
Abstract
We describe an approach to anxiety, depressive, trauma-related, and other disorders, which we conceptualize as “emotional disorders” because of shared underlying dimensions uncovered by the study of traits or temperaments. We then explicate a functional model of emotional disorders based largely, but not exclusively, on the temperament of neuroticism and describe common factors that account for the development and maintenance of these conditions. We conclude by describing, and presenting supporting data for, a unified transdiagnostic approach to the treatment of emotional disorders that directly targets the underlying temperament of neuroticism and associated temperamental characteristics.
Several years ago a prominent CEO of a national corporation traveled to our clinic, reporting that she had lost her ability to speak in corporate meetings and that, because this was absolutely essential to her position, her career was on the line. She recounted a meeting in which she had become furious at several participants who seemed to be conspiring against her. She was concerned that she would publicly explode in an unacceptable display of rage, and her anger quickly transformed into a full-blown panic attack, which rendered her unable to speak. After that experience, she stopped attending meetings out of fear of experiencing another panic attack if required to speak, but was running out of excuses. She noted that she typically excelled at running meetings and had been medically screened, so she knew that her inability to perform was a result of anxiety and that there would be no harm in returning to running meetings. In fact, it was the only rational thing to do. But she did not do it, playing out the age-old internal battle between reason and emotion in which, in the case of emotional disorders, emotion always wins.
Why would a sensible individual, weighing and balancing the consequences, engage in behavior that is at the same time self-defeating and self-perpetuating? More than 70 years ago, Mowrer (1950) called this puzzle the “neurotic paradox” and noted that it was the “absolutely central problem in neurosis and therapy” (p. 486; see Barlow, 2016).
Around that time, Eysenck (1947), in a prescient bit of theorizing, began considering higher-order temperamental factors as significant in the development of nonpsychotic mental disorders. In particular, he focused on what he considered to be a biologically based dimension of cortical activation and autonomic reactivity associated with the experience of frequent and intense negative emotions—a dimension that he called “neuroticism” (which he distinguished from neuroses). Utilizing an early version of a stress-diathesis model, he presumed that this temperament or trait interacted with stressful life events to produce psychological disorders. Since then, the study of personality traits and temperament has been prominent in psychology, and neuroticism has occupied a central role in the most well-known models of both personality and temperament, such as the Big 3 and the Big 5 (Clark & Watson, 2008).
The revolutionary taxonomy of mental disorders presented in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III; American Psychiatric Association, 1980) occasioned the death of “neurosis,” with its heavy theoretical baggage focused on etiology, as a construct (Barlow, 1982). But it became increasingly clear that the discrete diagnostic categories in the DSM—such as anxiety, depressive, trauma-related, and dissociative disorders, which can be grouped under the heading of emotional disorders (Bullis et al., 2019)—may describe minor variations of a broader underlying syndrome (Brown & Barlow, 2009). Over the decades, several investigators suggested that neuroticism or similar constructs, in combination with additional temperamental variables, most likely represent this syndrome (Achenbach, 2020; Barlow, 1988; Lahey, 2009; Tyrer, 1989). Indeed, newer quantitative models of psychopathology underscore higher-order domains common to the emotional disorders (see Lahey et al., 2021). Notable among these efforts is the Hierarchical Taxonomy of Psychopathology (HiTOP), which models the frequent co-occurrence (comorbidity) of these disorders (Kotov et al., 2021).
Finally, recent important evidence from research conducted at Northwestern University and UCLA has underscored the centrality of neuroticism and deficits in positive affect (extraversion) as underlying dimensional risk factors for the development of emotional disorders (e.g., Williams et al., 2021). Reviewing a number of streams of evidence, Cuijpers et al. (2010) noted the strong association between neuroticism and many different mental and physical disorders, along with the enormous economic cost associated with this trait, and advocated for the development of interventions focusing directly on neuroticism itself rather than its derivative outcomes (i.e., specific disorders).
