
Abstract
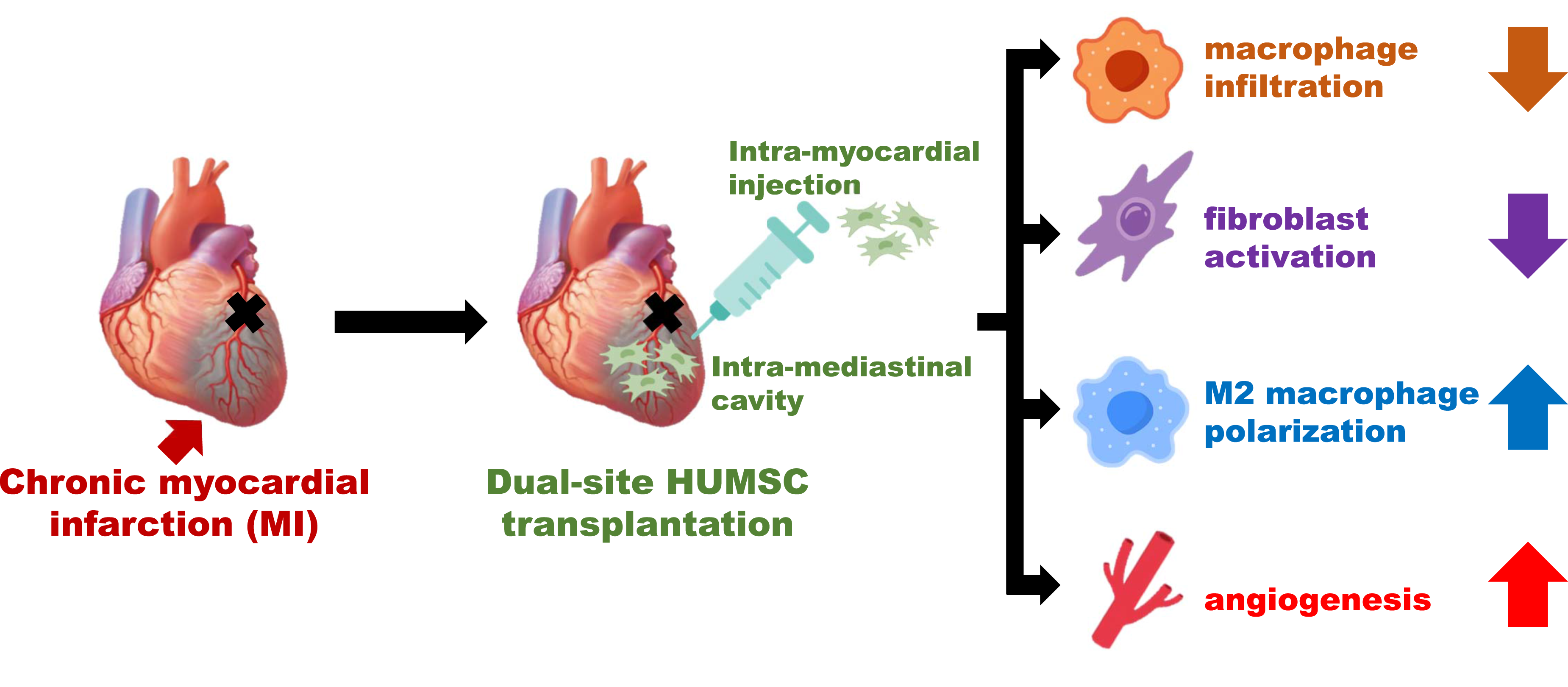
Myocardial infarction (MI), mainly caused by coronary artery occlusion, remains a leading cause of death worldwide. Although many patients survive after emergency treatment, chronic MI often develops, underscoring the need for effective therapies. This study evaluated the therapeutic potential of human umbilical mesenchymal stromal cells (HUMSCs) in a rat model with chronic MI. MI was induced by permanent ligation of the left anterior descending artery. Seven days post-ligation, 4×106 HUMSCs were transplanted into the peri-infarct myocardium, while an additional 2.5×107 HUMSCs were introduced into the mediastinal space around the ligation site. Successful model establishment was confirmed by elevated cardiac biomarkers and characteristic electrocardiographic changes. Echocardiography and magnetic resonance imaging demonstrated significant impairments in myocardial strain dynamics, reduced ejection fraction, and diminished fractional shortening, all of which improved following HUMSC transplantation. The transplantation also reduced macrophage infiltration, increased M2 macrophage polarization, suppressed fibroblast activation, attenuated fibrosis, and promoted angiogenesis, ultimately preserving cardiomyocytes and improving cardiac function. The transplanted HUMSCs were detected in rat’s myocardium without differentiating into cardiomyocytes or endothelial cells. These findings suggest that adequate HUMSC transplantation offers a promising therapy to attenuate progression of chronic MI or heart failure.
Keywords
Introduction
Despite advancements in medical technology, including early diagnostic testing, preventive measures, and acute-phase interventions, acute myocardial hypoxia remains a leading cause of mortality worldwide. 1 Patients who survive myocardial hypoxia develop inflammation, stenosis, and coronary artery occlusion, which result in ischemic or hypoxic cardiac damage. The ensuing cardiomyocyte death and fibrosis lead to chronic heart failure, which not only compromises patients’ health and quality of life but also imposes substantial burdens on patient family, society, and health-care systems. 2 Few pharmacological or interventional therapies are currently available for restoring cardiac function in chronic heart failure. Disease management instead relies on lifestyle modifications, dietary regulation, rehabilitation, and supportive therapies to prevent deterioration. 3 Thus, developing effective therapeutic approaches for chronic myocardial infarction (MI) remains a key goal in both basic and clinical medicine.
Several studies have explored the potential of stem cell therapy for myocardial repair. Sharp III et al. induced MI by occluding the left anterior descending coronary artery (LAD) for 90 min, followed by ischemia–reperfusion, and immediate transplantation of 2×106 swine cortical bone stromal cells into the myocardium. This intervention slowed the decline in cardiac output, reduced left ventricular dilation during both diastole and systole, minimized fibrotic area expansion, increased cardiomyocyte density, and reduced cell hypertrophy. 4 Similarly, Zhang et al. performed permanent coronary artery ligation in swine and transplanted 4 × 107 human umbilical mesenchymal stromal cells (HUMSCs) into the myocardium, which prevented cardiac output decline, enhanced vascularization, and mitigated fibrosis and apoptosis. 5 In another study, Nascimento et al. induced MI in mice via permanent coronary artery ligation and transplanted 2 × 105 HUMSCs into the myocardium, yielding comparable benefits, including preserved ventricular wall thickness. 6
HUMSCs, derived from Wharton’s jelly in the umbilical cord (a biological material typically discarded after birth) offer several advantages over embryonic- or bone marrow-derived stromal cells due to their ease of collection and ethical accessibility. Our previous studies demonstrated the successful transplantation of HUMSCs into the spinal cord, cerebral cortex, hippocampus, and cerebellum of rats, effectively treating conditions such as spinal cord injury, acute and chronic stroke, epilepsy, parkinsonism, amyotrophic lateral sclerosis and cerebellar atrophy.7–14 Beyond neurological disorders, HUMSCs have also been used to treat diabetes, osteoporosis, liver fibrosis, peritoneal fibrosis, and pulmonary fibrosis, demonstrating their therapeutic potential across multiple organ systems.15–21 Notably, HUMSCs do not elicit significant immune responses, making them a promising candidate for clinical transplantation.
Various animal models have been developed to study MI. In large animals, myocardial ischemia of the left ventricle can be induced using an ameroid constrictor or through balloon occlusion of the coronary artery, mimicking clinical MI. In small animals, ligation of the LAD is widely used for inducing MI.22–24 Two primary approaches used for ligation are ischemia–reperfusion and permanent ligation. Ischemia–reperfusion simulates cardiac damage due to thrombolytic treatment in patients with MI; notably, the extent of myocardial damage depends on the duration of ischemia. Permanent ligation induces irreversible ischemic necrosis of cardiomyocytes, leading to a consistent and severe injury in animal models.25,26
To establish a stable and reproducible rat model of severe MI, we used permanent ligation in the present study. Magnetic resonance imaging (MRI), one-week post-operation, confirmed considerable and consistent thinning of the anterior left ventricular wall, accompanied by a marked decline in left ventricular function. At this time point, we transplanted HUMSCs to investigate their therapeutic potential for treating chronic MI and improving cardiac function.
