
Abstract
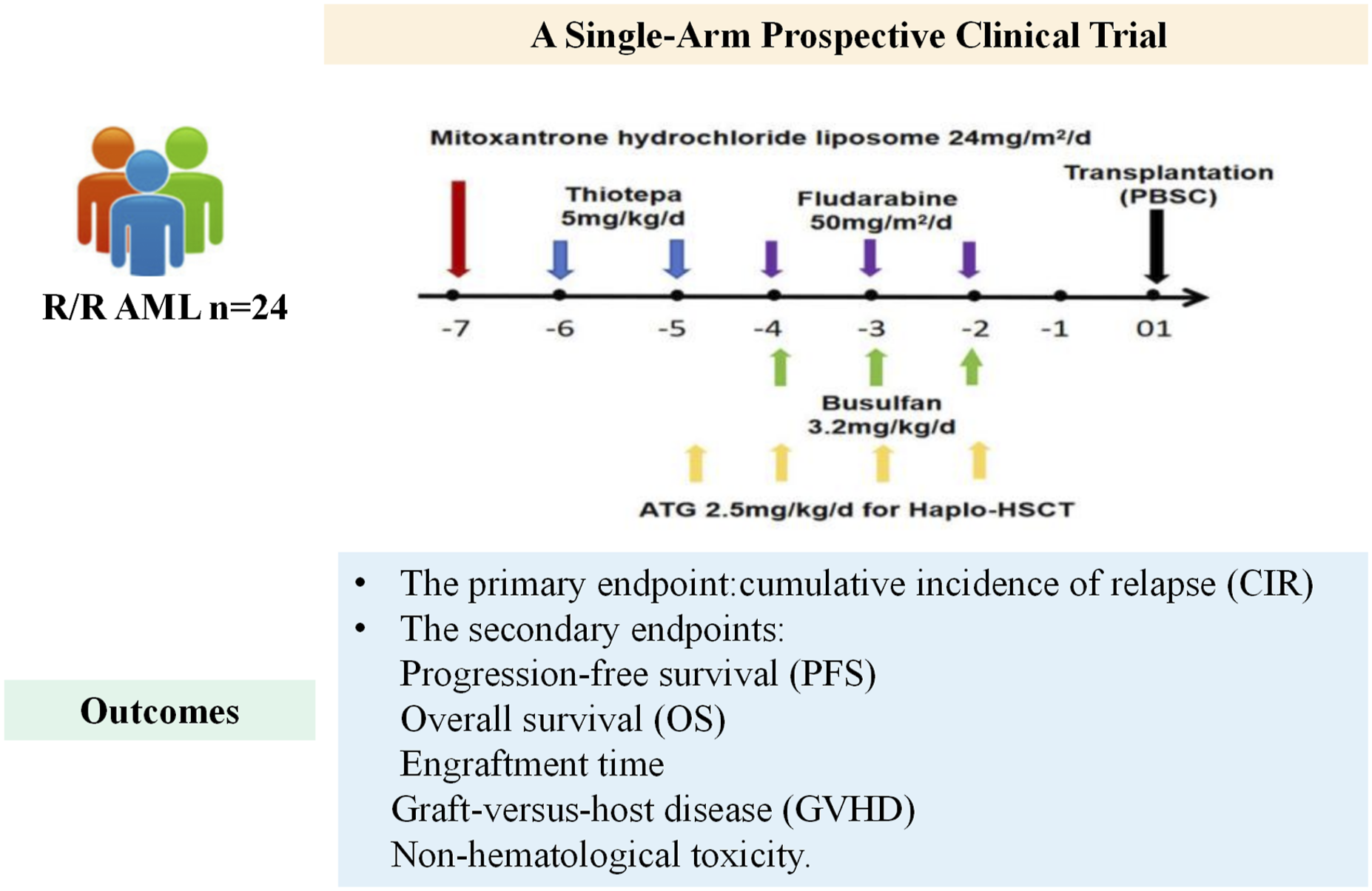
To investigate the efficacy and safety of MTBF as conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation (allo-HSCT) in patients with relapsed or refractory acute myeloid leukemia (R/R AML). We conducted a single-arm prospective clinical trial (NCT06385808). The main outcome was cumulative incidence of relapse (CIR), and the secondary outcomes were progression-free survival (PFS), overall survival (OS), engraftment time, graft-versus-host disease (GVHD), and non-hematological adverse effects. Twenty-four R/R AML patients from the First Affiliated Hospital of Xi’an Jiaotong University were enrolled, and all achieved engraftment. Mucositis was the predominant toxicity and was managed appropriately. The two-year CIR was 10%. The two-year OS and PFS were 78.9 ± 11.1% and 51.2 ± 19.3%, respectively. Two patients experienced relapse, and three patients died of infection. Subgroup analyses demonstrated that maintenance treatment post-transplantation may improve OS. The MTBF regimen for salvage allo-HSCT in R/R AML exhibited notable anti-leukemia activity and tolerable toxicity. (NCT06385808, Efficacy and Safety of MTBF Conditioning Regimen for Salvageable Allo-HSCT in the Treatment of R/R AML).
