
Abstract
Family violence is common and brings tremendous costs to individuals, relationships, and society. Victims are vulnerable to negative outcomes across a host of dimensions, including cognitive performance, impulse control, emotion regulation, and physical health. Links between family violence and various problems have been established, yet the specific processes underlying these associations are poorly understood, resulting in the stunted development of effective interventions. This article addresses two key questions: How and why does family violence cause these myriad problems? The self-control strength model of family violence provides novel answers. The model integrates components of existing theories, extending them by pinpointing self-control strength as an explanatory and predictive factor, and can serve as a framework for interventions.
Every year, millions of people experience family violence (World Health Organization, 2013). About 275 million children experience child abuse, and worldwide, more than 30% of women who have been in relationships have been exposed to intimate-partner violence during their lifetime. It is estimated that family violence kills about nine times more people than civil wars (Hoeffler & Fearon, 2014). Furthermore, exposure to family violence is an important risk factor for physical disease, psychopathology, professional and academic failure, substance use, and suicide (Felitti et al., 1998). What is more, experiencing family violence predicts people’s use of violence themselves (Ehrensaft et al., 2003).
Despite significant advances, mechanisms explaining these associations remain largely unknown, which hinders our ability to explain and predict family violence and, importantly, hampers the development of effective interventions. Therefore, important theoretical questions remain. We address the two most central—namely, how and why does family violence cause such myriad problems?
We introduce the self-control strength model of family violence and present existing, albeit initial, evidence that supports four hypotheses derived from the model. As shown in Figure 1, first, family violence and associated distal and proximal stressors (e.g., poverty, harsh and unpredictable social environments) reduce victims’ capacity for self-control (paths a and b). Second, depletion of self-control strength—a person’s current level of self-control, which is key to how successfully people can engage in self-control—results in family violence and associated stressors (paths d and e), and third, this helps explain the broad range of family violence’s negative effects on personal and social well-being (paths f and g). Fourth, and crucially, improving self-control strength can alleviate many of these ill effects (boldfaced labels in Fig. 1), indicating that the model has clear implications for treatment.
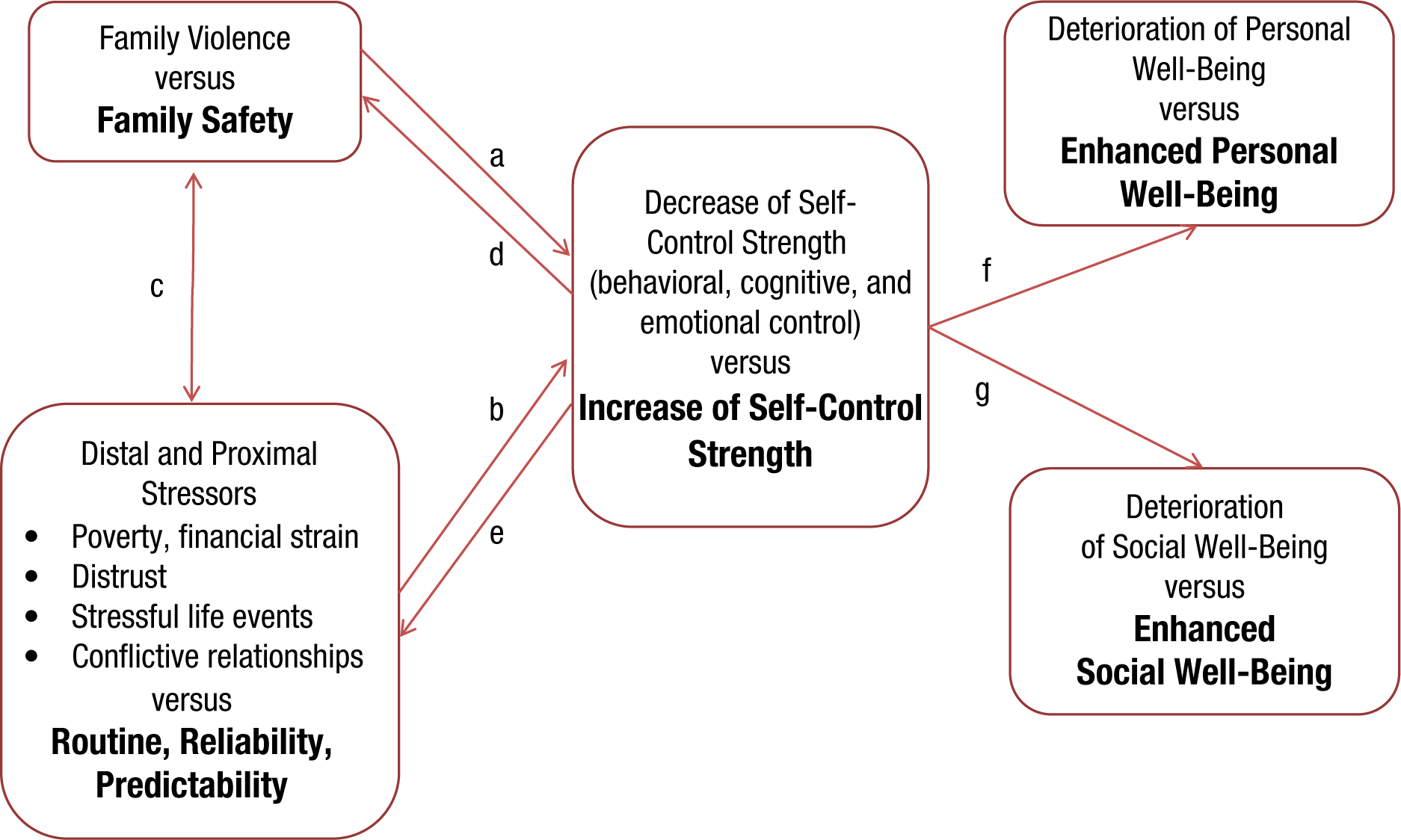
The self-control strength model of family violence.