Materials and methods
Establishment of a rat model of MI
All animals involved in the study were handled in accordance with ethical guidelines, and their care and use were approved by the Medical and Laboratory Animal Ethics Committee of National Yang Ming Chiao Tung University. Sprague–Dawley rats (male, 280–310 g) were anesthetized by administering an intraperitoneal injection of Zoletil 100 (Virbac) and xylazine hydrochloride (Sigma 23076359). Deep anesthesia was confirmed by the absence of the paw reflex and whisker movement. Hair was removed from the rat neck and chest. The rats were placed on a heating pad with their limbs secured. The surgical area and its surroundings were disinfected with 75% ethanol.
A tracheotomy was performed by making a 1-cm incision parallel to the ears at the neck. The muscle layers were gently separated with fine scissors until the trachea was exposed. A small incision was then made between the cartilage rings by using ophthalmic scissors, allowing the insertion of a plastic tube, which was connected to a ventilator (Harvard apparatus) set at a frequency of 60–62 breaths/min. The trachea was secured with a cotton thread by using slipknots to prevent air leakage. Synchronization of lung movement with the ventilator was monitored.
A thoracotomy was performed by making a 4-cm incision along the chest, extending from a point parallel to the armpit down to the abdomen. Through electrocautery (Birtcher), the chest wall muscles were separated to expose the ribs. The third and fourth ribs were cut, and the pleura were carefully opened without damaging the left lung. The chest cavity was held open to expose the heart, and the parietal pericardium was carefully dissected without damaging the thymus. The left auricle and lung were gently pressed aside by using cotton swabs. A 6-0 cotton thread (Silk ST126) was passed through the myocardium 2 to 3 mm below the left auricle and tied around the LAD to achieve permanent ligation. Excess thread was trimmed, and electrocardiography (EKG; Biopac Systems MP150) was performed to monitor waveform changes after ligation. Changes in myocardial color were also monitored to confirm procedural success. After ligation, the intercostal muscles, chest wall muscles, and skin were sequentially sutured with a 4-0 cotton thread (Silk ST204). Then, the plastic ventilator tube was removed, and the tracheal incision was sutured with a 6-0 thread. Once spontaneous breathing was confirmed, the neck incision was sutured with a 4-0 thread. The EKG waveform was monitored to confirm successful establishment of the MI model. After the procedure, the rats were placed on a heating pad and administered analgesic cream (Liprido Cream) until they fully recovered.
Rats were housed in a 45×24×20 transparent polycarbonate (PC) cage, with a 12-hour light/dark cycle and controlled temperature (25±2°C) and humidity (30%-70%). They had ad libitum access to food and water. Bedding materials were changed once every week.
Isolation and culture of HUMSCs
Human umbilical cord tissues were obtained from at the Obstetrics and Gynecology Department of the Taipei Veterans General Hospital (Taipei). Written informed consents were obtained from all expectant mothers. The human umbilical cord tissue sampling schemes were approved by the Ethics Review Committee of the Taipei Veterans General Hospital. Human umbilical cords were collected under sterile conditions in the delivery room and stored in Hank’s Balanced Salt Solution (Gibco 14185-052) at 4°C. Within 24 h, HUMSCs were isolated and cultured. All instruments were sterilized by autoclaving before use, and the entire procedure was performed under sterile conditions; 75% ethanol was used for disinfection and flame sterilization. In a sterile environment, the umbilical cord was disinfected with 75% ethanol and placed in Hank’s Balanced Salt Solution. It was then longitudinally sectioned, and the arteries and veins were removed. Wharton’s jelly was excised and cut into 0.5-mm cubes and then centrifuged at 4000 rpm for 5 min. The supernatant was discarded, and the remaining tissue was treated with collagenase and trypsin. The reaction was terminated by adding fetal bovine serum (FBS; Gibco 10437-028). At this stage, the tissue had been processed into HUMSCs. Finally, the isolated HUMSCs were resuspended in 10% FBS. The total cell count was determined, and the cells were either cultured or cryopreserved in liquid nitrogen for future use.
Transplantation of HUMSCs
HUMSCs were treated with 0.5% trypsin–ethylenediaminetetraacetate (Gibco 15400-054) for 2.5 min; the reaction was terminated by adding Dulbecco’s Modified Eagle Medium supplemented with 10% FBS. The cells were then centrifuged at 1500 rpm for 5 min, the supernatant was removed, and the pellet was washed with saline. A second centrifugation was performed to harvest HUMSCs.
One week after permanent ligation, tracheotomy and thoracotomy were performed again, thereby establishing a chronic MI model. A total of 4×106 HUMSCs were transplanted into the myocardium adjacent to the ligation site, and 2.5×107 HUMSCs were transplanted into the mediastinal cavity above the ligation site. Cell viability was assessed using trypan blue staining, and the viability rate was approximately 95%–98%.
Experimental grouping
Animals were randomized, blinded for treatments and assays. The rats were divided into five experimental groups: Group 1: Normal group. At 8 weeks of age, rats randomly underwent tracheotomy and thoracotomy without additional surgical intervention. One week later, tracheotomy and thoracotomy were performed again, but no treatment was administered. Group 2: MI+saline group. At 8 weeks of age, rats randomly underwent tracheotomy and thoracotomy, followed by permanent ligation of the LAD. One week later, saline was injected into the myocardium adjacent to the ligation site. Group 3: MI+SC(Im) Group. At 8 weeks of age, rats underwent tracheotomy and thoracotomy, followed by permanent ligation of the LAD. One week later, the rats were randomly assigned to receive an intramyocardial injection of 4 × 106 HUMSCs in the region adjacent to the ligation site. Group 4: MI+SC(IM) Group. At 8 weeks of age, rats underwent tracheotomy and thoracotomy, followed by permanent ligation of the LAD. One week later, the rats were randomly assigned to receive an injection of 2.5×107 HUMSCs into the mediastinal cavity above the ligation site. Group 5: MI+SC(Im+IM) Group. At 8 weeks of age, rats underwent tracheotomy and thoracotomy, followed by permanent ligation of the LAD. One week later, the rats were randomly assigned to receive an intramyocardial injection of 4 × 106 HUMSCs in the region adjacent to the ligation site, in addition, 2.5×107 HUMSCs were administered into the mediastinal cavity above the ligation site.
To ensure accurate comparison of transplantation outcomes in chronic MI, consistency in injury severity across rats was first established. One week after permanent ligation of the LAD, MRI was performed to confirm considerable and consistent thinning of the anterior left ventricular wall. Only after verifying similar injury levels, we performed HUMSC transplantation or saline injection.