Keywords
Introduction
Due to the poor prognosis of patients with relapsed/refractory acute myeloid leukemia (R/R AML) and allogeneic hematopoietic stem cell transplantation (allo-HSCT) may be one available curative approach, current clinical guidelines suggest that prompt transplantation should be carried out in such cases, instead of continuing with further chemotherapy. 1
The conditioning regimen was very important for these patients with R/R AML. An ideal conditioning regimen needs to have the strongest leukemia-fighting capability and the least toxic effects. TBF regimen composed of thiotepa, busulfan, and fludarabine has shown notable leukemia-fighting effectiveness in haploidentical, 2 matched sibling and unrelated-donor stem cell transplantation. This therapeutic approach delivers outcomes were comparable with other alternative protocols employed in relapsed or refractory AML, including FT and FLAMSA. The two-year overall survival (OS) rates were 37% for FT, 24% for TBF, and 34% for FLAMSA (p = 0.10). 3 Mitoxantrone hydrochloride liposome, being a PEGylated liposomal form of the mitoxantrone, exhibits favorable therapeutic effects and a manageable safety profile in treatment of AML. It was reported that mitoxantrone hydrochloride liposome may enhance responsiveness to gilteritinib in AML patients with FLT3-ITD mutations. 4 In high-risk pediatric AML, when patients underwent chemotherapy with mitoxantrone hydrochloride liposome, they attained remission levels comparable to those on conventional idarubicin-based treatment, while showing quicker restoration of blood cell counts and improved safety outcomes. 5 To enhance the anti-leukemia efficacy, a novel mitoxantrone hydrochloride liposome/thiotepa/busulfan/fludarabine ((MTBF) regimen was formulated. In this study, the outcomes of this single-arm, prospective clinical trial were reported, investigating the efficacy and safety of the MTBF conditioning regimen for allo-HSCT in patients with R/R AML.
Subjects and methods
Patients
This was a single-arm, prospective clinical trial (NCT06385808). Patients in the First Affiliated Hospital of Xi’an Jiaotong University from June 1st 2024 who underwent allo-HSCT was enrolled. The primary inclusion criteria were patients with adult R/R AML, who met the indication for allo-HSCT. Refractory acute myeloid leukemia was defined as patients with bone marrow (BM) blast cells surpassing 5%, and/or with extramedullary disease, and/or with leukemic blast cells in peripheral blood (PB) after two cycles of standard induction therapy. Patients with ≥ 5% blast cells in BM, the recurrence of blasts in PB, or extramedullary disease subsequent to the prior achievement of complete remission (CR) or CR with incomplete recovery (CRi) were defined as relapsed disease. All patients provided written informed consent to participate the trial. Prior to initiating the relevant investigation, the research protocol obtained authorization from the ethics review committee of the First Affiliated Hospital of Xi’an Jiaotong University (No.XJTU1AF -CRF-2023-XK014)on December 14th, 2023. This research conformed to the Helsinki Declaration.
Transplantation protocol
The detailed regimen of MTBF was as follows: On day -7, an intravenous infusion of mitoxantrone hydrochloride liposome was given at a dose of 24 mg/m2; Thiotepa was administered intravenously at 5 mg/kg daily from day -6 to day -5; From day -4 to day -2, busulfan was intravenously infused at 0.8 mg/kg every 6 hours; During the same period (day -4 to day -2), fludarabine was also given via intravenous infusion at 50 mg/m2daily. For haploidentical transplantation or matched unrelated transplantation, rabbit anti-thymocyte globulin (rATG, Sanofi) was given with total dosage of 10mg/kg administered over four days (day -5∼day -2). A combination therapy consisting of cyclosporine A, methotrexate, and mycophenolate mofetil was applied for preventing graft-versus-host disease (GVHD), Those patients with FLT3-ITD mutation, were given tyrosine kinase inhibitors as part of their maintenance treatment. Additionally, all adjunctive care measures were administered in line with the institutional guidelines.
Virologic surveillance and preemptive treatment strategy for CMV and EBV infection
All participants initiated letermovir 240 mg daily for CMV prophylaxis within 28 days post-HSCT and continued for 100±7 days. .Plasma CMV and Epstein-Barr virus (EBV) DNA levels were measured weekly during the first 3 months post-HSCT, and then biweekly for the following 3 months, using real-time quantitative polymerase chain reaction (qPCR). CMV and EBV DNAemia were defined as viral DNA levels >200 copies/mL by qPCR in two consecutive peripheral blood tests post-HSCT, without clinical symptoms. CMV disease was diagnosed based on elevated CMV-DNA levels in tissue or fluid samples obtained from the affected organ detected by qPCR. When a patient was diagnosed with CMV infection, letermovir was discontinued and intravenous ganciclovir or foscarnet was initiated. When a patient was diagnosed with EBV infection, intravenous ganciclovir or anti-CD20 antibody was initiated.
Minimal residual disease detection
Minimal residual disease (MRD) was detected by multicolor flow cytometry (MFC), with a positivity threshold of ≥0.01%. If patients had fusion genes or gene mutations, gene quantifications were detected by PCR or next-generation sequencing.
Study outcomes and definitions
The main outcome was two-year cumulative incidence of relapse (CIR). Secondary outcome included the one and two-year progression-free survival (PFS), OS, the reconstitution of neutrophils and platelets, acute and chronic GVHD, and non-hematological toxicity.
OS is defined as the time from transplantation to death caused by any factor. PFS was characterized as the period of survival following transplantation in the absence of disease recurrence or advancement. The grade of acute GVHD were evaluated according to the MAGIC criteria, 6 while chronic GVHD was identified based on the criteria of NIH. 7 All adverse events were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE, version 5.0).
Statistical analysis
OS, PFS, and CIR were all evaluated via Kaplan-Meier survival analysis methods. For all these analytical procedures, a probability value below 0.05 was taken to indicate statistically significant distinctions. For these analyses, all statistical assessments were performed with R software (version 4.3.4; R Foundation, Vienna, Austria).
