
Abstract
In this article, we argue that stigma may be an important, but heretofore underrecognized, source of heterogeneity in treatment effects of mental- and behavioral-health interventions. To support this hypothesis, we review recent evidence from randomized controlled trials and spatial meta-analyses suggesting that stigma may predict not only who responds more favorably to these health interventions (i.e., individuals with more stigma experiences), but also the social contexts that are more likely to undermine intervention effects (i.e., communities with greater structural stigma). By highlighting the potential role of personal and contextual stigma in shaping response to interventions, our review paves the way for additional research.
Keywords
Stigma—defined as the co-occurrence of labeling, stereotyping, status loss, and discrimination in a context where power is exercised (Link & Phelan, 2001)—is conceptualized as a fundamental cause of population health inequalities because of its pervasiveness, its disruption of multiple life domains, and its corrosive impact on determinants of health (Hatzenbuehler et al., 2013). Stigma contributes to health inequalities not only by impeding access to socioeconomic resources (e.g., education) that are necessary for health, but also by initiating a cascade of psychological (e.g., self-regulation), behavioral (e.g., concealment), and biological (e.g., inflammation) responses that undermine health (Hatzenbuehler et al., 2013; Major et al., 2013). Given the myriad ways in which stigma affects health, it seems reasonable to consider whether stigma may also shape how stigmatized individuals respond to mental- and behavioral-health interventions.
The primary way in which psychologists and other mental-health professionals have sought to answer this question is by conducting meta-analyses that examine whether treatment efficacy is moderated by group characteristics that correlate with exposure to stigma, such as minority race or ethnicity (e.g., Weisz et al., 2017) and minority gender identity (e.g., Hollinsaid et al., 2020). With rare exceptions, these studies have generally failed to find reliable between-groups differences in intervention efficacy, suggesting that stigma may not influence how individuals respond to these health interventions. Yet this approach may obscure the role of stigma in shaping response to interventions for at least two reasons.
First, because the individual studies included in these meta-analyses do not typically focus on stigmatized populations, exposure to stigma is inferred on the basis of group membership rather than explicitly measured, despite evidence of substantial within-group variation in stigma experiences (Major & O’Brien, 2005). Thus, individuals with differing types and levels of stigma experiences are pooled together; if these experiences are differentially associated with intervention efficacy, as they are with health outcomes (e.g., Major et al., 2013), this approach can lead to spurious inferences about who benefits from health interventions.
Second, these meta-analytic studies have typically been conducted without attending to the social contexts in which health interventions are delivered, despite evidence that contextual factors, including structural forms of stigma and discrimination (e.g., Hatzenbuehler, 2016; Williams & Collins, 2001), affect mental- and behavioral-health outcomes. Consequently, just as pooling individuals with diverse stigma experiences may obscure subgroup differences in intervention outcomes, so too can combining studies conducted in social contexts with differing levels of stigma.
Emerging evidence suggests that this predominant approach (i.e., comparing intervention effects between stigmatized and nonstigmatized groups) has, in fact, limited understanding of whether and how stigma moderates intervention responses. Drawing on recent methodological advances in measuring stigma and in studying its impact on intervention efficacy, we review new research suggesting that stigma may predict not only which individuals derive more benefit from mental- and behavioral-health interventions, but also the social contexts in which these interventions are more likely to flourish or fail.
Before we review this research, it is important to emphasize two points about the arguments we are advancing. Although we present recent evidence that individual and contextual sources of stigma may moderate intervention efficacy, we do not expect that stigma shapes intervention responses in all instances. In fact, as with other candidate moderators, it is necessary to identify for whom, for which treatments, and for which outcomes stigma moderates intervention effects. This information will enable researchers to ascertain boundary conditions—that is, to identify when stigma does (and does not) moderate the efficacy of health interventions. We return to this point in our discussion of future directions.
Additionally, by highlighting stigma as a potential moderator of response to treatment, we are not arguing that stigma is the only important moderator. Indeed, researchers have identified numerous other factors that may shape response to treatment in marginalized groups, such as level of acculturation (Lau, 2006). Yet, given the centrality of stigma as a source of stress for minority groups (Major & O’Brien, 2005), and the fact that stigma has motivated the adaptation of several mental- and behavioral-health treatments (e.g., Pachankis, 2018), it is striking that the field of intervention science has rarely examined stigmatizing experiences or stigmatizing contexts as predictors of treatment efficacy. We now turn to the literature that has begun to address this knowledge gap.