Blood samples were collected every week to measure cardiac biomarkers. In addition, EKG and MRI scans were performed. At 6 weeks after injury, the rats were euthanized, and a quantitative histopathological analysis was performed (Figure 1(a)). Establishment of a rat model of chronic MI and assessment of physiological parameters. (a) Flowchart depicting the induction of chronic MI in rats and subsequent transplantation of HUMSCs. Ligation of the LAD was performed on day 0. In the MI+SC(Im) group, HUMSCs were transplanted into the myocardium adjacent to the ligation site at Week 1 after injury. In the MI+SC(Im+IM) group, HUMSCs were transplanted into both the myocardium adjacent to the ligation site and the mediastinal space around the ligation site. (b) The successful establishment of animal model with MI was confirmed by characteristic changes in electrocardiographic (ECG) waveforms and (C- H) alterations in serum biochemical markers.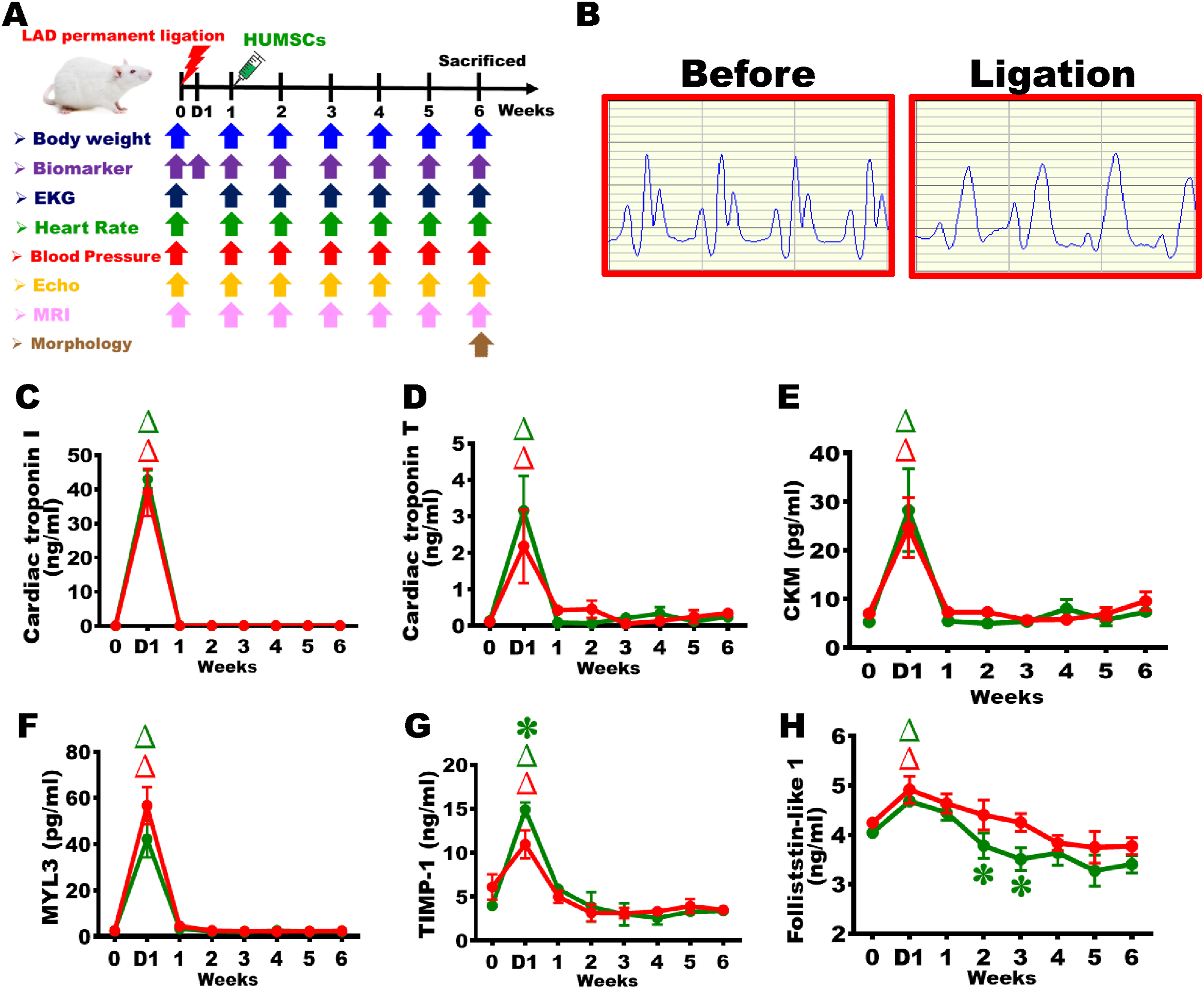
Evaluation of cardiac function
EKG (lead II)
After 7 min of isoflurane anesthesia (Baxter 228-194) in rats, the positive electrode of an EKG system was inserted into the left hindlimb, the negative electrode was inserted into the right forelimb, and the ground electrode was inserted into the right hindlimb to establish a Lead II configuration. Changes in the EKG waveform in Lead II were recorded using the Biopac MP150 system (Supplemental Figure 1).
Heart rate measurement
Heart rate was calculated on the basis of the recorded EKG data (Supplemental Figure 1).
Blood pressure measurement
After induction of isoflurane anesthesia, blood pressure was measured using the BP-2010 AUL system (Softron Biotechnology) on the basis of tail artery pressure.
Serum biochemical analysis
After anesthesia and skin disinfection (75% ethanol), 0.5 mL of whole blood was collected from the tail artery by using a 1-mL syringe with a 25G needle (Terumo). The blood was centrifuged at 8000 rpm for 10 min, and the resultant serum was collected and stored at −20°C. Cardiac biomarkers were quantified using the Milliplex Map Rat Cardiac Injury Magnetic Bead Panel 1 (Millipore RCI1MAG-87k). This panel measures cardiac troponin I, cardiac troponin T, creatine kinase muscle (CKM), follistatin-like protein 1 (FSTL1), myosin light chain 3 (MYL3), and tissue inhibitor of metalloproteinase-1 (TIMP-1).
Echocardiography
After anesthesia, the rats were placed in the supine position, and the chest fur was shaved. A water-soluble gel was applied to the left precordial region, and an ultrasound probe (L8-18i) was positioned over the heart. Through B-mode imaging, the long axis of the left ventricle was scanned, followed by M-mode imaging to capture the short axis of the left ventricle. Systolic and diastolic movements of the left ventricular myocardium were recorded.
Image-Pro Plus was used to measure the left ventricular end-diastolic diameter (LVEDD) and left ventricular end-systolic diameter (LVESD). Left ventricular ejection fraction (LVEF) and left ventricular fractional shortening (LVFS) were calculated using the following equations:


MRI
Cardiac MRI was performed using a Bruker Biospec 70/30 MRI system at the National Taiwan University Instrumentation Center. To accurately measure ventricular ejection fraction (EF), MRI scans were performed and analyzed at three predefined cardiac locations. The rats were placed in the prone position and scanned coronally to obtain images of the heart’s long axis. In addition, at distances of 1/2, 3/8, and 2/8 from the apex, approximately 20 cross-sectional images were acquired perpendicular to the heart’s long axis at each of the three locations. The maximum and minimum left ventricular diameters were quantified to calculate LVEF and LVFS (Supplemental Figure 2 – 4).
For each of the three selected locations, images were obtained at maximal diastole and systole. Image-Pro Plus was used to measure LVEDD and LVESD. LVEF and LVFS were calculated using the following equations:


Preparation of histological samples
Rats were anesthetized with intraperitoneal Zoletil 100 and Xylazine hydrochloride (Sigma 23076359). After confirming deep anesthesia, transcardial perfusion was performed with saline containing 0.2% sodium nitrate and 0.2% sodium citrate, followed by 4% paraformaldehyde and 7.5% picric acid in 0.01 M PBS. Hearts were excised, fixed at 4°C for 24 hours, photographed, and dehydrated through graded ethanol (70–100%). The ventricular portion was then processed with xylene, xylene–paraffin mixtures, embedded in paraffin, and sectioned.
Tissue sectioning and slide preparation
From the heart apex to the ventricular base, 15 consecutive horizontal sections were placed on slides A–O, followed by discarding the next 15 sections. This cycle was repeated (e.g., sections 1–15, 31–45, etc.) until the ligation site was reached, yielding seven slide sets with 315 sections in total (final section No. 615). Each slide contained three sections. Sets 1–2 corresponded to the apex, 3–5 to the mid-ventricle, and 6–7 to the ventricular base near the ligation site.
The first slide of each set (row A) was stained with hematoxylin–eosin (H&E) to examine tissue morphology. The second slide (row B) was stained for collagen fibers to assess fibrosis. The third slide (row C) stained with antibodies against α-smooth muscle actin (SMA) to detect myofibroblast activation. The fourth slide (row D) was stained with antibodies against CD163 to identify M2 macrophages. The fifth slide (row E) was stained with fluorescent wheat germ agglutinin (WGA) to measure cardiomyocyte cross-sectional area. The sixth slide (row F) was stained with antibodies against CD31 to label endothelial cells. The seventh slide (row G) was stained with antibodies against human nuclei to track HUMSC survival. The remaining slides (rows J–O) were preserved as backups (Supplemental Figure 5).
Histological and immunohistochemical staining
H&E staining
Sections were deparaffinized in xylene and rehydrated through graded ethanol to water. They were stained with hematoxylin and eosin, then dehydrated and mounted with Permount for imaging. The left ventricular area in each H&E-stained section was measured using Image-Pro Plus. Total left ventricular volume was calculated by summing the products of each area and section thickness.
Sirius red staining for collagen fibers
Following deparaffinization and rehydration, sections were stained with 0.1% Sirius Red in picric acid, then dehydrated through graded ethanol, cleared in xylene, and mounted. The left ventricular perimeter and collagen-stained area were quantified using Image-ProPlus.
Immunohistochemistry
After deparaffinization and rehydration, cardiac sections were immunostained. Sections were blocked (3% BSA, 1% Triton X-100, 5% FBS) for 1 h at room temperature, then incubated overnight at 4°C with primary antibodies: α-SMA (1:400; Sigma A2547), α-actinin (1:300; Sigma A7811), ED1 (1:400; Millipore MAB1435), CD163 (1:100; Abcam ab182422), and CD31 (1:50; Bio-Rad MCA1334GA). After washing, sections were incubated with biotin-conjugated secondary antibodies for 1 h, followed by detection with an avidin–biotin–HRP complex (ABC kit; Vector Laboratories PK-4000) and DAB development. Sections were dehydrated, cleared in xylene, and mounted for imaging.
Quantification was performed on sections from slide sets #2 (apex), #4 (mid-ventricle), and #6 (ventricular base):
Tissue fluorescent staining
Cardiac sections were deparaffinized, rehydrated, and incubated with Alexa Fluor 488–conjugated WGA (1:100) for 1 h at room temperature, followed by PBS washes and mounting with aqueous medium. Sections from set #4 (mid-left ventricle) were imaged via fluorescence microscopy. Cardiomyocyte cross-sectional area was measured in 16 random non-infarcted fields (40×) using Image-ProPlus.
