
Abstract
Intramedullary cellular transplantation within the human spinal cord has historically been regarded as a highly experimental intervention associated with substantial theoretical risk. However, cumulative clinical evidence progressively challenges this perception. Multiple early-phase clinical studies have demonstrated the technical feasibility and procedural tolerability of intramedullary and intralesional cellular delivery in spinal cord injury (SCI), employing heterogeneous cellular products, including bone marrow-derived mononuclear cells, mesenchymal stromal cells (MSCs), and neural stem cells. Despite considerable heterogeneity in cellular composition, dosing strategies, injection volumes, and delivery paradigms, severe injection-related complications remain uncommon. Reported adverse events are predominantly mild and transient, while procedure-induced neurological deterioration has not emerged as a reproducible safety signal. These observations suggest that controlled spinal cellular administration may represent a biologically tolerated intervention rather than an intrinsically destabilizing procedure. Beyond procedural considerations, long-term biological safety remains a central dimension of translational evaluation. While theoretical concerns persist — particularly regarding tumorigenesis, clonal selection, and potential genomic instability associated with ex vivo MSC expansion — currently available clinical data have not identified reproducible or causally attributable neoplastic transformation signals within currently reported follow-up durations. Interpretation of long-term safety outcomes therefore requires careful distinction between theoretical biological plausibility and empirical clinical observations. In parallel, minimally manipulated autologous cellular products such as freshly isolated stromal vascular fraction (SVF) introduce a complementary translational framework. By preserving physiological cellular heterogeneity and eliminating risks associated with ex vivo expansion, SVF-based approaches further emphasize the need to reinterpret cellular variability as an intrinsic biological property rather than a marker of product instability. Collectively, available evidence supports consideration of multidimensional safety frameworks integrating procedural, short-term biological, and long-term theoretical domains. Future progress will depend on harmonized reporting standards, extended longitudinal evaluation, and large-scale collaborative datasets capable of refining biologically grounded safety models for spinal cellular therapies.

Keywords
Highlights
• Intramedullary MSC delivery demonstrates consistent procedural tolerability in humans. • No reproducible or treatment-attributable neoplastic events reported to date. • Theoretical tumorigenic risk primarily relates to prolonged ex vivo expansion. • GMP-compliant manufacturing mitigates genomic instability concerns. • Cumulative SCI and ALS data expand documented intramedullary safety exposure.
Introduction
Intramedullary cell transplantation within the human spinal cord has historically been regarded as a highly experimental and potentially hazardous intervention. 1 The perceived vulnerability of spinal cord tissue, combined with concerns regarding procedure-induced neurological deterioration, has long limited clinical exploration. Over the past decade, however, multiple first-in-human investigations have progressively demonstrated the technical feasibility of direct intramedullary cellular delivery in spinal cord injury (SCI), without evidence of prohibitive procedural toxicity.2–4 Given the persistent functional disability, long-term healthcare burden, and substantial socioeconomic impact associated with SCI, development of safe regenerative strategies remains a major translational priority. 5
Importantly, early clinical studies involved heterogeneous cellular products, including neural stem cells and other non-mesenchymal populations, yet consistently reported acceptable procedural safety profiles. These findings challenge long-standing assumptions regarding the intrinsic intolerance of the human spinal cord to focal therapeutic targeting and suggest that controlled intramedullary interventions may be biologically tolerated under appropriate conditions.
Concurrently, mesenchymal stromal cells (MSCs) have emerged as leading candidates in regenerative medicine owing to their immunomodulatory, trophic, and neuroprotective properties. Despite their extensive clinical investigation, two principal safety concerns continue to shape translational and regulatory discussions: first, the procedural risks associated with intramedullary administration, and second, the long-term biological safety of transplanted MSCs, particularly the theoretical oncogenic risks linked to ex vivo expansion.
While procedural safety data derived from intramedullary transplantation studies provide important contextual reassurance for MSC-based strategies, long-term oncological safety remains a central point of debate. This debate is largely rooted in experimental observations of spontaneous chromosomal abnormalities during prolonged in vitro expansion, as well as theoretical parallels drawn from stem cell plasticity and tumor biology. To date, however, available clinical evidence has not identified reproducible tumorigenic signals following MSC transplantation, even in studies involving extended follow-up durations.
