
Abstract
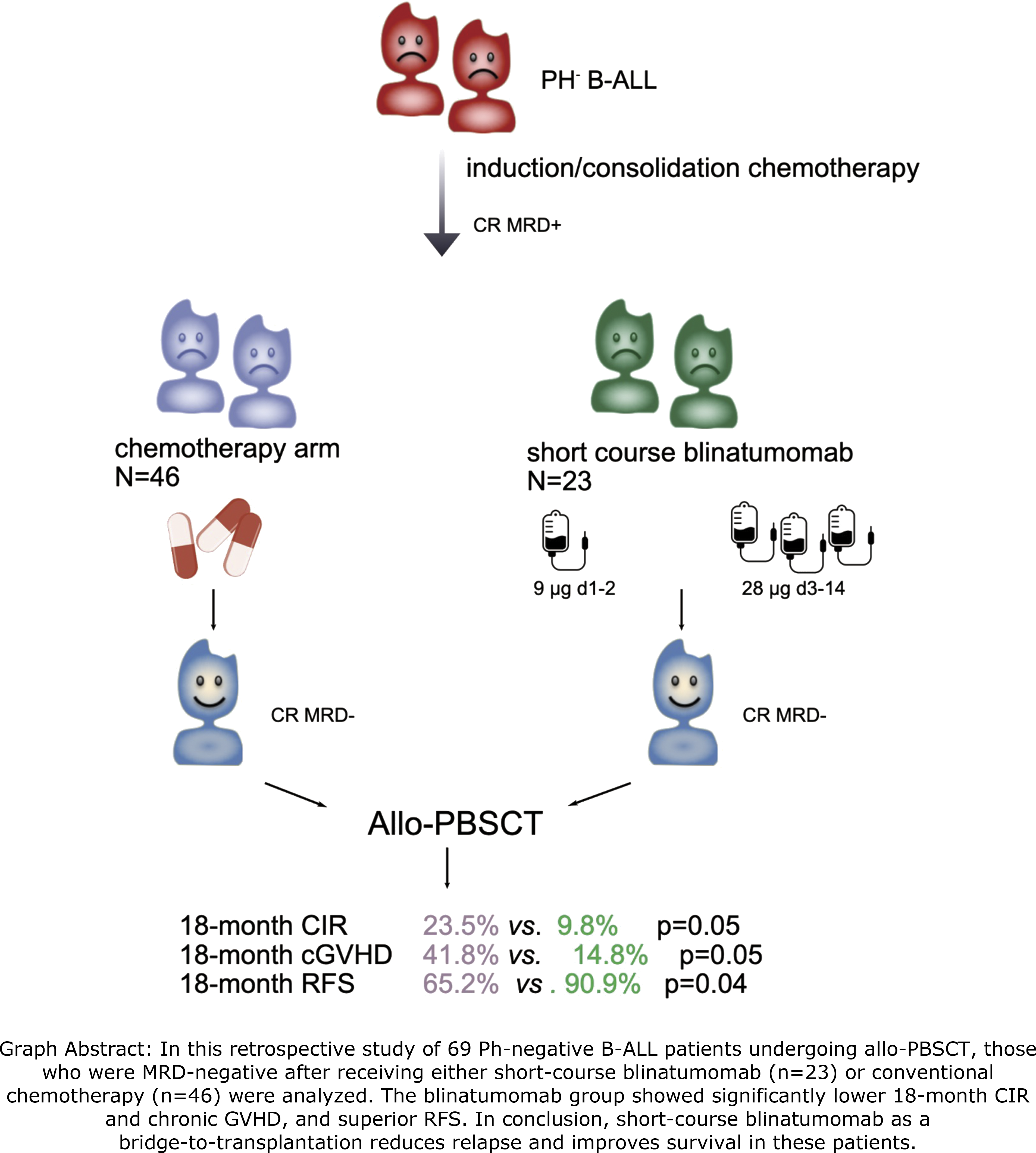
Post-transplant relapse remains the chief therapeutic challenge in Ph-negative B cell acute lymphoblastic leukemia (Ph- B-ALL). This retrospective study evaluated whether short-course blinatumomab for measurable resident disease (MRD) eradication could improve transplant outcomes. We compared 23 patients receiving pre-transplant short-course blinatumomab (2-week) for MRD eradication with 46 chemotherapy-only controls. All achieved MRD-negative before allogeneic peripheral blood stem cell transplantation (allo-PBSCT). Only two patients developed grade 2 cytokine release syndrome with blinatumomab. The neutrophil and platelet engraftment times were similar between the two groups. The blinatumomab cohort had a significantly lower 18-month cumulative incidence (CI) of relapse (p = 0.05) and chronic graft-versus-host disease (GVHD) (14.8% vs. 41.8%; p = 0.05), with comparable non-relapse mortality (NRM) (p = 0.98) and 180-day grade II-IV acute GVHD rates (p = 0.93). Consequently, this cohort showed superior 18-month relapse-free survival (RFS) (90.9% vs. 65.2%; HR 0.30, 95% CI 0.09-1.04; p = 0.04), improved 18-month overall survival (OS) (95.7% vs. 81.9%; HR 0.20, 95% CI 0.03-1.71), and a trend toward better GVHD-free and relapse-free survival (GRFS) (74.71% vs. 63.71%; HR 0.64, 95% CI 0.23-1.78). Multivariate analysis confirmed blinatumomab as an independent favorable factor for RFS. In conclusion, short-course blinatumomab as a bridge-to-transplantation could reduce the risk of relapse and improve survival for Ph- B-ALL patients undergoing allo-PBSCT.
