
Abstract
Between-individuals variation in neural responses to errors and rewards is associated with the degree of risk for developing depression and anxiety, but not all individuals with perturbations in systems that generate these responses go on to develop symptoms. We propose that exposure to stressful life events may determine when these individual differences in neural responses to errors and rewards result in anxiety or depression. In this article, we review key findings and discuss limitations and questions in research on how stressors interact with reward and error processing to predict the development of symptoms. We conclude by outlining future research directions.
Anxiety and depression are among the most prevalent and debilitating forms of disease worldwide. More than 500 million people around the world suffer from clinically significant anxiety or depression each year (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018), and many of these people develop chronic, recurrent illness, such that the burden of illness increases over time. This suggests a need to intervene early in the course of these disorders. Yet much is still unknown about what causes and maintains them, and even the best available prevention efforts are only moderately effective. Development of more effective targeted interventions depends critically on the ability to understand pathways to depression and anxiety and to accurately identify which people are most likely to become ill.
Barriers to these endeavors include the complicating factors of comorbidity (people often meet criteria for multiple diagnoses) and heterogeneity (people with the same diagnosis can show very different symptom profiles), which challenge categorical definitions of psychopathology. Recent initiatives have been undertaken to address these issues by attempting to move psychopathology research beyond studies of single categorical diagnoses and to identify fundamental dimensions of functioning that go awry in psychopathology and can be studied across diagnoses.
Error and reward sensitivity are two such dimensions. To effectively navigate a constantly changing environment, people must be able to evaluate their behavior and its consequences. To avoid disaster (e.g., tumbling down a rock face, incurring social disfavor), people must know when they have erred and why. To ensure that good things happen (e.g., affiliating with others, reproducing), people must process and connect those positive outcomes with what they did to make them happen. These functions operate in all people, but individuals differ in the sensitivity of their error- and reward-processing systems, and these differences have been linked to anxiety and depression. In particular, research has demonstrated heightened error sensitivity in individuals with some forms of anxiety (Weinberg et al., 2015) and dampening of reward responsiveness in individuals with some depressive profiles (Kujawa & Burkhouse, 2017). Moreover, measures of reward and error sensitivity are sometimes altered in people who are not currently ill but are at risk for anxiety and/or depression and can prospectively predict the onset of illness (Kujawa & Burkhouse, 2017; Weinberg et al., 2015). These findings suggest that aberrations in reward and error sensitivity are not symptoms of anxiety and depression, but instead may reflect vulnerabilities for the later emergence of psychopathology.
It is worth noting, however, that, not everyone with aberrant error and reward sensitivity will develop anxiety or depression (Riesel et al., 2019), which suggests that these vulnerabilities require a catalyst. Stressful life events are likely one such catalyst. Indeed, exposure to stressful life events is one of the most powerful predictors of anxiety and depression. We note here that the word “stress” can refer to multiple events, experiences, and emotions that differ in important ways. For instance, “stress” can be used to refer both to something that happens to a person (e.g., a global pandemic) and to the way in which that person reacts to that stressor (e.g., anxiety, dread). For a comprehensive overview of this topic, as well as of the challenges in measuring the types of stressors that matter for anxiety and depression, we refer readers to Harkness and Monroe (2016). However, we focus in this review on the moderating influence of the occurrence of stressful life events, also called stressors, on associations between error and reward sensitivity and subsequent symptoms, rather than on individuals’ subjective perception or experience of those stressors.
This is in part because subjective perceptions of stress are almost always at least partly confounded with the affective outcomes of interest in the studies we discuss. In particular, individuals who perceive events as more severe or stressful may be more likely to develop anxiety and/or depression. This is consistent with evidence that not everyone who experiences even severe stressors goes on to develop anxiety or depression—in fact, most people do not. Theories explaining these mixed outcomes abound, but one prominent theory is the diathesis-stress model, which posits that some individuals possess vulnerabilities, or diatheses, that render them more susceptible than other individuals to the adverse effects of stressful life events (Fig. 1). According to this model, individuals with these diatheses are more likely than individuals without them to develop anxiety or depression, particularly following stressful life events. In this article, we discuss promising new evidence that neural responses to rewards and errors reflect specific ways of being vulnerable to stressors, and that these vulnerabilities can result in distinct poststressor symptom profiles. In particular, we focus on neural responses to errors and rewards measured via event-related potentials (ERPs), brain responses derived from recordings of the brain’s electrical activity and time-locked to specific events (e.g., presentation of images or feedback to participants in a lab or errors made by participants). In what follows, we discuss evidence from two sensitive and specific ERP measures of neural response to errors and rewards.