For Whom Does Stigma Modify the Efficacy of Mental- and Behavioral-Health Interventions?
Psychologists and other mental-health professionals have been at the forefront of recent efforts to reduce stigma-related health burdens by developing mental- and behavioral-health interventions that are adapted to address stigma related to race (e.g., Anderson et al., 2018), ethnicity (e.g., Graham-LoPresti et al., 2017), gender identity (Budge et al., 2021), and sexual orientation (e.g., Pachankis, 2014). These adapted interventions are designed to improve mental- and behavioral-health outcomes among members of stigmatized groups by targeting specific mechanisms through which stigma shapes adverse outcomes. Examples of such stigma-related mechanisms include self-stigma (i.e., the extent to which individuals incorporate negative societal views into their self-concept; Lucksted et al., 2011), concealment (e.g., Pachankis, 2007), social identity threat (e.g., Major & O’Brien, 2005), and social isolation (e.g., Hatzenbuehler, 2009). In this section, we discuss studies examining whether individual-level stigma experiences predict variation in how individuals respond to these interventions. We focus on studies using randomized controlled trials that compared adapted treatments with control conditions and that measured stigma experiences at baseline.
Psychologists have identified numerous manifestations of stigma that compromise mental and behavioral health, as well as several psychological pathways through which this occurs. For instance, stigma experiences, such as discrimination, can generate a variety of coping responses—including detaching from others (i.e., social isolation), hiding aspects of one’s identity (i.e., concealment), and developing anxious expectations that one will be rejected because of one’s identity (i.e., status-based rejection sensitivity)—and these responses can, in turn, compromise mental and behavioral health, especially when prolonged and inflexible to context (Hatzenbuehler, 2009; Major & O’Brien, 2005; Pachankis, 2007). Thus, individuals who enter treatment with high levels of stigma-related experiences are a group for whom stigma-related stress is most impairing and for whom targeted clinical attention may be necessary.
Three recent studies (Lee et al., 2019; Millar et al., 2016; Pachankis et al., 2020) have shown that it is precisely this group who respond most robustly to adapted treatments. In these studies, four types of evidence-based interventions for mental- and behavioral-health problems—cognitive behavior therapy, expressive writing, self-affirmation, and motivational interviewing—were adapted for use with sexual-minority and Latinx populations. This adaptation was accomplished through several approaches, including consulting with members of stigmatized communities to generate new intervention content that consistently addressed stigma-related stressors (e.g., skills for learning to identify and adaptively respond to stigma-related cognitions, such as self-stigma). Because the adaptation process led to a set of principles and techniques uniquely geared toward addressing the stigma-based mechanisms affecting the mental and behavioral health of stigmatized groups, the resulting treatments can be considered adapted and distinct from the general treatments upon which they are based.
Across these studies, higher levels of stigma experiences (i.e., discrimination, victimization, self-stigma)—measured both implicitly (i.e., sexuality implicit association test) and explicitly (i.e., via self-report)—correlated with greater benefit from these adapted treatments. These benefits included greater reductions in symptoms of depression, anxiety, and suicidality (Millar et al., 2016; Pachankis et al., 2020) and in alcohol-related consequences (Lee et al., 2019). The magnitude of these symptom reductions for individuals reporting more stigma experiences has been relatively large; for example, the effect size for reduction in symptoms of depression in the adapted self-affirmation intervention (Pachankis et al., 2020) was nearly 3 times as large as the effect size in the control condition for those individuals reporting high (i.e., 1 SD above the mean) sexual orientation-related discrimination at baseline. However, studies have shown that individuals with low levels of stigma experiences at baseline derive similar benefits from adapted and control conditions (Lee et al., 2019; Pachankis et al., 2020).
In What Social Contexts Does Stigma Modify the Efficacy of Mental- and Behavioral-Health Interventions?
Whereas this first set of studies examined the stigmatizing experiences that predict individuals’ responses to adapted health interventions, another set of studies has focused instead on features of stigmatizing environments that modify intervention efficacy. To study potential moderating effects of stigmatizing social contexts, researchers have objectively measured structural forms of stigma, defined as societal-level conditions, cultural norms, and institutional policies and practices that constrain the lives of the stigmatized (Hatzenbuehler & Link, 2014). Examples of contexts characterized by structural stigma include states with laws denying services to same-sex couples, countries with restrictive immigration policies, and communities where residents endorse high levels of racial prejudice.
