
Abstract
Impairments in a variety of cognitive processes, including concentration and attention, learning and memory, processing speed, and problem solving, are present in people with schizophrenia. Also seen in the condition are notable impairments in the ability to perform everyday tasks and to achieve normal functional milestones such as work, stable social relationships, and living independently. In this article I discuss recent research that has focused on quantifying the predictors of disability in real-world functioning, with cognitive impairment being one of the major predictors. Other important developments include the development of direct measures of the ability to perform the skills required to achieve everyday functional goals—skills referred to as “functional capacity.” Studies have shown that these abilities may be influenced by cognitive impairments and may be better predictors of disability than are cognitive deficits. I also examine the current literature on the treatment of cognitive impairments and functional disability, including both pharmacological and behavioral interventions.
Schizophrenia is a neuropsychiatric disorder that has been studied for well over a century. Even when the illness was first described, the prominence of the cognitive impairments attracted the attention of both clinicians and researchers. Yet, while these cognitive impairments have been studied for years, their importance for the long-term course of schizophrenia has only recently been appreciated. Specifically, impairments in cognitive functioning, measured with standardized clinical neuropsychological tests, are a consistent predictor of lack of everyday-living skills. These impairments in real-world outcomes are common and severe, with the majority of patients with schizophrenia showing evidence of reduced achievement in vocational functioning, independent living, and social outcomes. Very recently, performance-based assessment instruments designed to directly measure social, everyday-living, and vocational skills in people with schizophrenia have been developed. Evidence for the validity of these performance-based measures of functional skills (often referred to as functional capacity) has rapidly accrued. These measures are not subject to the types of limitations associated with either self-reports of everyday functioning or informant reports of everyday-living outcomes. This review will focus on the characteristics of cognitive impairment and disability in schizophrenia and will focus on recent developments in the performance-based assessment of everyday-living skills.
Disability and Cognitive Impairment
The increasing study of cognitive functioning in schizophrenia in the past decade is likely due in part to the recognition that impaired performance on clinical neuropsychological tests (Green, Kern, Braff, & Mintz, 2000) is related to the inability of people with schizophrenia to function in real-world settings. There are several findings that show the robustness of the relationship between cognitive impairment and functional outcome. Harvey et al. (1998) studied three different samples of older people with schizophrenia: patients admitted to an acute treatment unit, long-stay patients in a state psychiatric hospital, and patients discharged to nursing home care from a long-stay psychiatric hospital. In all three samples, the single best predictor of real-world functioning, rated by a clinician with a structured rating scale, was cognitive impairment. This finding held up despite the fact that there was no overlap in either cognitive performance or functioning between the patients who were at the extremes of the range of lifetime functional outcome.
Most patients with schizophrenia have substantial cognitive impairments, when compared both to overall normative standards and to their own premorbid functioning. Whether normal-range cognitive performance ever occurs in people with schizophrenia is controversial, and it has been argued that there are no patients without evidence of some impairments on traditional neuropsychological tests (Wilk et al., 2004). Leung, Bowie, and Harvey (2008) identified patients with cognitive performance in the normal range relative to normative standards and compared their real-world outcomes to patients whose performance was in the impaired range. Based on previously published studies of the relationship between employment and disability, the results of which suggested that disability compensation reduces the likelihood of work, Leung et al. hypothesized that normal cognitive abilities were not likely to override the potent employment disincentive of disability compensation. In fact, of the three domains of real-world functioning examined—employment, social outcomes, and the level of independence and financial responsibility in community residence—only residential status was associated with cognitive functioning. The authors concluded that although cognitive impairment may predict some aspects of real-world outcome, social and environmental factors provide a very strong signal in certain functional domains.