Assessment of HUMSC survival and distribution
Following deparaffinization, rehydration, and antigen retrieval, cardiac sections were incubated with mouse anti-human nuclei antibody (1:100; Millipore MAB1281) at 4°C, followed by biotin-conjugated goat anti-mouse IgG (1:250; Millipore AP124B) for 1 h at room temperature. Detection was performed using an avidin–biotin–HRP complex and DAB. Sections were then dehydrated, mounted, and analyzed to assess HUMSC survival in rat hearts.
RNA extraction and reverse transcription polymerase chain reaction
Cardiac tissue was placed in a mortar and ground while adding liquid nitrogen. Then, TRIzol (Sigma T9424) was added, and the tissue was further homogenized. The homogenate was centrifuged at 12,000 rpm for 15 min at 4°C, and the supernatant was collected. RNA was precipitated with isopropanol, washed with 75% ethanol, and centrifuged. The supernatant was discarded, and the pellet was air-dried before dissolving in an appropriate volume of diethylpyrocarbonate-treated water. The RNA concentration was measured.
RNA extraction and reverse transcription polymerase chain reaction (PCR) were performed using 2 μg of RNA (Bionovas AM0675-0050). After complementary DNA was synthesized, PCR was performed using 2 μg of template DNA and the following primers: (1) Human PECAM1 Forward:5′-TCAAGAAAAGCAACACAGTCC-3′ Reverse:5′-ACTCCGATGATAACCACTGC-3′ Size: 652 bp (2) Human troponin I3 (TNNI3) Forward:5′-TTTGACCTTCGAGGCAAGTTT-3′ Reverse:5′-CCCGGTTTTCCTTCTCGGTG-3′ Size: 163 bp (3) Human myosin heavy chain 6 (MYH6) Forward:5′-ATTGCTGAAACCGAGAATGG-3′ Reverse:5′-CGCTCCTTGAGGTTGAAAAG-3′ Size: 146 bp (4) Human glyceraldehyde 3-phosphate dehydrogenase (GAPDH) Forward:5′-TCCTCCACCTTTGACGCT -3′ Reverse:5′-TCTTCCTCTTGTGCTCTTGC-3′ Size: 589 bp (5) Rat GAPDH Forward:5′-CTCTACCCACGGCAAGTTCAAC-3′ Reverse:5′-GGTGAAGACGCCAGTAGACTCCA-3′ Size: 160 bp
The thermal cycling conditions were as follows: enzyme activation at 95°C for 10 min; followed by 35 cycles of denaturation at 95°C for 30 s, annealing at 56°C –62°C for 30 s, and extension at 72°C for 1 min; and final extension at 72°C for 5 min. PCR products were subjected to 2% agarose gel electrophoresis and visualized under ultraviolet light.
Statistical analysis
Data are presented in terms of mean ± standard error of the mean values. Comparisons between means were performed using one-way or two-way analysis of variance, followed by Fisher’s least significant difference test for multiple comparisons. A p value of <0.05 was considered statistically significant.
Results
Establishment of a rat model with MI
EKG recordings were used to assess myocardial conduction. Before ligation, a clear QRS complex was observed, indicating normal cardiac conduction. Following MI induction, ST-segment elevation and a tombstone-shaped waveform confirmed successful MI via permanent ligation (Figure 1(b)). Arterial blood was collected weekly to assess serum levels of myocardial injury biomarkers, including cardiac troponin I (cTnI), cardiac troponin T (cTnT), creatine kinase muscle (CKM), myosin light chain 3 (MYL3), tissue inhibitor of metalloproteinase-1 (TIMP-1), and Follistatin-like Protein 1 (FSTL1). In the MI+saline group, all biomarkers rose sharply within 1 day post-MI and returned to baseline by the following day, confirming successful model establishment. A similar pattern was observed in the MI+SC (Im+IM) group. Notably, FSTL1 levels differed significantly between groups at Weeks 2 and 3, indicating that HUMSC transplantation may accelerate biochemical recovery following acute MI (Figure 1(c)–(h)).
Baseline assessments were performed on day 0 (before MI induction), and body weight was monitored weekly. The Normal group exhibited a gradual increase in body weight over time. In the MI+saline group, body weight stagnated at Week 1 after injury. Although weight gain resumed thereafter, it remained significantly lower than that in the Normal group from Week 5 onward. In both the MI+SC(Im) and MI+SC(Im+IM) groups, body weight followed a stagnation trend similar to that in the MI+saline group at Week 1 after injury. However, Week 3 onward, body weight began to increase steadily and continued to rise until Week 6, indicating no significant difference from the trend in the Normal group. These findings suggest that HUMSC transplantation promotes body weight recovery in rats with chronic MI and support steady weight gain (Supplemental Figure 1(a)). No significant differences in heart rate and systolic blood pressure were noted among the three groups (Supplemental Figure 1(b) and 1(c)).