Neuroticism and Emotional Disorders: A Functional Model
At the core of neuroticism is the experience of intense and frequent negative emotionality accompanied by a sense of uncontrollability and unpredictability of stressful or challenging events. This sense of limited control can be described as an unhelpful belief about one’s own self-efficacy to tolerate or influence personally salient events and outcomes. This belief drives an aversion or negative reaction to such anticipated events, including the emotional experiences themselves; this aversion can be considered an integral component of neuroticism (Barlow, 1988, 2002; Lilienfeld et al., 1993). In turn, this negative reactivity to intense emotions contributes to the development and maintenance of pathology characterized in large part by avoidant coping (Barlow, 1988; Bullis et al., 2019). Avoidant-coping strategies, which can manifest themselves at the level of cognition or behavior, provide relief from uncomfortable emotion in the short term, thereby creating a false sense of control or certainty, but, paradoxically, they result in a subsequent increase in the intensity and frequency of negative emotions (e.g., Wegner et al., 1987). Overreliance on these strategies also narrows one’s behavioral repertoire for responding to naturally occurring negative emotions, ultimately preventing disconfirmation of the negative beliefs that maintain the pattern. Indeed, it is this aversive reactivity to emotional experiences and resultant emotion-motivated avoidant coping that form the bridge from neuroticism to the emotional disorders and that are, in our view, the transdiagnostic functional mechanism fundamental to all disorders of emotion (Sauer-Zavala & Barlow, in press).
Constructs reflecting aversive reactivity to emotional experience
During the past 20 years, the identification of constructs that are found across the emotional disorders and that function to regulate intense emotion has greatly expanded. These constructs include those that reflect aversive reactivity to emotional experiences, such as anxiety sensitivity (aversion to physical manifestations of intense anxiety), experiential avoidance (aversion to and avoidance of internal thoughts and feelings; a construct that also contains avoidant-coping components), intolerance of uncertainty, and distress intolerance. Although similar, most of these constructs were originally considered, and continue to be conceived as, only narrowly associated with one DSM disorder or another. For example, anxiety sensitivity was (and still is) thought to be primarily a risk factor for panic disorder (e.g., Reiss & McNally, 1985), and intolerance of uncertainty was thought to be closely related to the onset of generalized anxiety disorder (Dugas et al., 1998).
Naragon-Gainey and Watson (2018), highly respected theorists in the area of temperament, affect, and emotional disorders, described a subset of constructs—specifically, anxiety sensitivity, intolerance of uncertainty, perfectionism, and experiential avoidance—as “social-cognitive vulnerabilities” (p. 143; in another publication, they used the term “affect-laden clinical traits”—Naragon-Gainey et al., 2018, p. 1177). They then went on to review a substantial body of literature demonstrating that these four vulnerabilities were all primarily associated with neuroticism more generally, but that at least some of them accounted for a small amount of additional variance in some, but not all, emotional disorders, and that these traits are more proximal and convenient targets for treatment. Similarly, specific types of negative emotions, such as sadness or depression, fear, anxiety, and anger or hostility, are often considered facets of neuroticism, and examining these constructs individually sometimes leads to modest gains in predictive power (Naragon-Gainey & Watson, 2018).
But the distinction between these vulnerabilities mirrors the “splitting versus lumping” controversy that has so permeated classification of mental disorders; that is, there is often an initial tendency to associate one construct or “clinical trait” with one emotional disorder, although additional analysis reveals not only more general transdiagnostic characteristics, but also that these dimensional traits are, for the most part, integral parts of neuroticism itself. Our own view is that any incremental validity conferred by individual social-cognitive traits in predicting aspects of specific disorders may be an artifact of initially constructing assessments of these traits to ascertain specific vulnerabilities for specific disorders. Of course, as suggested by Naragon-Gainey et al. (2018), this does not reduce their utility. Indeed, a number of these clinical traits are useful in assessing outcomes of transdiagnostic interventions for emotional disorders (Barlow, Farchione, Sauer-Zavala, et al., 2017).