Dimensions of Cognitive Impairment
For decades, there has been interest in whether specific profiles of cognitive impairments in schizophrenia provide a window into impaired brain functions that might underlie the illness. These specific profiles have been defined in terms of either the cognitive domains involved—such as learning and memory, attention, and verbal and spatial skills—or in terms of the brain regions associated with tasks that show impairment in neurologically injured patients—such as the frontal lobe, temporal lobe, or parietal lobe. Despite this long-term interest in profiles and specific neurological substrates for cognitive deficits, the empirical data from comprehensive cognitive assessments using standard neuropsychological tests have suggested a relatively homogenous profile of impairments across virtually all cognitive ability areas (Dickinson, Iannone, Wilk, & Gold, 2004). When data from very-large-scale studies of people with schizophrenia are examined, a very simple dimensional structure has often been detected. For instance, in the Controlled Antipsychotic Trials of Intervention Effectiveness (CATIE) study, a sample of more than 1,300 people with schizophrenia was assessed with a comprehensive cognitive assessment battery. The best-fitting model, obtained with confirmatory factor analysis, was a single-factor model, in contrast to previous smaller-sample studies that generated more complex solutions, even though 16 cognitive tests were administered (Keefe, Bilder, et al., 2006). Also interesting was the finding that a very small subset of the cognitive measures—four tests that took a total of 18 minutes to complete—accounted for 87% of the variance in the total score from the entire battery. These findings are consistent with the conclusions of other researchers that impairments on neuropsychological tests are global in nature and do not describe either multiple cognitive domains or impairments that would be consistent with regional brain dysfunctions affecting only a few cognitive abilities, and that the overall severity of impairment can be indexed with a few measures. Of special interest is the finding that abbreviated measures of processing speed—tests such as trail making and various coding tests—are typically the tests on which people with schizophrenia show the most impairment overall and that performance on such tests is also the single best predictor of total performance scores on extended batteries of tests (Keefe, Bilder, et al., 2006).
Refining the Assessment of Predictors of Disability
Interest in isolating the skills that are required to succeed at crucial daily activities and assessing them directly has increased recently. Specifically, performance-based measures to examine social competence, vocational potential, and the ability to perform everyday-living skills have been developed. While most of these measures were initially developed to measure aging-related changes in activities of daily living, a number of them have been developed or adapted for use in populations with severe mental illnesses such as schizophrenia.
One of the reasons that these measures have achieved rapid acceptance is that several lines of evidence suggest that the measurement of real-world functioning in schizophrenia may be more complicated than a superficial consideration would suggest. Several recent studies have suggested that people with schizophrenia have deficits in the ability to evaluate the severity of their own cognitive and functional disabilities. For instance, Keefe, Poe, Walker, Kang, and Harvey (2006) obtained ratings of cognitive functioning on a structured scale from, in each case, a schizophrenia patient, an informant, and the interviewer who interviewed the two. The overlap between self-reports and performance on a cognitive assessment battery was negligible (Pearson's r = .04), whereas informants and interviewers provided ratings that were much more closely congruent with a patient’s actual performance. McKibbin, Patterson, and Jeste (2004) found that self-reports of disability on the part of people with schizophrenia were essentially uncorrelated with performance-based assessments of cognition and functional skills. Similarly, Bowie et al. (2007) found that case managers who were unaware of a patient’s performance on cognitive and functional assessment batteries provided real-world functioning ratings that were much more convergent with the patient’s performance than with the patient’s self-report of his or her functioning.
Although it is unclear if the factors that lead to misestimated cognition and functional outcomes are the same as those that lead to unawareness of symptoms, there are clearly significant problems with relying on patient self-report as the sole index of real-world functioning. Performance-based measures address what an individual can do in an assessment setting—often referred to as “skills competence” or “functional capacity.” In contrast, while real-world outcomes are constrained by competence, what an individual actually does in the real world is affected by much more than ability. A number of studies of the relationship between functional capacity, cognitive performance, and real-world outcomes in schizophrenia have been conducted, and they have provided substantial information.