Dual-site HUMSC transplantation improved cardiac function in rats with chronic MI
Ultrasound imaging, B-mode and M-mode images, was used to assess left ventricular function. In the MI+saline group, EF and FS decreased from 75% and 50% at Day 0 to 44% and 25% at Week 1, and further to 38% and 21% by Week 6, with nearly absent anterior wall motion. (Figure 2(a)–(c)). Similar declines were observed in the MI+SC(Im), MI+SC(IM) and MI+SC(Im+IM) groups at Week 1. Thereafter, the MI+SC(Im) and MI+SC(IM) groups showed mild functional recovery with EF/FS 42%/24% and EF/FS 43%/26%, respectively, whereas the MI+SC(Im+IM) group demonstrated greater improvement, reaching EF of 47% and FS of 27% by Week 6 (Figure 2(a)–(c)). To minimize surgical variability, the cardiac function of each rat at Week 6 was subtracted from its corresponding Week 1 value, representing the individual change in cardiac function. In the MI+saline group, EF and FS decreased by 5.8% and 3.8%, indicating progressive deterioration. The MI+SC(Im) and MI+SC(IM) groups showed slight improvement, while the MI+SC(Im+IM) group demonstrated greater recovery, suggesting that dual-site HUMSC transplantation enhanced post-MI cardiac function (Figure 2(d) and (e)). HUMSC transplantation improved cardiac function in rats with chronic MI. (a) Echocardiographic scans of rats from each group were performed on day 0 and at Weeks 1, 2, 3, 4, 5, and 6. The upper panel presents B-mode images, whereas the lower panel presents M-mode images. Quantification of ejection fraction (b) and fraction shortening (c) over the 6-week period, along with changes in ejection fraction (d) and fraction shortening (e) from Week 1 to Week 6. Significant reductions were noted in left ventricular wall motion at Week 1 after injury. HUMSC transplantation promoted contraction of the left ventricular anterior wall, mitigating further decline in cardiac function.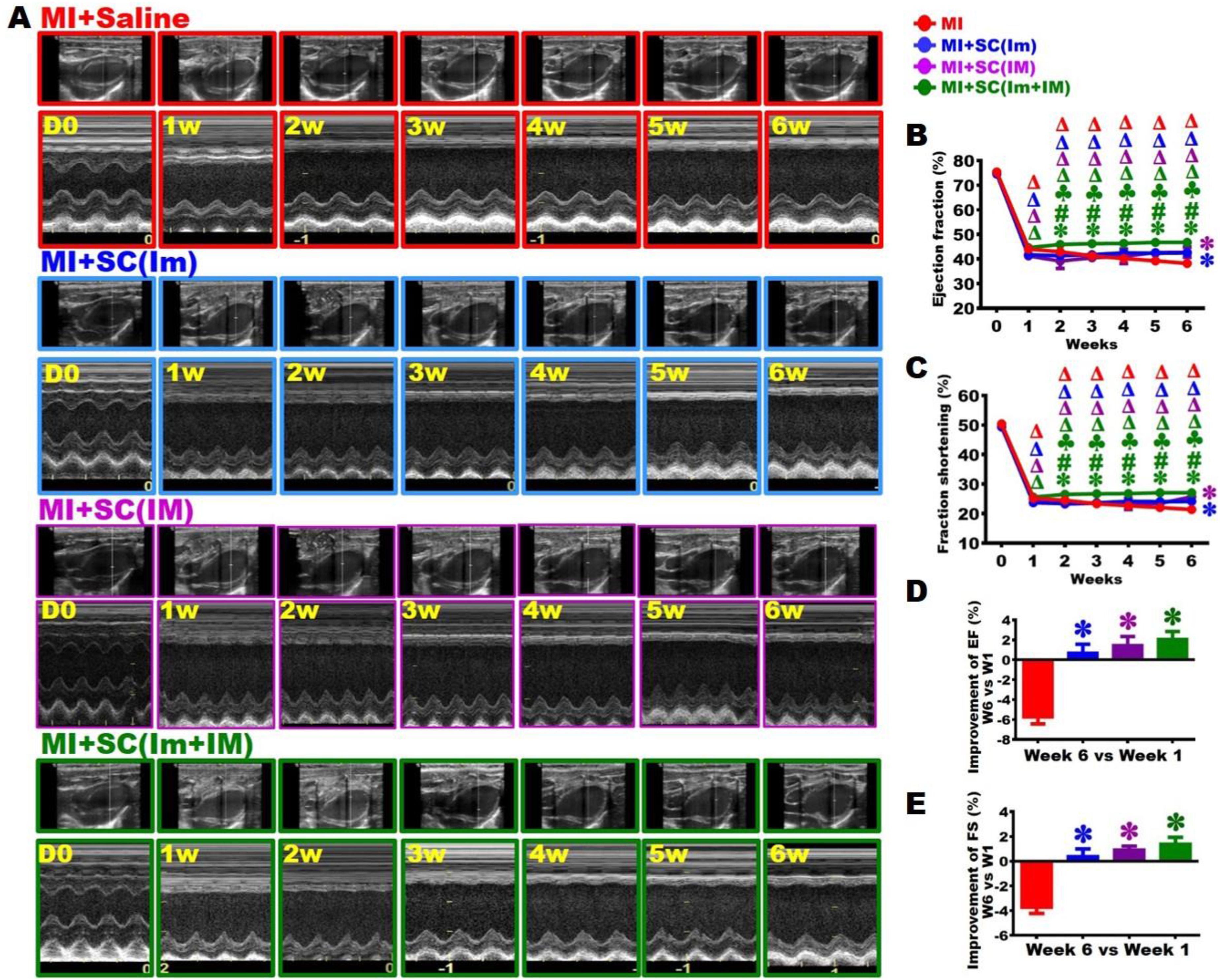
Furthermore, the left ventricular contractile function of rats in each group was analyzed weekly using MRI. At baseline, EF and FS were comparable between the MI+SC(Im) and MI+SC(Im+IM) groups (approximately 73% and 48%). One week after MI, both parameters declined to around 42% and 24%. In the MI+SC(Im) group, this impairment persisted through Week 6 (EF 41%; FS 23%). In contrast, the MI+SC(Im+IM) group exhibited gradual functional recovery from Week 2 onward, achieving an EF of 52% and FS of 31% by Week 6, significantly higher than those in the MI+saline and MI+SC(Im) groups (Figure 3(a)–(c)). HUMSC transplantation improved myocardial function in rats with chronic MI. (a) Cardiac magnetic resonance imaging scans of the three rat groups were obtained every week at the basal level of the ventricles (designated as plane ❶). The upper panel presents images at maximum diastole, whereas the lower panel presents images at maximum systole. Quantification of ejection fraction (b) and fraction shortening (c) over the 6-week period, along with changes in ejection fraction (d) and fraction shortening (e) from Week 1 to Week 6. Significant reductions were observed in left ventricular contractility at Week 1 after injury, with progressive enlargement of the maximum diastolic diameter over time. HUMSC transplantation preserved left ventricular contractility.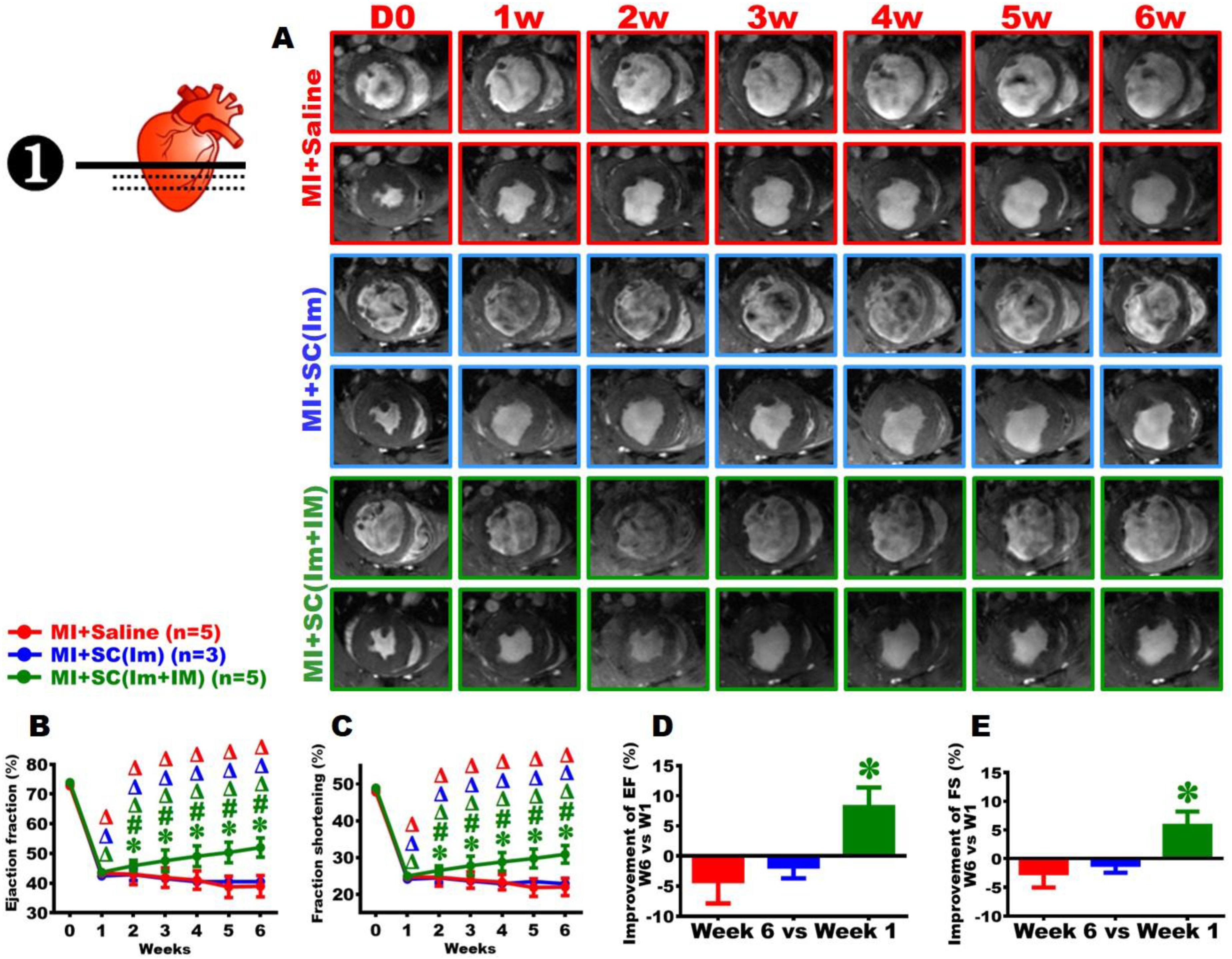
To minimize surgical variability, the cardiac function of each rat at Week 6 was subtracted from its corresponding Week 1 value, representing the individual change in cardiac function by MRI. In the MI+saline group, EF and FS declined by 4 % and 3%, respectively, indicating ongoing deterioration. The MI+SC(Im) group showed minimal decreases (EF: –1.9%; FS: –1.3%), suggesting attenuation of decline. Notably, the MI+SC(Im+IM) group exhibited functional recovery, with EF increasing by 8% and FS 6%, demonstrating significant improvement compared with the MI+saline group (Figure 3(d) and (e)).
From MRI analysis, functional decline was more pronounced at the mid-ventricular and apical levels than those at the base region (Supplemental Figure 3(a) – (c) and 4(a) – (c)). In the MI+SC(Im+IM) group, EF and FS at both levels improved significantly by Week 6, further confirming the therapeutic benefit of dual-site HUMSC transplantation (Supplemental Figure 3(d) and (e) and 4(d) and (e)).