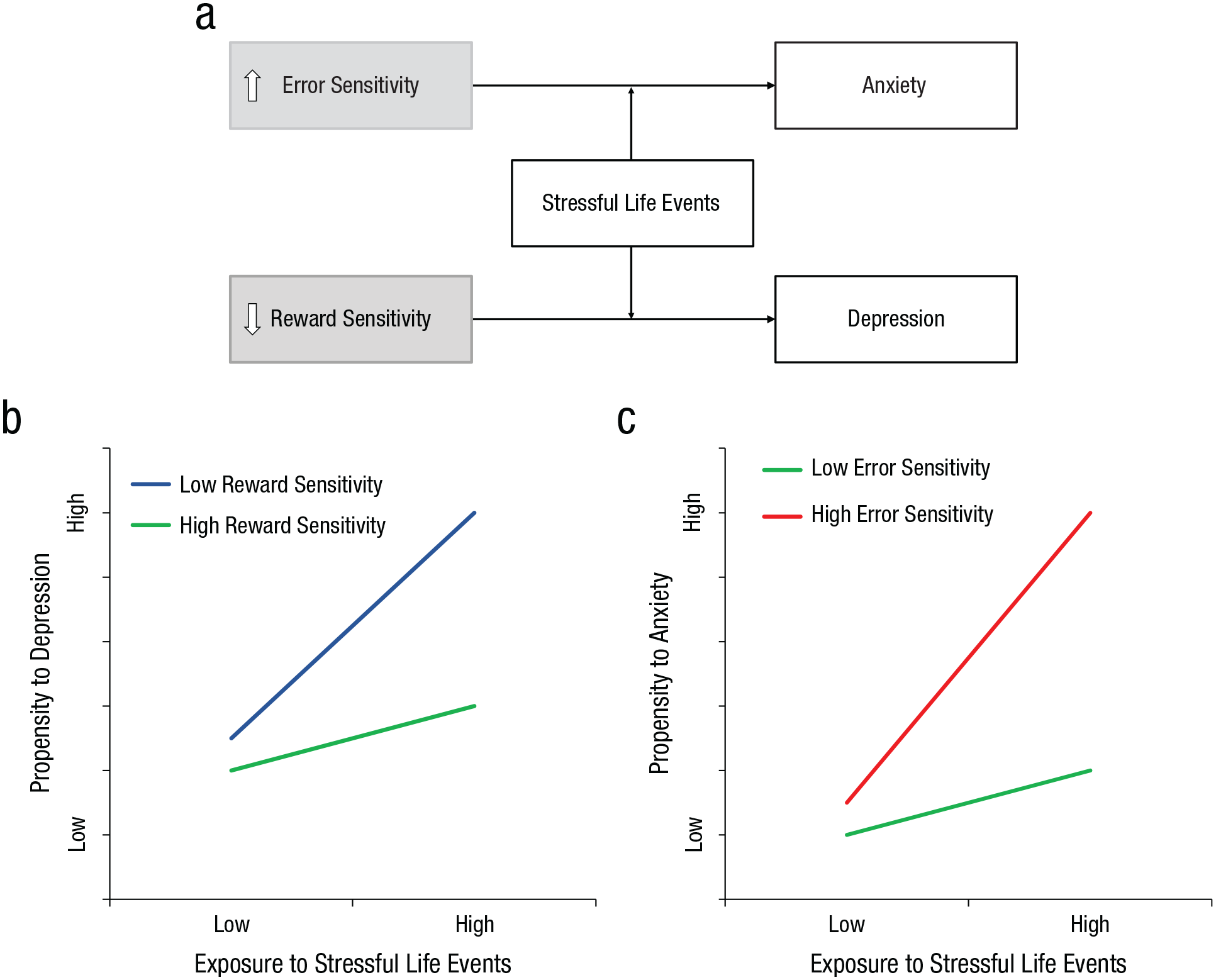
Illustration of the diathesis-stress model as it applies to the roles of the error-related negativity (ERN) and reward positivity (RewP) in the development of anxiety and depression following stressful life events. The schematic in (a) is a simplified representation of associations among error and reward sensitivity, exposure to stress, and anxiety and depression. As shown, trait-like differences in neural sensitivity to errors and rewards may become particularly maladaptive when individuals are exposed to stressful life events, resulting in heightened anxiety and/or depression. The graph in (b) is an example of how exposure to stress might affect the association between low reward sensitivity and proneness to depression: Although someone with a blunted neural response to rewards might be more prone to depression than someone with a larger neural response to rewards under even low levels of stress exposure, this vulnerability becomes particularly pronounced at high levels of exposure. The graph in (c) depicts the interaction between exposure to stressful life events and error sensitivity. Individuals with greater sensitivity to errors show a stronger association between exposure to stressful life events and subsequent anxiety.
Errors
For most people, errors are merely unpleasant, though in extreme cases, errors can be dangerous: A momentary slip while driving a car can be fatal. However, for some people, even minor errors seem catastrophic. These individuals are particularly sensitive to the commission of errors, and anxiously guard against them. We study neural markers of variation in this error sensitivity