Self-Control Strength
Self-control is the capacity to stop, override, or alter unwanted responses and behaviors in order to bring them into agreement with standards (Tangney, Baumeister, & Boone, 2004). The concept of self-control comprises self-regulation, deliberateness, executive functioning, and future orientation. It operates in a multitude of domains, including school and work achievement, healthy living, and social skills (De Ridder, Lensvelt-Mulders, Finkenauer, Stok, & Baumeister, 2012). Lacking self-control is linked to underachievement, mental and physical illness, relationship problems, substance abuse, crime, and violence (Tangney et al., 2004).
Self-control can be decomposed into a relatively stable trait component and a changeable state component. The stable component enables people to regulate their behavior in a consistent manner across time and circumstances. The changing component is a person’s current degree of self-control, which varies across time and circumstance. This changing component, self-control strength, is at the heart of our model. Exerting self-control requires energy and impairs further acts of self-control. Laboratory and field studies from all over the world have demonstrated that even brief exertions of self-control decrease self-control strength, causing decrements on other, seemingly unrelated tasks requiring self-control or decision making (Hagger, Wood, Stiff, & Chatzisarantis, 2010; Hofmann, Vohs, & Baumeister, 2012; Vohs et al., 2008). Converging evidence from longitudinal studies indicates that the stable component of self-control too can become depleted by the accumulation of stressors and their chronicity (e.g., Miller, Chen, & Parker, 2011). To illustrate, a longitudinal study by Lengua, Honorado, and Bush (2007) found that increases in the number of risk factors to which children were exposed, including poverty, household density, unpredictable living conditions, and stressful life events, predicted decrements in subsequent self-control. Thus, evidence from laboratory and field studies suggests that depleted self-control strength can reduce people’s ability to cope with everyday life, work, and relationships.
Self-control strength can be restored and improved after it has been depleted: Resting, remembering cherished values, and consuming glucose can bring people’s self-control strength back to prior levels (Baumeister, Vohs, & Tice, 2007; Schmeichel & Vohs, 2009). Further, similar to bodily strength, self-control strength improves with regular, judicious exercise (for reviews, see Baumeister, Gailliot, DeWall, & Oaten, 2006; Berkman, Graham, & Fisher, 2012; Diamond & Lee, 2011), and training effects may lead to a long-term change of the more stable component of self-control when people are motivated (cf. Hennecke, Bleidorn, Denissen, & Wood, 2014). One of the crucial benefits of training self-control is enhanced self-control in domains outside of those used in training (Piquero, Jennings, & Farrington, 2010).
The Self-Control Strength Model of Family Violence
We define family violence as relational escalations in which one or more family members engage in verbal or physical aggression (e.g., beating, threatening, pushing, swearing, slapping). During these affectively charged interactions, one or more family members typically engage in destructive behaviors (e.g., insult, yell at, or ignore the partner) and respond to such behavior in a similarly destructive fashion, escalating into patterns that fuel the cycle of violence.
The likelihood of perpetrating family violence is exacerbated by distal and proximal stressors (Fig. 1, path c). These include low socioeconomic status; abuse in the family of origin; alcohol use; stressful life events; anxiety and vigilance to threat; harsh, inconsistent, or unsupportive social networks; distrusting, conflictive, or neglectful relationships; and chaotic living conditions (e.g., Deater-Deckard, 2014; Felitti et al., 1998; Straus & Gelles, 1988). Therefore, one key to unraveling the effects and maintenance of family violence lies in understanding why stressors can eventuate in family violence. The answer to this question may lie in self-control strength.