Emotion-motivated avoidant coping
The primary mechanism that maintains emotional disorders, as well as neuroticism itself, over time is emotion-motivated avoidant coping, which refers to patterns of maladaptive behavioral and cognitive strategies used to avoid, dampen, or suppress negative affect (Sauer-Zavala & Barlow, in press; see Table 1). Often, such coping is manifest behaviorally as overt avoidance, such as refusing to enter a situation that elicits a negative emotion (e.g., not attending a gathering with unfamiliar people in the case of a person with social anxiety disorder). Avoidance can also be more subtle, such as averting one’s gaze or mapping out an exit strategy beforehand to facilitate escape if anxiety arises.
Some Examples of Emotion-Motivated Avoidant-Coping Strategies
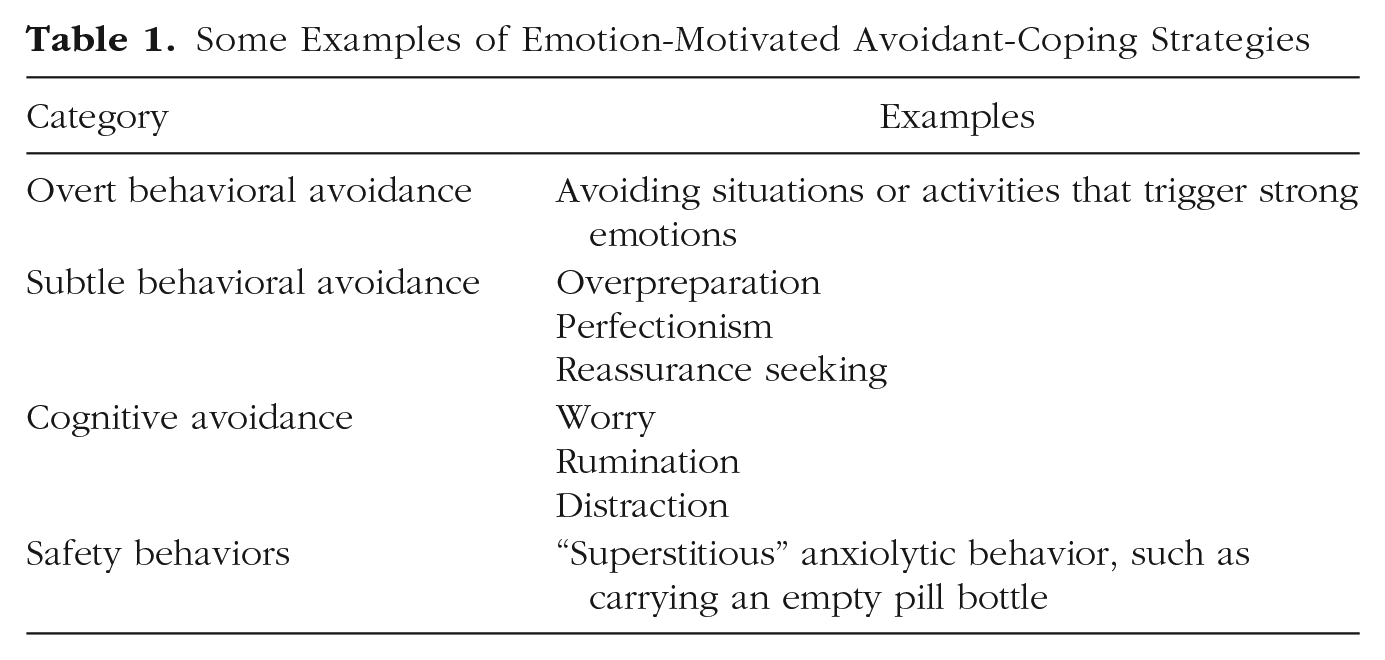
Avoidant coping can also manifest itself in cognitive strategies that are meant to reduce experiences of aversive emotional states. At the information-processing level, individuals with emotional disorders display an initial attentional bias toward negative stimuli, as a means of detecting threat, that is followed by a shift of attention away from these stimuli, as a means of avoidance (Mathews & MacLeod, 2005). Furthermore, repetitive negative thinking (i.e., difficult-to-control cognitive activity such as worry and rumination) serves to protect an individual from experiencing affective states that are perceived as especially distressing or unacceptable, particularly those relating to the themes of control, certainty, and predictability. For example, an anxious individual may worry excessively about future situations in a misguided attempt to make certain what is uncertain. Despite having initially been associated with generalized anxiety disorder and depression, repetitive negative thinking is ubiquitous across the emotional disorders (Ehring & Watkins, 2008).