Dual-site HUMSC transplantation preserved left ventricular volume in rats with chronic MI
At Week 6 post-MI, rats were euthanized and perfused, and the hearts were examined from both frontal and lateral views. In the MI+saline group, the left ventricle showed marked atrophy, with white fibrotic tissue replacing the infarcted myocardium. Similar fibrotic replacement was observed in the MI+SC(Im) and MI+SC(Im+IM) groups; however, the myocardium adjacent to the infarct zone appeared thicker than in the MI+saline group (Figure 4(a)). HUMSC transplantation preserved left ventricular myocardium in rats with chronic MI. (a) At Week 6, rats from each group were euthanized; representative gross images of rat hearts are presented, depicting the anterior (left) and lateral (right) views. (b) Hematoxylin–eosin-stained sections from the apex to the base (#1–#7) of the left ventricle are presented (magnification: 40×). (c–e) Fluorescent wheat germ agglutinin staining was performed to label cardiomyocyte membranes, thereby quantifying cardiomyocyte cross-sectional area in mid-ventricular sections (#4). HUMSC transplantation preserved a large volume of cardiac tissue and prevented morphological deformation of cardiomyocytes.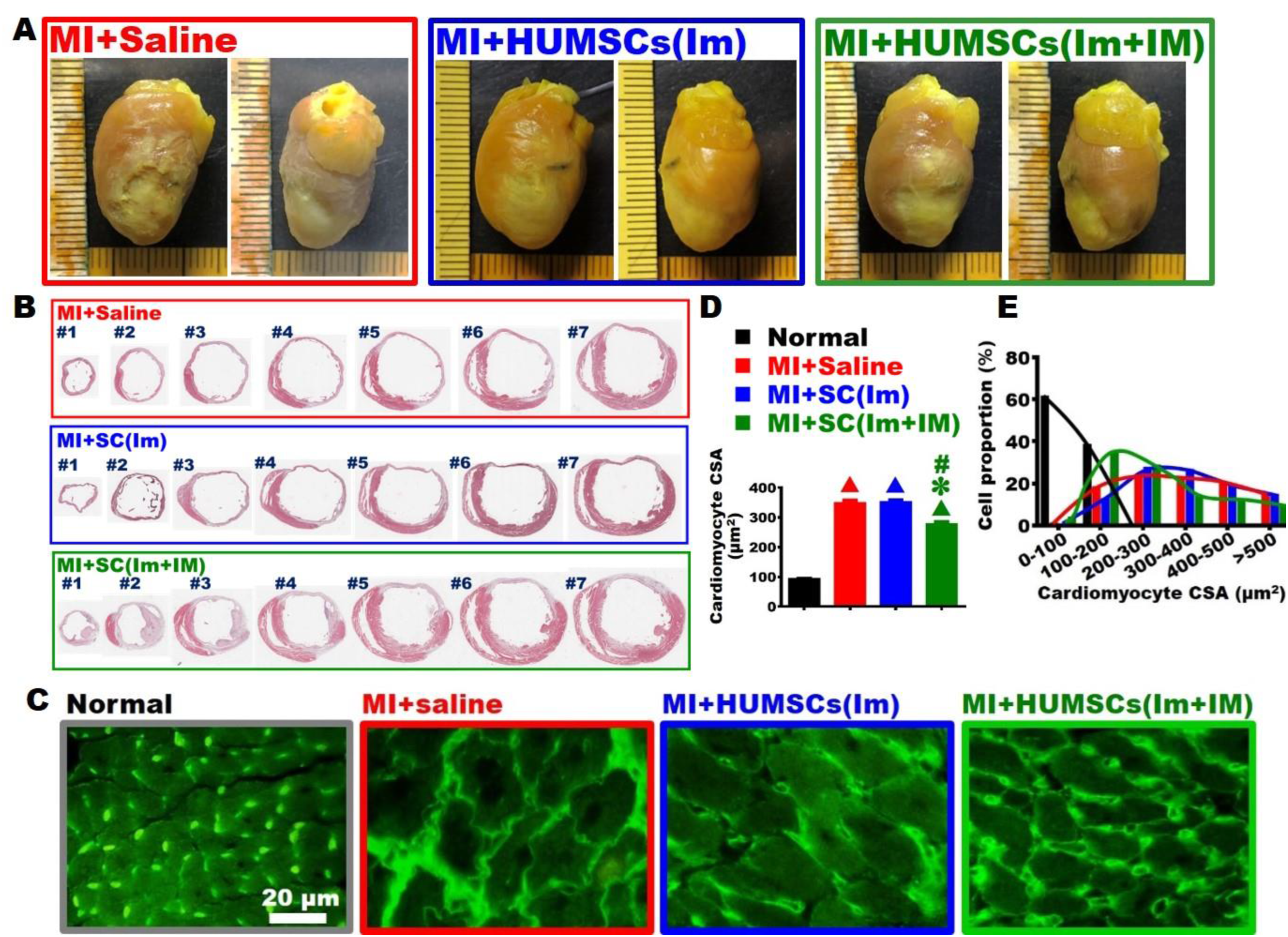
Histological analysis of serial cardiac sections (#1–#7, from apex to base) via H&E staining revealed severe wall thinning at the apex (#1 and #2) in the MI+saline group, with only sparse myocardial remnants. Atrophy extended to approximately two-thirds of the wall in the mid-ventricle (#3– #5) and one-third at the base (#6 and #7). In the MI+SC(Im) group, similar apical thinning was noted, but atrophy in the mid-ventricle was limited to about half the wall and diminished further toward the base. In the MI+SC(Im+IM) group, apical thinning was present, but the atrophied area in the mid-ventricle involved less than half the wall and was further reduced at the base, where myocardial thickness was greater than in the other two groups. These findings indicate that dual-site HUMSC transplantation better preserves myocardial structure and limits ventricular remodeling in chronic MI (Figure 4(b)).
Dual-site HUMSC transplantation mitigated the morphological deformation of cardiomyocytes in rats with chronic MI
Cardiac sections at the mid-ventricular level (#4) were stained with WGA to delineate cardiomyocyte membranes, and cross-sectional area was quantified. In the Normal group, most cardiomyocytes had a compact morphology with cross-sectional areas below 100 μm2. In contrast, the MI+saline group exhibited marked hypertrophy, with most cells ranging from 100 to 500 μm2. A similar enlargement was observed in the MI+SC(Im) group, showing a comparable distribution pattern. However, in the MI+SC(Im+IM) group, cardiomyocyte size was significantly reduced, with most cells falling between 100 and 300 μm2. Although still larger than in the Normal group, cardiomyocytes in the MI+SC(Im+IM) group were significantly smaller than those in the MI+saline and MI+SC(Im) groups. These results suggest that dual-site HUMSC transplantation helps attenuate pathological cardiomyocyte remodeling in chronic MI (Figure 4(c)–(e)).
Dual-site HUMSC transplantation suppressed the activation of cardiac fibroblasts in rats with chronic MI
Cardiac tissue sections from the apex (#2), mid-ventricle (#4), and base (#6) were stained with anti-α-SMA antibodies to identify activated cardiac fibroblasts, and the area of activated myofibroblasts in the infarcted region was quantified. In the MI+saline group, relatively large and dense clusters of activated myofibroblasts were observed in the apex (#2), mid-ventricle (#4), and base (#6), forming bundles within the infarcted region. The activated myofibroblast area in the MI+SC(Im+IM) group was significantly smaller, more scattered, and less dense than that in the MI+saline group. These findings suggest that HUMSC transplantation into both the myocardium and surrounding mediastinum can suppress the activation of cardiac fibroblasts, thereby downregulating collagen production in rats with chronic MI (Figure 5(a) and (b)). HUMSC transplantation suppressed inflammation and fibroblast activation in rats with chronic MI. (a) At Week 6 after injury, immunostaining of cardiac tissue sections with anti-α-smooth muscle actin antibodies revealed activated fibroblasts in infarct areas (left column) and border zones (right column) from sections near the apex (#2), mid-ventricle (#4), and base (#6). (b) Quantification of activated fibroblasts indicated that HUMSC transplantation reduced the number of activated fibroblasts in the hearts of rats with chronic MI. (c) Immunostaining with anti-ED1 antibodies was performed to detect macrophages within the infarcted and peri-infarcted regions. (d) Quantitative analysis demonstrated that HUMSC transplantation slightly reduced the overall number of macrophages in the heart. (e) Immunostaining with anti-CD163 antibodies was performed to label M2 macrophages in rat hearts. (f) The quantification results indicated that HUMSC transplantation increased the number of M2 macrophages and, moreover (g) increased the proportion of M2 macrophages among total macrophages. (h) Immunostaining with anti-CD31 antibodies was performed to label vascular endothelial cells. (i) The quantification results indicated that HUMSC transplantation increased the number of blood vessels.
Dual-site HUMSC transplantation strengthened the cardiac anti-inflammatory response in rats with chronic MI
Cardiac tissue sections from the apex (#2), mid-ventricle (#4), and base (#6) were analyzed for inflammation using ED1 immunostaining to identify macrophages. In the MI+saline group, macrophage infiltration was markedly elevated at all levels, with cells displaying heterogeneous sizes. In the MI+SC(Im+IM) group, macrophage numbers remained high; however, the cells appeared larger in size (Figure 5(c) and (d)).