Our model holds that family violence and decreased self-control strength have reciprocal relationships and can cause a potentially vicious circle. Conflictive, low-quality relationships (Miller et al., 2011) and harsh, inconsistent parenting (Lengua et al., 2007) deplete self-control strength. Depletion of self-control strength can cause aggression and intimate-partner violence. For example, participants who were ostensibly provoked by their partner were more aggressive toward their partner when they were experimentally depleted than when they were not depleted (Finkel, DeWall, Slotter, Oaten, & Foshee, 2009). In the following sections, we review four novel hypotheses drawn from the model and existing research supporting them.
Family violence and associated stressors deplete self-control strength
Depletion of self-control strength increases as a function of the severity and chronicity of family violence and associated stressors (Fig. 1, paths a and b), along with a paucity of opportunities to replenish self-control strength. For example, children exposed to family violence demonstrate poor academic and social competence compared to non-maltreated children, and low self-control explains this difference (Pears, Fisher, Bruce, Kim, & Yoerger, 2010). As compared to matched controls, child victims of family violence show deficits in neural circuits that support cognitive control (Mueller et al., 2010) and social functioning (Hanson et al., 2010). In a prospective longitudinal study, Evans and Schamberg (2009) found that childhood poverty predicts impairments in executive functioning over time and that this link is mediated by chronic stress. Finally, unpredictable parenting and living conditions exacerbate the impairment of self-control strength (Valiente, Lemery-Chalfant, & Reiser, 2007), which points to the potential of family violence and associated stressors to impair self-control strength.
Several pathways may explain the link between family violence and weakened self-control strength. Family violence undermines feelings of trust and security, causing activation of threat responses and stress (Davies & Woitach, 2008). Excessive threat vigilance may tax the limited resources needed to exert self-control in other areas of functioning (e.g., academic, social). Trauma-related problems associated with family violence, such as post-traumatic stress disorder, can undermine self-control strength (Van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005). Victims often suffer from sleep disturbances, difficulties concentrating, and intrusive thoughts about the trauma, any of which could impair self-control strength.
Research testing multiple pathways as integrated or separate (and testing them against each other) would be welcome. Adjacent to the current debate about mechanisms underlying self-control strength and depletion (Inzlicht, Legault, & Teper, 2014), work that can differentiate between victims’ ability versus motivation to exert self-control is important. Most likely, the two work together. Exposure to family violence may teach victims that exerting self-control (e.g., delaying gratification) is not adaptive because promised long-term rewards rarely materialize. Further, losing self-control can help people achieve goals (e.g., if aggression enables people to get their way or if emotion dysregulation leads them to get the attention they crave; Simons & Burt, 2011). The net result would be little practice using and/or lack of motivation to use self-control strength, thereby contributing to underdeveloped effectual ability.
Depletion of self-control strength contributes to the development and maintenance of family violence
The second hypothesis is that self-control depletion exacerbates family violence and related stressors (Fig. 1, paths d and e). During arguments, one family member may verbally, physically, or emotionally abuse another. The victim may have the urge to respond aggressively, thereby establishing a vicious circle of mutual harm. In order to prevent conflict from escalating into violence, self-control is needed to restrain aggressive impulses. People with depleted self-control cannot de-escalate well nor enact constructive behavior (Finkel et al., 2009).
Abundant research shows that low levels of self-control are causally related to intimate-partner violence, distrust, and harm. To illustrate, people whose self-control strength is depleted, compared to people whose self-control strength is intact, behave more aggressively toward strangers (DeWall, Baumeister, Stillman, & Gailliot, 2007) and toward their romantic partner (Finkel et al., 2009). Following a provocation, angry rumination impairs self-control strength, which in turn increases aggressive behavior (Denson, Pedersen, Friese, Hahm, & Roberts, 2011). Further, empirical evidence consistently shows that depleted self-control invites distrust (Righetti & Finkenauer, 2011). Finally, depletion of self-control strength undermines people’s capacity to inhibit undesirable behavior (risk taking, cheating, stealing, impulsive spending; e.g., Freeman & Muraven, 2010; Vohs & Faber, 2007). Thus, impairments in self-control strength make people more likely to engage in unwanted, impulsive, and unhealthy behavior, thereby exacerbating stressors and, ultimately, family violence.