From neuroticism to specific disorders
Emotion-motivated avoidant coping is highly individual and varies with the foci and triggers of the emotions to be avoided (e.g., intrusive, or obsessive, thoughts; physiological sensations associated with panic attacks; biased social comparisons associated with depression). We have used our functional model, outlined in Figure 1, to suggest specific pathways from neuroticism to disorders that would account for the clear phenotypic differences across the discrete DSM diagnoses, as more fully described in the “triple vulnerabilities” model of the etiology of neuroticism and emotional disorders (see Barlow et al., 2014; Sauer-Zavala & Barlow, in press). Specifically, early experiences may later evolve into specific disorders through learning processes (e.g., classical conditioning, observational learning) that link emotional reactions to specific foci or triggers referred to in the DSM diagnostic criteria (Barlow et al., 2014).
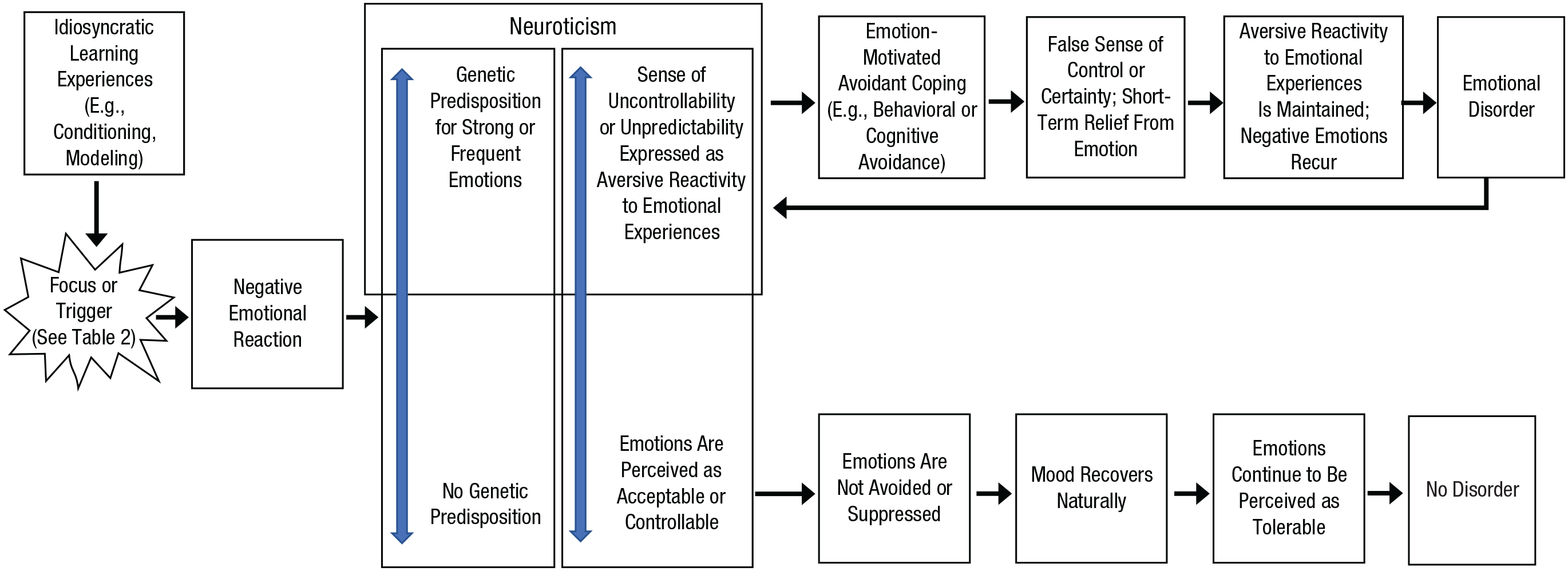
Model of the functional mechanisms in the development of emotional disorders versus normal emotional experience (adapted from Sauer-Zavala & Barlow, in press). Emotional triggers lead to negative emotional reactions in most people; however, the consequences of these negative emotional reactions differ depending on the individual’s level of neuroticism. The top pathway describes how individuals with a more neurotic temperament, who have also developed a sensitivity to certain triggers through learning experiences early in life, tend to engage in a set of processes that culminate in the development and maintenance of emotional disorders. In contrast, the bottom pathway depicts the cascade of adaptive responses to negative emotions that characterizes healthy emotional functioning in individuals lower in neuroticism.