using an ERP called the error-related negativity (ERN), a neural response generated by the anterior cingulate cortex after participants make mistakes in speeded reaction time tasks (e.g., tasks in which participants must quickly indicate the direction of a central arrow in a briefly presented array of arrows that may or may not be pointing in the same direction; Weinberg et al., 2015). Figure 2a depicts the ERN observed in a sample of adult participants performing such a task, and Figure 2b represents the areas on the scalp where the difference between errors and correct responses is largest. A larger (i.e., more negative) ERN—indicating greater sensitivity to errors—is evident across multiple anxiety and related disorders, including obsessive-compulsive disorder (OCD), generalized anxiety disorder (GAD), and social anxiety disorder (SAD; e.g., Riesel, 2019; Weinberg et al., 2015), as well as in individuals with similar subclinical symptoms. In contrast, an increased ERN has been less consistently observed in individuals with depression (see, e.g., Weinberg et al., 2015, for a review). Further, studies comparing the ERN in “pure” anxiety samples (i.e., people without depression) and comorbid samples (i.e., people showing clinical symptoms of both anxiety and depressive disorders) suggest that comorbid current depression can attenuate associations between anxiety and the ERN (see, e.g., Weinberg et al., 2015, for a review). Thus, an increased ERN appears to be somewhat specific to some forms of anxiety and associated traits, which suggests that abnormal error processing may ultimately help in differentiating some anxious from depressive pathologies.