To identify M2 macrophages, sections were stained with anti-CD163 antibodies. While M2 macrophages were present across all regions in the MI+saline group, their numbers at the mid-ventricle and base were significantly higher in the MI+SC(Im+IM) group, suggesting enhanced recruitment of reparative macrophages following HUMSC transplantation (Figure 5(e) and (f)). Quantification of M2 macrophages as a proportion of total macrophages revealed that, in the MI+saline group, M2 cells accounted for approximately 44%–52% across all regions. In contrast, the MI+SC(Im+IM) group showed a markedly increased proportion of 78%–87%. These findings indicate that dual-site HUMSC transplantation promotes M2 macrophage polarization and may enhance the anti-inflammatory response in chronic MI (Figure 5(g)).
Dual-site HUMSC transplantation promoted cardiac vascularization in rats with chronic MI
Cardiac tissue sections from the MI+saline and MI+SC(Im+IM) groups, near the ventricular base (#6), were analyzed through immunostaining with anti-CD31 antibodies to label vascular endothelial cells. The number of blood vessels was quantified. In the border zone of the damaged area, the MI+SC(Im+IM) group exhibited a significantly higher number of blood vessels than did the MI+saline group. These findings suggest that HUMSC transplantation into both the myocardium and surrounding mediastinum promotes vascularization, thereby supporting blood flow in the damaged border zone (Figure 5(h) and (i)).
HUMSCs survived and were distributed in the hearts of rats with chronic MI
Cardiac tissue sections from the MI+SC(Im) and MI+SC(Im+IM) groups, near the ventricular base (#6), were analyzed through immunostaining with anti-human nuclei antibodies to identify HUMSCs and assess their survival in the rat heart. The results confirmed the presence of HUMSCs within the cardiac tissue, with the majority concentrated in the infarcted area and a substantial portion distributed in the surrounding damaged regions (Figure 6(a)). HUMSCs survived and were scattered in the hearts of rats with MI without differentiation. (a) Immunostaining of sections near the ventricular base (#6) with anti-human nuclei antibody highlighted the presence and distribution of HUMSCs. (b) HUMSCs transplanted into rat hearts did not differentiate into vascular endothelial cells or cardiomyocytes. The asterisk (*) in the schematic indicates the site where HUMSCs were transplanted.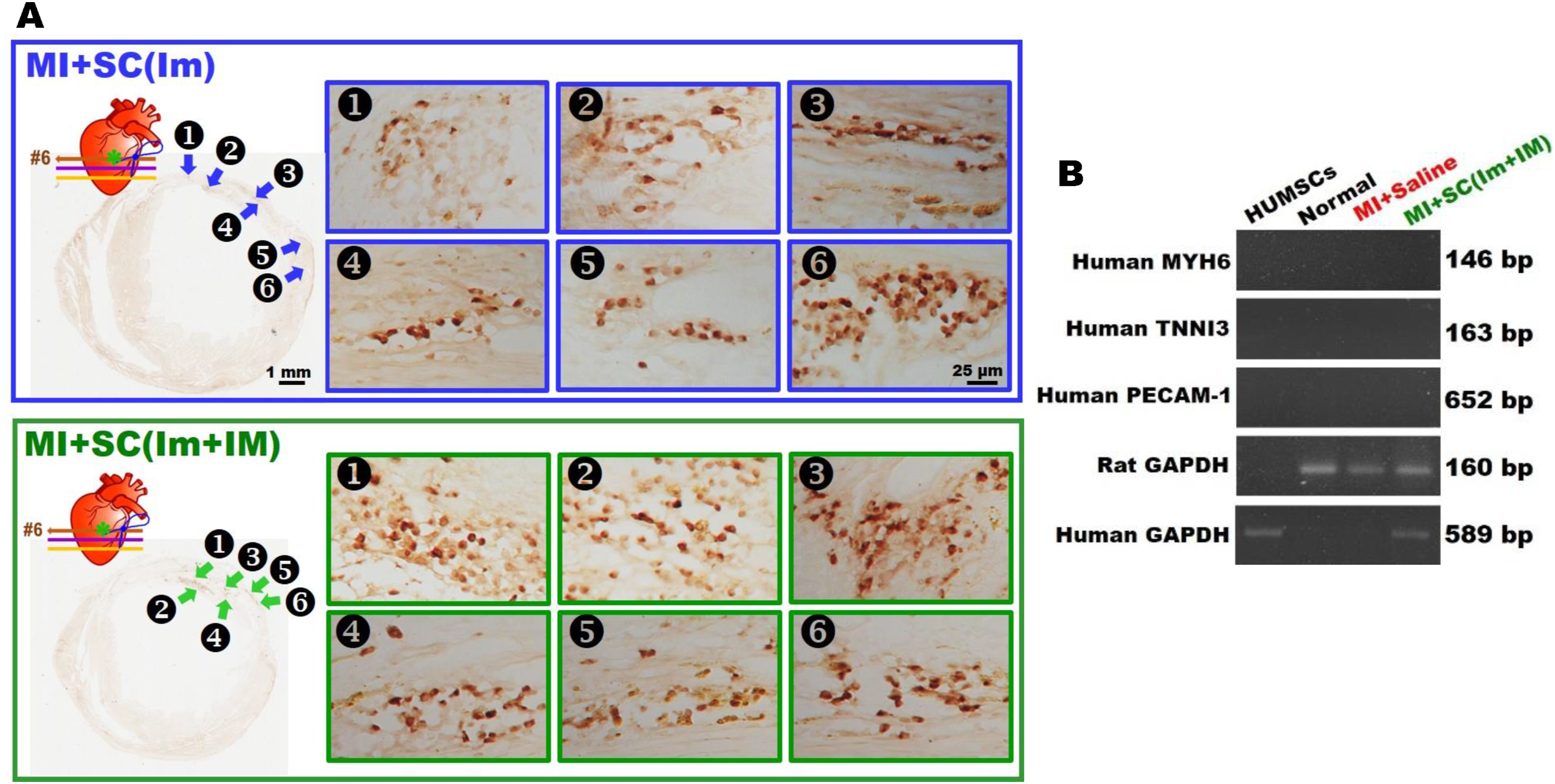
HUMSCs transplanted into rat hearts did not differentiate into vascular endothelial cells or cardiomyocytes
At Week 6, cardiac tissue samples were collected from each group. Reverse transcription PCR was performed to analyze the differentiation potential of HUMSCs. Human GAPDH was used as a positive control for HUMSCs, human PECAM1 was used as a biomarker of vascular endothelial cells, and human MYH6 and TNNI3 were used as biomarkers of cardiomyocytes. The results revealed that in the Normal and MI+saline groups, only rat GAPDH was expressed because no HUMSCs were transplanted. By contrast, in the MI+SC(Im+IM) group, both human GAPDH and rat GAPDH were detected, confirming the presence of HUMSC-derived genetic material due to transplantation. However, human MYH6, TNNI3, and PECAM1 were not detected in the heart samples from the MI+SC(Im+IM) group, which indicated that HUMSCs did not differentiate into cardiomyocytes or vascular endothelial cells. These findings suggest that the therapeutic effects of HUMSCs in chronic MI are not mediated by direct differentiation into cardiac or vascular cells (Figure 6(b)).
Discussion
In this study, we ellucidated that transplanting a large number of HUMSCs into the myocardium surrounding the infarct site while also applying them outside the heart may not only prevent additional myocardial degeneration, but also improve myocardial function.
We previously demonstrated that greater numbers of implanted HUMSCs were associated with better therapeutic outcomes in rat models of various diseases. These findings suggest that the survival and retention of transplanted HUMSCs within target tissues are critical determinants of tissue regeneration.7–21 To enhance myocardial repair, HUMSCs were directly implanted into the myocardium to maximize therapeutic efficacy. However, due to the limited thickness of the rat ventricular wall, direct intramyocardial injection of large numbers of HUMSCs was technically challenging. Therefore, additional HUMSCs were transplanted into the mediastinal space adjacent to the coronary ligation site. In our previous studies, 1×106 HUMSCs were transplanted into the cerebellum, 11 whereas 2.5×107 HUMSCs were administered into the lungs.19–21 Based on the relative sizes of the heart and mediastinal cavity, 4×106 HUMSCs were injected into the peri-infarct myocardium and 2.5×107 HUMSCs into the mediastinum. Consequently, rats in the MI+SC (Im+IM) group received a total of 2.9×107 HUMSCs. We suggest that transplantation of a larger number of HUMSCs may result in superior therapeutic efficacy. Following the initial thoracotomy for coronary artery ligation, fibrotic connective tissue had formed within the mediastinal space, allowing the implanted HUMSCs to remain localized and minimizing leakage into surrounding areas.