Keywords
Introduction
Philadelphia chromosome-negative B-cell acute lymphoblastic leukemia (Ph-negative B-ALL) is the most common type of adult ALL. Although nearly 90% of patients could achieve complete remission (CR) with chemotherapy, relapse rates remain high (40-50%), and the 5-year overall survival (OS) rate is only ranging from 30% to 50%.1,2 Even in the allogeneic hematopoietic stem cell transplantation (allo-HSCT) era, post-transplant relapse rates remain substantial (20-30%).1,3
Pre-transplant measurable residual disease (MRD) status is one of the most important risk factors for post-transplant relapse. Clinical evidence has demonstrated that the patients with positive MRD prior to transplantation significantly increased the risk of relapse and reduced the survival after allo-HSCT. 4 Achieving deeper MRD clearance at earlier treatment before allo-HSCT is associated with superior long-term survival and lower relapse rates.5,6Blinatumomab—a bispecific antibody engaging CD3 on T cells and CD19 on leukemic B cells—induces cytotoxic T-cell effector activation by physically bridging these cell populations. 7 Growing clinical data have indicated that blinatumomab-facilitated bridging to allo-HSCT expands transplant eligibility and enhances durable survival.8–11 Furthermore, blinatumomab has also been shown to enhance overall survival even in MRD-negative B-ALL patients. 12 However, it is not clear whether short-course (2 weeks) blinatumomab as a bridge to allo-HSCT could reduce the relapse risk and improve survival for MRD-positive (MRD+) B-ALL patients.
Here, we present the single-center results of short-course blinatumomab for MRD+ B-ALL patients undergoing allogeneic peripheral blood stem cell transplantation (Allo-PBSCT). The results showed that the short-course blinatumomab could decrease the relapse risk and improve the relapse-free survival for MRD+ B-ALL patients.
Methods
Patients
Total 69 patients diagnosed with Ph-negative B-ALL undergoing allo-PBSCT in our center from November 2021 to June 2024 were enrolled into the retrospective single-center observational study. All patients received VDLP regimen for induction therapy. The dosage of anthracycline was adjusted based on patient’s age and ECOG. All patients who achieved CR after one cycle of induction then received two cycles of consolidation therapy, including at least one cycle of high-dose methotrexate. Among these patients, those who remained MRD-positive after consolidation were managed differently. Twenty-three patients MRD-positive prior to transplantation received a short course of blinatumomab to eradicate MRD (Blina group) and were hospitalized for the entire 14-day infusion period, with no toxicity-related admissions during or after the course. Concurrently, the other 46 patients, who were also MRD-positive after consolidation, continued conventional chemotherapy for one to two cycles with VDCP (vincristine, daunorubicin, cyclophosphamide, prednisone) and CAM (cyclophosphamide, cytosine arabinoside, 6-mercaptopurine) regimens in sequence, and achieved MRD-negative status before transplantation (Control group). The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee of Shanghai General Hospital (Ethical approval number: 2025009). Written informed consent was obtained from all participants or their authorized guardians.
Treatment selection and financial considerations
During the study period (November 2021 – June 2024), blinatumomab was not covered by China’s National Reimbursement Drug List. The 14-day short-course blinatumomab regimen cost approximately $ 1595–2215 per patient with no insurance reimbursement, while conventional chemotherapy was covered by basic medical insurance (70-90% reimbursement), with estimated out-of-pocket costs of $ 295–1329 per patient. Financial constraints were the primary reason the 46 control group patients continued with conventional chemotherapy rather than receiving blinatumomab. Patients in the blinatumomab group had financial support enabling them to afford the drug.
MRD eradication with short-course blinatumomab
The short course was defined as 14-day blinatumomab treatment as compared with routine 28-day course.13,14 Blinatumomab was administered with 24-h continuous intravenous infusion (9 μg/day on days 1-2 and 28 μg/day on days 3–14). Pretreatment with corticosteroids was mandatory to prevent neurological events and cytokine release syndrome (CRS). After one week of finishing the blinatumomab with MRD eradication, the transplantation course was initiated.
Transplantation procedures
Donors were from haploidentical, matched sibling and unrelated donors based on high-resolution HLA typing. 15 Reduced intensity conditioning (RIC) was used for patients with age ≥55 years or hematopoietic stem cell transplantation-comorbidity index (HCT-CI) > 2, which was based on busulfan (3.2 mg/m2/d for 2 days) and fludarabine (30 mg/m2/d for 5 days),16,17 while myeloablative conditioning (MAC) was prescribed to patients with age < 55 years or HCT-CI ≤2, which was based on busulfan (3.2 mg/m2/d for 4 days) or total body irradiation (TBI 10 Gy). 18 Graft-versus-host disease (GVHD) prophylaxis regimens included low-dose anti-thymocyte globulin (ATG)/post-transplant cyclophosphamide (PTCy)-based for haplo- and unrelated donor transplantation, and cyclosporine A-based for HLA matched sibling donor transplantation.19–21 All patients received granulocyte-stimulating colony factor (G-CSF) mobilized peripheral blood stem cells (PBSCs) as grafts.
