37. More critically, AM allows for the precise control of internal pore architecture—specifically the construction of triply periodic minimal surface (TPMS) structures (e.g., gyroid, diamond). These mathematically defined architectures optimize the trade-off between mechanical strength and permeability, facilitating superior biological mass transport compared to traditional grid-like structures 38 .
However, adapting MBG—a brittle, inorganic silicate material—to 3D printing processes presents significant physicochemical challenges. The following sections critically analyze the four mainstream AM strategies: DIW, SLA/DLP, SLS, and FDM, focusing on their ink/resin formulations, printing mechanisms, and material-process interactions. Figure 2 provides a schematic comparison of these four mainstream AM strategies.
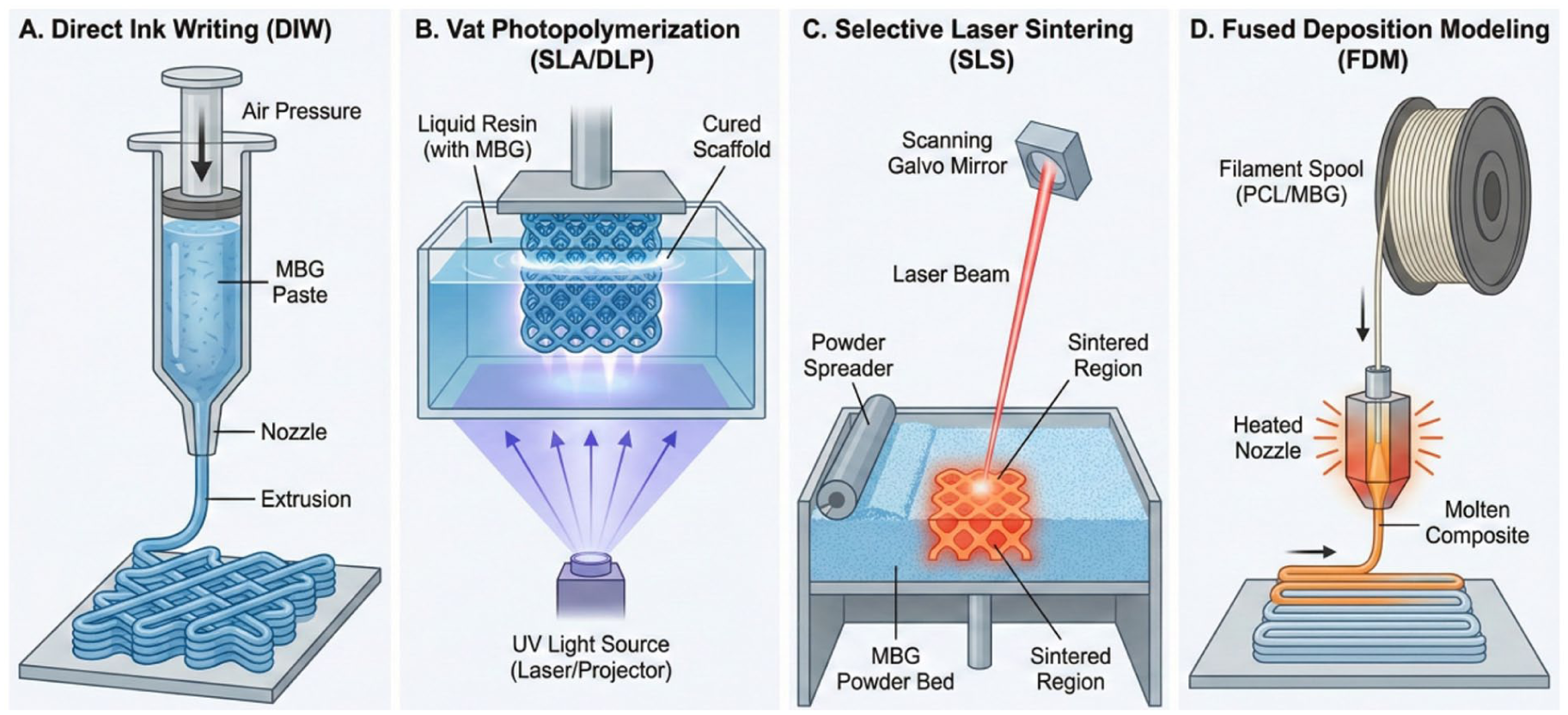
Schematic comparison of the four mainstream additive manufacturing strategies for fabricating mesoporous bioactive glass (MBG)-based scaffolds. (a) Direct ink writing (DIW): room-temperature extrusion of viscoelastic MBG pastes, ideal for drug loading but limited in resolution. (b) Vat photopolymerization (stereolithography/digital light processing): light-induced curing of MBG-loaded photosensitive resins, enabling high-resolution triply periodic minimal surface structures. (c) Selective laser sintering (SLS): laser fusion of MBG powder beds without binders, though risking devitrification. (d) Fused deposition modeling (FDM): melt extrusion of thermoplastic/MBG composite filaments, providing toughness but masking surface bioactivity.
DIW: The rheological balancing act
DIW, also known as robocasting, is currently the most widely investigated technique for fabricating MBG scaffolds due to its cost-effectiveness, material versatility, and ambient processing conditions39–41.
Mechanism and ink formulation
In DIW, a colloidal ink (paste) containing MBG powders is extruded through a micro-nozzle (typically 200–600 μm) under pneumatic or mechanical pressure. The success of DIW hinges entirely on the rheological properties of the ink. A printable MBG ink must exhibit shear-thinning behavior (viscosity decreases under shear stress to flow through the nozzle) and rapid thixotropic recovery (viscosity increases immediately after deposition to maintain shape) 27 . To achieve this, MBG powders are mixed with a liquid carrier and organic binders. Traditional binders include polyvinyl alcohol (PVA), methylcellulose, or Pluronic F-12742,43. Pluronic F-127 is particularly popular as a “universal template” because it serves a dual role: it acts as a viscoelastic agent for printing and as a mesopore template during synthesis 44 .
Challenges and optimization
A major limitation of DIW is the trade-off between solid loading and printability. High solid loading (>40 vol%) is desirable to reduce sintering shrinkage and enhance mechanical strength, but it dramatically increases viscosity, leading to nozzle clogging 45 . Conversely, low solid loading results in excessive shrinkage (up to 30–40% linearly) and warping during the post-sintering debinding phase46,47.
Recent advances have focused on “Green Printing” strategies. In the context of 3DPMBG, “Green Printing” refers to fabrication processes that offer both environmental sustainability (by eliminating volatile organic solvents) and biological safety (by avoiding cytotoxic degradation products). Traditional DIW relies heavily on organic binders (e.g., Pluronic F-127, PVA) to achieve printability. However, removing these polymeric binders requires high-temperature sintering. This burnout process not only risks thermal devitrification but also causes excessive volumetric shrinkage (often exceeding 30%) as the bulky organic phase is volatilized 42 . Furthermore, incomplete debinding can leave behind cytotoxic carbon residues that trigger severe foreign body reactions (FBRs) in vivo 48 .
To circumvent these fundamental drawbacks, recent research has pioneered the development of pure inorganic colloidal inks. The underlying mechanism of these “binder-free” inks relies on finely tuning the electrostatic interactions (e.g., zeta potential) and hydrogen bonding between the MBG nanoparticles and an aqueous dispersion medium, creating a printable thixotropic hydrogel without any organic additives 49 . Because the structural integrity is maintained by dense nanoparticle networking rather than a temporary polymer matrix, the printed scaffolds undergo significantly less shrinkage during post-processing. More importantly, this approach entirely eliminates the generation of toxic carbon residues. This latest work (2025) further advanced this technology, enabling the consolidation of mechanically robust MBG scaffolds at low or room temperatures. This represents a significant advantage over traditional organic binders, as it completely avoids the high-temperature sintering (>1000°C) that typically destroys the intrinsic mesoporous architecture and the amorphous bioactive phase of MBG 49 .
Resolution limit
The resolution of DIW is dictated by the nozzle diameter (typically >200 μm) and the “die swell” effect of the extruded filament. While sufficient for macroscopic bone ingrowth, DIW struggles to produce the intricate, micron-level surface features possible with light-based methods50,51.
Vat photopolymerization (SLA and DLP): Precision meets chemistry
SLA and DLP represent the pinnacle of resolution in ceramic 3D printing. These techniques utilize a photosensitive resin loaded with MBG particles, which is cured layer-by-layer using an ultraviolet (UV) laser (SLA) or a projected light mask (DLP)52,53.
Photochemical mechanism
Since pure MBG is not photosensitive, the surface of MBG particles must be functionalized. A common strategy involves grafting a silane coupling agent, such as 3-(trimethoxysilyl) propyl methacrylate (TMSPMA), onto the glass network 54 . The methacrylate groups (C=C bonds) on the surface then copolymerize with the resin monomers, such as 1,6-hexanediol diacrylate (HDDA) and poly(ethylene glycol) diacrylate (PEGDA), under UV irradiation, covalently linking the ceramic phase to the polymer matrix 55 .
The scattering challenge
The “Achilles’ heel” of printing MBG via SLA/DLP is the refractive index (RI) mismatch53,56. The RI of silicate glass (~1.45–1.50) often differs from that of resin 57 . This mismatch causes significant light scattering, which limits the cure depth (Beer-Lambert law) and broadens the cured spot, reducing lateral resolution. High solid loading exacerbates this scattering, often leading to delamination or incomplete curing53,56. To mitigate this, researchers are optimizing resin formulations to match the RI of MBG or developing “top-down” printing approaches where the platform moves downward into a shallow vat to minimize the required penetration depth 58 .