Low self-control mediates the link from family-violence exposure to poor psychosocial functioning
Exposure to family violence and associated stressors can have devastating consequences for victims’ personal (Felitti et al., 1998) and social well-being and relationships (Ehrensaft et al., 2003). Victims exhibit elevated rates of depression, physical illness (e.g., cancer, obesity, heart disease), alcohol and drug use, unemployment, and mortality. Social problems include teenage pregnancy, lack of social support, social isolation, and divorce. This panoply of psychosocial problems is strikingly similar to those associated with low levels of self-control (Tangney et al., 2004). Such similarity fits the third hypothesis from the model—namely, that impaired self-control mediates the problems stemming from family-violence victimization (Fig. 1).
Studies that pinpoint why self-control strength may be relatively absent among victims of family violence and how this weakness contributes to poor psychosocial functioning will be important. Particularly promising candidate mechanisms include cognitive processes (e.g., vigilance, angry rumination), affective responses (e.g., anxious arousal, stress), and behavioral problems (e.g., poor emotion regulation, inhibition).
Effects of family violence can be alleviated by strengthening self-control
Fourth, and crucially, the model predicts that strengthening self-control may help diminish, and possibly reverse, the devastating consequences of family violence (Fig. 1, boldfaced labels). Individual, social, and environmental changes can increase self-control strength and other functions of the executive system. Adoption studies show that executive functioning and self-regulation improve significantly after children with histories of abuse and/or neglect are separated from their parents (e.g., Jaffee, 2007). Reflecting such improvement, Duyme, Dumaret, and Tomkiewicz (1999) found that children who had been abused and/or neglected during infancy experienced an increase of between 8 and 19 IQ points after adoption.
Self-control strength can also be improved directly through exercises and other activities. A meta-analysis by Piquero et al. (2010) concluded that intervention programs have successfully improved self-control among children and adolescents—and also reduced delinquent behavior. Diamond and Lee (2011) showed that children’s executive functioning can be improved by various activities such as games, aerobics, martial arts, yoga, and mindfulness training. These are most effective when they require repeated self-control activities that gradually increase in difficulty.
Studies with young adults showed that self-control can be improved through habit-breaking exercises, such as switching to use one’s nondominant hand for minor tasks like opening doors and brushing teeth and following speech rules (e.g., saying “yes” instead of “yeah”; not swearing; Baumeister et al., 2006). Finkel et al. (2009) showed that after doing these exercises for 2 weeks, romantic partners exhibited significantly reduced aggressive responses to provocations. Even physical exercises seem to build self-control. Hung and Labroo (2011) showed that strengthening physical muscles improved self-control, enabling people to resist food temptations and tolerate pain longer. Oaten and Cheng (2006) showed that a 2-month physical-exercise regimen improved performance on laboratory tests of self-control and also yielded behavioral improvements in healthy eating, spending, and household routines. Still, more research on building self-control strength is needed, particularly with high-risk samples such as victims and witnesses of family violence.
Conclusions and Implications
Impairments of self-control strength appear to play a crucial role in many aspects of the maintenance and consequences of family violence, which supports the self-control strength model of family violence. An implication of this model is that researchers and practitioners should expect impairment of self-control strength and problems with self-regulation in the wake of family violence, as opposed to treating them as deviant responses or separate problems. Victims of family violence may lose control over interpersonal relationships, work performance, and a host of other duties needed for everyday life.
Parts of the model require further investigation. Research testing the full model directly using prospective longitudinal designs would be fruitful. Such correlational research would benefit from complementary, ideally experimental, work that examines whether and how pathways in the model vary across different aspects of self-control (executive functioning, emotion regulation), roles (targets of violence, witnesses, and perpetrators), and age groups (children, adolescents, adults). Research examining individual differences and the interplay of stable and changing components of self-control in response to family violence and associated stressors is needed. Advances in genetic methodologies will allow for separating the roles played by environmental and genetic risk mechanisms in self-control and family violence, inasmuch as genes have been implicated in self-control (Deater-Deckard, 2014) and susceptibility and resilience to family violence and associated stressors (Belsky & Pluess, 2009).
Although family violence is detrimental to the personal and social well-being of both victims and perpetrators, the malleability of self-control strength suggests promising avenues for therapeutic intervention and improvement. Programs to build, restore, and maintain self-control strength may potentially reduce and even counteract some harms. If so, then troubled families and damaged individuals may be able to reclaim some degree of well-being and happiness.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
C. Finkenauer and K. Schoemaker were supported by Grant ZonMw 80-82470-98-017 from the Netherlands Organisation for Health Research and Development. M. Bartels and C. Finkenauer have received funding from the European Union Seventh Framework Programme (FP7/2007-2013) under Grant Agreement No. 602768.