Supportive care
G-CSF was given from day +5 until neutrophil recovery. Chimerism was assessed by short tandem repeat (STR) PCR analysis on bone marrow (BM) CD3+ T cells. Full donor chimerism was defined as ≥ 95% donor-derived T cells in BM samples. 22 Quantitative PCR assays for cytomegalovirus (CMV)-DNA and Epstein-Barr Virus (EBV)-DNA levels in peripheral blood were monitored weekly or biweekly until day +100 or beyond. Viral reactivation was defined as two consecutive detections of viral DNA exceeding 1000 copies/mL.23,24 Letermovir was prescribed to prevent CMV re-activation from day +1 to 3 months post-transplant. Acyclovir was administered from the time of engraftment until 1-year post-transplant. Additionally, posaconazole (300 mg orally daily) was started on the first day of conditioning regimen and continued for at least 3 months after transplantation.
Definitions
Remission was subclassified depending on peripheral blood count recovery into CR with full hematologic recovery (CR: Bone marrow blasts < 5%; absence of circulating blasts; absence of extramedullary disease; Absolute neutrophil count (ANC) ≥ 1.0 × 109/L; platelet count ≥ 100 × 109/L). MRD evaluation was performed with multiparameter flow-cytometry (MFC) and MRD negativity was defined as < 0.01% (<10−4) of leukemia-associated immunophenotype (LAIP) cells in bone marrow samples. Relapse was defined by the reappearance of over 5% blasts in the bone marrow or by the presence of extramedullary disease post‐CR, including central nervous system (CNS) involvement. Neutrophil engraftment was achieved when the absolute neutrophil count (ANC) reached ≥ 0.5 × 109/L for 3 consecutive days post-transplantation without G-CSF support. Platelet engraftment was defined as the first of 7 consecutive days with platelet count > 20 × 109/L in the absence of platelet transfusion. Acute GVHD (aGVHD) was diagnosed and graded according to the modified Glucksberg criteria. 25 Chronic GVHD (cGVHD) was assessed and classified as mild, moderate, or severe based on the 2014 National Institutes of Health (NIH) consensus criteria. 26
Statistical analysis