Determining whether structural stigma modifies intervention efficacy presents several methodological challenges. Because communities differ in many respects other than structural stigma, researchers must first establish that structural stigma uniquely shapes health outcomes. Researchers have used several strategies for establishing strong inferences regarding the relationship between structural stigma and health (for reviews, see Hatzenbuehler, 2014, 2016, 2017). These strategies include (a) triangulating evidence across a range of measures, methods, groups, and outcomes; (b) documenting specificity of associations to stigmatized groups (and not to nonstigmatized comparison groups); (c) controlling for potential individual- and structural-level confounders; (d) conducting falsification tests to show that structural stigma does not predict outcomes it should not theoretically influence (e.g., fruit-juice consumption); and (e) ruling out plausible alternative explanations, such as healthier respondents moving to low-stigma communities. Given the robustness and consistency of this evidence base, researchers can more confidently examine structural stigma as a distinct moderator of the efficacy of health interventions.
Additionally, studying structural stigma as a moderator of intervention response requires sampling mental- and behavioral-health interventions across a range of social contexts (e.g., counties) that differ in the level of structural stigma. However, intervention studies are typically conducted in one community. Consequently, individuals are ubiquitously exposed to the same environment, which limits the variation necessary to detect associations between structural stigma and intervention efficacy. To overcome this challenge, researchers recently developed a novel method called spatial meta-analysis (Johnson et al., 2017). This approach retains many aspects of a traditional meta-analysis, with the added step that studies are geolocated, which allows researchers to characterize each included study in terms of the social context in which it was conducted. Spatial meta-analyses therefore leverage the contextual variability that naturally exists across studies to examine associations between contextual variables, such as structural stigma, and study outcomes, such as intervention efficacy.
Two spatial meta-analyses of behavioral-health intervention studies (i.e., HIV-prevention interventions: 99 effect sizes, Reid et al., 2014) and mental-health intervention studies (i.e., psychotherapies: 385 effect sizes, Price et al., 2021) have addressed whether structural stigma moderates intervention efficacy. The interventions in these studies were typically nonadapted; that is, they were general health interventions designed to reduce adverse mental- and behavioral-health outcomes among all respondents, irrespective of whether they had a stigmatized identity, condition, or status. Consequently, unlike the adapted treatments reviewed in the previous section, stigma-related mechanisms were not specifically targeted in these nonadapted treatments. In both meta-analyses, the efficacy of these nonadapted health interventions was evaluated against one or more control conditions.
Both spatial meta-analyses examined structural stigma related to race, which was measured by aggregating racial attitudes in the counties (Reid et al., 2014) and states (Price et al., 2021) where these interventions were conducted. (Reid et al., 2014, additionally measured racial residential segregation, which yielded similar results.) These studies produced three important findings. First, on average, the efficacy of HIV-prevention interventions (Fig. 1; Reid et al., 2014) and psychotherapies (Fig. 2, left panel; Price et al., 2021) among majority-Black samples was significantly weaker in high-structural-stigma environments than in low-structural-stigma environments. In fact, intervention effect sizes were between 3 (Price et al., 2021) and 4 (Reid et al., 2014) times as large in low- than in high-structural-stigma environments.