Results
Patient characteristics
A total of thirty-two patients were recruited and twenty-four patients were incorporated into the analysis, and a flow diagram was shown in Figure 1(A). All patients recieved MTBF conditioning regimen (Figure 1(B)). rATG was supplemented during haploidentical and matched unrelated donor transplantation. Flow chart of the trial and the protocol of the MTBF conditioning regimen. (A) Flow chart of the trial. (B) MTBF regimen: Mitoxantrone hydrochloride liposome at a dosage of 24 mg/m2 was administered via intravenous drip on day -7,Thiotepa at 5 mg/kg was given through intravenous drip from day -6 to -5,Busulfan at 0.8 mg/kg was intravenously infused every 6 hours from day -4 to -2, Fludarabine at 50 mg/m2 was intravenously dripped from day -4 to -2,rATG was supplemented during haploidentical and matched unrelated donor transplantation.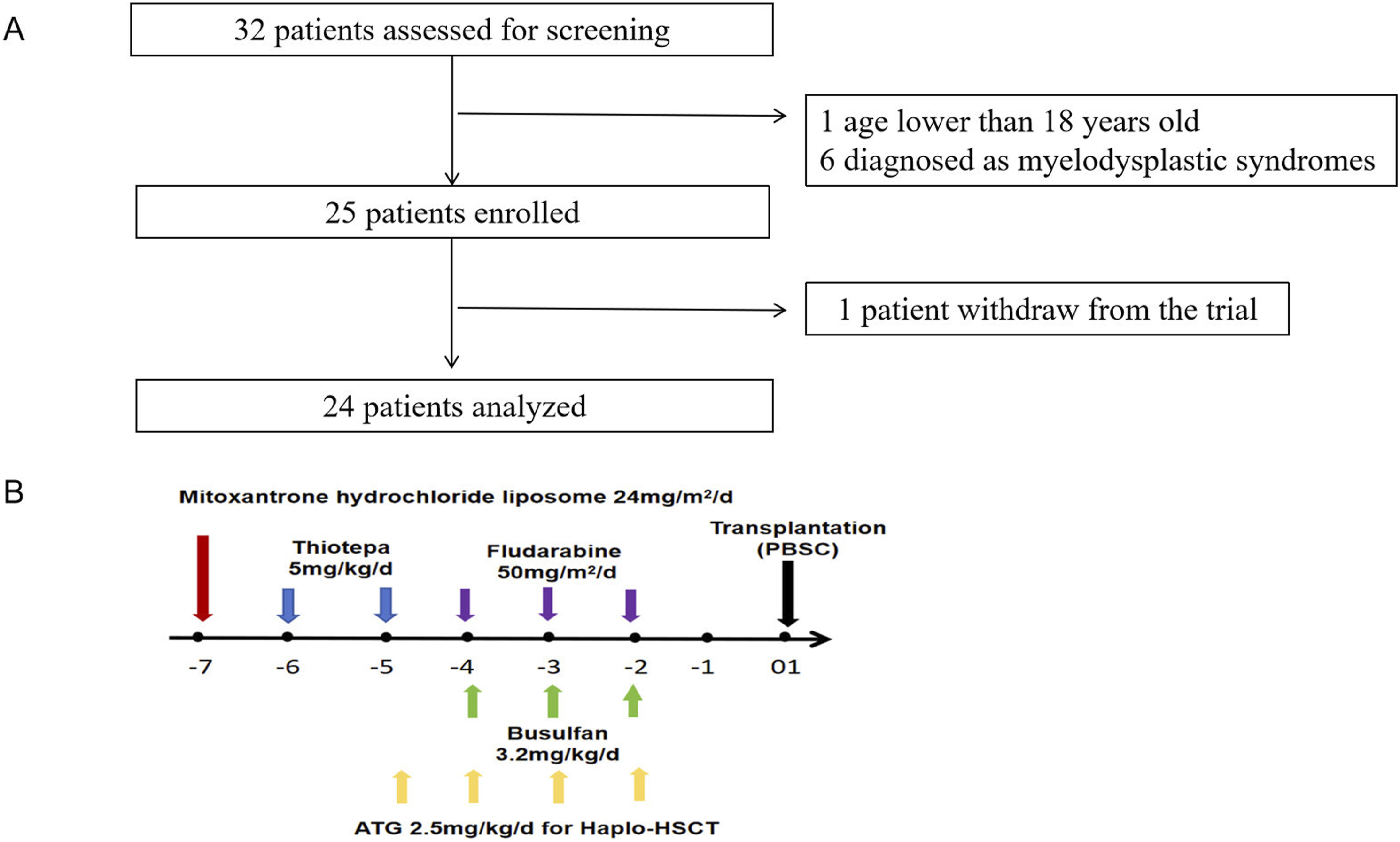
Basic characteristics of the enrolled patients.
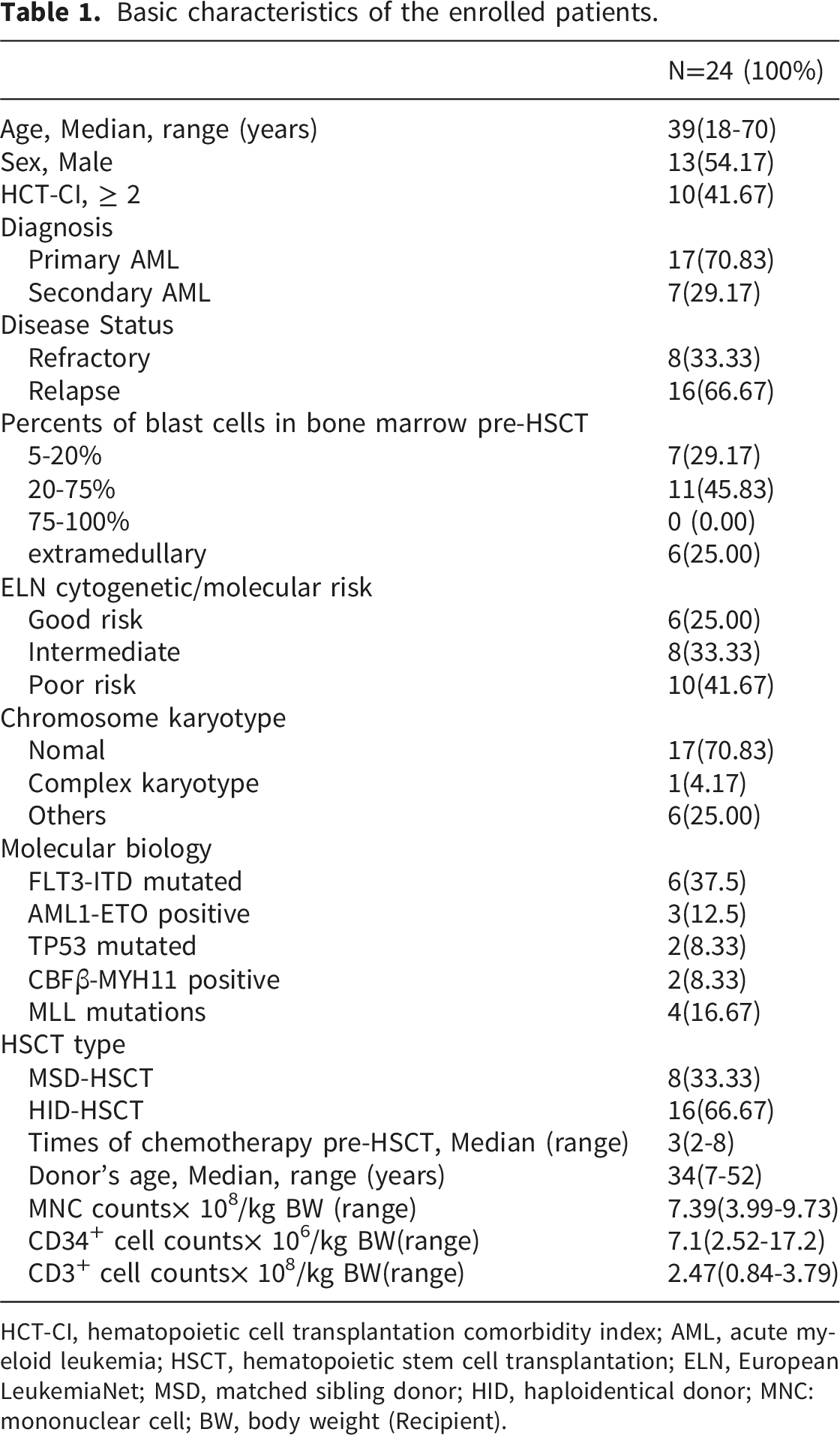
HCT-CI, hematopoietic cell transplantation comorbidity index; AML, acute myeloid leukemia; HSCT, hematopoietic stem cell transplantation; ELN, European LeukemiaNet; MSD, matched sibling donor; HID, haploidentical donor; MNC:mononuclear cell; BW, body weight (Recipient).
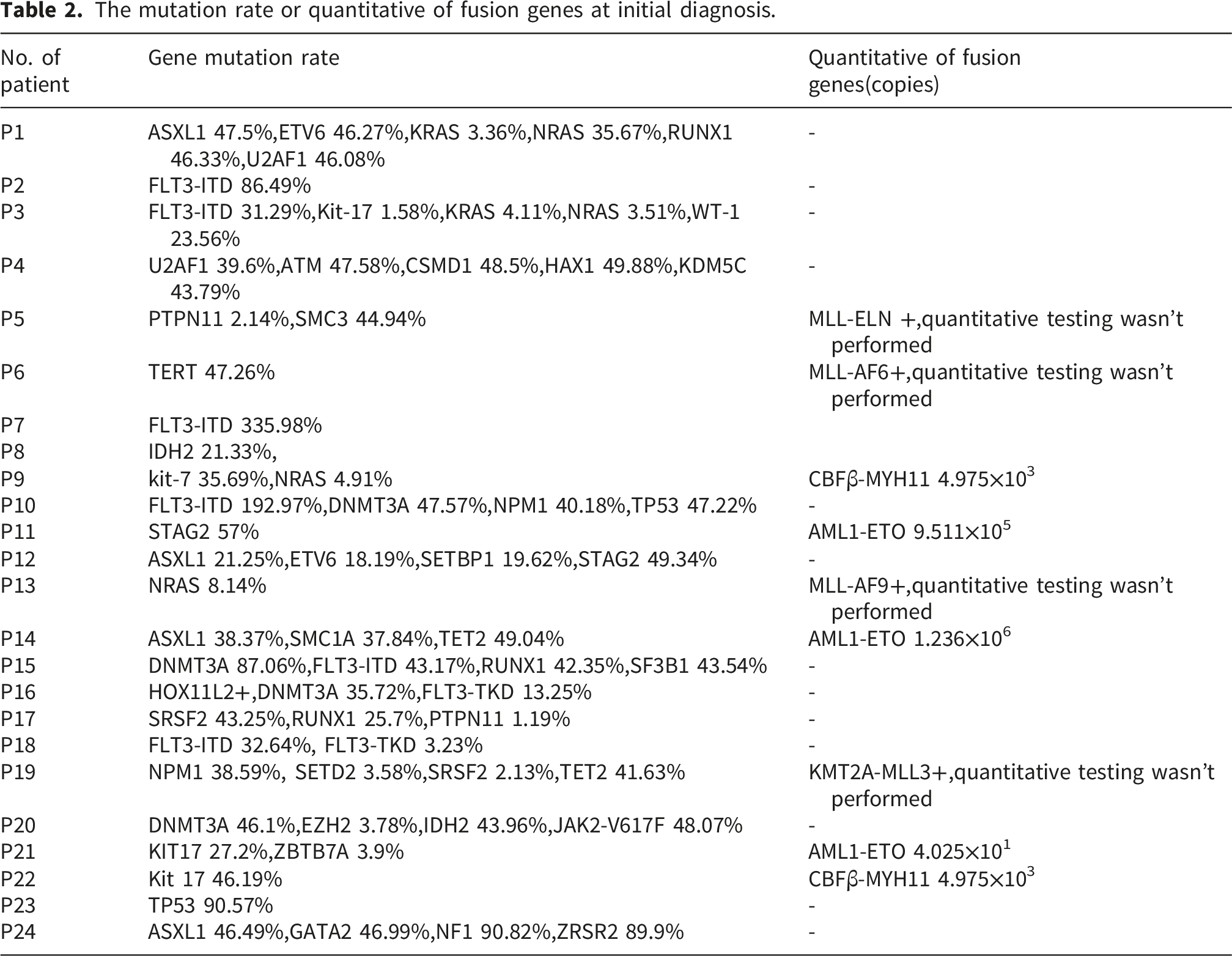
The mutation rate or quantitative of fusion genes at initial diagnosis.