Structural advantages
Despite formulation difficulties, SLA/DLP can fabricate structures with strut sizes as small as 20–50 μm59,60. At the cellular level, this micron-scale resolution is biologically critical for in vivo functionality. Cells interact with their microenvironment via mechanotransduction; providing structural features that match the scale of a single OB (~20–30 μm) which maximizes focal adhesion formation and provides specific local curvatures that drive osteogenic differentiation 61 . Furthermore, because native capillaries are approximately 5–10 μm in diameter, these high-resolution micro-architectures provide the necessary spatial confinement to guide endothelial cell (EC) alignment and accelerate functional angiogenesis 62 . This capability allows for the creation of anisotropic structures that mimic the trabecular orientation of natural alveolar bone or the incorporation of internal micro-channels designed for nerve guidance, which is impossible with the macroscopic extrusion of DIW59,63.
SLS: The thermal dilemma
SLS employs a high-energy laser (CO2 or fiber laser) to selectively fuse particles in a powder bed. Unlike DIW and SLA, SLS does not necessarily require a binder, offering a direct path to pure ceramic scaffolds 64 .
Thermodynamics and crystallization
The primary challenge in SLS of BG is the thermal window40,65. MBG is a non-crystalline (amorphous) solid 65 . The high instantaneous energy of the laser can induce devitrification (crystallization), transforming the bioactive amorphous phase into crystalline phases like wollastonite (β-CaSiO3) or cristobalite 65 . While crystallization increases mechanical strength, it significantly reduces biodegradation rates and bioactivity, as the ion release from a crystalline lattice is much slower than that from a glass network 33 . Optimization of laser power, scan speed, and hatch spacing is critical to achieve “liquid phase sintering” where particles neck together without fully melting or crystallizing40,65. However, the inherent porosity of SLS parts (due to powder packing limits) often results in lower mechanical strength than sintered SLA parts26,40.
FDM: Composite solutions
FDM (or FFF) is the most accessible 3D printing technology, typically using thermoplastic filaments, such as polycaprolactone (PCL) and poly(lactic acid) (PLA). For bone regeneration, MBG is incorporated as a filler to create polymer/ceramic composites66,67.
The “masking effect”
While FDM scaffolds are tough and flexible (mimicking collagen fibers), a major drawback is the polymeric masking effect. The hydrophobic polymer matrix tends to encapsulate the bioactive MBG particles, preventing their direct contact with body fluids. This severely delays the onset of ion release and apatite formation 66 . To counter this, post-processing strategies such as plasma etching or using porogens (e.g., PEG, salt) that leach out to create surface micropores are employed to expose the MBG particles 68 . Recent “low-temperature FDM” modifications allow for the printing of PCL/MBG pastes at 60–80°C, preventing the thermal degradation of loaded growth factors 69 .
Comparative analysis of AM technologies
The selection of a specific 3D printing technology for CMF regeneration is a decision matrix involving resolution, mechanical requirements, and biological functionality. Table 1 summarizes the key technical parameters, reported mechanical and biological outcomes from the literature, and clinical applicability of these methods to provide a comprehensive comparative analysis.
Quantitative and comparative analysis of mainstream additive manufacturing technologies for MBG-based scaffolds.
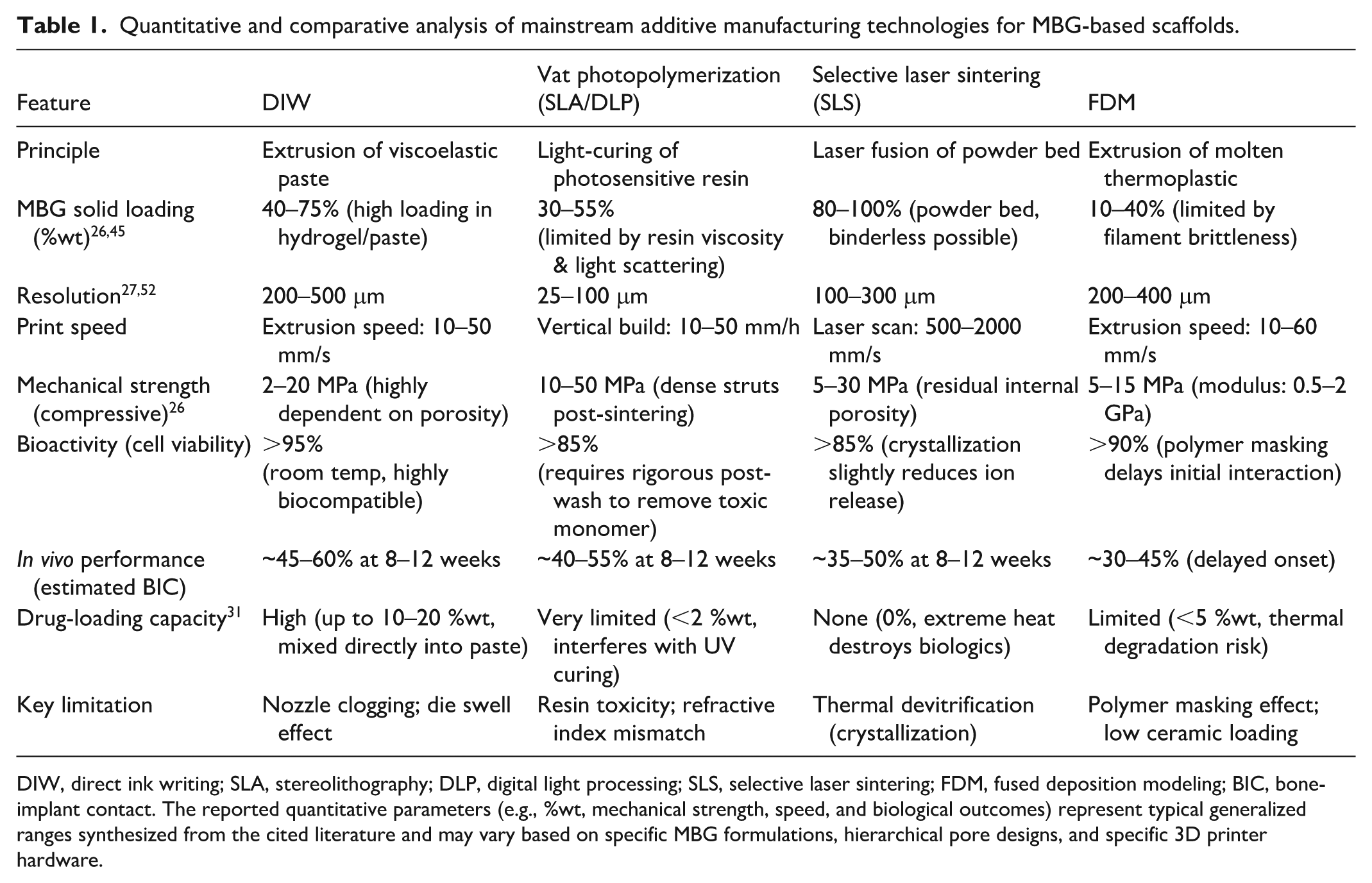
DIW, direct ink writing; SLA, stereolithography; DLP, digital light processing; SLS, selective laser sintering; FDM, fused deposition modeling; BIC, bone-implant contact. The reported quantitative parameters (e.g., %wt, mechanical strength, speed, and biological outcomes) represent typical generalized ranges synthesized from the cited literature and may vary based on specific MBG formulations, hierarchical pore designs, and specific 3D printer hardware.
Summary and selection strategy
For alveolar ridge preservation where geometry is small but intricate, DLP is increasingly preferred due to its ability to print highly permeable gyroid structures that facilitate rapid vascularization.
Conversely, for large-volume mandibular defects requiring significant drug delivery (e.g., antibiotics for osteomyelitis), DIW remains the gold standard for drug and cell delivery. This is fundamentally dictated by its material-processing conditions. Unlike SLS or FDM, which involves extreme thermal processing that denatures delicate biologics, or SLA, which relies on cytotoxic photo-initiators and high-energy UV irradiation, DIW provides a mild, bio-friendly environment58,69. Because it operates via the room-temperature extrusion of aqueous or hydrogel-based pastes, high doses of heat-sensitive therapeutic agents, or even living cells, can be homogeneously mixed directly into the ink prior to printing without compromising their biological activity 51 . Future hybrid printers combining DIW (for drug delivery) and FDM (for mechanical frame) represent the next frontier in functional scaffold fabrication.
Biological mechanisms and molecular orchestration
The therapeutic efficacy of 3DPMBG extends far beyond its role as a passive void filler27,70. Upon implantation into the CMF defect, the scaffold initiates a dynamic, bidirectional dialogue with the host microenvironment 70 . This interaction is mediated primarily by the controlled degradation of the glass network, which releases a cascade of therapeutic ions (e.g., Si4+, Ca2+, Sr2+, Cu2+) while exposing a nanotopographically rich surface21,27. These physicochemical cues function as “inorganic growth factors,” orchestrating a complex sequence of biological events ranging from early immune modulation to late-stage bone remodeling21,70,71.
This section dissects the biological mechanisms of 3DPMBG into three interconnected axes, as depicted in Figure 3: (1) ionic regulation of osteogenesis, (2) angiogenic coupling and hypoxia mimicry, and (3) osteoimmunomodulation.