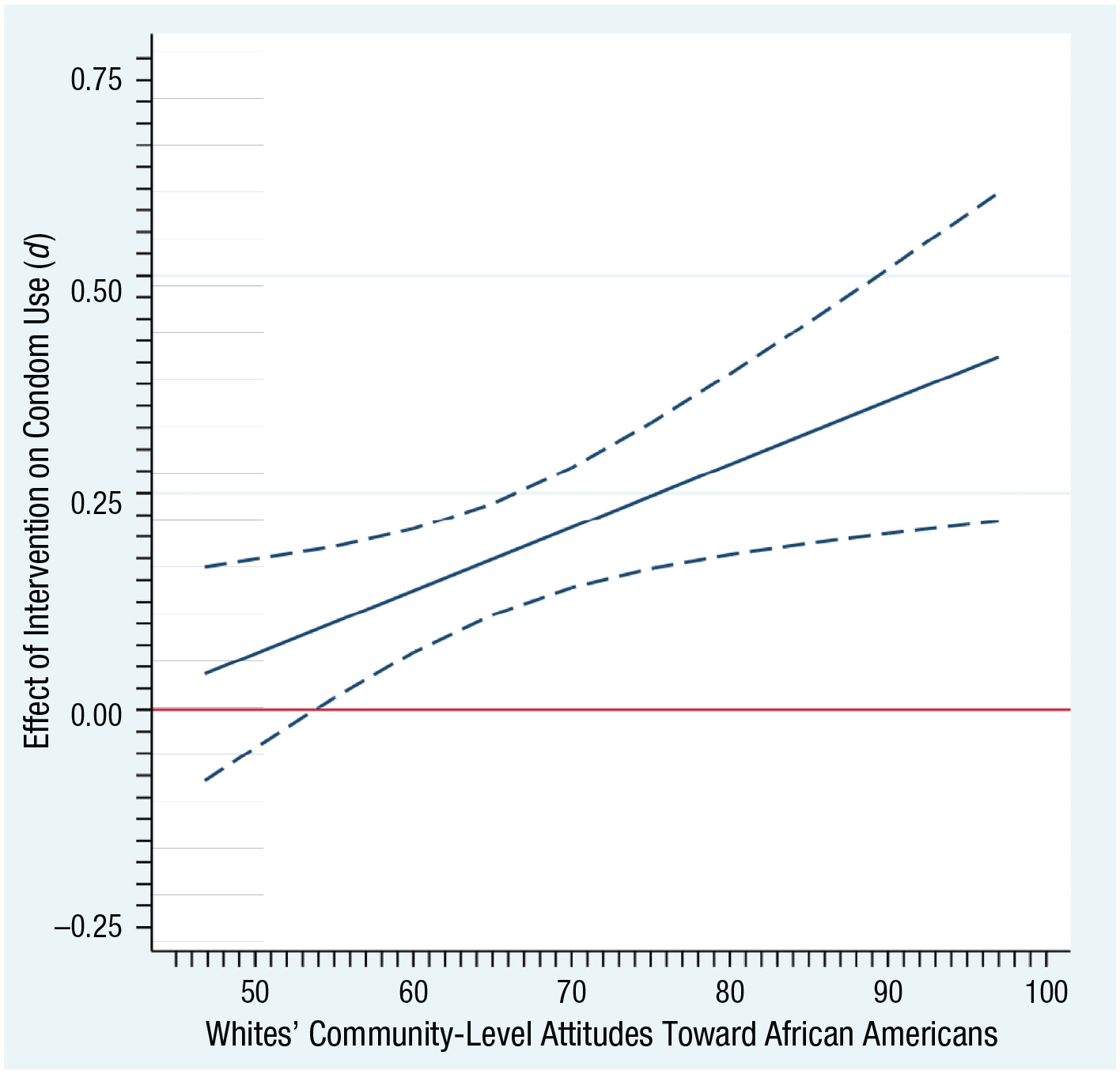
Results from Reid et al.’s (2014) spatial meta-analysis of the relationship between race-related structural stigma and the efficacy of HIV-prevention interventions among majority-Black samples: predicted estimates (with 95% confidence intervals) of the standardized mean difference (d) in condom use between the intervention and control groups as a function of Whites’ community-level attitudes toward African Americans. Positive values for condom use imply that the intervention groups were more likely to use condoms than the control groups. Higher scores for community-level attitudes indicate lower levels of racial prejudice. Adapted with permission from a figure presented by A. Reid at the Society of Behavioral Medicine 39th Annual Meeting, New Orleans, LA, April 11–14, 2018.