OS was defined as the time from the date of HSCT to death from any cause or the last follow-up. RFS was defined as the time interval from HSCT until the first occurrence of relapse or death from any cause. GVHD-free and relapse-free survival (GRFS) was calculated as a composite endpoint that without grade III-IV aGVHD, cGVHD requiring systemic immunosuppressive treatment, relapse, or death from any cause. To better evaluate the effect of post-transplant remission, the 18-month rates of OS, RFS, and GRFS were analyzed concurrently. Cumulative incidence of relapse (CIR) and non-relapse mortality (NRM) were measured from the date of transplant, with CIR defined by relapse and NRM by death from any cause other than relapse. 27 Cumulative incidence of aGVHD and cGVHD was calculated at 180 day and 18 months post-transplantation, respectively. Data are presented as descriptive values, including percentages, medians, and ranges, as appropriate. Nonparametric tests were performed for comparisons among groups (χ 2 and Fisher exact tests for categorical variables and Mann-Whitney and Kruskal-Wallis tests for continuous variables). OS, RFS, and GRFS, with 95% confidence intervals, were estimated using the Kaplan-Meier product limit estimator and compared using the log-rank test. The cumulative incidence method was applied to analyze aGVHD and cGVHD, NRM, and CIR. Multivariate analysis was performed using Cox proportional hazards models for variables with p value < 0.15 in univariate analysis. All Statistical analyses were conducted using R software (version 4.5.1). All tests were two-sided, with a P value <0.05 considered statistically significant.
Results
Patients characteristics
Clinical characteristics of patients.
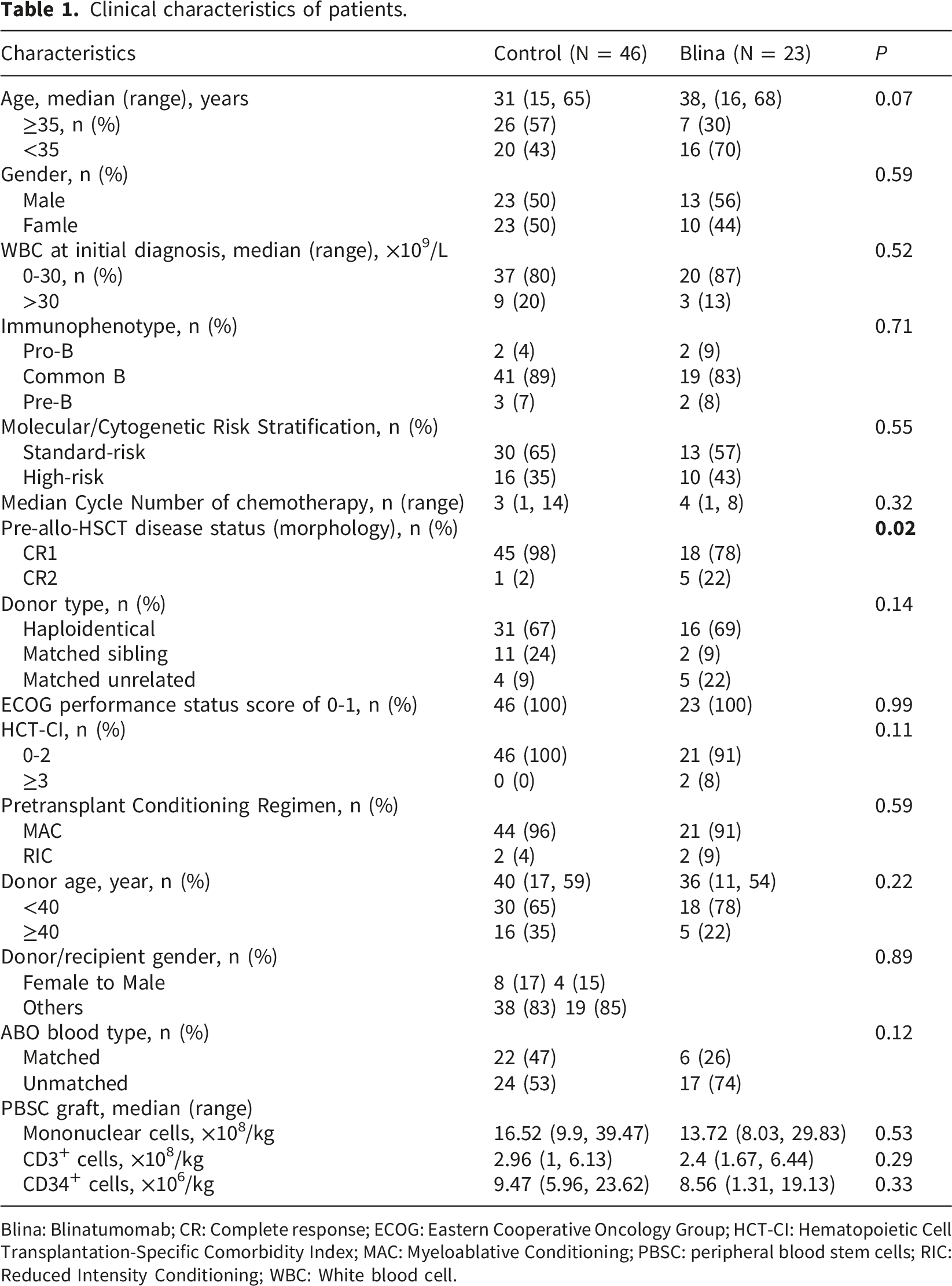
Blina: Blinatumomab; CR: Complete response; ECOG: Eastern Cooperative Oncology Group; HCT-CI: Hematopoietic Cell Transplantation-Specific Comorbidity Index; MAC: Myeloablative Conditioning; PBSC: peripheral blood stem cells; RIC: Reduced Intensity Conditioning; WBC: White blood cell.
MRD response and treatment-related toxicity of short-course blinatumomab