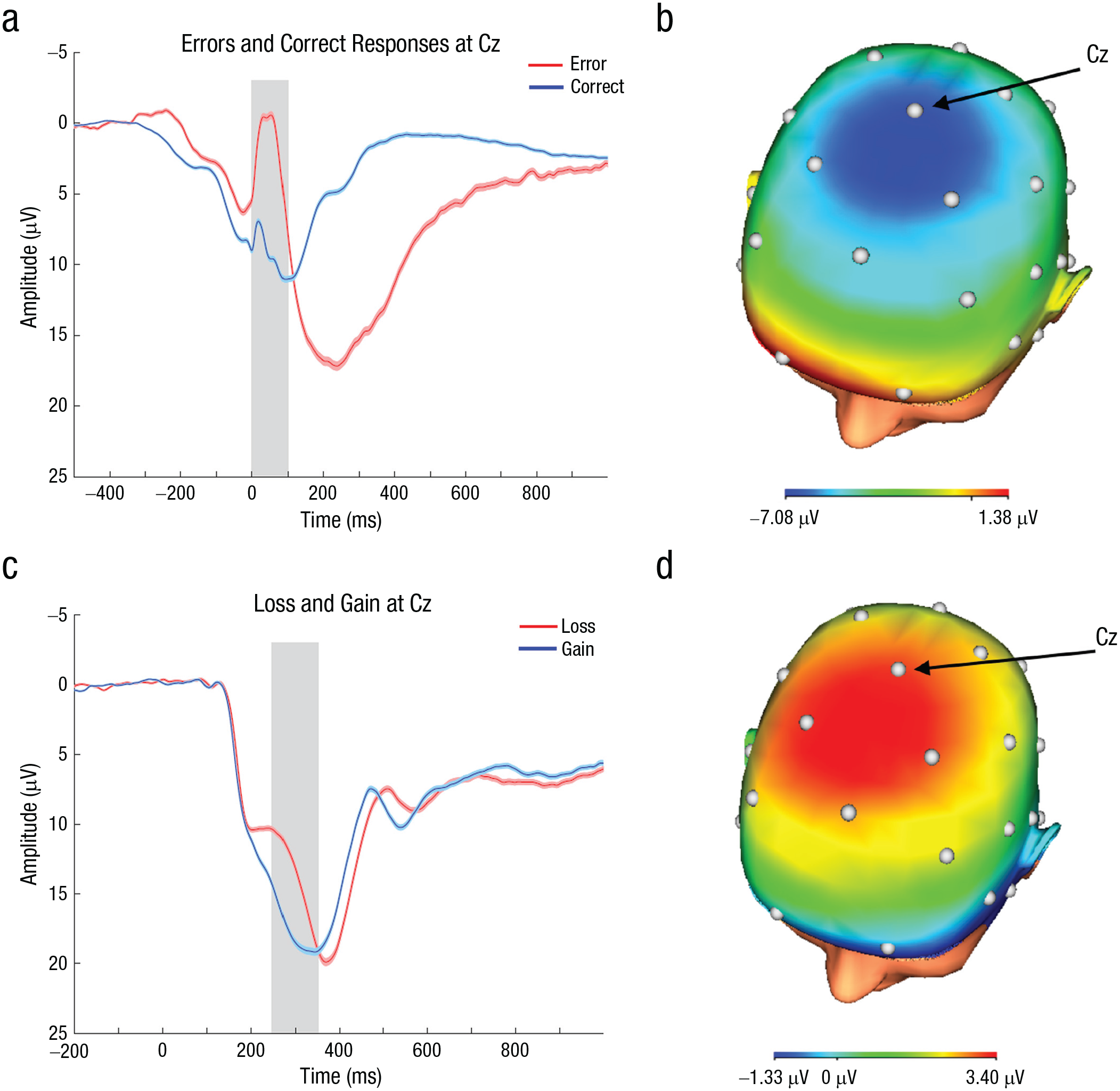
Illustration of the error-related negativity (ERN) and the reward positivity (RewP), event-related potentials (ERPs) elicited following errors and rewards, respectively. The graph in (a) shows average ERP waveforms in a sample of 357 participants. Separate waveforms are shown for trials on which participants responded correctly and incorrectly. Also shown in lighter color around each waveform is the standard error of the mean at each time point. Time in milliseconds is shown on the x-axis (0 ms is the time when the response was made), and the amplitude of the component in microvolts is depicted on the y-axis. Per ERP convention, negative is plotted up. The ERN is a negative-going deflection in the waveform (relative to the waveform following correct responses), peaking approximately 50 ms following the commission of an error on a speeded response task. The gray shaded area highlights the time interval during which the ERN was measured, between 0 and 100 ms following the commission of a mistake. The image in (b) shows the scalp distribution of the difference between neural responses to incorrect and correct responses (incorrect minus correct) during the first 100 ms following response. The ERN tends to be maximal at frontocentral sites on the scalp (e.g., Cz), as indicated by the areas of darker blue. A larger ERN means a greater difference between neural responses to errors and correct responses in this time window; a smaller ERN means less differentiation between these two responses. The graph in (c) shows average waveforms in a sample of 365 adult participants, in a simple guessing task in which they won or lost money. Separate waveforms are shown for gain and loss trials. The conventions for plotting the waveforms are the same as in (a). The RewP is a positive-going deflection in the waveform (relative to the waveform following losses) approximately 250 to 350 ms following a gain. The gray shaded area highlights this time interval during which the RewP was measured. The image in (d) shows the scalp distribution of the difference between neural responses to gains and losses (gains minus losses) between 250 and 350 ms after feedback. The RewP is maximal at frontocentral sites on the scalp (e.g., Cz), as indicated by the areas of darker red. The RewP is understood to reflect the degree to which individuals differentiate positive from negative feedback. That is, individuals with a larger RewP show a greater difference between neural responses to feedback signaling positive outcomes and neural responses to feedback indicating negative outcomes.