Hematopoietic recovery and efficacy
All patients achieved hematopoietic recovery, and sustained complete donor chimerism was confirmed between days +21 and +28 after transplantation. For neutrophil reconstitution, the median time was 11 (9–13) days, whereas the median time for platelet reconstitution was 12 (9-23) days. At the time of reconstitution, every patient exhibited favorable responses, with 100% MRD-negative complete remission.
GVHD, infections, and regimen-Related toxicities
Within 100 days after transplantation, 9 patients experienced acute GVHD including 5 cases of grade II acute GVHD, 3 cases of grade III, and one of grade IV. Among them, two patients had skin acute GVHD, two had intestine acute GVHD and three had liver acute GVHD. Two patients were found to have involvement of multiple organs. The incidence of grade II–IV and III–IV acute GVHD were 37.50% and 16.67% respectively. The median onset time of acute GVHD was 39 days (range, 12-90 days). Ten patients developed chronic GVHD including five patients with mild to moderate skin chronic GVHD, four cases of liver chronic GVHD and one of lung chronic GVHD. The incidence of total chronic GVHD and severe chronic GVHD were 41.67% and 8.33% respectively. There was no significant difference of aGVHD between patients received matched sibling donor transplantation and haploidentical stem cell transplantation(P=0.11),but the incidence of cGVHD of patients received matched sibling donor transplantation was higher than that of patients received haploidentical stem cell transplantation(P=0.01).
The overall incidence of infection within one year post-transplantation was 29.17% (n = 7), with pulmonary infections being the most common type of infection at 25.00% (n = 6), followed by intestinal infections at 10.3% (n = 6). The overall incidence rate of CMV reactivation was 8.33% within 6 months post-transplantation, and the cumulative incidence rate of EBV reactivation was 8.33%. The occurrence rate of hemorrhagic cystitis was 16.67%.Among these cases, one was grade I, two were grade II, and one was grade III. The BK virus in urine was positive in all of patients with hemorrhagic cystitis. The onset time of hemorrhagic cystitis were from 16 to 34 days post-transplantation and all were alleviated after symptomatic treatment.
The non-hematologic toxicities included nausea (n = 16, 66.67%), diarrhea (n = 12, 50.00%), mucositis (n = 12, 50.00%), skin discoloration (n = 4, 16.67%), gastrointes tinal bleeding (n = 5, 20.83%), and elevated aspartate aminotransferase (n = 4, 17%). These complications were alleviated through symptomatic treatment. No deaths were caused by life-threatening organ damage arising from the conditioning treatment. Additionally, no cases of veno-occlusive disease or transplant-associated thrombotic microangiopathy were identified. The non-relapse mortality rate within 6 months was 8.33%.