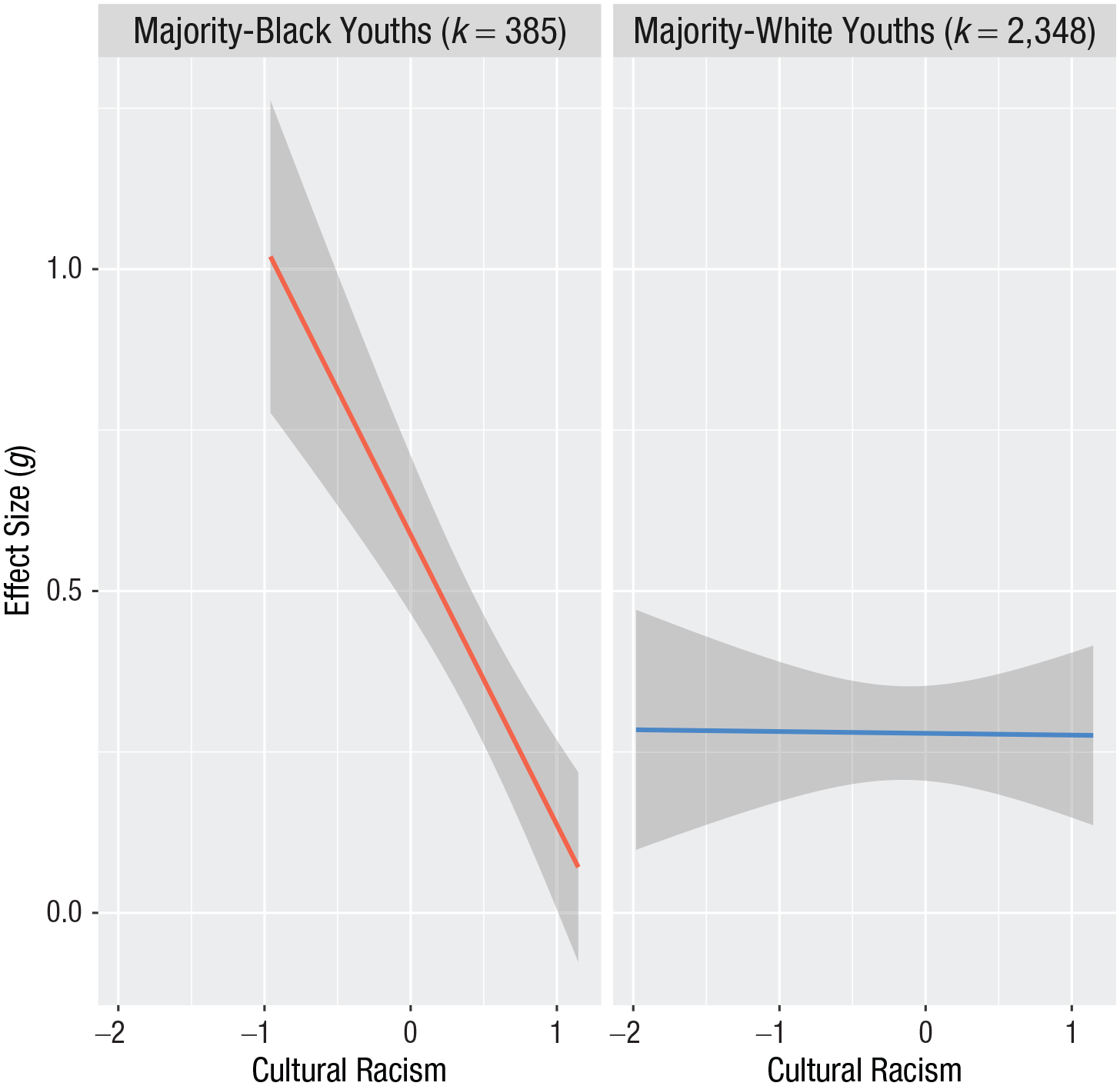
Results from Price et al.’s (2021) spatial meta-analysis of the relationship between race-related structural stigma and the efficacy of psychotherapy interventions among youth: effect size (Hedges’s g—the standardized mean difference between the intervention and control conditions) as a function of cultural racism, which was measured with a composite index of 31 items assessing explicit racial attitudes. These items were obtained from three different sources: the General Social Survey (e.g., “Are we spending too much, too little, or about the right amount on improving the conditions of Blacks?”), the American National Election Survey (e.g., “Irish, Italians, Jewish and many other minorities overcame prejudice and worked their way up. Blacks should do the same without any special favors.”), and Project Implicit (e.g., “I would rather not have Black people live in the same apartment building I live in.”). The racism data were aggregated to the state level; higher scores indicate higher levels of racism in the communities where the psychotherapy interventions were conducted. The gray shading represents 95% confidence intervals. The left-hand graph shows results for samples with more than 50% Black participants; the right-hand graph shows results for samples with more than 50% White participants. Adapted from “Are Psychotherapies Less Effective for Black Youth in Communities With Higher Levels of Anti-Black Racism?” by M. A. Price, J. R. Weisz, S. McKetta, N. L. Hollinsaid, M. R. Lattanner, A. E. Reid, and M. L. Hatzenbuehler, 2021, Journal of the American Academy of Child and Adolescent Psychiatry, advance online publication, Fig. 1 (https://doi.org/10.1016/j.jaac.2021.07.808). Copyright 2021 by the American Academy of Child and Adolescent Psychiatry.