Several functional-capacity measures have been employed in schizophrenia research, and they have largely been focused on everyday-living skills and social competence. In several studies examining prediction of real-world outcomes, we have used the Social Skills Performance Assessment (SSPA; Patterson, Moscona, McKibbin, Davidson, & Jeste, 2001) and/or the UCSD Performance-Based Skills Assessment (UPSA; Patterson, Goldman, McKibbin, Hughs, & Jeste, 2001). The SSPA has two role-played interactions, one instrumental and one social. The UPSA has five subscales assessing financial, communication, planning, transportation, and home-based activities in a set of performance tasks.
In the first of these studies (Bowie, Reichenberg, Patterson, Heaton, & Harvey, 2006), we found that scores on the performance-based capacity measures mediated the relationships between performance on clinical neuropsychological tests and real-world outcomes rated by clinicians who saw the patients often enough to be quite familiar with them. Further, we found that clinical symptoms of the illness, including psychosis, negative symptoms such as blunted affect and amotivation, and depression, did not influence scores on performance-based measures of functional capacity but that these symptoms did add to ability of the performance-based measures to predict real-world functional outcomes. Later studies have refined these findings and identified the specific relationships among different domains of cognitive functioning, functional-capacity measures, and real-world outcomes (Bowie et al., 2008), as well as identifying specific negative and positive (psychotic) symptoms that mediate the relationship between these capacity measures and real-world outcomes (Leifker, Bowie, & Harvey, 2009).
Across seven published studies that used the UPSA, several interesting consistencies have emerged. First, performance on cognitive assessments have been remarkably consistent with UPSA scores, with correlations ranging very narrowly (from r = .60 to r = .65; see Leifker, Patterson, Heaton, & Harvey, in press, for a review). Second, test–retest stability has been consistently high (r > .70) and improvements in performance with practice consistently low (changes less than 0.2 standard deviations over multiple retests). Finally, as noted earlier, as with cognitive performance, the severity of current clinical symptoms has consistently been found to be uncorrelated with performance on these measures; this finding is consistent with the results of the correlation between neuropsychological test performance and clinical symptoms.
Several studies have shown that these performance-based functional-capacity measures are sensitive to change in clinical treatment studies. For instance, Patterson et al. (2006) reported that UPSA scores improved by more than a standard deviation in response to a functional skills training program. Harvey, Patterson, Potter, Zhong, and Brecher (2006) found that SSPA scores improved substantially in response to antipsychotic treatment, with the extent of treatment-related change predicted by, but not completely accounted for by, improvements in cognitive performance.
It has been understood for years that cognitive impairments are an intrinsic part of the schizophrenia syndrome, and it has been found that cognition is similarly impaired in schizophrenia patients across multiple Western countries. Recently, we expanded these results to functional-capacity measures. In a study that used performance-based measures to examine cognition and everyday-living skills, as well as collecting case manager ratings of real-world functioning and milestones such as residential status, Harvey et al. (2009) found that cognitive performance and the ability to perform everyday-living skills were strikingly similar in people with schizophrenia living in urban New York and in those living in rural Sweden. Further, case manager ratings of patients' abilities to perform everyday-living skills were essentially identical across both samples. Interestingly, the rates of independence in residential status were quite different in the two countries, likely because of the substantial social support received in Sweden compared to the United States. Most directly, the local health authority directly pays more than 90% of the rent of people diagnosed with schizophrenia in that Swedish region, markedly influencing the correlation between ability and real-world outcomes.
The results of this study lead to two conclusions. First is that the functional abilities measured with performance-based measures may, like cognitive impairments, be a central feature of schizophrenia. Functional capacity was as similar across different Western countries as cognitive test performance was and, like cognitive impairments, did not differ in the level of impairment as a function of the local environment or severity of symptoms. The second important point is that factors that are not associated with abilities can influence real-world functional outcomes. Thus, these data suggest that measurement of cognitive impairment or functional abilities will not perfectly predict real-world outcomes, and they also indicate that a careful assessment of environmental, cultural, and other variables such as motivation needs to be performed. Similarly, treatment of cognitive impairment or of deficits in functional capacity will almost certainly not be adequate to improve real-world functional outcomes on its own.
