
Abstract
Biogenetic explanations of mental disorder are increasingly prominent. However, they have decidedly mixed implications for how affected persons are perceived. We review evidence of these mixed blessings from three perspectives: how people with mental disorders are viewed by the public, by themselves, and by clinicians. Although biogenetic explanations may soften public stigma by diminishing blame, they increase it by inducing pessimism, avoidance, and the belief that affected people are dangerous and unpredictable. These explanations may also induce pessimism and helplessness among affected people and reduce the empathy their treating clinicians feel for them. We interpret these findings in light of social psychology research on essentialist and mechanistic thinking.
Keywords
Biological explanations are on the rise in the mental health professions. Researchers are making rapid advances in the neurobiology and genetics of mental disorders, supported by major initiatives. The National Institute of Mental Health’s new Research Domain Criteria framework is shaking up classification, abandoning the Diagnostic and Statistical Manual of Mental Disorders’s explanatory agnosticism by classifying mental disorders according to their biological causes. Rates of psychopharmacological treatment increased from 1998 to 2007 while rates of psychotherapy declined, the former easily exceeding the latter (Olfson & Marcus, 2010). Psychiatry journals dominate the clinical literature, influencing clinical psychology journals much more than clinical psychology journals influence them (Haslam & Lusher, 2011).
This trend has not been confined to scientists and clinicians but has altered how laypeople think about abnormality. Over the past decade, neuroscience has received increasing media coverage, and psychopathology is the second most common context in which it is raised (O’Connor, Rees, & Joffe, 2012). Much of this coverage has been optimistic and laudatory, presenting neurobiological processes as the ultimate source of mental illness and the proper target for clinical intervention (Racine, Waldman, Rosenberg, & Illes, 2010).
A recent meta-analysis demonstrated that the public’s understanding of mental disorder has changed in ways that track these media developments. Combining studies conducted in the United States, Europe, and Australia, Schomerus et al. (2012) found that the proportion of people endorsing genetic inheritance and brain disease as causes of schizophrenia and depression rose steeply between 1990 and 2006. In the case of depression, parallel increases were evident in the proportion of people endorsing medication as the most appropriate treatment and medically trained psychiatrists as the most appropriate treating clinicians (the increase for schizophrenia, from a very high baseline, was not significant).
It is tempting to view these historical developments as signs of unambiguous progress. On this view, advances in neuroscience and psychiatric genetics improve the understanding, diagnosis, and treatment of mental disorders and enhance the public’s mental health literacy. Unfortunately, this appealing progress narrative is challenged by evidence that public attitudes have become less enlightened, not more. Schomerus and colleagues (2012), for example, found that at the same time biogenetic explanations were becoming more popular, social acceptance of people suffering from depression was unchanged and acceptance of people with schizophrenia sharply declined.
Biogenetic Explanations and Stigma
These historical trends mirror a body of survey and experimental research showing that biogenetic explanations of mental disorders are often associated with more stigmatizing attitudes. Although some writers had hoped that biogenetic explanations might reduce the stigma of mental disorder by reducing the personal responsibility and blame that are commonly ascribed to sufferers, early studies found that people who endorsed these explanations were more fearful, rejecting, and punitive (Dietrich et al., 2004; Mehta & Farina, 1997; Phelan, 2005; Walker & Read, 2002). One challenge in assessing this work is that stigma is not monolithic, and its different aspects might respond differently to biogenetic explanations. Stigma can be seen as encompassing the tendency to blame affected people for their problems, the perception that they are dangerous and unpredictable, and the belief that they are unlikely to recover (“prognostic pessimism”).
In an effort to clarify this complex literature, Kvaale, Gottdiener, and Haslam (2013; Kvaale, Haslam, & Gottdiener, 2013) carried out two meta-analytic projects on the links between biogenetic explanations and these multiple components of stigma. One project examined 25 correlational studies on the naturally occurring associations between explanations and stigma for a variety of mental disorders, and the other examined 28 studies in which explanations were manipulated experimentally.
Findings were highly consistent across the two projects. In both the correlational and the experimental analyses, biogenetic explanations were associated with a reduced tendency to blame people with mental disorders for their problems but an increased tendency to perceive them as dangerous and unpredictable. Biogenetic explanations were associated with a desire for greater social distance in correlational studies, although they were not reliably associated with social distance in experimental studies. Finally, biogenetic explanations were associated with greater prognostic pessimism in the experimental studies. These effects were generally small to medium in magnitude by conventional standards, with the blame-reduction effects the strongest, and evidence that they translate into discriminatory behavior is currently lacking. Nevertheless, this comprehensive quantitative review reveals that biogenetic explanations have mixed blessings for stigma, reducing one component but increasing others.