A growing number of studies support the idea that abnormalities in ERN magnitude may be a neural vulnerability for later symptom development. That is, an enhanced ERN does not appear to be merely a correlate of anxiety symptoms. Instead, people at risk for anxiety or OCD, by virtue of a family history of these disorders, show an enhanced neural response to errors even in the absence of any significant symptoms (e.g., Riesel, 2019). Further, increased ERN amplitude persists after successful treatment for anxiety disorders and OCD (Hajcak et al., 2008; Kujawa et al., 2016; Riesel et al., 2015), and an enhanced ERN in childhood and adolescence can prospectively predict subsequent increases in anxiety in later development (e.g., Meyer, 2017). Combined, these data suggest that the ERN may be useful in indicating individuals who are at greatest risk for anxiety and related disorders, even before they show symptoms.
However, these data also raise the question of why some individuals with this risk marker become ill and others do not. This has led us to investigate the role that exposure to stress may play in pathways to clinically significant anxiety. There is emerging evidence that an enhanced neural response to errors makes people particularly susceptible to adverse effects of stressors. For instance, one recent study showed that among first-year undergraduates who experienced a large number of stressors across the course of their first year, students with a larger ERN at entry to university were more likely to show heightened anxiety by the end of the year than those who had a smaller ERN at baseline (Banica et al., 2020). Another study found a similar effect in children exposed to a natural disaster (Meyer et al., 2017), and in a study of adults, a heightened ERN prior to the COVID-19 pandemic was indirectly associated with increases in symptoms during the first COVID-19 wave, through effects on perceived risk and stress (Riesel et al., 2021). Overall, these results indicate that the ERN is a promising marker of risk for anxiety and related disorders, particularly following exposure to stress.
Reward
Whereas heightened sensitivity to errors appears to be relevant to many forms of anxiety, abnormalities in neural response to rewards, as captured by the reward positivity (RewP), may relate more strongly to depression and risk for depression. The RewP (also referred to as the feedback negativity or FN/FRN) is an enhanced positivity in the ERP following reward feedback, compared with negative or neutral feedback, and peaks 250 to 350 ms after the onset of feedback over frontocentral sites (Proudfit, 2015). Figure 2c depicts the RewP recorded during a simple monetary reward task, and Figure 2d represents the areas on the scalp where the difference between gains and losses is largest. The RewP is reliably observed from childhood through late adulthood in tasks using a variety of reinforcement types (e.g., money, social approval; Ethridge & Weinberg, 2018; Kujawa et al., 2018). Studies leveraging both ERP and neuroimaging methods indicate associations between the RewP and activation of reward-related brain circuits, including the ventral striatum and medial prefrontal cortex (e.g., Carlson et al., 2011). Further, a reduced RewP has been observed in both adults and youth with current depression, which is consistent with evidence for blunted motivation and hedonic function in depression (e.g., Foti et al., 2014; Klawohn et al., 2020), and there is some evidence of specific links between a reduced RewP and anhedonia symptoms (e.g., Foti et al., 2014). In contrast, a reduced RewP has not typically been observed in anxiety disorders, with the exception of GAD, which shows significant symptom overlap with depression (e.g., Kessel et al., 2015).