All 23 patients achieved MRD negativity after short-course blinatumomab. The most common associated toxicities were pyrexia (occurring in 20 cases, 77%). Only two patients developed grade 2 cytokine release syndrome (CRS; fever with hypotension), which resolved rapidly following tocilizumab intervention. No grade 3 or more CRS, neurologic toxicity, pneumonia, or sepsis was observed.
Engraftment
All patients achieved full-donor chimerism by day 28 post-transplantation, with a median donor chimerism level of 98.59% (range, 96.25%–100%). The time to neutrophil engraftment and platelet engraftment did not differ significantly between the blinatumomab and control groups. The median time to neutrophil engraftment was 12 days (range, 10–20) and 13 days (range, 9–17) in the blinatumomab and control groups (p = 0.173), and to platelet engraftment was 13 days (range, 11 – 30) and 14 days (range, 10 – 28) (p = 0.321), respectively.
Graft-verus-host disease
The 180-day cumulative incidence (CI) of grade II-IV aGVHD in the entire cohort was 8.7% (95% CI, 3.5%-16.8%). Bridging therapy with short-course blinatumomab had no impact on the incidence of grade II-IV aGVHD (8.5% vs. 9.0%; p = 0.93) (Figure 1(a)). The 18-month CI of cGVHD in the overall cohort was 34.3% (95% CI, 20.5%-48.6%). However, the short-course blinatumomab significantly reduced the overall incidence of cGVHD (14.8% vs. 41.8%; p = 0.05) (Figure 1(b)). This benefit was specifically observed for mild cGVHD (8.3% vs. 38.7%; p = 0.04, Supplementary Fig. A). In contrast, no significant difference was observed in moderate-to-severe cGVHD (7.1% vs. 4.7%; p = 0.85, Supplementary Fig. B). Cumulative incidence of grade Ⅱ-Ⅳ acute graft-versus-host disease (GVHD), chronic GVHD (cGVHD), non-relapse mortality (NRM), and cumulative incidence of relapse (CIR). (a) The cumulative incidence of grade Ⅱ-Ⅳ acute GVHD (aGVHD); (b) cGVHD; (c) NRM; (d) CIR.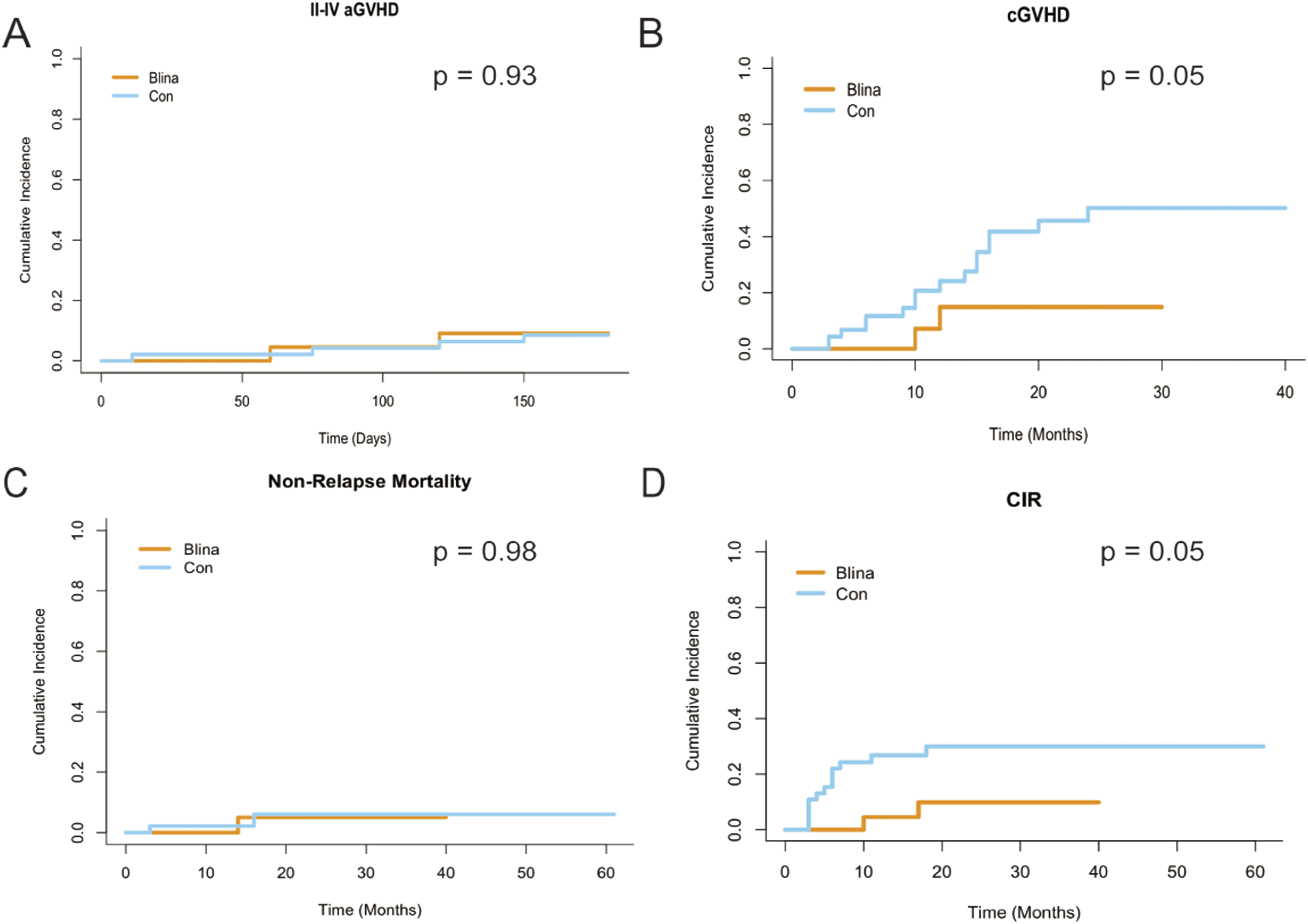
Non-relapse mortality, relapse, and infection
Causes of non-relapse mortality and viral infection.
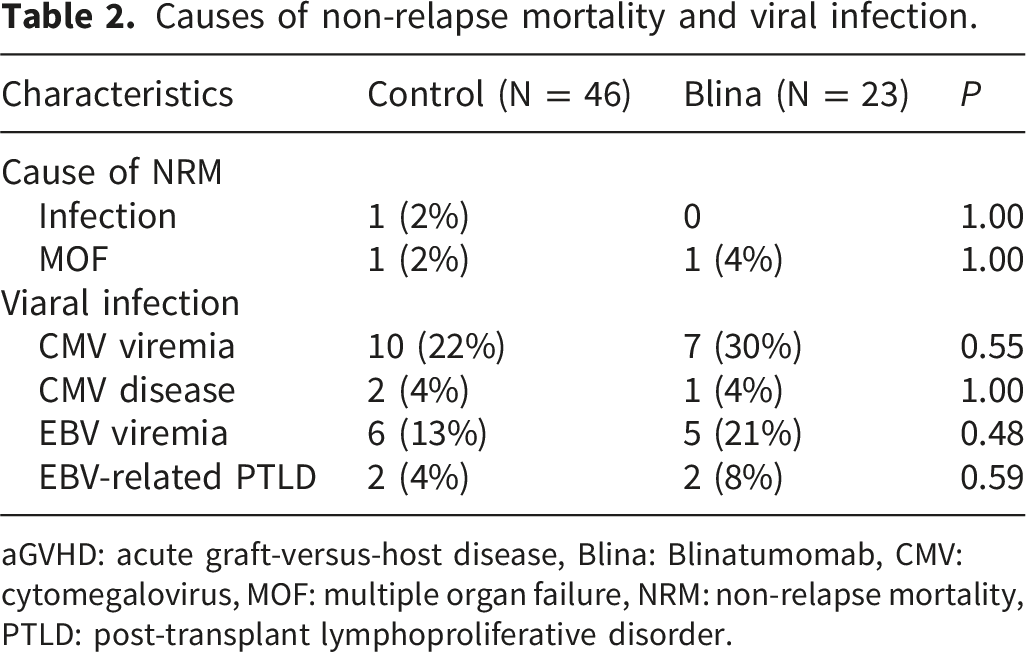
aGVHD: acute graft-versus-host disease, Blina: Blinatumomab, CMV: cytomegalovirus, MOF: multiple organ failure, NRM: non-relapse mortality, PTLD: post-transplant lymphoproliferative disorder.