In parallel, minimally manipulated autologous cellular products, including freshly isolated stromal vascular fraction (SVF), have attracted increasing interest. Prepared without ex vivo expansion, SVF introduces a distinct safety paradigm characterized by preserved physiological cellular heterogeneity and immediate therapeutic availability. Recent evidence emphasizes the favorable safety profile of SVF-based therapies across diverse clinical contexts. 6
Given the expanding clinical experience with intramedullary interventions and the evolving landscape of regenerative strategies, a structured reassessment of MSC safety appears warranted. The present review therefore critically re-evaluates both the procedural safety of intramedullary cellular delivery and the long-term oncological considerations associated with MSC transplantation in humans.
Methods
The search was conducted between January and March 2026. After removal of duplicate records and screening of titles and abstracts, full-text articles were assessed for relevance. Studies were selected based on their contribution to procedural safety, biological safety, or oncological risk assessment in human spinal cellular transplantation. Reference lists of included articles were also manually screened to identify additional relevant publications. Search terms included combinations of: “mesenchymal stromal cells”, “mesenchymal stem cells”, “intramedullary”, “intraspinal”, “spinal cord injury”, “amyotrophic lateral sclerosis”, “tumorigenesis”, “oncological safety”, and “cell transplantation”.
Clinical studies involving direct intramedullary, intralesional, or intraspinal cellular transplantation in humans were prioritized. In the present review, “intramedullary” refers to direct injection within spinal cord parenchyma, whereas “intralesional” refers to administration within lesion cavities or structurally altered injury sites. Although partially overlapping in clinical practice, these approaches may involve distinct procedural and biological considerations. Both MSC-based and non-MSC cellular transplantation studies were included when relevant to procedural or biological safety considerations. Preclinical studies were selectively considered to contextualize mechanistic aspects of genomic instability and tumorigenesis.
Articles not involving spinal cellular delivery, duplicate reports, and studies lacking safety-related outcomes were excluded. Given the heterogeneity and limited number of available clinical studies, a narrative synthesis approach was adopted rather than formal meta-analysis.
Review
Procedural safety of intramedullary and intralesional cellular delivery
Injection characteristics, delivery paradigms, and reported procedural safety outcomes across published human intramedullary and intralesional cellular transplantation studies.
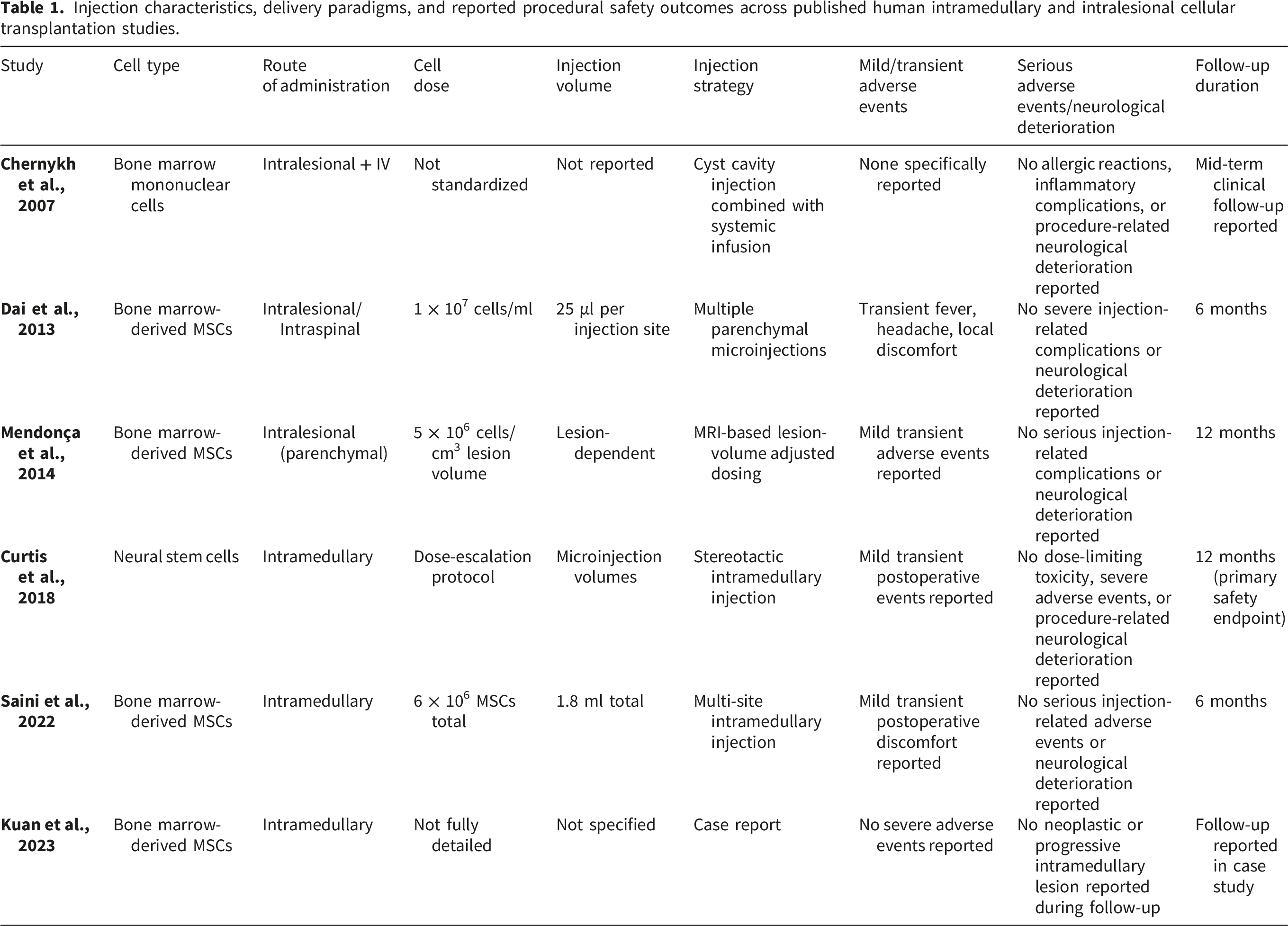
Intramedullary and intralesional cellular transplantation within the human spinal cord has long been perceived as inherently hazardous due to the structural fragility of neural tissue and the theoretical risk of procedure-induced neurological deterioration. However, cumulative clinical evidence increasingly challenges this assumption. Across early-phase clinical studies employing diverse cellular products, direct spinal delivery has consistently demonstrated an acceptable procedural safety profile.