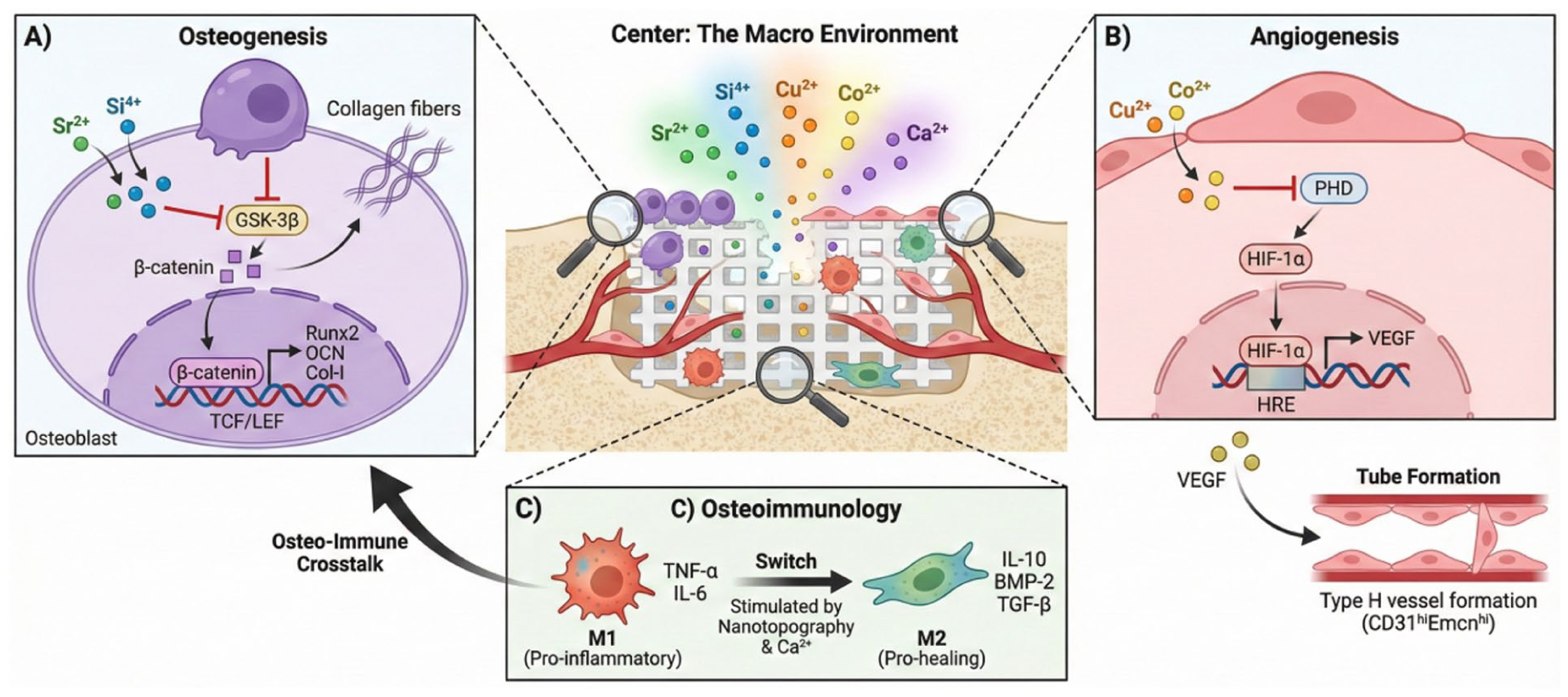
Schematic illustration of the molecular orchestration of bone regeneration by 3DPMBG scaffolds. (Center) The implanted scaffold creates a bioactive microenvironment via ionic release and nanotopographical cues. (a) Osteogenesis: released Sr2+ and Si4+ ions enter osteoprogenitor cells, inhibiting GSK-3β and stabilizing β-catenin. This activates the canonical Wnt signaling pathway, leading to the nuclear translocation of β-catenin and the upregulation of osteogenic genes (Runx2, OCN). (b) Angiogenesis: Cu2+ and Co2+ ions mimic a hypoxic environment by competitively inhibiting prolyl hydroxylase domain enzymes. This stabilizes hypoxia-inducible factor-1α (HIF-1α), which binds to hypoxia response elements (HRE) in the nucleus, triggering the secretion of vascular endothelial growth factor to promote endothelial tube formation and Type H vessel coupling. (c) Osteoimmunomodulation: The mesoporous nanotopography and ionic cues promote the polarization of macrophages from the pro-inflammatory M1 phenotype (secreting TNF-α) to the pro-healing M2 phenotype (secreting IL-10 and BMP-2), creating an immune-favorable niche for tissue repair.
Optimal MBG compositions and topological lattice configurations
The biological efficacy of 3DPMBG is fundamentally dictated by its multiscale design: the nanoscale elemental composition and the macroscale topological lattice.
Stoichiometric optimization of dopants
Regarding chemical composition, a high silica network (typically 60–80 mol% SiO2) is mandatory to maintain the ordered mesoporous channels and provide sufficient silanol (Si-OH) groups for rapid apatite nucleation 32 . For enhanced osteo-angiogenesis, trace element doping requires precise stoichiometric optimization. Efficacy must be perfectly balanced against potential heavy metal cytotoxicity or glass network disruption. The optimal doping windows and specific biological roles of common therapeutic ions (e.g., Sr, Cu, Co, Mg) are quantitatively summarized in Table 234,36.
Quantitative optimization of elemental compositions in MBG scaffolds.
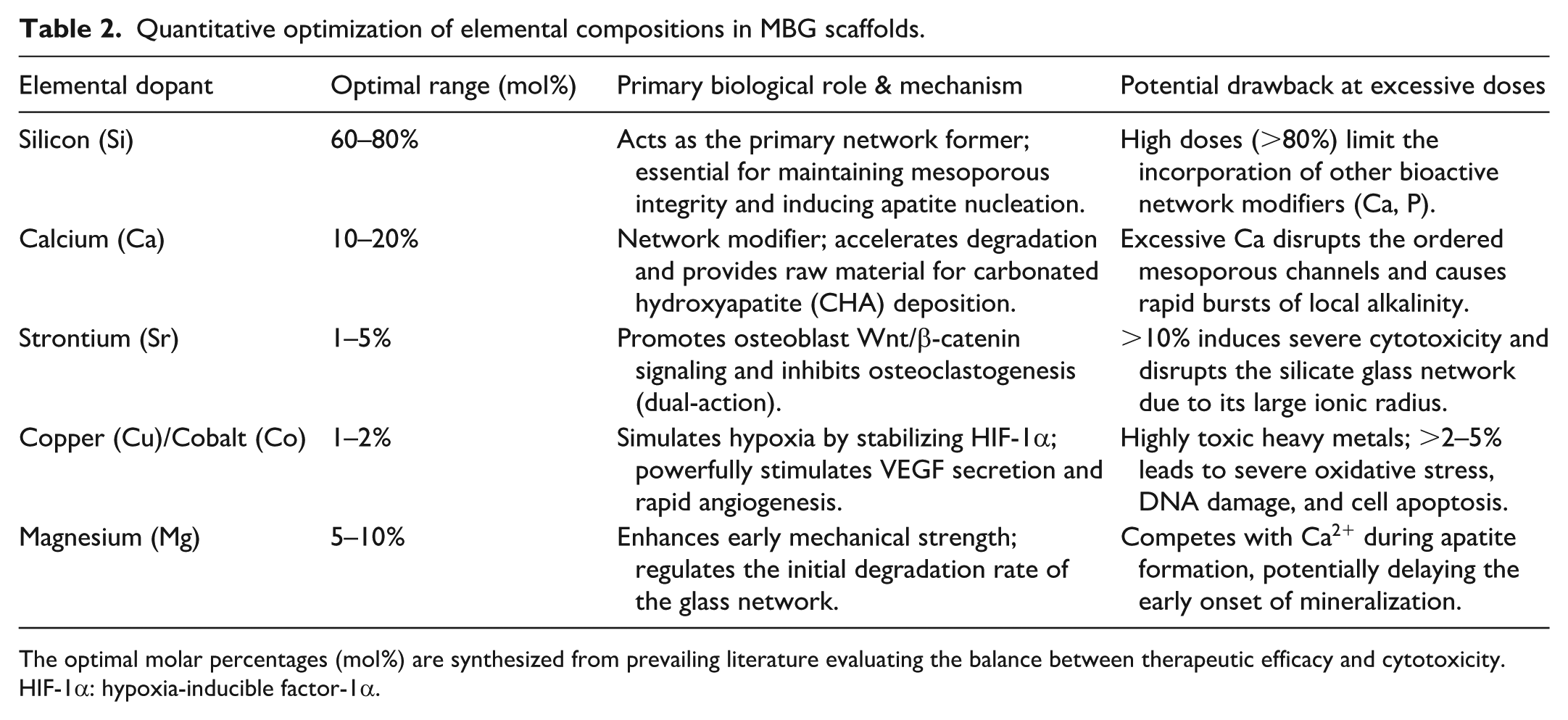
The optimal molar percentages (mol%) are synthesized from prevailing literature evaluating the balance between therapeutic efficacy and cytotoxicity. HIF-1α: hypoxia-inducible factor-1α.
Mathematical design of TPMS architectures
Beyond chemistry, the 3D topological configuration profoundly influences cellular mechanotransduction and fluid dynamics. While traditional orthogonal “woodpile” (grid) patterns are easily fabricated, advanced TPMS architectures are currently recognized as the optimal biomimetic geometries 38 . TPMS structures possess zero mean curvature, perfectly mimicking the continuous, anisotropic architecture of native trabecular bone. Mathematically, these complex topologies are generated using nodal approximations based on trigonometric parametric equations 38 . The three most prominently utilized TPMS structures in bone tissue engineering are the gyroid (G), diamond (D), and primitive (P) surfaces, defined by the following fundamental level-set equations (where x, y, and z are spatial coordinates and c defines the solid volume fraction):
Combined with an optimal macropore size of 300–500 μm, these mathematically derived TPMS lattices uniquely distribute localized stress, maximize fluid shear stress for OB mechanosensing, and provide ideal non-linear spatial geometry for rapid vascular network penetration 30 . A comparative analysis of these topological architectures is detailed in Table 3.
Comparative topological analysis of 3D printed lattice configurations.