Maintenance treatment post-HSCT
Overall, eight patients (33.33%) received maintenance therapy following allo-HSCT. Among these patients, the median time of initiation of maintenance treatment was 2.5 months (range: 2-3 months). FLT3 inhibitors was the primary maintenance therapy medication (66.67%). Furthermore, decitabine was used as monotherapy for maintenance treatment in only one patient, five patients were administered FLT3-ITD inhibitor as maintenance therapy medication, Moreover, intrathecal chemotherapy was administered to two cases to prevent central nervous system relapse.
Overall survival, progression-free survival, and cumulative incidence of relapse
At the end of follow-up, 21 patients were still living. Infection was the primary reason for mortality. One case had a mixed infection of Malassezia haematolytica, Klebsiella pneumoniae, Enterococcus faecium, Leptospira brucii, Aspergillus fumigatus, Candida tropicalis, and herpes simplex virus, occurring 15 days post-transplantation; another case presented with Pseudomonas aeruginosa infection at 1 year post-transplantation; and another case exhibited HHV-6 virus infection at 31 days post-transplantation.
Over a median follow-up duration of 15 months (range: 7 to 27 months), 1-year OS and PFS rates were 94.4 ± 5.4% (95% CI: 84.4-100) and 82.0 ± 13.2% (95% CI: 59.8-100), respectively. The 2-year OS and PFS were 78.9 ± 11.1% (95% confidence interval [CI]: 59.9-100) and 51.2 ± 19.3% (95% CI: 24.5-100), respectively. Two individuals had a recurrence of primary disease, with the time spans from allo-HSCT to recurrence being 11 months and 2 months, respectively. The 2-year cumulative incidence rate of relapse was 10% (95% CI: 0-27) (Figure 2). OS, PFS, and CIR of patients: A: Overall survival; B: Progression-free survival; C: Cumulative incidence of relapse.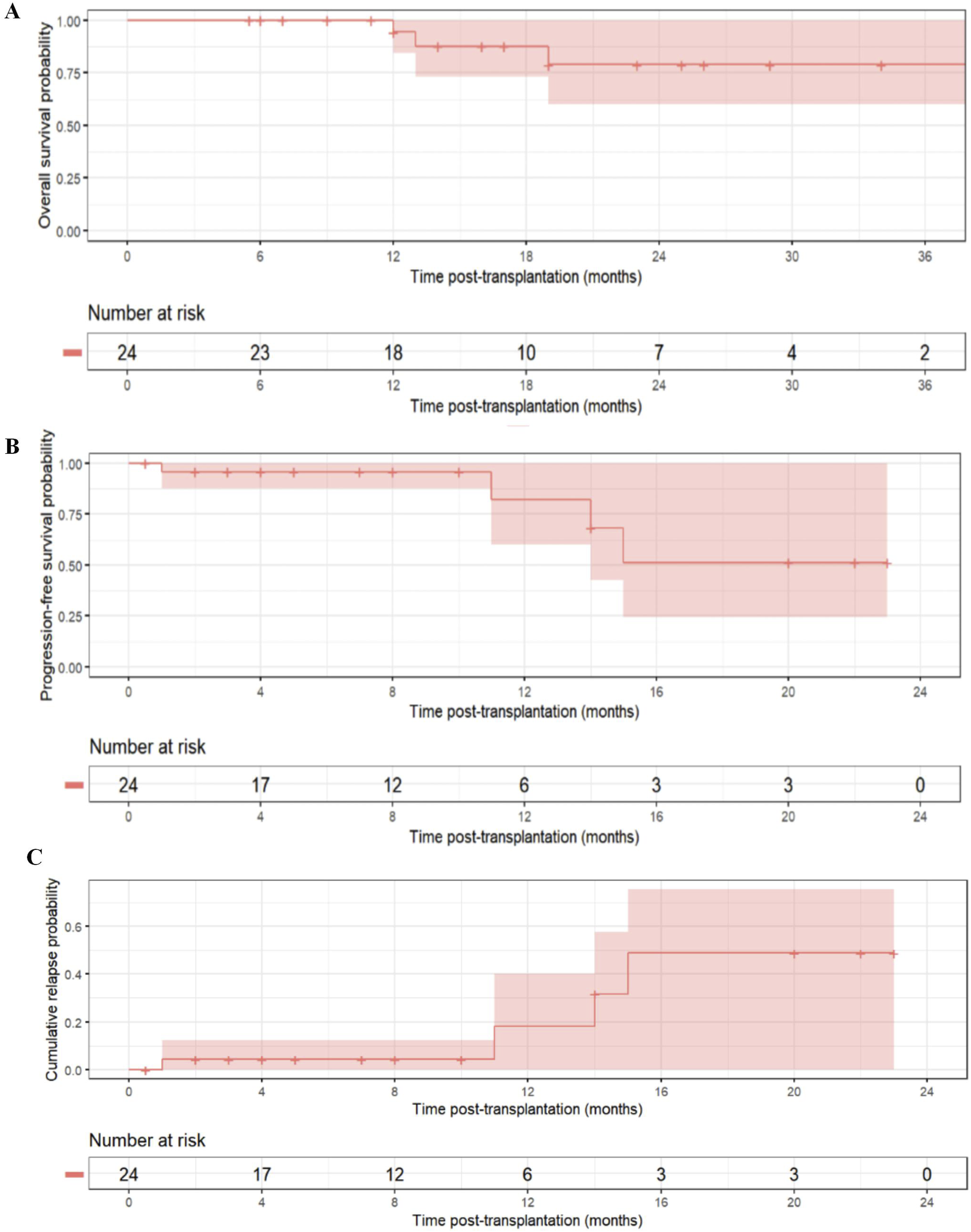
Subgroup analyses of overall survival
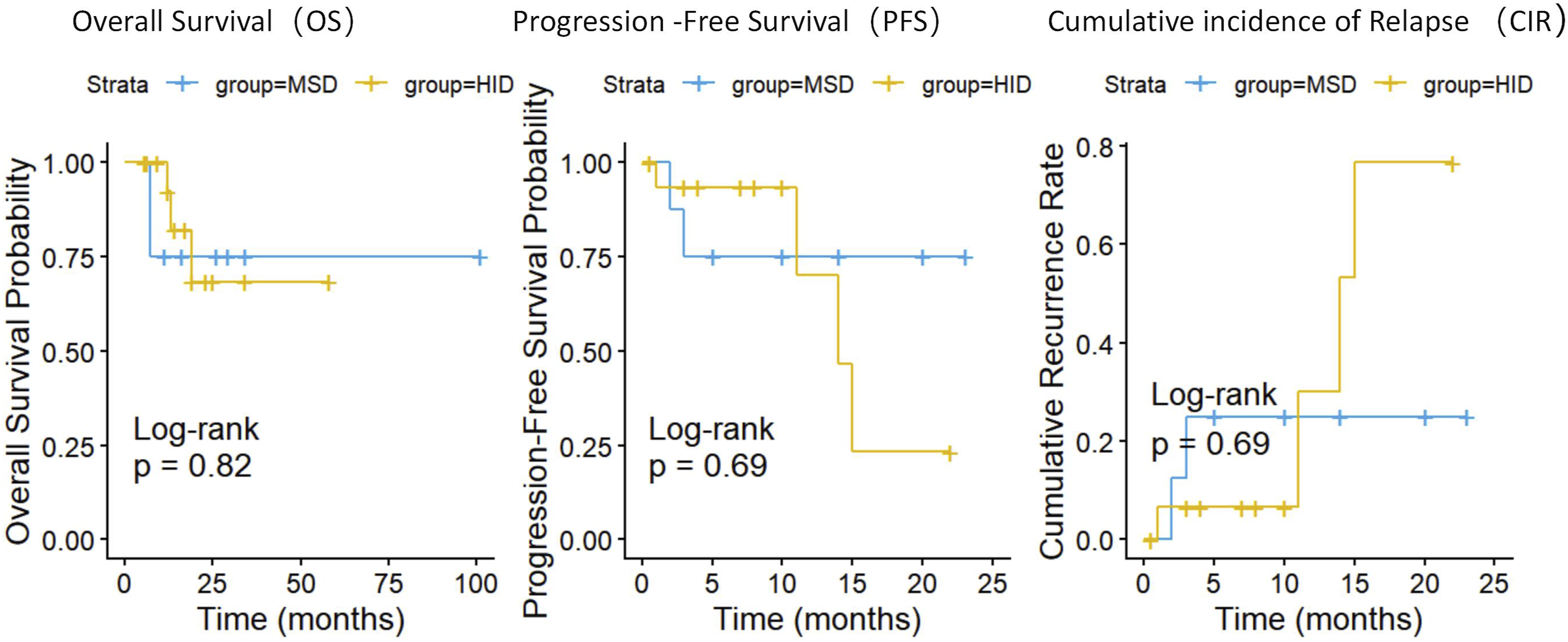
Studies have indicated that counts of blast cells before hematopoietic stem cell transplantation or risk classification can influence the outcomes of allo-HSCT. Consequently, an analysis of subgroups was based on the counts of bone marrow blast cells. The results indicated that percents of blast cells in bone marrow>20% before transplantation, active extramedullary disease, and risk stratification at diagnosis did not