As summarized in Table 1, heterogeneous cellular populations, including bone marrow-derived mononuclear cells, MSCs, and neural stem cells, have been administered using distinct injection paradigms. These approaches range from focal microinjection strategies, 7 lesion-volume adjusted dosing models, 8 bulk intramedullary injections, 4 and stereotactic dose-escalation designs. 3
Despite substantial heterogeneity in cell dose, injection volume, and delivery techniques (Table 1), severe injection-related complications remain remarkably uncommon. Reported adverse events are predominantly mild and transient, including low-grade fever, headache, or local discomfort. Importantly, no reproducible pattern of procedure-induced neurological deterioration has been identified across studies (Table 1).
This convergence of safety observations across divergent procedural strategies suggests that controlled spinal cellular administration may represent a biologically tolerated intervention rather than an intrinsically destabilizing insult.
Heterogeneity of dosing and injection strategies
A defining characteristic of spinal cellular transplantation studies lies in the considerable variability of dosing paradigms. Rather than reflecting methodological inconsistency, this heterogeneity may represent a biologically rational adaptation to lesion-specific variables. However, this heterogeneity also complicates interpretation of the available safety evidence. Differences in cell source, manufacturing processes, expansion protocols, cell dose, injection volume, and delivery routes may influence both biological activity and adverse event profiles. Consequently, the apparent consistency of safety findings across studies should not be interpreted as evidence of equivalence between cellular products or administration strategies. The current literature remains insufficient to determine whether specific products, doses, or delivery paradigms confer differential safety risks.
Distinct conceptual dosing strategies are evident in Table 1, including concentration-based administration, 7 lesion-volume normalized cell density, 8 empiric fixed-dose regimens, 4 and dose-escalation safety designs. 3 These divergent approaches reflect fundamental uncertainties regarding optimal therapeutic dose metrics in structurally heterogeneous spinal cord lesions.
Importantly, procedural safety stability across heterogeneous dosing frameworks (Table 1) reinforces the interpretation that variability in injection parameters does not inherently translate into increased procedural risk.
Long-term biological safety considerations
Beyond procedural tolerability, long-term biological safety remains a central consideration in cellular therapy discussions. Theoretical concerns surrounding tumorigenesis, ectopic tissue formation, aberrant differentiation, and delayed neurological deterioration continue to shape regulatory and translational debates.