Second, the study by Price and colleagues (2021) included a nonstigmatized comparison (i.e., majority-White samples). No association was observed between structural stigma and intervention efficacy in the nonstigmatized group (Fig. 2, right panel). The lack of an association among majority-White samples provides evidence of specificity and reduces concerns that the associations reflect other contextual factors that correlate with structural stigma (e.g., area-level conservatism).
Third, in both studies, there was an interaction between structural stigma and time since the intervention (see Fig. 3 for results from Price et al., 2021). Immediately after treatment, the effect sizes for the interventions relative to the control conditions differed little between high- and low-stigma communities. However, these effect sizes increased over time in low-stigma communities, which suggests that identity-affirming environments may facilitate the gains made during treatment. In contrast, in high-stigma communities, the intervention effect sizes decreased over time and became significantly different from the effect sizes observed in low-stigma communities, which suggests that any minimal initial benefits accrued from the interventions eroded in identity-threatening environments (Price et al., 2021; Reid et al., 2014). Although neither study identified specific mechanisms linking high structural stigma to reduced intervention efficacy, these divergent effects across time suggest that the search for potential mechanisms should include both psychological (e.g., identity threat; Major & O’Brien, 2005) and intergroup (e.g., mistrust; Major et al., 2013) factors that exist outside the intervention context.
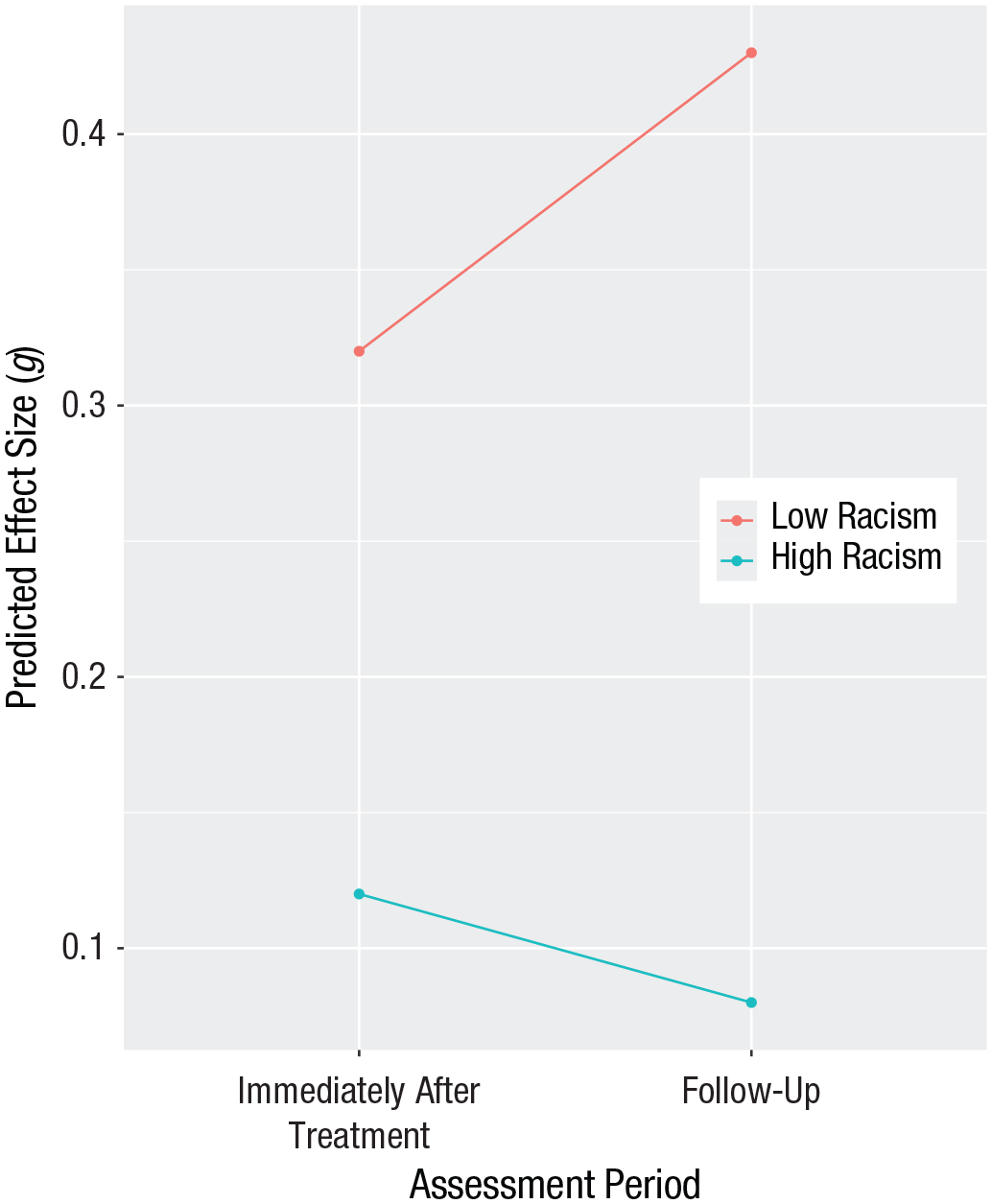
Results from Price et al.’s (2021) spatial meta-analysis examining the interaction between race-related structural stigma (high vs. low; see Fig. 2 for details) and time of postintervention assessment (immediate vs. follow-up) in predicting the efficacy of psychotherapy interventions among samples of majority-Black youth. Effect size was measured as Hedges’s g, the standardized mean difference between the intervention and control conditions. Adapted from “Are Psychotherapies Less Effective for Black Youth in Communities With Higher Levels of Anti-Black Racism?” by M. A. Price, J. R. Weisz, S. McKetta, N. L. Hollinsaid, M. R. Lattanner, A. E. Reid, and M. L. Hatzenbuehler, 2021, Journal of the American Academy of Child and Adolescent Psychiatry, advance online publication, Fig. 2 (https://doi.org/10.1016/j.jaac.2021.07.808). Copyright 2021 by the American Academy of Child and Adolescent Psychiatry.
Future Research
We end by discussing four research directions that are needed to advance this emerging literature on stigma and intervention efficacy: (a) identifying additional stigma-related moderators, stigmatized groups, and treatment-related outcomes; (b) uncovering mediating mechanisms linking stigma experiences to intervention efficacy; (c) evaluating more comprehensively whether, when, and how to effectively adapt stigma-based health interventions; and (d) expanding research methods.