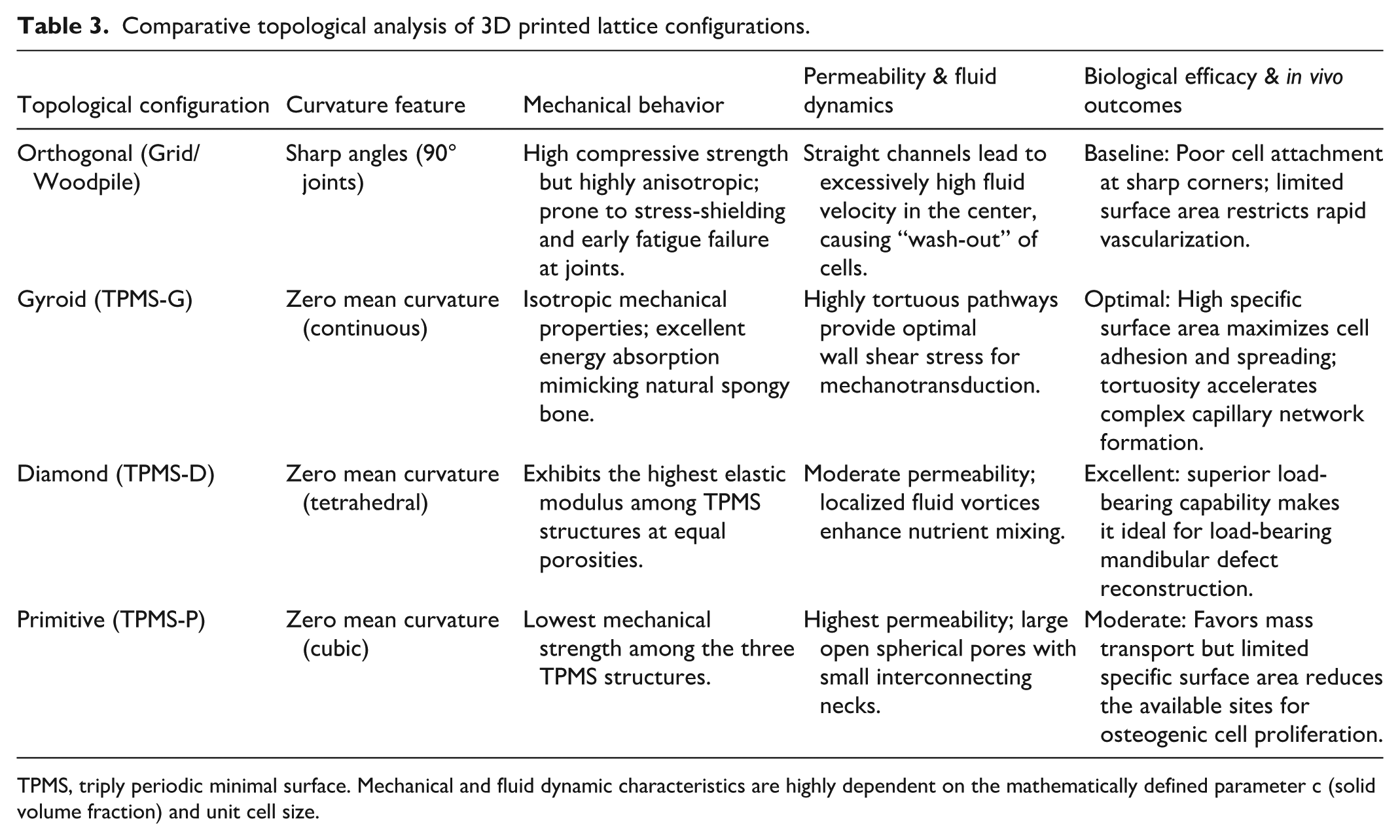
TPMS, triply periodic minimal surface. Mechanical and fluid dynamic characteristics are highly dependent on the mathematically defined parameter c (solid volume fraction) and unit cell size.
Ionic orchestration of osteogenesis
The osteogenic capacity of 3DPMBG is driven by the “ionic dissolution products” released into the extracellular matrix21,31. These ions are transported into cells via ion channels or endocytosis, where they trigger specific intracellular signaling pathways that govern the fate of mesenchymal stem cells (MSCs) and OBs21,72,73.
The silicon-calcium axis
The Hench mechanism: The fundamental bioactivity of MBG relies on the release of soluble silica species (Si(OH)4) and calcium ions (Ca2+)74,75. While Ca2+ is a ubiquitous second messenger 76 , soluble silicon has been identified as a potent mitogen for OBs 77 .
Mechanism
Silicon species enter the cell and stimulate the mitogen-activated protein kinase (MAPK) pathway, specifically phosphorylating ERK1/2. This activation leads to the nuclear translocation of transcription factors that upregulate cell cycle progression (Cyclin D1) and extracellular matrix synthesis (Collagen Type I)78,79. Simultaneously, the high local concentration of Ca2+ stimulates calcium-sensing receptors (CaSR) on the OB membrane, activating the phospholipase C (PLC) pathway to further enhance cell proliferation80,81.
Strontium (Sr2+): The dual-action modulator
Strontium is arguably the most valuable dopant for CMF regeneration due to its unique “dual-action” mechanism: it simultaneously promotes bone formation (anabolic) and inhibits bone resorption (anti-catabolic)82,83.
Anabolic pathway (Wnt/β-catenin)
Sr2+ ions function as agonists for the CaSR. Upon binding, Sr2+ activates the Wnt/β-catenin signaling pathway, a master regulator of osteogenesis. Activation of Wnt signaling inhibits glycogen synthase kinase-3β (GSK-3β), preventing the degradation of β-catenin. Stabilized β-catenin accumulates in the cytoplasm and translocates to the nucleus, where it binds to T-cell factor/lymphoid enhancer-binding factor (TCF/LEF) transcription factors to drive the expression of osteogenic master genes, including Runx2, Osterix (Osx), and osteocalcin (OCN)84–86.
Anti-catabolic pathway (RANKL/OPG ratio)
Sr2+ acts on the OB-osteoclast communication axis by upregulating the secretion of osteoprotegerin (OPG) and downregulating the expression of Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL). Since RANKL is essential for osteoclast differentiation and OPG is its decoy receptor, a high OPG/RANKL ratio effectively blocks osteoclastogenesis, thereby preserving existing bone mass—a critical feature for patients with osteoporotic alveolar bone83,87.
Magnesium (Mg2+) and zinc (Zn2+)
Magnesium and zinc ions contribute to osteogenic adhesion and bone matrix mineralization.
Magnesium (Mg2+)
As a cofactor for alkaline phosphatase (ALP), Mg2+ plays a pivotal role in the mineralization of the bone matrix. Furthermore, Mg2+ facilitates the initial adhesion of MSCs to the scaffold surface by upregulating the expression of integrins (α5β1), which bind to fibronectin absorbed on the MBG surface88,89.
Zinc (Zn2+)
Zinc is vital for the synthesis of protein and DNA. At the molecular level, Zn2+ prevents OB apoptosis by inhibiting the caspase-3 pathway. In addition, Zn2+ has been shown to enhance the synthesis of aminoacyl-tRNA synthetase, thereby promoting protein translation essential for collagen production90,91.
Angiogenic coupling: The “Type H” vessel hypothesis
Bone regeneration is metabolically demanding; no bone forms without blood. In large CMF defects, the core of the scaffold often fails due to hypoxia-induced necrosis. 3DPMBG addresses this by promoting rapid vascularization, specifically targeting CD31ʰⁱEmcnʰⁱ (Type H) capillaries, which are known to couple angiogenesis with osteogenesis92,93.
Hypoxia mimicry via copper (Cu2+) and cobalt (Co2+)
A sophisticated strategy to induce angiogenesis is “hypoxia mimicry.” Under normoxic conditions, hypoxia-inducible factor-1α (HIF-1α) is rapidly degraded by prolyl hydroxylase domain (PHD) enzymes94,95.
Molecular mechanism
Therapeutic ions like Cu2+ and Co2+ competitively inhibit PHD enzymes. This inhibition prevents the hydroxylation and subsequent ubiquitin-proteasome degradation of HIF-1α, leading to its accumulation in the cytoplasm even in the presence of oxygen 96 . Stabilized HIF-1α translocates to the nucleus and binds to hypoxia response elements (HRE), triggering the transcription of key angiogenic genes, most notably vascular endothelial growth factor (VEGF) and stromal cell-derived factor-1 (SDF-1) 97 .
Outcome
VEGF secreted by local cells (MSCs, OBs) acts paracrinely on ECs, stimulating their proliferation, migration, and tube formation into functional capillary networks within the macropores of the 3D scaffold98,99.
The crosstalk (angiocrine signaling)
The relationship is bidirectional. ECs stimulated by MBG dissolution products secrete angiocrine factors (e.g., Noggin, BMP-2) that further stimulate the osteogenic differentiation of pericytes and MSCs, creating a positive feedback loop that accelerates total tissue regeneration100,101.
Osteoimmunomodulation: From “bio-inert” to “immuno-active”
Traditionally, biomaterials were designed to be “bio-inert,” aiming to avoid the host immune response. However, modern “Osteoimmunology” dictates that the immune system is the primary orchestrator of healing 102 . The implantation of 3DPMBG inevitably triggers a foreign body response (FBR), where macrophages play the central role 103 .
Macrophage polarization (the M1/M2 switch)
Macrophages exhibit high plasticity and can polarize into two distinct phenotypes.
M1 phenotype (pro-inflammatory)
The M1 phenotype is characterized by the secretion of TNF-α, IL-1β, and IL-6. An initial, transient M1 phase is necessary to clear debris and prevent infection. However, prolonged M1 activation leads to chronic inflammation and the formation of a fibrous capsule that isolates the scaffold from the bone, leading to failure104,105.
M2 phenotype (anti-inflammatory/pro-healing)
The M2 phenotype is characterized by the expression of CD206 and Arg-1 and the secretion of IL-10, TGF-β, and BMP-2. This phenotype is directly associated with tissue repair and bone deposition104,106.
Mechanism of MBG-induced immunomodulation
3DPMBG modulates macrophage polarization through both chemical and physical cues84,107.
Ionic cues
Dissolution products, particularly calcium and strontium, have been shown to downregulate the NF-κB signaling pathway (a major pro-inflammatory pathway) in macrophages, thereby suppressing M1 polarization. Simultaneously, they activate the STAT3 pathway, which promotes the shift toward the regenerative M2 phenotype107,108.
Nanotopography cues
The inherent mesoporous nanotexture (pores of 2–50 nm) of MBG provides physical cues that affect macrophage morphology. Studies indicate that macrophages adherent to nanostructured surfaces tend to adopt an elongated morphology (indicative of M2) rather than a round morphology (indicative of M1), possibly due to cytoskeletal rearrangement affecting gene expression84,109.