The Mixed-Blessings Model
The findings of the two meta-analyses, and our proposed account of them, are presented in Figure 1. Biogenetic explanations for mental disorders reduce blame because symptoms are attributed to causes that are outside the person’s control. The attributional account of responses to deviant behavior (Weiner, 1993) argues that blame and attributions of responsibility hinge on whether or not the behavior’s cause is seen as controllable and that people tend to be more sympathetic when an undesirable behavior is perceived to be uncontrollable. An alternative way to frame this distinction is whether the behavior is explained mechanistically or in terms of free will. For example, Shariff et al. (2014) recently showed that people who read a magazine article propounding a mechanistic neuroscience-based explanation of behavior judged an offender to be less blameworthy than those who read a neutral article, and were less punitive toward the offender for this reason.
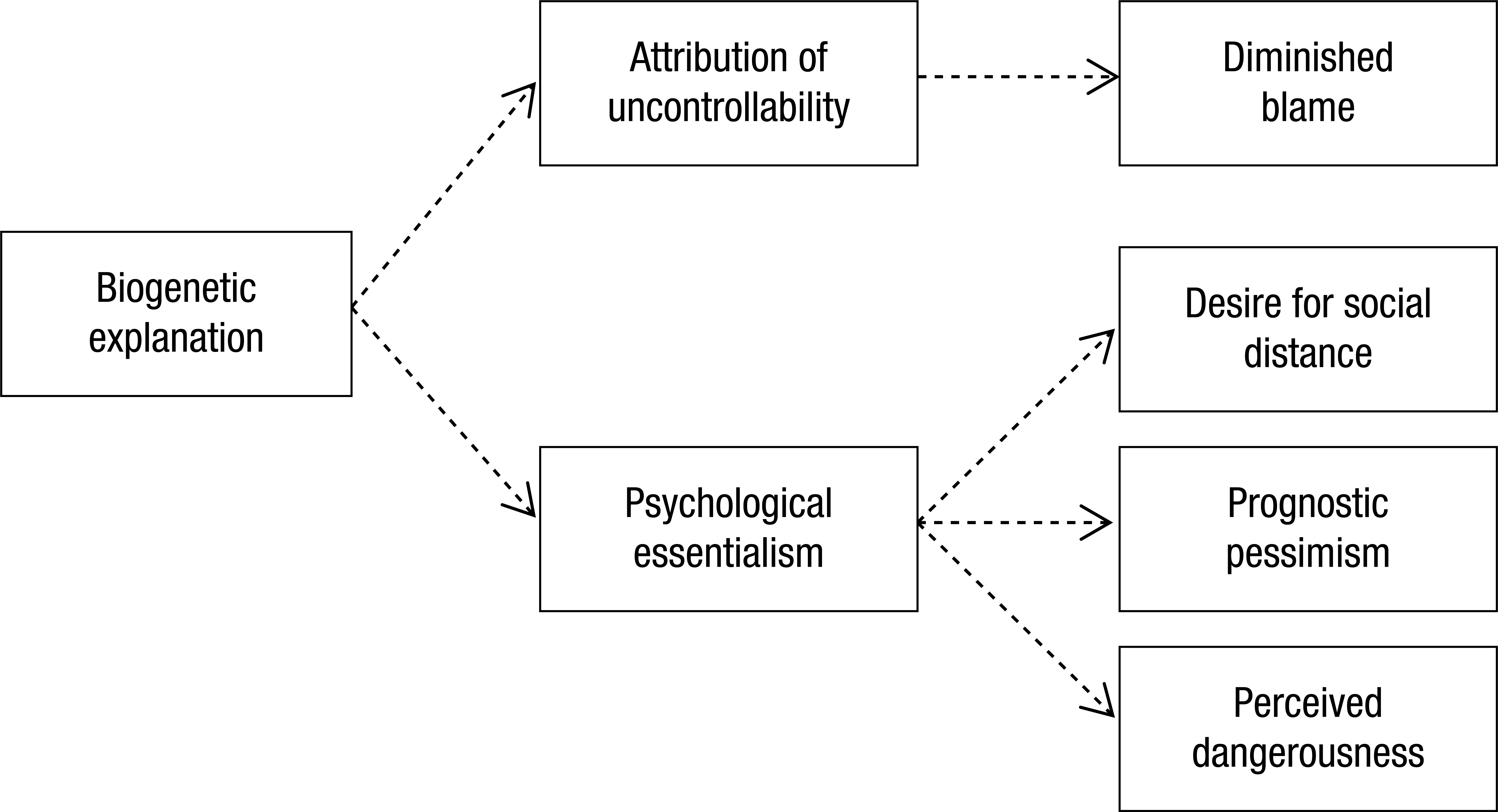
The mixed-blessings model of biogenetic explanations and stigma. Because they engender two distinct ways of thinking about people with mental disorders (attribution of uncontrollability of symptoms and psychological essentialism), biogenetic explanations reduce one facet of stigma (blame) but increase three others (desire for social distance, prognostic pessimism, and perceived dangerousness).