Critically, there is also growing evidence that a reduced RewP is not a correlate of depressive symptoms, but is instead an early-emerging vulnerability for the later development of depression. Specifically, a reduced RewP has been observed in children of mothers with histories of pure depression without comorbid anxiety (Kujawa et al., 2014). Further, multiple longitudinal studies have indicated that a blunted RewP prospectively predicts increases in depressive symptoms across adolescence (e.g., Kujawa et al., 2019) and reflects a relatively specific vulnerability for depression, as opposed to anxiety (Kujawa et al., 2014).
Yet, again, not everyone with a small RewP will develop depression. Furthering the notion that low reward responsiveness could make people particularly vulnerable when they encounter stressors, studies have indicated that exposure to stressful life events moderates the association between the RewP and depressive symptoms across adolescence and early adulthood, such that the combination of low reward responsiveness and high stress is associated with the greatest risk for depression (e.g., Burani et al., 2021). Similarly, in recent studies, exposure to stressful events related to the COVID-19 pandemic (e.g., social isolation, job loss, financial strain) predicted the strength of associations between the RewP and increases in symptoms of depression across the course of the early days and months of the pandemic (Feurer et al., 2021; Freeman et al., 2021).
Future Directions
Although we believe that the ERN and RewP will be useful in advancing understanding of trajectories to internalizing psychopathology (e.g., anxiety and depression), there are many additional considerations. First, as noted above, both anxiety and depression are highly heterogeneous and often co-occur with other disorders, and more specific phenotypes within these broad diagnostic categories exhibit different associations with the ERN and RewP. For instance, although a relatively large ERN has been observed in OCD, GAD, and SAD, it is not observed across all anxiety disorders (for a review, see, e.g., Weinberg et al., 2015). Similarly, there is emerging evidence that the RewP may relate more specifically to manifestations of depression characterized most strongly by anhedonia (e.g., Foti et al., 2014), though this requires further investigation. Additionally, there is evidence for a blunted RewP in GAD (Kessel et al., 2015), an anxiety disorder that shows considerable comorbidity with depression, but an anxiety disorder nonetheless. Further complicating this story is evidence that comorbidity between anxiety and depression can alter their associations with both the ERN (e.g., Weinberg et al., 2015, 2016) and the RewP (e.g., Kujawa et al., 2014). The fact that nominally similar diagnoses show distinct associations with neurobiological markers, and nominally distinct diagnoses show similar associations, while comorbidity can change the nature of these associations, further illustrates the necessity of research that can identify more specific clinical phenotypes within and across broad diagnostic categories. It is our hope that the ERN and the RewP will be useful in this regard.
A similar problem is the fact that life stress is also not monolithic—in its characteristics, the domains in which it occurs, or its timing. Stressors can be episodic (e.g., a mugging) or chronic (e.g., sustained maltreatment during childhood), can reflect threats to one’s relationships or physical safety, and may have occurred in early life or in the past few days. An important future direction will be to determine whether these different properties of stressors determine the extent to which they interact with error and reward sensitivity to determine mental-health outcomes.
Additionally, it is not yet clear why a larger ERN or a smaller RewP might make individuals more vulnerable to the effects of stress. We have previously argued that the ERN reflects the degree to which individuals catastrophize errors, and the degree to which they will work to avoid them (e.g., Weinberg et al., 2015). Errors may become even more threatening to individuals with a large ERN when they are exposed to stress, as errors may be more costly in these situations. Thus, individuals with a larger-than-average ERN may appraise stressful life events as overly threatening, may overestimate the probability of and risk for adverse outcomes (e.g., Riesel et al., 2021), may monitor their own performance quite stringently to avoid errors, and may engage in behaviors that can reduce anxiety in the short term (e.g., checking behaviors, worry; Weinberg et al., 2015) but tend to be associated with increases in anxiety over time.