A final issue is the impact of amotivation and other negative symptoms on real-world outcomes. In a recent study (Leifker et al., 2009), we examined the impact of clinically rated social amotivation (reduced motivation to engage in social activities) and social competence as measured with the SSPA on case-manager-rated real-world social outcomes. What we found was that social amotivation had a much greater impact on social outcomes than did social competence. While cognitive functioning and social competence were correlated with real-world social outcomes, neither predicted real-world social outcomes when motivation to engage in social activities was taken into account. Thus, social skills training might be expected to make minimal headway in reducing real-world social functioning deficits in patients showing reduced motivation to engage in social activities. Figure 1 shows our current working model of the relationships between cognitive functioning, functional capacity, symptoms, social factors, and real-world outcomes. Note that skills performance refers to real-world functioning, as the end product of all of the factors described earlier.
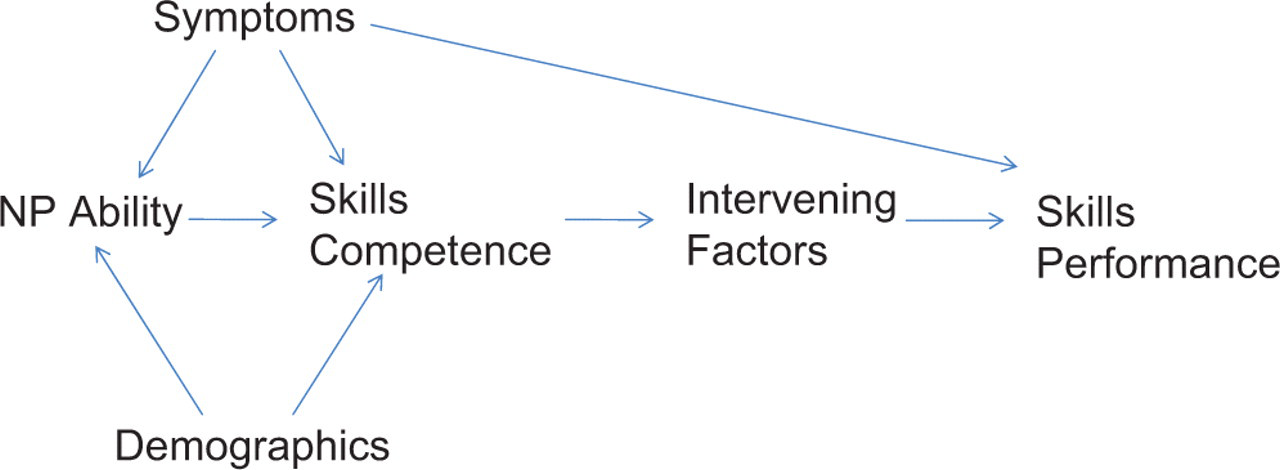
Functional capacity, functional outcomes, and intervening factors. Neuropsychological (NP) ability may impact the ability to perform everyday living skills, which in turn impacts functional milestones in real-world settings via intervening factors such as disability compensation. Symptoms of schizophrenia may impact at several different levels, including influences on NP ability, everyday living skills, and direct impact on real-world functioning.
Treatment of Cognitive Impairments
Although there are multiple influences on real-world outcomes besides cognitive or functional abilities, these abilities will constrain the extent to which people with schizophrenia can function in the community. As a result, treating cognitive and functional deficits is important. There was considerable optimism regarding the possibility that second-generation antipsychotics, in contrast to older medications, would have a substantial impact on cognitive functioning. This optimism has largely dissipated because of the mostly negative cognitive enhancement results of the CATIE trial (Keefe et al., 2007) and the recent demonstrations that cognitive changes with atypical medications may simply reflect the typical improvements in performance associated with practice and exposure to test materials (Goldberg et al., 2007). Multiple pharmacological strategies have also been attempted following the development of the Measurement and Treatment Research for Improving Cognition in Schizophrenia (MATRICS) consensus criteria on suitable research designs. To date, the success of these interventions has been quite limited (see Recommended Reading for some reviews of this topic), but there are multiple as-yet-untested pharmacological interventions that could be evaluated in the near future.