If attributions of uncontrollability or mechanistic thinking were the only implications of biogenetic explanations, then they might have uniformly positive effects on stigma. However, there is now strong evidence that these explanations also trigger essentialist thinking. Psychological essentialism is the belief that a fixed, hidden, and identity-determining cause—such as the atomic structure of a chemical element or the DNA of a biological species—generates the observed properties of a category. People intuit the existence of the essence without being able to observe it, often believing that there are “essence experts” who could identify it (Proctor & Keil, 2006).
When applied to social categories, essentialist thinking is often grounded in biological differences between people, and it frequently has destructive implications. Social psychologists have explored its bearing on conceptions of gender, race, sexuality, and mental disorder (e.g., Haslam & Ernst, 2002). Essentialist understandings of race, for example, are associated with racial prejudice (Keller, 2006) and the desire not to cross perceived racial boundaries (Williams & Eberhardt, 2008). In addition to deepening and accentuating social divides by portraying social groups as homogeneous and categorically different, essentialist thinking is associated with greater endorsement of social stereotypes (Bastian & Haslam, 2006). Genetic and neurobiological causes are particularly apt to be seen as essence-like (Dar-Nimrod & Heine, 2011; Haslam, 2011): unmalleable, invisible, deterministic, and central to personhood.
Ideas of “genetic essentialism” and “neuro-essentialism” can help account for the dark side of our mixed-blessings model—namely, the links between biogenetic explanations and greater stigma. First, these explanations promote a desire for social distance from people with mental disorders because they portray them as categorically different: possessors of the pathological essence. Second, by triggering essentialist thinking, biogenetic explanations promote the view that mental disorders are not malleable, encouraging prognostic pessimism. Third, because essentialist thinking is associated with the endorsement of social stereotypes, biogenetic explanations are associated with acceptance of the widespread stereotype that people with mental disorders are unpredictable and dangerous. Attributions of uncontrollability might also promote this perception. In sum, the mixed-blessings model asserts that biogenetic explanations have positive as well as negative effects on stigma. They do so because they engender two distinct ways of thinking with markedly different attitudinal consequences.
Biogenetic Explanations Among Patients
Laypeople’s explanations of mental disorder clearly influence their views about affected people, but these explanations may also influence affected people’s views of themselves. Biogenetic explanations might have more favorable implications in this context, allowing affected people to see their condition as a disease like any other rather than as a blot on their character.
Regrettably, the research evidence fails to support this hopeful possibility (see Lebowitz, 2014, for a review). People who hold biogenetic explanations for their psychological problems are more likely to be pessimistic about recovery and less likely to see value in psychological interventions. In a recent study, Kemp, Lickel, and Deacon (2014) gave a bogus cheek-swab test to a sample of depressed participants, informing half that their condition was caused by a serotonin deficiency and telling the other half that their serotonin levels were in the normal range. Participants in the chemical-imbalance condition were less optimistic about their eventual recovery, less confident in their ability to regulate their negative moods, and more positively disposed to medication over psychological treatment. In a related vein, Dar-Nimrod, Zuckerman, and Duberstein (2012) found that leading healthy participants to believe that they had a genetic susceptibility for alcoholism engendered reductions in their perceived control over their drinking. Research on other behavioral phenomena (e.g., obesity, math performance, criminal culpability) has yielded similar findings.
Once again, this pattern of findings is consistent with the view that neurobiological explanations lead affected persons to “essentialize” their troubles as fixed organic pathologies over which they have limited control. This view encourages a passive approach to treatment, which must target the brain directly and be administered by someone else: the deferred-to biomedical “essence expert.”
Biogenetic Explanations Among Clinicians
Biogenetic explanations have some troubling implications for public stigma and for the private self-perceptions of people experiencing mental disorders. Do they also bear on how mental health professionals perceive affected people? There has been almost no research on this possibility, but a recent article revealed that biogenetic explanations may be problematic in this context as well, with potentially significant consequences for the therapeutic relationship.