The immune-osteo axis
The cytokines secreted by M2 macrophages (e.g., BMP-2, Oncostatin M) act as potent osteoinductive signals for recruiting MSCs to the defect site. Thus, 3DPMBG scaffolds create an “immune-favorable microenvironment” where the immune response is not suppressed but harnessed to drive bone regeneration108,110.
Adverse immune responses and failure modes
Although 3DPMBG scaffolds are engineered to promote a pro-healing M2 macrophage phenotype, adverse immune responses leading to scaffold failure remain a critical clinical risk. If the scaffold undergoes excessively rapid degradation or mechanical attrition under local biomechanical loading, it can generate an overwhelming amount of particulate debris. Macrophages attempting to clear this debris may undergo “frustrated phagocytosis,” which sustains a prolonged M1 pro-inflammatory state and triggers a severe FBR 103 . This state of chronic inflammation effectively blocks the osteogenic differentiation of MSCs and instead hyper-stimulates fibroblast proliferation. Consequently, a dense, avascular fibrous capsule forms around the implant, isolating the scaffold from the surrounding native bone network. Clinically, this fibrous encapsulation prevents osseointegration, leading to aseptic loosening, implant micro-motion, and ultimate clinical failure of the CMF reconstruction 104 . Furthermore, as previously noted, any residual organic binders from the 3D printing process or trace endotoxin contamination can act as potent immunogens, severely exacerbating this adverse inflammatory cascade. Therefore, precisely tuning the mechanical stability and degradation kinetics of 3DPMBG is mandatory to avert these immunologically driven failure modes.
In vivo degradation and ion-release kinetics
While in vitro simulated body fluid (SBF) assays provide baseline dissolution data, the in vivo degradation of 3DPMBG is a far more complex, dynamically driven process governed by physiological fluid perfusion, cellular activity, and local pH fluctuations. Unlike the static conditions in vitro, in vivo release kinetics exhibit a distinct biphasic profile.
Initially, the exceptionally high specific surface area and hierarchical porosity facilitate rapid fluid permeation, resulting in an initial burst release of therapeutic ions (e.g., Si, Ca, Sr) within the first 3–7 days 21 . This early burst is clinically advantageous, as it rapidly establishes the localized concentration gradient necessary for M2 macrophage polarization and initial angiogenesis.
Subsequently, the kinetics transition into a sustained, diffusion-controlled release phase lasting for weeks to months. This deceleration occurs because a dense layer of carbonated hydroxyapatite (CHA) rapidly precipitates on the scaffold surface in vivo, acting as a natural diffusion barrier that slows further dissolution of the underlying glass network74,75. Furthermore, in vivo degradation is actively mediated by osteoclasts; the mildly acidic microenvironment (pH ~4.5) within the osteoclastic resorption lacunae dynamically accelerates localized glass dissolution82,103. Crucially, the macroscopic degradation timeline of optimized 3DPMBG scaffolds (typically 3–6 months) aligns perfectly with the physiological rate of autologous bone creeping substitution 111 . This synchronized degradation prevents premature mechanical collapse—a common pitfall of highly soluble biomaterials (e.g., borate glasses)—while avoiding the permanent stress-shielding and FBRs associated with non-resorbable crystalline bioceramics10,112.
Synergistic effects and temporal control
In clinical reality, these mechanisms do not occur in isolation. The ideal 3DPMBG scaffold acts as a “temporal conductor” 113 .
Phase 1 (days 1–7): Rapid release of soluble Si4+/Ca2+ and immunomodulatory ions (e.g., Zn2+, Sr2+) regulates the macrophage switch (M1 → M2) and prevents infection 113 .
Phase 2 (weeks 1–4): Sustained release of angiogenic ions (Cu2+, Co2+) stabilizes HIF-1α, guiding blood vessel ingrowth into the macro-channels of the 3D scaffold34,114.
Phase 3 (months 1–6): The osteoconductive apatite layer formed on the MBG surface, combined with the activation of Wnt/β-catenin pathways, facilitates massive bone deposition and remodeling, ultimately leading to the replacement of the scaffold by autologous bone via the creeping substitution process. 115
Crucially, this temporal orchestration by 3DPMBG presents a significantly accelerated healing timeline relative to traditional bone substitutes. While highly crystalline bioceramics (e.g., conventional HA or inert titanium) often exhibit a delayed onset of osseointegration due to their slow degradation and lack of active ionic stimulation, the exceptionally high specific surface area of MBG ensures an immediate and proactive interaction with the host9,10. This rapid initial ionic burst effectively shortens the prolonged inflammatory phase typically seen with inert materials and fast-tracks the onset of angiogenesis (shifting it to the critical first week)34,113,114. Consequently, 3DPMBG shifts the entire regenerative timeline forward, transitioning the material from a passive space-maintainer to an active catalyst for early-stage healing, as comparatively summarized in Table 4.
Comparative timeline of in vivo healing events: 3DPMBG scaffolds vs. traditional bone substitutes.
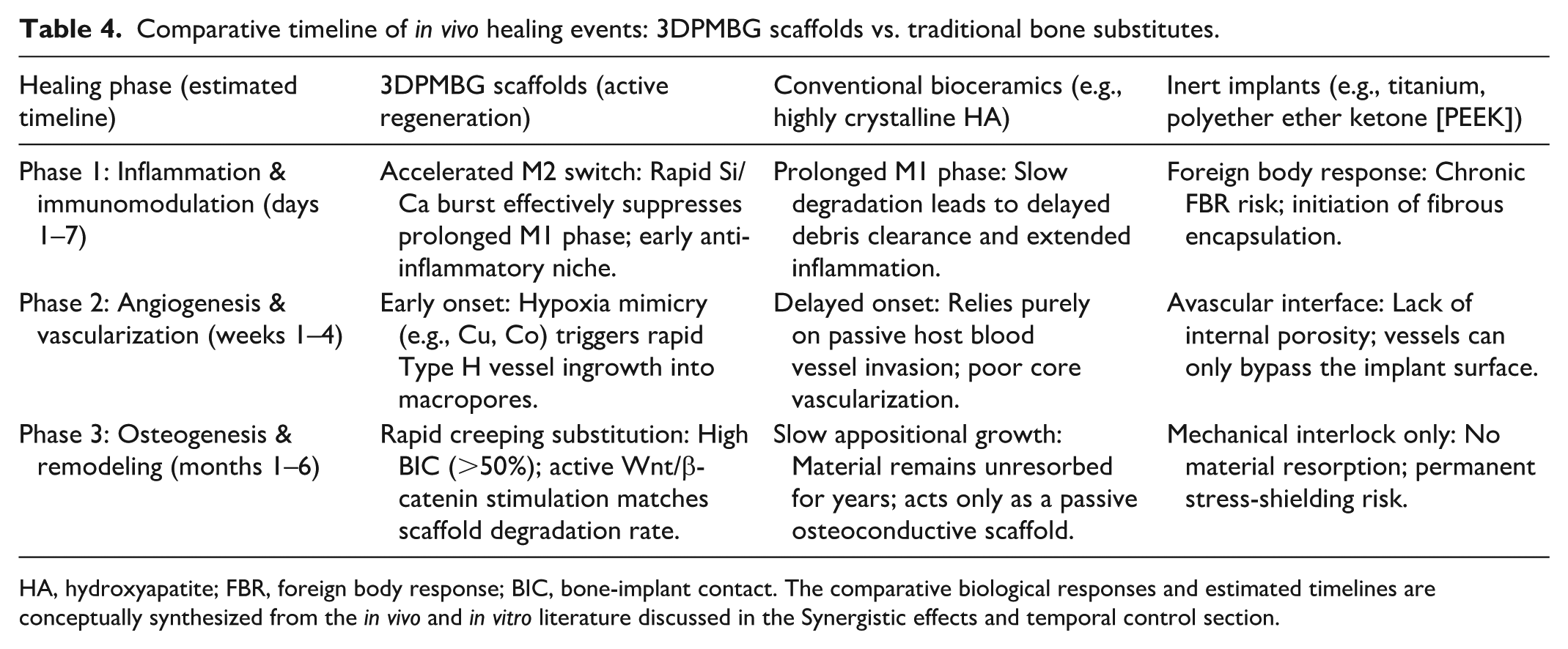
HA, hydroxyapatite; FBR, foreign body response; BIC, bone-implant contact. The comparative biological responses and estimated timelines are conceptually synthesized from the in vivo and in vitro literature discussed in the Synergistic effects and temporal control section.
Preclinical validation and roadmap to clinical translation
While the molecular mechanisms of 3DPMBG have been elucidated in vitro, the transition from the laboratory bench to the clinical bedside—often termed the “Valley of Death”—requires rigorous validation in complex physiological environments116,117. This section critically evaluates the therapeutic efficacy of 3DPMBG across hierarchical animal models and analyzes the regulatory and manufacturing barriers impeding its widespread clinical adoption, highlighting critical bottlenecks (see Figure 4) 27 .