One area that has had considerably more success has been that of cognitive remediation, which is typically delivered as a computerized drill-and-practice plus executive functioning training program aimed at improving cognitive abilities. Although historically this approach has had little success in schizophrenia, recent modifications in the way that these interventions are delivered have led to an increase in the number of positive results (see McGurk, Twamley, Sitzer, McHugo, & Mueser, 2007, for a review). Several findings have been important and encouraging. For example, studies conducted with subtly different remediation systems have all led to real-world functional gains, particularly in the area of employment success (McGurk, Mueser, Feldman, Wolfe, & Pascaris, 2007; Wexler & Bell, 2005). An important feature of all of these interventions was that all patients who received cognitive remediation were also involved in supported programs aimed at vocational functioning. Further, these gains were found to be persistent long after the intervention ended, at follow-ups up to 3 years (McGurk, Mueser, et al., 2007).
A series of recent papers has also suggested that these cognitive remediation interventions have direct biological as well as cognitive effects. For example, Fisher, Holland, Merzenich, and Vinogradov (2009) showed that cognitive remediation interventions that led to improvements in verbal memory performance, including both working memory and episodic memory, also led to changes in psychophysiological indices of the intactness of verbal information processing. Further, a follow-up analysis (Vinogradov et al., 2009) suggested that there was a correlation between improvements in memory functioning and serum levels of brain-derived neurotrophic factor, an index of brain repair processes. Thus, not only does cognitive remediation lead to improvements in cognitive performance and real-world outcomes, it also appears to exert its effect through measurable brain processes, and this may give us further guidance in developing more efficient interventions.
Conclusion
Disability in schizophrenia is related to cognitive impairments and to deficits in the ability to perform critical social, vocational, and everyday-living skills. Recent research has evaluated the relationships between these performance-based assessments of functional capacity and patient characteristics such as negative symptoms and depression, as well as societal factors such as disability compensation and social support. The results of these studies suggest that ability variables define an individual’s functional potential in the real world and that functional outcomes are influenced, sometimes very substantially, by factors other than skills and abilities. Thus, it has been recognized that skills-based interventions, whether they involve teaching and training or are pharmacological interventions aimed at augmenting performance, are likely to be insufficient on their own to reduce disability in people with schizophrenia. It has also been found that scores on performance-based measures of everyday-living skills are also very similar across samples of people with schizophrenia in the United States and Sweden, which could suggest that these skills deficits are as intrinsic to schizophrenia as cognitive deficits are. The next decade of research in this area may reveal even more substantial ways to improve cognitive functioning and functional disability in schizophrenia.
Recommended Reading
Green, M.F., Kern, R.S., Braff, D.L., & Mintz, J. (2000). Neurocognitive deficits and functional outcome in schizophrenia: Are we measuring the “right stuff?” Schizophrenia Bulletin, 26, 119–136. A landmark paper providing the rationale for cognitive enhancement in schizophrenia.
Harvey, P.D. (2009). Pharmacological cognitive enhancement in schizophrenia. Neuropsychology Review, 19, 324–335. Describes the results of previous studies of cognitive enhancement in schizophrenia.
Sharma, T., & Harvey, P.D. (Eds.). (2000). Cognitive functioning in schizophrenia: Characteristics, correlates, and treatment strategies. Oxford, England: Oxford University Press. Reviews the state of the art of research on cognitive functioning in schizophrenia, with the highest-profile experts in the field contributing.
Footnotes
The author declared that he had no conflicts of interest with respect to his authorship or the publication of this article.