Survival analysis
In the entire cohort, the median OS (Figure 2(a)) and RFS (Figure 2(b)) were not reached, while the median GRFS was 15 months (Figure 2(c)). Landmark analysis at 18 months revealed that although the difference was not statistically significant, the short-course blinatumomab cohort showed a trend toward improved OS (95.65% vs. 81.92%; HR = 0.21, 95% CI: 0.03-1.71; p= 0.15) (Figure 2(d)). A significant improvement in 18-month RFS rates was observed (90.87% vs. 65.19%; HR = 0.30, 95 % CI 0.09-1.04; p= 0.04) (Figure 2(e)). The 18-month GRFS rate was also numerical higher in the blinatumomab cohort (74.71% vs. 63.71%; HR 0.64, 95% CI 0.23-1.78; p = 0.38), but this difference did not reach statistical significance (Figure 2(f)). Survival outcomes. (a–c) For all patients. (a) Overall survival (OS); (b) Relapse-free survival (RFS); (c) GVHD-free, relapse-free survival (GRFS). (d)–(f) For patients in different groups. (d) OS; (e) RFS; (f) GRFS.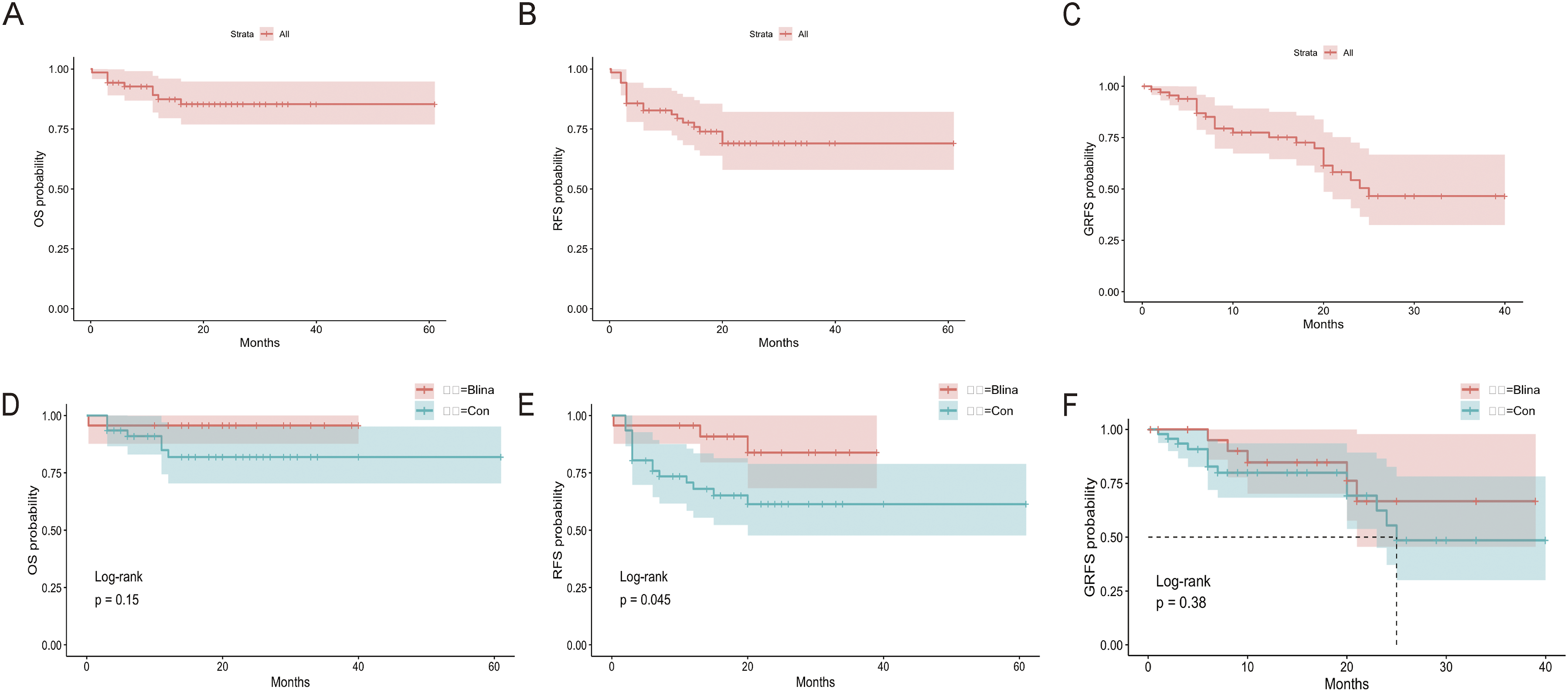
OS was adversely affected by high-risk molecular/cytogenetic status, which remained a significant independent poor prognostic factor in the multivariate analysis (Figure 3(a)). Concerning RFS, the high-risk status predicted worse outcomes, whereas pre-transplant short-course blinatumomab therapy was identified as a favorable prognostic factor in univariate analysis. Both factors retained independent significance in multivariate analysis (Figure 3(b)). Similarly, high-risk molecular/cytogenetic status was associated with a higher CIR and remained an independent prognostic factor in the multivariate model (Figure 3(c)). Upon evaluating prognostic interactions, standard-risk Ph-negative B-ALL patients exhibited particularly favorable outcomes, especially those who received short-course blinatumomab prior to HSCT. Univariate and multivariate analysis for Overall survival (OS), relapse-free survival (RFS) and cumulative incidence of relapse (CIR). (a) OS; (b) RFS, and (c) CIR.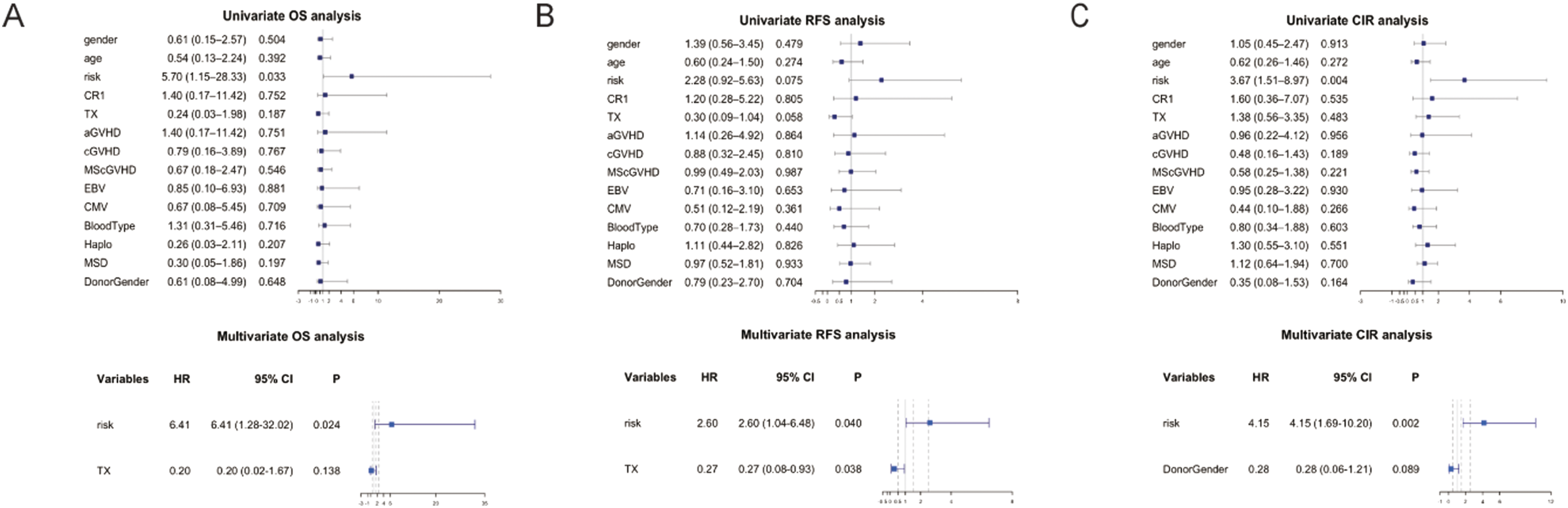
Discussion
In the present study, the results showed that the short-course blinatumomab for MRD eradication could significantly reduce the CIR post-transplant and improve the survival, especially RFS for Ph- B-ALL. The short-course blinatumomab didn’t have impact on acute GVHD, while significantly lowered the CI of total cGVHD. It also did not increase the infection risk and NRM. This approach thus represents a favorable clinical intervention to improve the efficacy of allo-HSCT for B-ALL patients.