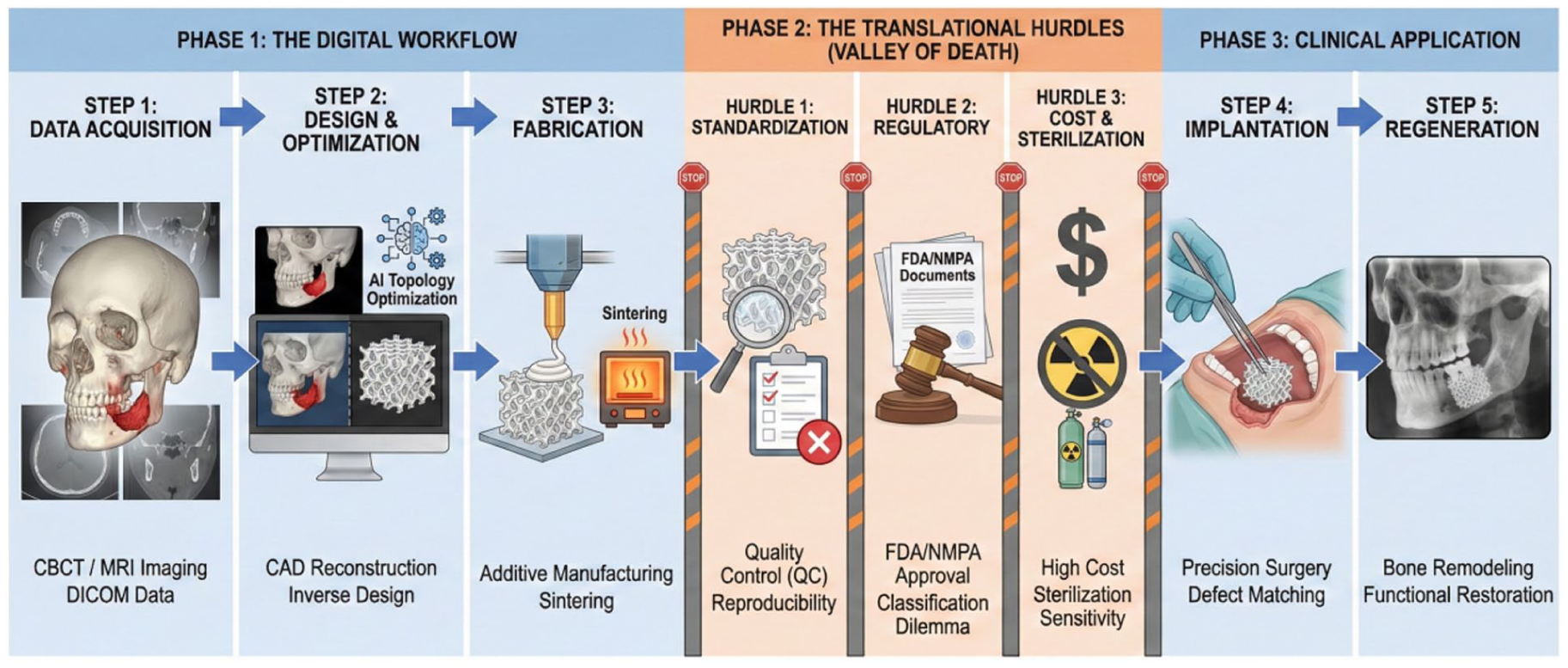
The translational roadmap of 3DPMBG from digital design to clinical application, highlighting critical bottlenecks. The workflow begins with (1) data acquisition via patient CBCT/MRI, followed by (2) CAD/AI-driven design to generate biologically optimized TPMS structures. (3) Fabrication involves printing and sintering the MBG scaffold. However, the transition to (4) clinical implantation is impeded by significant “translational hurdles”: the lack of standardized quality control (QC) for personalized batches, the complexity of regulatory approval by the U.S. Food and Drug Administration (FDA) and National Medical Products Administration (NMPA) for custom-made devices, and the challenges of cost-effectiveness and sterilization sensitivity. Successfully overcoming these barriers leads to (5) functional regeneration and successful implant-supported rehabilitation.
Hierarchical preclinical evaluation: From rodents to large animals
The validation of CMF bone substitutes typically follows a “pyramid” strategy, moving from proof-of-concept in small animals to translational verification in large animals that closely mimic human physiology112,118.
Small animal models (proof-of-mechanism)
Rat calvarial defects (typically 5–8 mm critical-sized defects) serve as the standard model for evaluating osteoconductivity and osteoinductivity due to the lack of spontaneous healing.
Quantitative outcomes
A meta-analysis of recent studies indicates that functionalized 3DPMBG scaffolds consistently outperform traditional controls. For instance, in an 8-week study comparing strontium-doped 3DPMBG with β-TCP scaffolds, micro-CT analysis revealed a significantly higher bone volume fraction (BV/TV) in the 3DPMBG group (45% ± 5% vs. 25% ± 4%) 111 .
Histological evidence
Histomorphometric analysis (Van Gieson or Masson trichrome staining) typically demonstrates that while β-TCP degrades rapidly leaving fibrous gaps, 3DPMBG scaffolds maintain structural integrity while facilitating “through-and-through” bone ingrowth. The interface analysis reveals a direct bonding layer (apatite formation) without intervening fibrous tissue, confirming superior osseointegration 111 .
Infection models
In infected bone defect models (e.g., Staphylococcus aureus-induced osteomyelitis in rat femur), Ag-doped or antibiotic-loaded MBG scaffolds have demonstrated a dual capacity: reducing bacterial load by 99.9% (3-log reduction) within the first week while maintaining osteogenic potential, a feat unachievable by systemic antibiotics alone due to poor perfusion in necrotic bone119,120.
Critical appraisal and inter-study variability
Despite these promising outcomes, the overall quality of current preclinical evidence is limited by inherent biases and significant inter-study heterogeneity. Many small animal studies lack rigorous blinding or randomization protocols, introducing potential observational bias121,122. Furthermore, direct comparisons between studies are severely confounded by multiple variables. For instance, defect sizes in rat calvarial models typically range from 5 mm to 8 mm; the latter represents a true critical-sized defect, whereas 5-mm defects may undergo partial spontaneous healing, potentially inflating the perceived efficacy of the scaffold123,124.
Importantly, profound inter-study variability exists regarding the specific MBG composition (e.g., variations in the SiO2/CaO ratio or dopant concentrations), precise pore size, and specific AM parameters (such as layer thickness, hatch spacing, or laser speed)26,45. For instance, scaffolds fabricated via DIW often possess much larger macropores and distinct surface roughness compared to the high-resolution constructs produced by SLA, leading to drastic variations in mechanical modulus, ion release kinetics, and vascularization rates27,125. Consequently, this multi-variable heterogeneity severely limits the direct comparability of preclinical efficacy across different studies. Moreover, disparities in the control matrices used (e.g., empty defects, autografts, or distinct commercial bioceramics) and the duration of follow-up periods (typically ranging from 4 to 12 weeks) further complicate the standardized evaluation of 3DPMBG. Standardizing these experimental parameters in future studies is imperative for drawing definitive and comparable conclusions.
Translational models: From rabbits to large animals
Data from rodents often fail to predict outcomes in humans due to differences in bone metabolic rates (rats heal much faster). Therefore, validating scaffolds in transitional models (e.g., rabbits) and large animal models (e.g., minipigs) is essential for evaluating mechanical stability and long-term degradation under physiological loads.
Rabbit femoral defects (the translational bridge): Although not a large animal in the strictest sense, the rabbit model provides a critical bridge between rodents and clinical application 126 . Studies using 3D-printed composite or bioceramic scaffolds in rabbit femoral and condyle defect models have demonstrated enhanced new bone formation and satisfactory in vivo performance by micro-CT and histological analyses, supporting the translational value of this model for evaluating scaffold osteoconductivity and mechanical behavior127,128.
Porcine zygomatic/Cranial defects (preclinical gold standard): Moving to large animals that share a similar bone remodeling rate (lamellar bone structure) with humans, studies utilizing patient-specific 3DPMBG scaffolds in porcine zygomatic defects have validated the precision of fit. Postoperative CT imaging confirmed that the deviation between the designed and actual implant position was within <1 mm, highlighting the accuracy of the digital workflow 129 . Furthermore, push-out tests revealed that the interfacial bonding strength of 3DPMBG increased over time (reaching >3 MPa at 12 weeks), indicating functional biological fixation 130 .
The regulatory landscape: The paradox of personalization
Despite promising preclinical data, the commercialization of 3DPMBG faces a unique regulatory hurdle: the conflict between “mass standardization” (the basis of traditional regulations) and “mass customization” (the essence of 3D printing) 131 .
Regulatory classifications by the U.S. Food and Drug Administration (FDA) and National Medical Products Administration (NMPA)
United States — U.S. Food and Drug Administration (FDA): Three-dimensionally printed bone scaffolds are generally classified as class II (moderate risk) or class III (high risk) devices. If the scaffold contains a drug or biologic (e.g., BMP-2, antibiotics), it is regulated as a combination product, which exponentially increases the complexity of approval. The “custom device exemption” is limited to unique cases (compassionate use) and does not support mass production. Therefore, manufacturers must seek clearance via the 510(k) pathway (proving substantial equivalence to a predicate device) or the arduous PMA (premarket approval) 132 . The challenge lies in defining a “predicate” for a device whose shape changes for every patient.
China — National Medical Products Administration (NMPA): In 2020, China implemented the “Regulations on the Supervision and Administration of Customized Medical Devices (Trial),” providing a legal framework for 3D printed implants 133 . However, this regulation requires a rigid collaboration between the clinical institution and the manufacturer, with strict liability definitions.
Beyond regional classifications, the core challenge lies in the validation methodology. Recent literature highlighted that the lack of standardized testing guidelines for PSIs remains a primary bottleneck for regulatory clearance, as traditional “batch testing” protocols are inapplicable to unique geometries 134 .
Furthermore, the paradigm shift toward “point-of-care” (PoC) manufacturing—where hospitals print implants in-house—raises unprecedented questions regarding liability and quality assurance. As demonstrated in recent analyses, establishing a “digital thread” for traceability from design to implantation is essential to mitigate these legal risks 135 .
In addition, recent studies have emphasized that harmonizing these diverse regulatory frameworks across international borders, such as differences between the U.S. Food and Drug Administration (FDA) regulatory framework and the European Union Medical Device Regulation (EU MDR), remains a critical hurdle for the global commercialization of 3D-printed CMF solutions 136 .
The shift from “product testing” to “process validation”
Traditionally, quality control (QC) relies on the destructive mechanical testing of a representative sample from each batch. However, for personalized 3DPMBG implants where “batch size equals one,” destructive testing is impossible. Consequently, the regulatory paradigm is shifting toward “process validation” and non-destructive evaluation. Experts have emphasized that ensuring the fidelity of the digital workflow—from Digital Imaging and Communications in Medicine (DICOM) segmentation to Standard Tessellation Language (STL) slicing—is the first line of defense, requiring rigorous software validation to prevent geometric errors before printing 131 .