Existing studies have focused on a limited range of stigma variables, including implicit self-stigma (e.g., Millar et al., 2016), perceived discrimination (e.g., Lee et al., 2019), and structural stigma (e.g., Price et al., 2021). Thus, there is a need to search for additional stigma-related moderators of treatment efficacy, which can inform the selection of individuals for whom particular health interventions may be most efficacious. For instance, individuals differ in how central their stigmatized identities are to their self-concept (Quinn & Chaudoir, 2009), which may shape how they respond to interventions designed to address stigma-related mechanisms. Further, existing research has focused on a limited number of stigmatized identities related to race, ethnicity, and sexuality; the extent to which the findings generalize to other stigmatized groups is an important area for future inquiry. Additionally, although our analysis focused on intervention efficacy, stigma experiences and environments may predict other intervention-related outcomes—such as engagement in, attrition from, and satisfaction with treatment—which should be explored in future studies. As noted at the outset, we do not expect all potential stigma processes to moderate each of these outcomes among every stigmatized group; as new evidence emerges, it will be possible to generate more precise theoretical predictions about whether and in what contexts these moderating effects are likely (and unlikely) to occur.
The studies we have reviewed suggest that stigma experiences are associated with the efficacy of adapted mental- and behavioral-health interventions. The assumption underlying these studies is that by specifically addressing stigma-related mechanisms through targeted interventions, health will improve, particularly among individuals reporting the highest levels of stigma. An alternative explanation for these findings is that individuals reporting more stigma at baseline experience greater intervention efficacy merely because they have higher levels of initial psychological distress, and thus greater room for improvement. The general literature is mixed regarding whether participants who report worse mental-health symptoms at baseline derive greater intervention benefits, and some studies have found that greater symptom severity actually predicts worse outcomes in psychotherapy interventions (e.g., Compton et al., 2014). Nevertheless, additional research is needed to rule out alternative explanations and to bolster the working hypothesis that stigma experiences per se shape intervention efficacy. One way to do so is to identify the mediating mechanisms underlying the associations between stigma experiences and intervention efficacy. For instance, support for a causal role of stigma would be enhanced if factors known to mediate the association between stigma and health outcomes—including stigma-specific mechanisms (e.g., concealment; Pachankis, 2007) and general psychosocial mechanisms (e.g., emotion-regulation deficits; Hatzenbuehler, 2009)—decreased as a result of adapted stigma-based interventions. Recent studies (e.g., Pachankis et al., 2015) have provided preliminary support that adapted stigma-based interventions can effectively target both sets of mechanisms, but more work is needed.