significantly influence the patients’ outcomes (Figure 3(A)–(C)). Within this subgroup analysis, the prompt implementation of maintenance therapy may lowered the risk of relapse after allo-HSCT (Figure 3(D)). For individuals undergoing maintenance treatment following allo-HSCT, the 2-year OS rate was 100%; in contrast, the 2-year OS rate was 50% among those without post-HSCT maintenance treatment. There were no significant differences of OS,PFS and CIR between patients received matched sibling donor transplantation and haploidentical stem cell transplantation(P=0.82,0.69,0.69) (Figure 4). OS of subgroup patients:A:percent of blast cells in bone marrow before transplantation; B:extramedullary disease; C:high risk at diagnosis; D:maintenance therapy post-HSCT. OS, PFS and CIR between patients received matched sibling donor transplantation and haploidentical stem cell transplantation.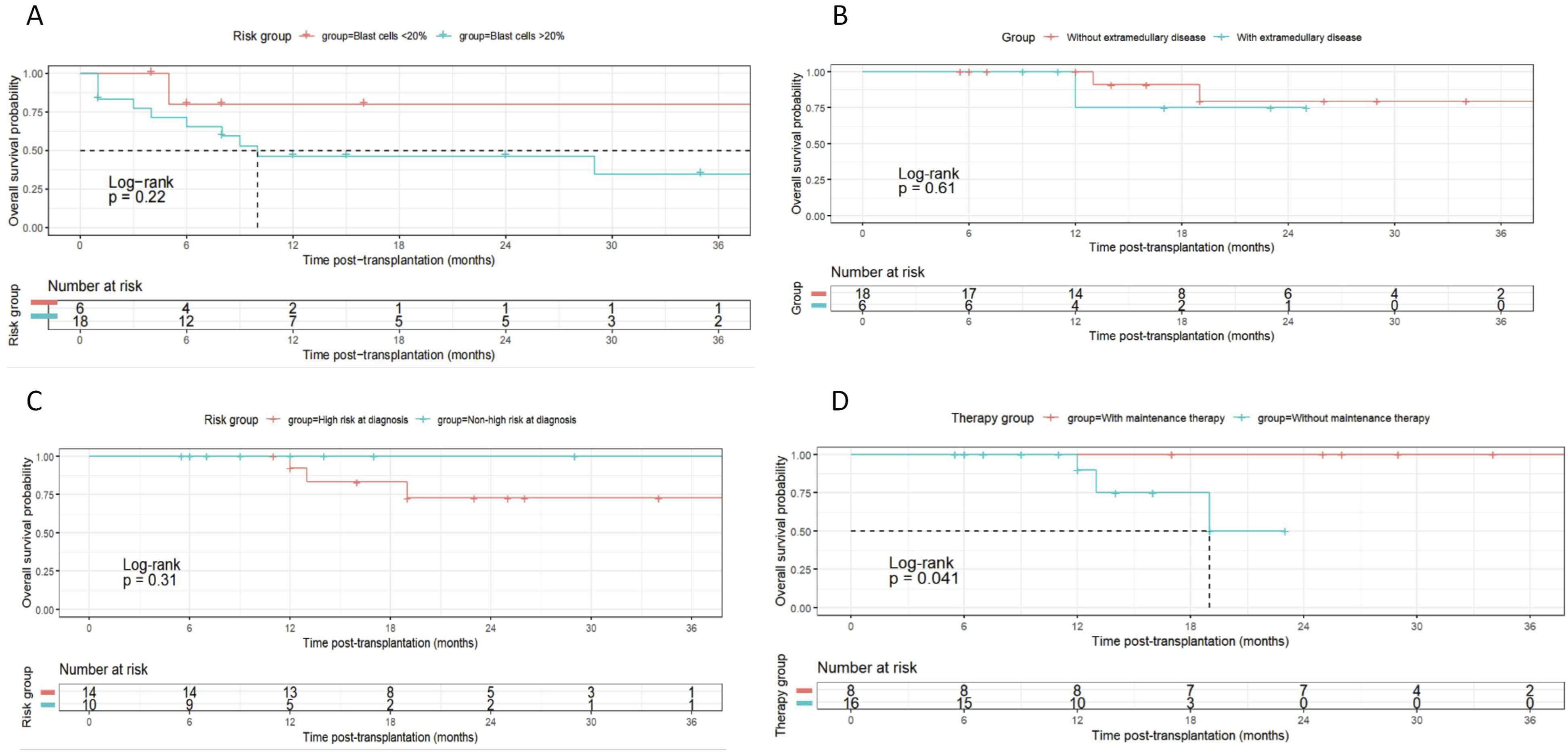
Discussion
Patients with R/R AML have unfavorable prognosis, allo-HSCT remains the only potential curative approach available at present. Concerning the optimal timing of allo-HSCT for R/R AML patients, the conventional perspective posits that transplantation should be carried out subsequent to attaining CR to optimize therapeutic efficacy and mitigate the risk of relapse. Nevertheless, for R/R AML patients, re-achieving CR through conventional chemotherapy proves to be extremely arduous. The waiting period for CR frequently results in further progression of the disease or deterioration of the patient’s physical condition, thereby causing the patient to miss the transplantation window. Over the past few years, there has been growing recognition that direct allo-HSCT represents a viable “salvage” strategy for selected patients whose disease is under control or who demonstrate a partial response to salvage chemotherapy, even in the absence of CR.8,9 The patients enrolled in this study are representative of this high-risk cohort. The successful practice in this study offers further corroboration for the concept of a “transplant window,” indicating that transplantation should be performed when the disease has not yet completely spiraled out of control and when the graft-versus-leukemia (GVL) effect can potentially exert maximal efficacy. The GVL effect may eliminate residual leukemic cells post-transplantation, even if CR was not achieved prior to the procedure. Consequently, for R/R AML patients, clinicians ought to avoid strictly requiring CR attainment and rather take a more active approach to evaluate patient condition and tumor load in order to determine the best time for transplant.