The study rationale incorporated multiple elements. First, in relapsed/refractory ALL (R/R ALL), blinatumomab demonstrated greater efficacy during the first salvage attempt compared to subsequent ones. 7 Additionally, MRD positivity was associated with a substantially elevated risk of relapse and death.4,28,29 Most patients achieved MRD negativity after blinatumomab treatment and experienced improved survival relative to historical data.12,30 Our findings demonstrated that short-course blinatumomab achieved a 100 % MRD clearance rate, positioning it as a highly effective bridging strategy for achieving this critical state. Moreover, despite achieving MRD negativity before allo-HSCT in the conventional chemotherapy group, the short-course blinatumomab cohort still demonstrated superior long-term survival. This may be attributable to blinatumomab inducing deeper molecular remission beyond conventional detection thresholds, which warrants further investigation using next-generation sequencing (NGS-MRD).
Building upon existing evidence, a full-course blinatumomab regimen bridging to HSCT for Ph-negative B-ALL demonstrated significant long-term survival benefits in a Phase III trial (NCT02013167), 31 where 405 R/R B-ALL patients achieved 100 % 12-month OS. Real-world data from 106 patients further confirmed blinatumomab’s efficacy and safety profile, with 2-year PFS and OS rates of 48% and 58%, respectively. 32 Considering the potent anti-leukemia effect of blinatumomab in B-ALL, integrating it into pre-transplant bridging therapy shows clinical promise. 9 Despite its efficacy, blinatumomab’s short half-life necessitates 24-hour continuous infusion (typically 4-week cycles with 2-week intervals), and its prohibitive cost limits broad clinical adoption. This has prompted the exploration of abbreviated, or short-course, blinatumomab protocols. Using a 14-day course of blinatumomab could facilitate rapid bridging to transplantation, and shortening the duration may improve tolerability and reduce financial burden while preserving efficacy, as suggested by emerging literature. 13 In line with this rationale, no severe adverse events were observed in the present study, which may be potentially attributable to the shortened treatment duration and prophylactic use of dexamethasone.