Our results revealed that the MI+SC(Im+IM) group received greater therapeutic benefits than did the MI+SC(Im) group. This difference may be attributable to the relatively high total number of transplanted HUMSCs and the strategic placement of the cells in the mediastinal space, which mitigated the risk of additional myocardial injury associated with direct puncture implantation. Our experimental findings revealed that HUMSCs did not differentiate into cardiomyocytes or vascular endothelial cells. We suggest that the transplanted HUMSCs exerted their therapeutic effects primarily through paracrine effects. Accordingly, the greater number of HUMSCs located within the mediastinal space may have provided additional paracrine support to prevent myocardial deterioration, which could explain the significantly better preservation of myocardial contractile function observed in the MI+SC(Im+IM) group.
Various stem cell transplantation strategies have been explored for the treatment of MI. Most studies have focused on direct myocardial implantation to achieve tissue repair 22,27–29 Other approaches have included intravenous delivery and coronary artery transplantation. Lim et al. administered HUMSCs intravenously, whereas Liu et al. transplanted them into the coronary artery, both of which successfully prevented myocardial deterioration and preserved ventricular contractile function.24,30 In another study, human embryonic stem cell–derived cardiomyocyte clusters sewn onto the surface of the mouse heart conferred therapeutic benefits. 31 Perin et al. investigated bone marrow mesenchymal stem cell transplantation in a canine model of MI; one group received cells through coronary artery infusion, whereas the other underwent endocardial implantation. Their results indicated that only the endocardial-implanted group exhibited improved cardiac output, increased vascular density, and reduced fibrosis. 23 Most studies performed intramyocardial stem cell transplantation during the acute phase following coronary artery ligation (either immediately or within 90 minutes). At the time of transplantation, the ventricular wall had not yet become thinned, and these studies demonstrated prevention of further deterioration in myocardial function as well as therapeutic benefits for acute myocardial infarction.4–6 In the present study, HUMSCs were transplanted intramyocardially one week after permanent coronary artery ligation, at a time when echocardiographic and cardiac MRI evaluations had already confirmed thinning of the anterior wall of the left ventricle. We suggest that the limited therapeutic effect observed in the MI+SC(Im) group may be attributable to the different timing of transplantation, resulting in outcomes that differed from those reported in the published studies involving stem cell transplantation during the acute phase of myocardial infarction.4–6
Many studies have investigated the therapeutic mechanisms of stem cell transplantation in acute phase or chronic phase of MI. Liu et al. transplanted human embryonic stem cell–derived cardiomyocytes into the myocardium of monkeys 2 weeks after MI. The results revealed improved EF and reduced fibrosis in the treatment group. Over time, the transplanted cardiomyocytes became more mature, exhibiting striations, gap junctions, and alignment into bundles; increased vascularization was noted within the transplanted region, further improving cardiac function. 28 Our study revealed that transplanted HUMSCs did not differentiate into cardiomyocytes or vascular endothelial cells, suggesting that cardiac repair was mediated through a paracrine effect rather than direct differentiation. A similar observation was also reported by Liang et al. 32 In the future, simultaneously transplanting both HUMSCs and differentiated cardiomyocytes may further advance the treatment of chronic MI and heart failure. This is an area we look forward to exploring.
Zhang et al. performed permanent ligation of the LAD in pigs and then immediately transplanted HUMSCs into the myocardium; They observed a marked reduction in fibrosis in the treatment group. 5 Similarly, Lim et al. transplanted pig umbilical mesenchymal stromal cells at 120 min and 4 weeks after permanent ligation of the LAD in pigs; they observed reductions in the levels of inflammation-related cytokines, such as interleukin-6 and tumor necrosis factor-α. 30 In our study, immunostaining with anti-ED1 antibodies (to label macrophages) and anti-CD163 antibodies (to label M2 macrophages) revealed that HUMSC transplantation up-regulated the expression of M2 macrophages, and thereby effectively alleviating cardiac inflammation in rats with chronic MI and strengthening the anti-inflammatory response. Immunostaining with anti-α-SMA antibodies (to label activated fibroblasts) indicated that fibroblast distribution was relatively dispersed in rats treated with HUMSCs; moreover, fibroblast count was significantly lower in these rats than in untreated rats. HUMSC transplantation prevented excessive extracellular matrix accumulation and limited fibrosis progression in the hearts of rats with chronic MI.
Evidence suggests that stem cell transplantation, whether administered during the acute or chronic phase of MI, confers therapeutic benefits by improving ventricular function, primarily by promoting vascularization.24,27,31,33 In our study, immunostaining with anti-CD31 antibodies (to label vascular endothelial cells in the heart) revealed that HUMSC transplantation increased the number of blood vessels, thereby ensuring blood supply to the damaged border region.
Sharp III et al. performed temporary occlusion of the LAD in pigs for 90 min through balloon angioplasty; this was followed by ischemia–reperfusion and immediate transplantation of bone marrow mesenchymal stromal cells into the injured myocardium. They found that the treatment group had smaller and more cardiomyocytes than did the untreated group. 4 In our study, WGA fluorescent staining (to label the cardiomyocyte membrane and quantify the cross-sectional area of cardiomyocytes) revealed that HUMSC transplantation helped maintain cardiomyocytes in a relatively small and normal morphology.
There are three major limitations to the clinical application of HUMSCs transplantation for chronic MI or heart failure: the number of transplanted cells, the timing of transplantation, and the route of administration. First, regarding the number of transplanted cells, our results suggest that a sufficient number of stem cells is required to achieve therapeutic efficacy. However, in patients with chronic MI, the optimal cell dose should be carefully evaluated according to body weight and personal medical history. Second, regarding the timing of transplantation, stem cells were transplanted one week after permanent coronary artery ligation in this study, which was effective in attenuating further deterioration of cardiac function. In clinical practice, however, performing stem cell transplantation within one week after coronary occlusion may be difficult. Third, in this study, the cells were delivered through thoracotomy with intramyocardial and mediastinal implantation. Since patients with heart failure are often already in a fragile condition, open-chest surgery carries substantial risk. How to achieve optimal clinical therapeutic efficacy requires further careful consideration.
Conclusion
In this study, chronic MI was induced via permanent LAD ligation in rats. HUMSC transplantation mitigated cardiac deterioration by reducing inflammation and fibrosis, enhancing vascularization, preserving cardiomyocytes, and limiting their deformation. Despite no evidence of HUMSC differentiation, the therapeutic benefits appeared to result from paracrine signaling. Ventricular function improved by 7- 8%. Future research may explore higher cell doses or HUMSC-derived cardiomyocytes to enhance efficacy. These findings support HUMSC transplantation as a promising therapy for chronic MI and heart failure.
Supplemental material
Supplemental material - Transplantation of human umbilical mesenchymal stromal cells attenuates heart failure progression in a rat model
Supplemental material for Transplantation of human umbilical mesenchymal stromal cells attenuates heart failure progression in a rat model by Chen-Yuan Hsiao, Jian-Hong Ye, Chang-Ching Yeh, Pei-Jiun Tsai, Po-Hsun Huang, Cheng-Hsiung Huang, and Yu-Show Fu in Cell Transplantation.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to Dr. Arthur Er-Terg Chiou of the Institute of Biophotonics, National Yang Ming Chiao Tung University, for his invaluable assistance in critically reviewing the manuscript and providing English language editing. All authors declare that no scientific data has been generated or modified using AI in this manuscript.
Ethical considerations
The use of human umbilical cord in this study was approved by the research project titled “Study on the potential and mechanism of xenograft of human umbilical mesenchymal stem cells from Wharton’s jelly treats chronic myocardial infarction in rats-in vivo and in vitro studies” and granted by the Institutional Review Board of Taipei Veterans General Hospital. The ethics approval number for this project is 2021-12-016CC, and the date of approval is Dec 20,2021.
Consent to participate
All expectant mothers who choose to donate their umbilical cords have provided written informed consent for the use of umbilical cords in this study.
Author contributions
Hsiao CY and Ye JH performed the experiments and analyzed the data. Yeh CC and Tsai PJ supported the materials. Huang PH discuss the results. Hsiao CY and Fu YS wrote the manuscript. Huang CH and Fu YS designed the experiments, reviewed and edited drafts of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant MOST 111-2320-B-A49-013 from the National Science and Technology Council in Taiwan.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data included in this study are available upon request by contact with the corresponding author.
Animal approval
The ethics approval for the research project titled “Study on the potential and mechanism of xenograft of human umbilical mesenchymal stem cells from Wharton’s jelly treats chronic myocardial infarction in rats-in vivo and in vitro studies” was granted by the Medical and Laboratory Animal Ethics Committee of National Yang Ming Chiao Tung University, Taipei. The approval number for this project is 1110308, and the date of approval is March 03,2022.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.