What is important is that most triggers and foci, such as panic attacks or trauma, are commonly experienced in the population but in most cases do not lead to an emotional disorder (see Table 2). For example, the unwanted intrusive thoughts that characterize obsessive-compulsive disorder, including bizarre ego-dystonic thoughts such as thoughts about harming one’s family, occur in up to 80% of the general population when under stress (Barlow, 2002; Rachman & de Silva, 1978; Sauer-Zavala & Barlow, in press). For the vast majority of the population, these thoughts are unsettling and may provoke some emotion but are quickly dismissed. Similarly, up to one third of the population experience panic attacks when under stress, but just a small fraction of those individuals (1%–2%) go on to develop panic disorder (Craske & Barlow, in press). Many people experience the sudden and unexpected death of a loved one, but only a few subsequently develop prolonged grief disorder, and many people who experience occasional insufficient sexual arousal or erectile failure or restless unsatisfying sleep do not go on to develop sexual dysfunction or insomnia disorder. The differentiating factor seems to be the presence of a neurotic temperament along with early learning experiences that predispose sensitivity to some emotional triggers but not others (Barlow et al., 2014; Sauer-Zavala & Barlow, in press). For example, individuals with panic disorder report that during childhood, they were “sensitized” by caregivers to the dangers of unexplained physical sensations such as rapid heart rate, and individuals with obsessive-compulsive disorder report learning that intrusive, unwanted thoughts (e.g., sexual or violent thoughts) are as blameworthy as actually engaging in those actions (thought-action fusion).