Previous studies on short-course blinatumomab before HSCT have shown variable outcomes. A retrospective single-center study reported that 82.62% 2-year OS and 78.35% 2-year PFS were achieved with the short-course blinatumomab bridging to HSCT among adult R/R B-ALL patients, 13 while pediatric R/R cases (n = 33) showed enhanced tolerability but no short-term survival gains. 33 In the present study, we evaluated short-course blinatumomab in non-R/R B-ALL patients and observed compelling outcomes even in a group with a higher prevalence of adverse cytogenetic and molecular features. Following blinatumomab bridging, all achieved MRD negativity with significantly reduced relapse rates, with 18-month OS of 95.65% and 18-month RFS of 90.87% (p = 0.05), the latter demonstrating a statistically significant difference versus controls. A borderline significant trend towards superior OS (p = 0.15) may reflect limited sample size and follow-up duration, which may attain statistical significance with extended follow-up and larger patient cohorts. The superior outcomes (the longer RFS, lower relapse, lower incidence rate of cGVHD) were achieved despite the higher baseline risk profile of the blinatumomab group.
Multiple observations support the potential of abbreviated blinatumomab regimens. First, pharmacodynamically, blinatumomab achieves steady-state T-cell activation within days, 9 and in patients with low tumor burden (MRD-positive but in morphologic CR), as shown by the 100% MRD negativity rate in our cohort. Second, published studies using abbreviated (14-day) blinatumomab have reported post-transplant outcomes comparable to historical 28-day data.13,33 Third, our 18-month RFS of 90.9% is numerically similar to that reported in trials employing full-course blinatumomab. Nonetheless, we acknowledge that lack of a direct 28-day comparator is a major limitation, and prospective randomized trials are urgently needed to establish non-inferiority of the short-course regimen. Short-course blinatumomab demonstrated improved survival without increasing risk of infection versus standard extended regimens in Ph-negative ALL. Collectively, short-course blinatumomab represents a viable, well-tolerated, and cost-effective bridging strategy that significantly reduces relapse and improves survival outcomes in Ph-negative B-ALL patients.
In our study, short-course blinatumomab significantly reduced the incidence of cGVHD (p = 0.05). Substantial preclinical evidence indicates that blinatumomab ameliorates cGVHD through: (1) B-cell depletion-mediated reduction of BAFF levels; (2) inhibition of Th17/TFH cell differentiation; and (3) promotion of Treg expansion and functional enhancement—collectively suppressing autoantibody production and decreasing profibrotic cytokines IL-17.34,35 Our findings provide clinical validation for these mechanisms. In contrast, aGVHD pathogenesis primarily involves CD8+ T cells and Th1 cells mediating tissue necrosis via massive inflammatory cytokine release. 36 These molecular mechanisms potentially underlie blinatumomab’s significant reduction in cGVHD incidence, for which our study provides empirical support. Further investigation into blinatumomab’s precise mechanisms in GVHD modulation remains warranted. Although our study did not include a full-course blinatumomab cohort, published data indicate that patients who received ≥ two cycles of blinatumomab had a trend towards increased cumulative incidence of cGVHD versus single-cycle recipients. 9
Conclusion
This single-center retrospective observational study confirms the feasibility of short-course blinatumomab bridging to HSCT in patients with Ph-negative B-ALL, achieving not only MRD negativity but also demonstrating potential for long-term survival with reduced treatment-related toxicities. Although our study presented limitations, including the limited sample size, relatively short follow-up duration, and absence of a full-course blinatumomab comparator group, these results provide a foundation for future prospective investigations.
Supplemental material
Supplemental material -Short-course blinatumomab as a bridge-to-transplantation improves the survival of Ph-negative MRD-positive B-ALL
Supplemental material for Short-course blinatumomab as a bridge-to-transplantation improves the survival of Ph-negative MRD-positive B-ALL by Xia Shao, Miao Zhang, Huiying Qiu, Jun Yang, Xinxin Xia, Yu Cai, Yin Tong, Chongmei Huang, Baoxia Dong, Kun Zhou, Liping Wan, Yuhu Feng, and Xianmin Song in Cell Transplantation.
Footnotes
Acknowledgements
This study was conducted at the Department of Hematology, Shanghai General Hospital, Shanghai Jiaotong University School of Medicine. The authors sincerely thank all the staff and participants for their important contributions.
Ethical considerations
This study was approved by the Ethics Committee of Shanghai General Hospital on January 23, 2025 (Ethical approval number: 2025009).
Consent to participate
Written informed consent was obtained from all participants or their authorized guardians.
Author contributions
This study was conceived and designed by Song X and Feng Y; Shao X and Zhang M was responsible for data acquisition, analysis, and interpretation, and drafted the manuscript; Qiu H, Yang J and Xia X acquired data and played an important role in interpreting the results; Cai Y, Tong Y, Huang C, Dong B, Zhou K and Wan L took care of patients in clinical practice. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82270226 for Xianmin Song); the three-year development project from Shanghai Shen Kang Hospital Development Center (SHDC2020CR1012B for Xianmin Song).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.