For patients with R/R AML, the selection of a conditioning protocol holds significant importance, as the ideal approach should balance robust leukemia-suppressing efficacy with reduced harmful effects on normal tissues.10–12 Conventional high-intensity conditioning regimens (e.g., based on busulfan or total body irradiation) are limited by organ toxicity due to their non-specific killing action and may have limited efficacy against resistant leukemic cells. Recent advances in conditioning regimens have focused on two main areas: firstly, optimization of dose intensity, such as the use of thiotepa-based regimens, which are noted for their strong ability to cross the blood-brain barrier and eradicate stem cells. The TBF combination exhibited strong anti-leukemic effectiveness in haploidentical, matched sibling donor, and unrelated donor transplants. It has the same prognosis as other regimens used for relapsed and refractory AML, such as FT and FLAMSA.13–15 Secondly, the integration of targeted agents and novel chemotherapeutic drugs. Among these, Mitoxantrone Liposome, as a new-generation anthracycline, has attracted significant attention due to its unique pharmacological properties. Unlike the standard form of mitoxantrone, its liposomal structure enables more precise targeting to cancerous tissues via the enhanced permeability and retention mechanism, which may boost leukemia-fighting effectiveness while notably lessening the dose-restricting adverse reactions of traditional anthracyclines, including heart toxicity and extramedullary toxicity.16,17 This has demonstrated its advantage in salvage therapy for R/R AML and provides a rationale for its incorporation into transplant conditioning regimens. In vitro experiments have shown that mitoxantrone liposomes can enhance sensitivity to gilteritinib in FLT3-ITD mutated AML patients. 4 In high-risk pediatric AML, patients treated with mitoxantrone liposome chemotherapy had similar remission rates compared to those receiving traditional idarubicin chemotherapy, but they experienced faster blood cell recovery and better safety profiles. 5 This trial evaluated the efficacy and safety of a novel conditioning regimen for allo-HSCT in patients with R/R AML. Our primary findings confirm that this regimen was a safe and effective conditioning regimen for R/R AML patients with poor prognosis.
Most importantly, through subgroup analysis, we identified in this specific context that the administration of post-transplant maintenance therapy may affect long-term disease-free survival. This finding is highly consistent with the recent consensus in the allo-HSCT field. The first one or two years post-transplant represent a high-risk period for relapse, a time when donor immune cells may not have fully established a potent GVL effect, or when residual leukemic cells may escape via immune editing mechanisms. The goal of maintenance therapy during this “window of vulnerability” is not to induce remission, but to eliminate MRD and prevent clinical relapse. Available maintenance strategies include hypomethylating agents (azacitidine, decitabine), targeted agents (e.g., FLT3 inhibitors, IDH1/2 inhibitors), or immunomodulatory drugs.18–22 Our data suggested that in patients receiving our novel conditioning regimen, subsequent maintenance therapy may improve OS.
Finally, there were some limitations of this study. Initially, the investigation was designed as a single -center prospective trial lacking direct random allocation when compared with a conventional conditioning protocol. Therefore, the observed efficacy advantages may be subject to selection bias. Secondly, the small sample size may have affected the power of the subgroup analyses and restricted our ability to explore efficacy in rarer subgroups (e.g., those with specific genetic mutations) in greater depth. Thirdly, regarding maintenance therapy, this study did not involve randomized assignment, and there was heterogeneity in the drugs, dosage and duration, introducing potential confounding factors in the interpretation of the results. Key questions remain unanswered, such as which patients benefit most from maintenance therapy, what the optimal duration is, and whether the prior use of Mitoxantrone Liposome influences the choice and efficacy of subsequent maintenance strategies. Future multi-center, randomized controlled clinical trials, incorporating comprehensive biomarker profiling, are needed to precisely identify the patient population most suitable for this regimen and to optimize post-transplant maintenance strategies.
Conclusion
In summary, this study provides a novel and promising conditioning regimen for R/R AML patients received salvage allo-HSCT, with the incorporation of Mitoxantrone Liposome being a core highlight of the regimen design.
Supplemental material
Supplemental material - Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial
Supplemental material for Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial by Juan Ren, Tongxin Zhang, Yuqi Wang, Huachao Zhu, Ruimin Liu, Pengcheng He, Xiaoning Wang in Cell Transplantation.
Supplemental material
Supplemental material - Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial
Supplemental material for Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial by Juan Ren, Tongxin Zhang, Yuqi Wang, Huachao Zhu, Ruimin Liu, Pengcheng He, Xiaoning Wang in Cell Transplantation.
Supplemental material
Supplemental material - Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial
Supplemental material for Efficacy and safety of mitoxantrone hydrochloride liposome/ thiotepa/ busulfan/fludarabine (MTBF) conditioning regimen for salvage allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory acute myeloid leukemia: A single - Arm prospective clinical trial by Juan Ren, Tongxin Zhang, Yuqi Wang, Huachao Zhu, Ruimin Liu, Pengcheng He, Xiaoning Wang in Cell Transplantation.
Footnotes
Acknowledgements
We thank all patients who participated in this study. No scientific data has been generated or modified using AI.
Ethical considerations
The study was in accordance with the Declaration of Helsinki and were approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University(No. XJTU1AF-CRF-2023- XK014)at December 14th, 2023.
Consent to participate
The patients/participants provided their written informed consent to participate in this study and publish the paper.
Author contributions
Xiaoning Wang and Juan Ren designed the trial and wrote the main manuscript text.Huachao Zhu,Yuqi Wang and Tongxin Zhang done the clinical observation. Ruimin Liu performed statistical data analysis and prepared figures. Pengcheng He coordinated and guided and reviewed the writing. All authors contributed to the manuscript’s draft and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was Supported by Clinical Medical Research Center Project of Xi’an Jiaotong University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Any data will be available at the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.