Long-term biological safety domains reported across spinal cellular transplantation studies. Data derived from published early-phase clinical studies in spinal cord injury and intraspinal amyotrophic lateral sclerosis trials.9–12 Follow-up durations remain limited relative to lifetime oncological risk assessment.
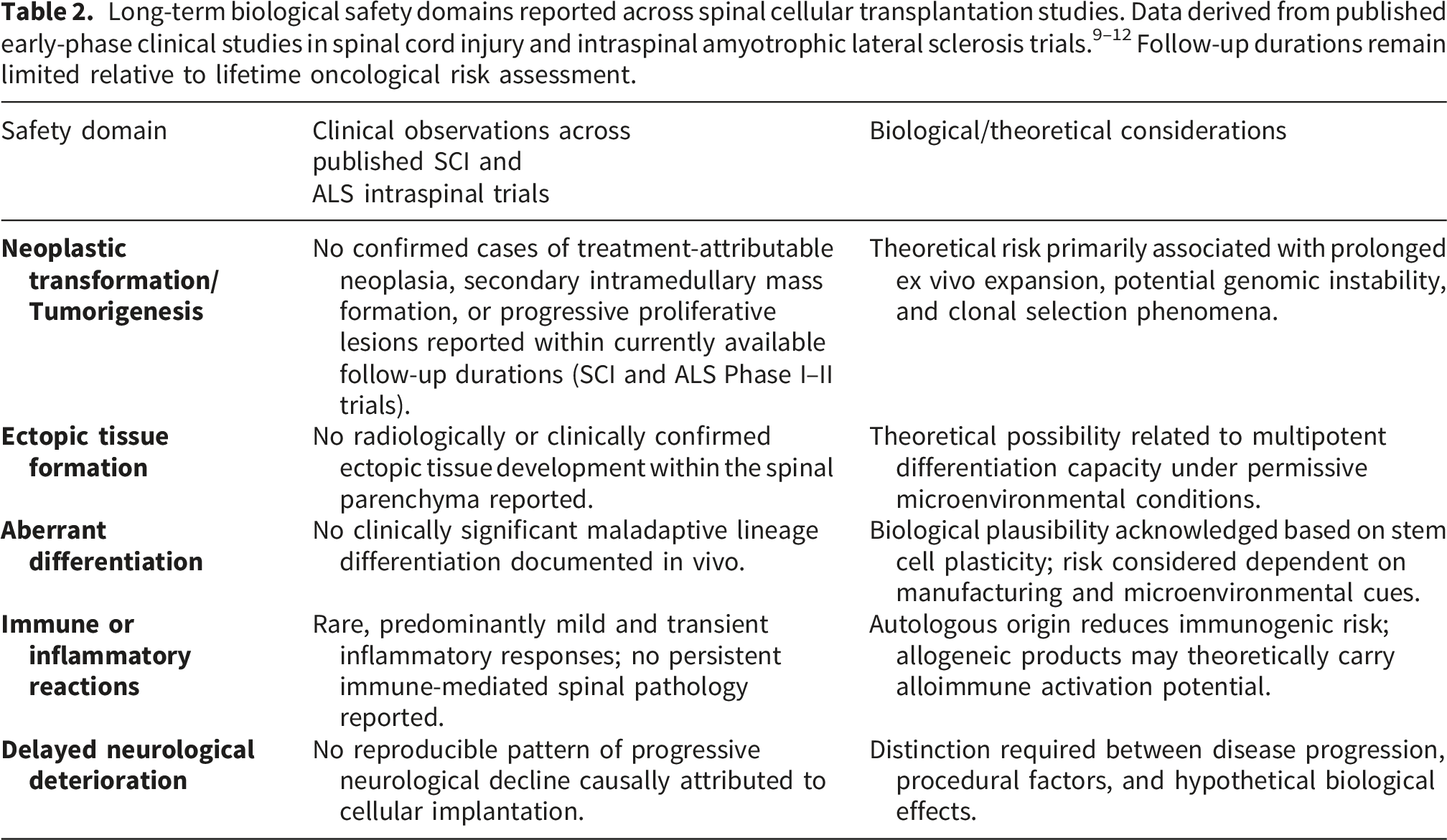
This consistency across early-phase trials is further supported by isolated case reports describing intramedullary MSC implantation in complete spinal cord injury without emergence of neoplastic or progressive mass lesions during reported follow-up intervals. 13
Importantly, interpretation of long-term safety outcomes (Table 2) must distinguish between empirical clinical observations and theoretical biological plausibility.