Our review uncovered an apparent incongruence: Whereas individuals with higher levels of stigma experiences benefited more from health interventions, individuals in high-stigma environments benefited less from health interventions compared with individuals in low-stigma environments. However, stigma experiences and environments are confounded by type of intervention in existing research—that is, studies that examined the association between stigmatizing experiences and intervention efficacy involved adapted interventions, whereas studies that examined the association between stigmatizing environments and intervention efficacy involved nonadapted treatments. Thus, there is currently insufficient data to determine whether (a) intervention efficacy depends in part on the level at which stigma is measured (i.e., individual experiences vs. structural contexts) or (b) this apparent divergence in effects across levels is simply an artifact of the types of interventions that have been conducted at each level (i.e., adapted vs. nonadapted).
One way to adjudicate these competing explanations in future research is to incorporate measures of stigma experiences into studies that compare nonadapted with adapted health interventions. Because stigma-adapted interventions do not target stigma at its source (i.e., they do not eradicate stigma), it is possible that adapted interventions work no better than their nonadapted versions for individuals with high levels of stigma experiences. Yet one study found that among Latinx participants who had reported high discrimination at baseline, those in the adapted intervention experienced a mean reduction in the frequency of alcohol-related consequences at the 3-month follow-up that was nearly twice as large as the decrease observed among those in the nonadapted intervention (Lee et al., 2019). More comparative studies are needed to determine when selective and directed adaptations (Lau, 2006) of health interventions are warranted to address stigma-related mechanisms.
Finally, existing research has evaluated structural stigma as a moderator of intervention efficacy using spatial meta-analyses (Price et al., 2021; Reid et al., 2014). Although this method has many advantages, future research would benefit from the inclusion of additional methods for exploring associations between structural stigma and intervention efficacy in order to triangulate evidence. These methods could include multisite studies in which treatment sites that differ on structural stigma are strategically selected, online intervention studies delivered across diverse structural-stigma contexts, and single-site studies that leverage variability in prior exposure to diverse structural-stigma contexts that might continue to compromise health. These studies should include both adapted and nonadapted treatments to determine whether stigma-adapted treatments, compared with nonadapted interventions, can more effectively buffer against the adverse consequences of structural stigma.
Conclusion
We have reviewed emerging evidence from randomized controlled trials and spatial meta-analyses indicating that stigma may be an important, but heretofore underrecognized, source of treatment-effect heterogeneity in mental- and behavioral-health interventions. This research suggests that stigma may predict not only the individuals for whom these interventions are more efficacious (i.e., those with more stigma experiences), but also the social contexts that are more likely to undermine intervention efficacy (i.e., communities with greater structural stigma). By highlighting the potential role of personal and contextual stigma in shaping intervention response, we hope our review paves the way for additional research.
Recommended Reading
Hatzenbuehler, M. L. (2017). (See References). A comprehensive overview of the literature on structural stigma and health as it relates to several stigmatized groups.
Johnson, B. T., Cromley, E. K., & Marrouch, N. (2017). (See References). A helpful resource describing how to conduct spatial meta-analyses.
Millar, B. M., Wang, K., & Pachankis, J. E. (2016). (See References). A report on one of the first studies to use an implicit measure of stigma and to show that it predicts variation in response to a mental-health intervention among gay and bisexual men.
Pachankis, J. E., Williams, S. L., Behari, K., Job, S., McConocha, E. M., & Chaudoir, S. R. (2020). (See References). A report on one of the few studies to examine whether treatment-effect heterogeneity is related to stigma experiences, which showed that lesbian, gay, bisexual, and transgender young adults who report more stigma experience at baseline derive greater benefit from brief interventions focused on coping with stigma.
Reid, A. E., Dovidio, J. F., Ballester, E., & Johnson, B. T. (2014). (See References). A report on an empirical application of the spatial meta-analytic approach to the study of structural stigma as a moderator of the efficacy of a behavioral intervention.