Furthermore, “Surrogate Testing” has emerged as a viable alternative, where standardized test coupons are printed alongside the PSI in the same build chamber. These surrogates undergo mechanical and sterility testing as a proxy for the actual device. Recent strategies also advocate for the use of micro-CT as a routine non-destructive QC tool to detect internal micro-cracks or pore occlusions without compromising the implant’s integrity137,138.
Technical and economic barriers to commercialization
Beyond regulations, practical hurdles impede the routine clinical use of 3DPMBG.
Sterilization sensitivity
MBG is a metastable material. Traditional sterilization methods have drawbacks: Autoclaving (steam) initiates premature hydration and apatite conversion, reducing shelf-life bioactivity. Gamma irradiation can induce color centers and potential structural defects in the glass network. Ethylene oxide (EtO) is the preferred method but requires rigorous aeration to remove toxic residues from the mesopores. Developing a validated, standard sterilization protocol that preserves the mesoporous structure and drug payload is a critical industrial gap24,139,140.
Specifically, a comprehensive review elucidated the trade-offs between modalities, reporting that gamma irradiation frequently induces point defects (color centers) in the silicate network, which can unpredictably alter ion-release profiles 58 . Conversely, as demonstrated in studies regarding 3D-printed composite scaffolds, steam sterilization (autoclaving) can trigger surface hydrolysis and premature HA crystallization, effectively reducing the material’s bioactive potential before it even reaches the patient141,142.
The cost-benefit analysis
The economic feasibility of 3DPMBG remains a contentious barrier to widespread adoption. The fabrication workflow—encompassing high-resolution CT segmentation, expert CAD design, printing, and post-sintering—is labor-intensive, often costing 3–5 times more than off-the-shelf prefabricated blocks. To justify coverage by insurance systems (e.g., CMS in the US, DRGs in China), clinical trials must demonstrate value beyond mere survival. A systematic review on the health economics of 3D printing in surgery revealed that the higher upfront manufacturing costs are often offset by significant reductions in operating room (OR) time (average savings of 62 minutes per case) and decreased anesthesia exposure 143 .
Therefore, future clinical studies should prioritize “time-driven activity-based costing” (TDABC) to objectively quantify these systemic savings and support reimbursement applications 135 .
Long-term biosafety of ion-doped scaffolds
While the incorporation of therapeutic ions (e.g., Sr2+, Cu2+, Co2+, Ag+) significantly enhances the biological functions of 3DPMBG, their long-term biosafety remains a critical translational concern. The “therapeutic window” for many of these trace elements is notably narrow. For instance, while silver (Ag+) provides potent antibacterial efficacy, an uncontrolled burst release can induce severe local cytotoxicity against OBs and ECs 35 . Similarly, transition metals like copper (Cu2+) and cobalt (Co2+), which are utilized for hypoxia mimicry, pose risks of heavy metal accumulation. Excessive local concentrations of Cu2+ can generate reactive oxygen species (ROS), leading to oxidative stress and tissue necrosis, whereas systemic accumulation of Co2+ has historically been linked to metallosis and neuro-cardiovascular toxicity in orthopedic implants21,114. Even strontium (Sr2+), widely considered safe, can paradoxically impair physiological bone mineralization if released in excessively high doses over prolonged periods 83 . Therefore, engineering the mesoporous architecture to ensure a sustained, zero-order release strictly within the physiological safety thresholds is paramount. Future translational efforts must mandate long-term in vivo studies (e.g., >12 months in large animals) focusing not only on local bone healing but also on systemic ion biodistribution and organ clearance (hepatic/renal) before regulatory clearance can be achieved.
Current clinical status and the drive for commercial translation
While 3D-printed titanium and polyether ether ketone (PEEK) implants are routine in CMF surgery, 3D-printed bioactive ceramics are in their infancy. Most human applications of 3DPMBG are currently restricted to pilot clinical trials or investigator-initiated studies (IITs) 37 . Preclinical evidence indicates that 3D-printed borate and silicate BG scaffolds facilitate bone regeneration in critical-sized craniofacial defects. Their tailored structural designs notably enhance osteogenesis and vascularization. Specifically, scaffolds fabricated by SLS show improved regenerative capacity, especially when combined with osteoinductive factors 127 . In addition, 3D-printed borosilicate scaffolds incorporating MBG coatings demonstrate significantly boosted OB activity and bone formation in femoral defects, highlighting the critical role of mesoporous architectures 144 .
However, transitioning these encouraging early outcomes into widespread clinical adoption requires navigating a complex commercial landscape. Currently, the global CMF and periodontal bone graft market is heavily dominated by particulate xenografts (e.g., Geistlich Bio-Oss®) and traditional BG putties (e.g., NovaBone®). While clinically ubiquitous, these commercial mainstays possess inherent functional ceilings. Particulate xenografts often exhibit extremely slow resorption rates, remaining encapsulated in vivo without integrating into the natural bone remodeling cycle15,17. Conversely, while commercial 45S5 BG putties offer excellent osteostimulation, they completely lack the macroscopic mechanical integrity required for the structural reconstruction of complex, load-bearing maxillofacial defects (e.g., severe alveolar ridge atrophy or segmental mandibular resections)18,22.
This technological gap highlights the immense translational value of 3DPMBG, positioning it not merely as another bone filler, but as a next-generation “patient-specific regenerative device.” Realizing this potential requires a robust “industry-university-research-clinical” translational ecosystem. There is a particularly urgent strategic demand to industrialize high-end oral medical devices to break the monopoly of traditional imported products and address the massive epidemiological burden of CMF defects. Transitioning MBG from an academic research project to a standardized, commercially viable medical device hinges on overcoming scalable manufacturing bottlenecks, establishing non-destructive QC, and conducting large-scale randomized controlled trials (RCTs) benchmarking 3DPMBG against autogenous bone grafts131,134,145. Successfully navigating this commercialization pathway will not only disrupt the current dental biomaterials market but also provide a superior, cost-effective regenerative solution tailored to the specific anatomical and biological needs of the patient.
Intrinsic limitations and translational pitfalls of MBG
While 3DPMBG presents immense regenerative potential, explicitly acknowledging its intrinsic limitations and potential clinical pitfalls is crucial for a realistic translational roadmap. First, despite the structural optimization provided by AM, the inherent brittleness and low fracture toughness of pure silicate glasses remain a significant pitfall. This fundamentally limits their standalone application in major load-bearing CMF sites (e.g., segmental mandibular resections). To mitigate this mechanical fragility, current translational research is increasingly pivoting toward composite formulations, incorporating secondary biomaterial phases such as HA, tricalcium phosphate (β-TCP), or medical-grade flexible polymers like PCL. These composite strategies effectively deflect crack propagation and significantly enhance the macroscopic fracture toughness and load-bearing capacity of the scaffolds26,66,67,141.
Second, the primary advantage of MBG—its extraordinarily high surface area and rapid ion release—can paradoxically become a toxicological pitfall. If the formulation is not perfectly optimized, an uncontrolled “burst release” of therapeutic heavy metal dopants (e.g., Cu2+, Co2+, Ag+) can easily exceed the local physiological tolerance, inducing severe cytotoxicity, oxidative stress (ROS generation), and adverse FBRs21,35,114. Finally, there is a critical risk of a “degradation-regeneration mismatch.” In highly vascularized defect sites, if the mesoporous scaffold degrades and loses its structural integrity faster than the host’s osteogenic rate, premature mechanical collapse of the regenerated site may occur10,112. Future translational efforts must specifically address these pitfalls through precise multiscale composite engineering before routine clinical adoption can be achieved.
Conclusion and future perspectives
Concluding remarks: An evolution in regeneration
The emergence of 3DPMBG represents a highly promising trend in CMF surgery. Although largely still in the preclinical and early translational stages, we are witnessing an encouraging evolution from the era of “passive substitution”—where inert blocks merely filled voids—to the era of “active regeneration,” where smart, hierarchical scaffolds possess the potential to actively instruct the host body to heal.
By synergizing the intrinsic bioactivity of sol-gel glasses with the geometric freedom of AM, 3DPMBG overcomes the historical dichotomy between biological function and mechanical competence. The evidence synthesized in this review confirms that through precise ionic doping (Sr2+, Cu2+, Ag+) and topological optimization (TPMS structures), these scaffolds can successfully orchestrate the “bone-vascular-immune” triad. However, the journey from a promising prototype to a standard-of-care medical device is fraught with challenges in standardization, stability, and regulatory compliance. As we stand on the precipice of clinical translation, the field must evolve beyond “trial-and-error” fabrication toward intelligent, dynamic, and predictive regenerative medicine.
Future horizons: The next generation of CMF scaffolds
To transcend current limitations, future research must converge materials science with digital intelligence and developmental biology. We propose three transformative directions that will define the next decade of research, offering a conceptual illustration of next-generation paradigms (Figure 5).