From a mechanistic perspective, theoretical concerns regarding MSC-associated tumorigenesis primarily arise from observations of genomic instability during prolonged in vitro expansion. Extended culture duration may promote replicative senescence, epigenetic drift, telomere shortening, and, in rare experimental contexts, chromosomal abnormalities or clonal selection events. Such alterations have been described predominantly in preclinical models under non-clinically compliant expansion conditions. Importantly, current Good Manufacturing Practice (GMP)-compliant protocols incorporate strict passage limits, cytogenetic monitoring, and release criteria designed to mitigate these risks. To date, no clinically verified cases of malignant transformation causally attributable to transplanted MSCs have been reported to date, although available follow-up durations remain limited in intramedullary human applications.
More broadly, despite extensive cumulative clinical exposure to culture-expanded MSC products across diverse therapeutic indications worldwide, no reproducible or causally established cases of treatment-induced malignant transformation have been documented in regulated clinical settings within reported follow-up durations.
Additional safety data relevant to intramedullary exposure derive from intraspinal cellular transplantation trials conducted in amyotrophic lateral sclerosis (ALS). Although pathophysiologically distinct from traumatic spinal cord injury, these studies involved direct lumbar and cervical intramedullary injections of mesenchymal stromal cells, bone marrow mononuclear cells, or neural stem cells. Across multiple Phase I and II trials, including extended follow-up analyses, no treatment-attributable tumor formation, secondary intramedullary mass lesions, or delayed proliferative complications have been reported.9–12
While extrapolation between neurodegenerative and traumatic contexts requires caution, these cumulative observations substantially expand documented human exposure to intraspinal cellular products without identification of a reproducible, treatment-attributable clinical oncogenic signal within currently observed follow-up intervals.
Conceptual implications for cellular therapy risk frameworks
Collectively, these findings support interpretation of spinal cellular transplantation safety within a multidimensional risk framework integrating procedural outcomes (Table 1) and long-term biological considerations (Table 2).
Procedural safety signals appear generally favorable across heterogeneous injection paradigms, while long-term biological risks remain largely theoretical within current clinical observation windows (Table 2). This dissociation between theoretical concerns and empirical safety signals highlights the need for biologically grounded risk interpretation models.
Importantly, the absence of observed tumorigenesis in clinical contexts must be interpreted within the framework of exposure time and biological plausibility. Theoretical oncogenic risk, while biologically conceivable, appears to require conditions (extended culture duration, genomic instability, immune escape) that may not be systematically present in clinically compliant MSC manufacturing protocols.
Limitations
Several limitations should be acknowledged when interpreting the findings of the present review. First, the available clinical literature remains characterized by substantial heterogeneity in study design, patient populations, cellular products, dosing strategies, and injection methodologies. Such variability inherently limits direct quantitative comparability across studies.
Second, reporting standards for injection parameters, including total cell dose, concentration, injected volume, and distribution strategies, were not uniformly applied. In several studies, critical procedural variables were incompletely described, reflecting the exploratory nature of early-phase clinical investigations.
Third, follow-up durations remain relatively limited when considering long-term biological safety outcomes, particularly with respect to theoretical risks such as tumorigenesis or delayed aberrant tissue responses. Absence of observed adverse events within current observation windows should therefore be interpreted cautiously and not as definitive exclusion of rare long-term events. Given the potentially prolonged latency of oncogenic processes, follow-up periods extending beyond 5-10 years may ultimately be required to adequately characterize very late biological risks associated with intramedullary cellular therapies.
Publication bias must also be considered, as early-phase studies reporting favorable procedural safety outcomes are more likely to reach publication than studies reporting severe adverse events or unsuccessful translational experiences.
Finally, the majority of available studies were designed primarily to assess feasibility and procedural safety rather than long-term biological endpoints. Consequently, conclusions regarding biological risk profiles remain probabilistic rather than deterministic.
Despite these limitations, the relative consistency of procedural safety observations across heterogeneous injection paradigms provides meaningful convergent evidence supporting the biological tolerability of controlled spinal cellular administration.