Precipitating Events (Triggers) for Negative Emotions and Possible Emotional Disorder (Adapted From Sauer-Zavala & Barlow, in press)
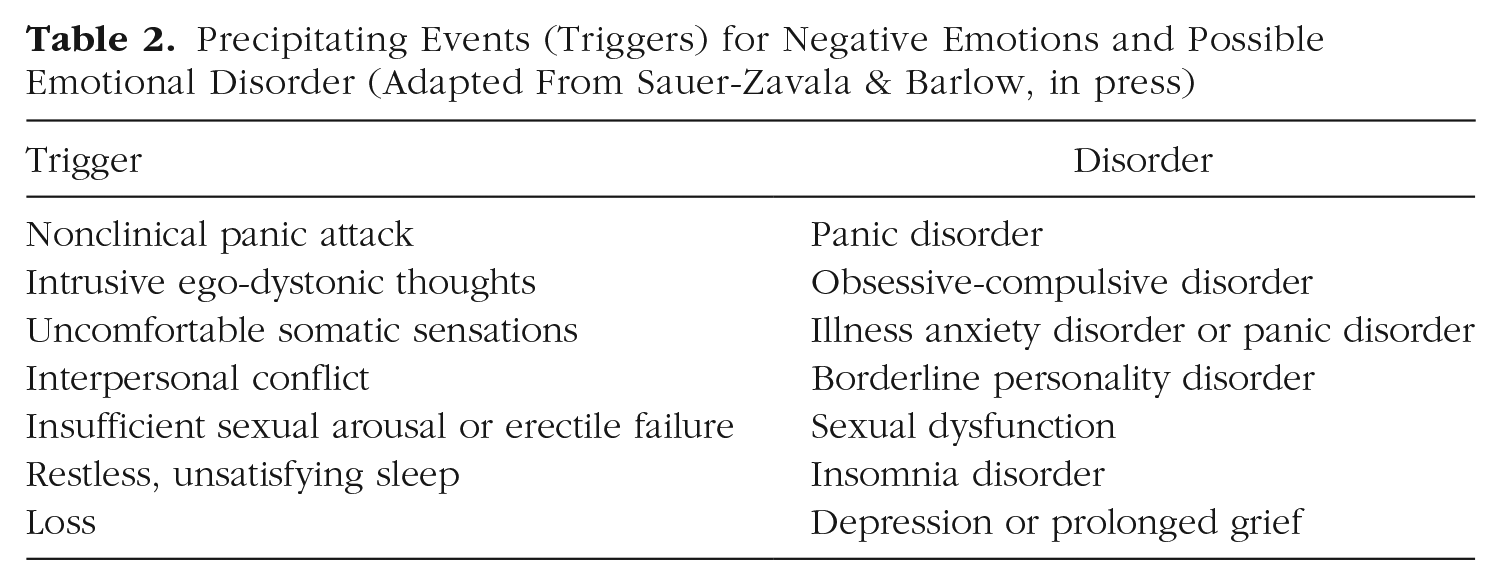
Although the DSM diagnostic criteria for many emotional disorders are largely based on specific foci or triggers, it is our view that these triggers (panic attacks, obsessions) are relatively trivial (in the scientific sense) contextual differences, and that the core functional model we have outlined in Figure 1 offers a more heuristic framework for understanding, and ultimately treating, emotional disorders.
Transdiagnostic treatment of emotional disorders
Given the potential benefits of addressing underlying temperamental features as opposed to disorder-specific symptoms, our research group sought to develop a unified, transdiagnostic approach to treating emotional disorders (Barlow et al., 2004). Drawn from our functional model of neuroticism, the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders (UP; Barlow, Farchione, Sauer-Zavala, et al., 2017) comprises a series of treatment modules intended to alter the functional pathway between neuroticism and psychopathology. Four of the five core modules focus on psychoeducation on the functional and adaptive nature of emotion (to counter attributions that emotions are dangerous), emotional-awareness exercises (to begin the process of countering avoidance of emotional experience), cognitive flexibility (to provide alternatives to negative and dangerous attributions and appraisals reflecting aversive reactivity to emotional experiences), and modification of emotion-driven behaviors that serve to reduce or eliminate aversive emotions (e.g., fight or flight driven by fear or withdrawal driven by depression). The fifth and most central module consists of exposure to intense emotional experiences, particularly interoceptive (somatic) components of emotions, to facilitate inhibitory learning and extinction of anxiety and distress associated with intense emotional experience. Thus, these modules target both aversive reactivity to emotional experiences and emotion-motivated avoidant coping in order to normalize emotional experience. This approach differs from a majority of evidence-based treatments that target symptoms and triggers of single DSM disorders, as opposed to addressing underlying temperamental constructs.