In three studies, Lebowitz and Ahn (2014) presented American mental health clinicians—psychiatrists, psychologists, and social workers—with vignettes describing individuals with an assortment of conditions. Holding the basic description of each case constant, these conditions were presented as either psychosocially or biogenetically caused. For example, for a social-phobia vignette, the psychosocial version invoked bullying, negligent parents, and the patient’s failure to learn to trust others, whereas the biogenetic version invoked low serotonin levels, abnormally active amygdales, and a hereditary component. After reading each vignette, the clinicians reported their levels of empathy toward the fictitious patient using a standard questionnaire.
In every study, clinicians reported consistently less empathy for patients when their problems were explained biogenetically rather than psychosocially. Empathy was also consistently lower among clinicians with biomedical training (i.e., psychiatrists). Further, clinicians judged treatments that aligned with the explanation provided to be more effective, perceiving medication as better when conditions were explained biogenetically and psychotherapy as better when they were explained psychosocially. Lebowitz and Ahn (2014) argued that biogenetic explanations promote a mechanistic way of thinking that leads clinicians to overlook empirically supported psychological interventions and that may impede clinical compassion, a linchpin of the therapeutic relationship. That crucial relationship may be eroded from both sides, because just as biogenetically oriented clinicians may less empathic toward their clients, people may also be inclined to perceive them as lacking warmth (Lebowitz, Ahn, & Oltman, in press).
What Can Be Done?
Biogenetic explanations of psychopathology are increasingly popular within the mental health professions and are shaping laypeople’s “folk psychiatry” (Haslam, 2005). Although these developments represent scientific progress and popular enlightenment to some degree, the research evidence shows that they also have a dark side. How should we respond to these side effects of medicalization?
One thing we cannot do is turn our back on biogenetic approaches to psychopathology. However much their findings may be overhyped (Racine et al., 2010), these approaches enable genuine advances in understanding etiology, diagnosis, and treatment. To repudiate such advances because they promote some forms of stigma among laypeople would be to throw a rather large baby out with its bathwater. Indeed, some of the troubling implications of biogenetic explanation may reflect the public’s misunderstandings. Experts appreciate that neurobiological and genetic etiologies are not essence-like and deterministic but simply parts of a complex and malleable web of processes that interact reciprocally with experience and the social environment.
Combating essentialist misunderstandings of neuroscience and psychiatric genetics may therefore be a way to decouple biogenetic explanation and stigma. Lebowitz, Ahn, and Nolen-Hoeksema (2013), for example, demonstrated that depressed people who endorsed biogenetic explanations for their problems were more hopeless and less confident in their ability to improve their condition. However, their prognostic pessimism and passivity were reduced when they were shown a short video that explained the malleability of genetic and biochemical effects and the epigenetic interaction of biological and experiential factors in depression. Psychoeducation of patients and the lay public might therefore reduce the damaging effects of biogenetic explanation on stigma, although the strong tendency for people to interpret genetic and neural phenomena in an essentialist fashion—as fixed, hidden essences—implies that such education will have to swim against a cognitive tide.
However, it is unlikely that all of the ill effects of biogenetic explanation can be reversed simply by educating laypeople about bioscience, or that the fundamental problem is their ignorance of neuroplasticity and epigenesis. One reason to doubt this view is that experts themselves are liable to respond poorly to biogenetic explanations. As Lebowitz and Ahn (2014) showed, expert clinicians who have undergone extensive scientific training report less empathy when a fictitious patient’s symptoms are explained biogenetically, a response likely to weaken the therapeutic relationship. Mental health professionals may hold complex, “biopsychosocial” explicit theories of mental disorder, but they continue to apply starkly dualistic views to patients and their disorders (Ahn, Proctor, & Flanagan, 2009; Miresco & Kirmayer, 2006), distinguishing psychosocial (mind) and biogenetic (brain) factors and evaluating diagnosis, prognosis, and treatment in correspondingly polarized ways. If even expert clinicians fail to employ causal models that give both psychosocial and biogenetic factors their due when thinking about individuals, the problems of biogenetic explanation cannot be ascribed to laypeople’s ignorance alone.
Conclusions
Overcoming the now well-established problems of biogenetic explanations for mental disorder is an important challenge. These increasingly dominant explanations have some troubling implications for people experiencing psychological problems: for how they view their conditions, how members of the public view them, and how clinicians treat them. The first step toward counteracting these implications is to be mindful of them. Neuroscience and genetic researchers need to be aware that their findings may be misinterpreted as evidence of embodied defectiveness, clinicians to be aware that patients must not be reduced to broken mechanisms, and patients to be aware that their agency and optimism are not dissolved if their problems have a biological dimension.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to their authorship or the publication of this article.
Funding
The work presented in this article was supported by Australian Research Council Discovery Project DP140104527 to Ilan Dar-Nimrod and Nick Haslam.