Future perspectives: SVF and minimally manipulated cellular therapies
Although no clinical studies have specifically evaluated intramedullary SVF injection in humans, minimally manipulated autologous cellular products have gained increasing attention in regenerative medicine as alternative approaches to culture-expanded MSC therapies. Unlike ex vivo expanded cellular products, freshly isolated SVF preserves the native cellular heterogeneity of adipose-derived tissue, including stromal progenitors, endothelial lineage cells, perivascular populations, and immune cells within a physiologically preserved cellular microenvironment. Importantly, SVF should not be conflated with mechanically derived stromal tissue products such as nanofat or stromal vascular tissue, which differ substantially in cellular composition, isolation methodology, and biological properties. 14
From a theoretical safety perspective, SVF introduces a distinct translational framework. Because preparation is performed without prolonged in vitro expansion, SVF may theoretically circumvent risks associated with prolonged ex vivo expansion, including culture-induced phenotypic drift, replicative senescence, and theoretical genomic instability. Immediate preparation and administration may additionally preserve endogenous cellular interactions while reducing manufacturing complexity. This logistical advantage may be particularly relevant in acute neurological settings, where time-dependent therapeutic windows may limit the feasibility of prolonged ex vivo expansion protocols. 15
Importantly, available clinical data across non-spinal applications have generally reported favorable short-term safety profiles for SVF-based therapies, with adverse events predominantly mild and transient. 6 Nevertheless, direct extrapolation to intramedullary administration remains speculative in the absence of dedicated human spinal studies.
Consequently, SVF should not currently be interpreted as an evidence-based alternative to intramedullary MSC transplantation, but rather as a potential future direction within the broader landscape of minimally manipulated cellular therapies. Further preclinical and clinical investigations will be required to determine whether preservation of physiological cellular heterogeneity may translate into distinct safety or biological properties in spinal applications.
Conclusions
Intramedullary and intralesional cellular transplantation within the human spinal cord has historically been regarded as a highly experimental intervention associated with substantial theoretical risk. However, cumulative clinical evidence progressively challenges this perception. Across heterogeneous studies employing diverse cellular products, controlled spinal cellular administration has demonstrated consistent procedural tolerability, with adverse events predominantly mild and transient.
Importantly, currently available early-phase data have not identified major procedural safety concerns despite substantial variability in cell type, dosing strategies, injection volumes, and delivery paradigms. This convergence suggests that spinal cellular interventions appear to be biologically tolerated within currently reported follow-up periods under appropriately controlled conditions rather than representing intrinsically destabilizing procedures.
Beyond procedural considerations, long-term biological safety remains a central dimension of translational evaluation. While theoretical concerns persist, particularly regarding tumorigenesis and aberrant tissue responses, currently available clinical evidence has not identified reproducible or causally attributable neoplastic events within reported observation windows. Interpretation of long-term safety outcomes therefore requires careful distinction between empirical observations and theoretical biological plausibility.
In parallel, minimally manipulated autologous cellular products such as SVF introduce a complementary translational framework. By preserving physiological cellular heterogeneity and eliminating risks associated with ex vivo expansion, SVF-based approaches further highlight the need to reinterpret cellular variability as an intrinsic biological feature rather than a marker of instability.
Collectively, these findings support the adoption of multidimensional safety frameworks integrating procedural, short-term biological, and long-term theoretical domains. Future progress will depend on harmonized reporting standards, prospective long-term registries, extended follow-up, and large-scale collaborative datasets. Continued vigilance through long-term surveillance and harmonized adverse event reporting will remain essential to definitively characterize the oncological risk profile of intramedullary MSC therapies.
Footnotes
Acknowledgements
The authors thank all investigators and clinical teams whose early-phase studies contributed to the advancement of spinal cellular transplantation research.
Ethical considerations
Ethical approval was not required for this narrative review, as no human participants, patient data, or animal experiments were directly involved.
Author contributions
CN and NS contributed equally to this work. CN participated in literature review, data interpretation, manuscript drafting, and critical revision of the manuscript. NS conceptualized the study, supervised the project, participated in literature review and interpretation, and critically revised the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No original datasets were generated or analyzed during the present study. All data discussed in this review are derived from previously published studies cited in the reference section.
Use of artificial intelligence statement
Artificial intelligence-assisted language tools were used exclusively for English language refinement and manuscript editing. No scientific data, analyses, results, references, or interpretations were generated by artificial intelligence. The authors remain fully responsible for the accuracy, originality, and integrity of the manuscript.