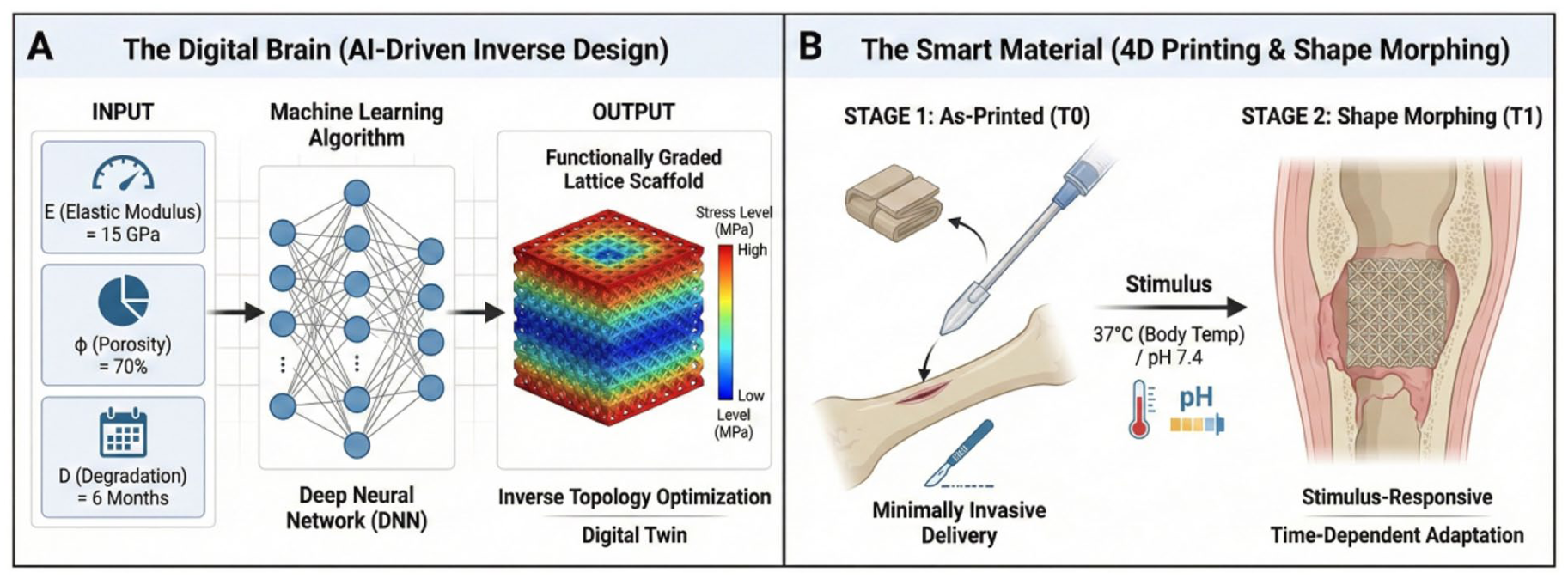
Conceptual illustration of next-generation paradigms for CMF regeneration. (a) AI-driven inverse design: unlike traditional forward engineering, this approach utilizes machine learning algorithms to reverse engineer scaffold topology based on specific clinical requirements (e.g., target elastic modulus, porosity, and degradation rate), enabling the creation of functionally graded structures that precisely match the host bone mechanics. (b) Four-dimensional printing (shape morphing): by introducing “time” as the fourth dimension, stimuli-responsive smart scaffolds can alter their geometry (e.g., expansion or unfolding) in response to physiological triggers (e.g., body temperature or pH). This capability facilitates minimally invasive implantation and allows the scaffold to dynamically adapt to skeletal growth or defect geometry after the surgery.
From 3D to 4D printing: Time-dependent adaptability
Reconstructing CMF defects is challenging because the skeletal system is dynamic, especially in pediatric patients undergoing rapid growth. Four-dimensional printing introduces “time” as the fourth dimension, utilizing stimuli-responsive inks that change shape or function post printing in response to physiological triggers (e.g., pH, temperature, enzymatic activity). This capability enables the fabrication of “smart” shape-memory scaffolds that can be compressed for minimally invasive delivery and subsequently recover their preprogrammed geometry at body temperature. Such dynamic adaptation not only facilitates surgical implantation but also ensures optimal contact with irregular defect margins, offering a superior alternative to rigid static implants146,147.
Shape-morphing scaffolds
Envision a scaffold for a cleft palate patient that autonomously expands in response to the localized mechanical strain of growth, mimicking the function of a distraction osteogenesis device but without external screws. This could be achieved by printing “shape-memory” polymer composites (e.g., MBG/Polyurethane) that unfold or elongate at body temperature. Validating this concept, recent studies have demonstrated that shape-memory polyurethane scaffolds—whether thermally actuated or water-driven—can be compressed for minimally invasive delivery and subsequently recover their geometry in situ. This capability allows the construct to precisely fill irregular defects, confirming the clinical feasibility of dynamic, space-filling implants148,149,150.
On-demand drug release
Unlike traditional scaffolds that rely on passive diffusion—often resulting in an initial “burst release” followed by sub-therapeutic levels, future scaffolds could incorporate “smart gates” (e.g., pH-sensitive hydrogel valves or supramolecular switches) within the mesopores. These gates remain closed under physiological conditions (pH 7.4). However, in the event of post-operative infection (which typically lowers local pH to 5.5 due to bacterial metabolism), the scaffold would autonomously detect the acidosis and trigger a precise release of antibiotics. This “self-medicating” capability not only ensures high local drug concentrations to penetrate biofilms but also minimizes systemic toxicity and the risk of antimicrobial resistance caused by long-term low-dose exposure151,152.
AI-driven inverse design and digital twins
Current scaffold design is largely “forward-engineered”: researchers typically design a lattice, fabricate it, and then test its biological performance in a laborious trial-and-error loop. However, this approach is constrained by the limited design space human intuition can explore, often failing to address the complex, multiscale hierarchy of native bone. The future lies in “inverse design” powered by artificial intelligence (AI) and machine learning (ML). By processing vast datasets of structure-property relationships, AI can identify non-intuitive geometric features that maximize biological performance, shifting the paradigm from “manufacturing-centered” to “data-driven” regeneration153,154.
Predictive topology optimization
Instead of manually selecting a pore structure, clinicians will input the desired biological outcome (e.g., “Young’s modulus of 15 MPa, degradation time of 6 months, vascular density of 20%”). Generative AI algorithms will then reverse engineer the exact micro-architecture required to achieve these targets, creating non-uniform, functionally graded structures that human designers could never conceive.
Although AI application in MBG is in its infancy, similar strategies have been successfully applied in bioceramic composites. Recent studies have utilized ML algorithms to inversely design bio-inspired scaffolds with tailored mechanical moduli matching native bone, significantly outperforming traditional trial-and-error topological designs155,156.
Digital twins
We envision the creation of a “Digital Twin” for the patient’s defect—a dynamic virtual simulation that transcends static CT imaging by integrating the patient’s specific bone density, metabolic rate, and immune status. Through multiphysics modeling (coupling finite element analysis with computational fluid dynamics), this system can predict how the scaffold interacts with physiological loads and fluid flow over time 157 . Consequently, the scaffold’s performance—specifically the balance between degradation rate and new bone growth—can be rigorously tested in this virtual environment. This approach enables “In Silico Clinical Trials,” which minimize failure risks and optimize implant topology before the physical manufacturing process ever begins 158 .
Beyond animal models
Traditional reliance on animal models is increasingly challenged, not only by ethical and cost concerns but also by their poor predictive value for human outcomes. Statistics indicate that over 90% of drugs entering clinical trials fail despite promising animal data, largely due to the inability of non-human models to recapitulate human-specific osteoimmunology and metabolic turnover. To address this crisis, the field is pivoting toward microphysiological systems (MPS), or “bone-on-a-chip” devices. Unlike passive cell cultures, these dynamic platforms incorporate 3D-printed scaffolds into perfused micro-chambers, effectively creating a “human bone biopsy” on a chip for high-fidelity validation159,160.
Recapitulating the niche
Unlike static cell cultures, these microfluidic platforms can mimic the physiological interstitial fluid flow found in the lacunar-canalicular network. Recent research has demonstrated that by controlling fluid shear stress within a chip loaded with biomimetic scaffolds, one can precisely simulate the mechanical loading experienced by osteocytes in vivo. This dynamic environment activates key mechanotransduction pathways, providing a high-fidelity platform to optimize scaffold design parameters (e.g., pore architecture and ion-doping) under physiological conditions 161 .
Personalized screening
Furthermore, these systems allow for the co-culture of patient-derived cells (e.g., osteoblasts [OBs] and peripheral blood mononuclear cells [PBMCs]) to create a personalized immune model. Since immune responses exhibit significant inter-patient heterogeneity, “personalized screening” is crucial to predict idiosyncratic reactions, such as hypersensitivity or cytokine storms—that generic animal models often miss. By identifying these risks ex vivo, specifically investigating the crosstalk between the bioactive material and the host immune system, clinicians can select the most compatible scaffold for high-risk patients, truly realizing the promise of precision regenerative medicine 162 .
Final thought: Moving toward active regeneration
The development of 3DPMBG reflects an ongoing shift in biomaterial design for CMF reconstruction, moving away from passive space-maintaining grafts toward more biologically instructive microenvironments. By integrating the intrinsic bioactivity of mesoporous glass with the precise geometric control of AM, and anticipating future integrations with AI and 4D printing, the field is moving closer to bridging the gap between materials science and clinical application.
Ultimately, the successful translation of 3DPMBG relies on utilizing these scaffolds as active modulators of the local bone-vascular-immune axis. Overcoming the remaining translational barriers—specifically, establishing standardized regulatory frameworks for personalized devices and validating non-destructive QC methods—will require sustained interdisciplinary efforts among material scientists, bioengineers, clinicians, and regulatory agencies. Through such collaboration, 3DPMBG holds the potential to advance the clinical objective of CMF surgery from mere structural repair to restitutio in integrum—achieving comprehensive anatomical and functional regeneration.
Footnotes
Acknowledgements
The authors express their gratitude to Guangxi Medical University and Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine for their support during the joint training program. The authors utilized the AI tool Gemini Pro 3 solely for the generation of schematic illustrations in this manuscript. The authors reviewed and edited the content and take full responsibility for the integrity of the work.
Ethical considerations
Ethical approval is not applicable because this article is a comprehensive review of existing literature and does not involve any animal or human experiments.
Author contributions
Tianqi Wu: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing–original draft, Writing–review & editing, Visualization.
Yijie Du: Methodology, Validation, Formal analysis, Investigation, Data curation, Writing–review & editing, Visualization.
Baofeng Yang: Methodology, Validation, Formal analysis, Investigation, Data curation, Writing–review & editing, Visualization.
Jinwu Wang: Conceptualization, Methodology, Resources, Writing–review & editing, Supervision, Project administration, Funding acquisition.
All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China under Grant No. 82372377.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.
Statement of informed consent
There are no human subjects in this article, and informed consent is not applicable.