Since the publication of the UP’s first edition in 2011 (Barlow et al., 2011), research has consistently demonstrated that this approach is effective at treating a wide range of emotional disorders. Initial findings were supported in a large randomized controlled trial demonstrating that the UP is as effective as four well-established single-disorder cognitive behavior therapy protocols (SDPs) in treating patients with primary anxiety disorders. At the end of treatment, similar percentages of patients no longer met criteria for their primary diagnosis (UP condition: 63.6%; SDP conditions: 57.1%; Barlow, Farchione, Bullis, et al., 2017). These results were sustained at a 12-month follow-up (Eustis et al., 2020). Furthermore, these results were consistent across diagnoses, which suggests that the UP addresses underlying transdiagnostic processes as opposed to symptoms associated with specific disorders.
Given that our functional model implicates neuroticism and associated aversive emotional reactivity as key processes in the maintenance of emotional disorders, our research group has sought to identify the UP’s impact on these processes. In an early trial, the UP was associated with reduction in two kinds of aversive reactivity to emotional experiences (i.e., anxiety focused on emotions and anxiety sensitivity), both of which were correlated with reductions in symptoms even after controlling for the frequency of negative emotions (Sauer-Zavala et al., 2012). More recently, a secondary analysis of the randomized controlled trial mentioned earlier (Barlow, Farchione, Bullis, et al., 2017) showed that the UP was associated with greater decreases in neuroticism than symptom-focused SDPs (Sauer-Zavala et al., 2020). Taken together, these studies support the hypothesis that both neuroticism and aversive reactivity to emotional experiences are important in the expression of emotional-disorder symptoms, and they suggest that the UP may work through targeting these key features. Because of its evident effectiveness at reducing neuroticism, the UP has now been applied to a range of emotional disorders, with positive results. These include posttraumatic stress disorder, borderline personality disorder, eating disorders, insomnia, depression, dissociative identity disorder, bipolar disorder with comorbid anxiety, nonsuicidal self-injury, affective components of substance use disorders, chronic pain, irritable bowel syndrome, and anxiety and depression associated with Parkinson’s disease (see Cassiello-Robbins et al., 2020).
Conclusion
The study of temperament and personality, on the one hand, and the study of the psychopathology of emotional disorders, on the other hand, were largely unrelated to each other during the last decades of the 20th century, but they now seem to be inextricably interrelated. Indeed, at the core of disorders of emotion are relatively stable patterns of temperament—particularly, but not limited to, neuroticism—and associated aversive reactions to emotional experiences that form the functional pathway between temperament and psychopathology. Advances in understanding of emotional disorders should benefit from a deeper focus on these temperamental contributions.
Recommended Reading
Barlow, D. H., Ellard, K. K., Sauer-Zavala, S., Bullis, J. R., & Carl, J. R. (2014). (See References). Describes a theory of the development of neuroticism that integrates genetic, neurobiological, and environmental factors related to the trait.
Barlow, D. H., Farchione, T. J., Bullis, J. R., Gallagher, M. W., Murray-Latin, H., Sauer-Zavala, S., Bentley, K. H., Thompson-Hollands, J., Conklin, L. R., Boswell, J. F., Ametaj, A., Carl, J. R., Boettcher, H. T., & Cassiello-Robbins, C. (2017). (See References). Presents results from the largest randomized controlled trial on the Unified Protocol to date.
Cassiello-Robbins, C., Southward, M. W., Tirpak, J. W., & Sauer-Zavala, S. (2020). (See References). Comprehensively reviews the existing literature on applications of the Unified Protocol to treat a range of emotional disorders in adult populations.
Sauer-Zavala, S., & Barlow, D. H. (in press). (See References). Presents a detailed and comprehensive exploration of neuroticism, including factors that contribute to its development, maintenance, and treatment.
Sauer-Zavala, S., Gutner, C. A., Farchione, T. J., Boettcher, H. T., Bullis, J. R., & Barlow, D. H. (2017). Current definitions of “transdiagnostic” in treatment development: A search for consensus. Behavior Therapy, 48(1), 128–138. https://doi.org/10.1016/j.beth.2016.09.004. Examines the term “transdiagnostic” within the treatment-development literature.