One possible explanation for the link between a blunted RewP and greater susceptibility to stressors is that the blunted RewP may be related to greater physiological reactivity to stressors, for instance, in the form of increased cortisol (e.g., Ethridge et al., 2020). Prolonged exposure to high levels of cortisol as a result of severe or chronic stressors may then cause further alterations to systems that process rewards in the environment, making individuals with this initially blunted reward response still more vulnerable to the effects of subsequent stressors. Another possible explanation is that a blunted neural response to rewards may be related to reduced incentive or ability to pursue rewards in the environment and lead to depression in times of stress when available reinforcers are limited (e.g., because of loss of a loved one or job). Additionally, there is emerging evidence that a blunted RewP may be related to reduced ability to sustain positive affect in the presence of stress (e.g., Renault et al., 2022), which suggests that processes reflected by a blunted RewP may limit individuals’ ability to cope adaptively with stressors.
Additionally, although the data we have discussed are promising and indicate that the ERN and RewP will be helpful indices of who will become symptomatic following exposure to stress, it will also be important to extend these bivariate and unidirectional findings and consider bidirectional, multivariate, and dynamic associations over time. For instance, both real-world and laboratory stressors have been associated with alterations in the ERN and RewP (e.g., Ethridge et al., 2020; Kujawa et al., 2020; Riesel et al., 2012), and there is evidence that heightened error sensitivity and diminished reward sensitivity can be mediators, or mechanisms, of the effects of stress exposure on anxiety and depression, respectively (e.g., Kujawa et al., 2020). Thus, researchers will need to consider the ways in which stressful experiences—particularly those occurring during periods of pronounced neural plasticity, such as infancy, early childhood, and the transition to puberty—might cause adaptations in systems that process errors and rewards (e.g., Kujawa et al., 2020). These early adaptations might then also render individuals more susceptible to future stressors occurring in different contexts.
Further, many of the studies we have discussed considered the ERN and/or RewP as independent of the experience of subsequent stressors. However, people actively construct the environments in which they exist, and traits—including neural traits—can influence the types of experiences people have. Our work has just begun to consider how neural responses to rewards or errors might predict which individuals are more likely to experience stressors across time, and what kinds of stressors they are likely to experience. There is preliminary evidence that a blunted RewP can prospectively predict increases in dependent stressors (i.e., stressors to which an individual contributes, such as interpersonal conflict), and that these stressors may mediate the pathway from a blunted RewP to depression (Mackin et al., 2019), though further work is warranted. However, the mechanisms by which a blunted RewP or enhanced ERN results in greater exposure to stress have yet to be identified.
One avenue that we have pursued is the possibility that a smaller RewP in response to positive feedback might less effectively guide adaptive behaviors, particularly interpersonal behaviors (Weinberg et al., 2021), thereby leading to greater interpersonal stress. Supporting this idea, one of our recent studies demonstrated that women with a history of depression show a blunted RewP in response to social acceptance, and that this blunted RewP is associated with decreased relationship quality outside of the lab. Critically, we found the same blunted RewP in their never-depressed adolescent daughters, who did not yet show the associations with interpersonal functioning (Freeman et al., in press). In short, there is emerging evidence that neural traits reflected by ERPs critically influence the ways in which people perceive, experience, and construct their environment.
Finally, a crucial next question is how to bridge the gap between these basic neuroscience findings and interventions that can improve outcomes for people with, or at risk for, anxiety and depression. The results described above suggest that the ERN and RewP are promising neural vulnerability markers that precede symptoms and make people more vulnerable to the effects of stress exposure. These neural responses may therefore be targets for mechanism-based prevention and intervention. Early attempts to target altered error processing either via therapy-based interventions (Meyer et al., 2020) or via brain stimulation (Reinhart et al., 2015) are promising and point to a fruitful avenue for future research. Likewise, there is emerging evidence that the RewP is sensitive to both transcranial magnetic stimulation (Biernacki et al., 2020) and manipulations that increase motivation and the personal salience of potential rewards (Pegg & Kujawa, 2020). Combined, these studies support the possibility of targeting error and reward responsiveness in youth at risk in order to prevent later psychopathology.
Conclusion
ERPs are an economical and well-tolerated neuroimaging methodology, and the ERN and RewP can capture perturbations in neural systems involved in processing errors and rewards. A larger-than-average ERN and smaller-than-average RewP appear to index early-emerging vulnerabilities that can improve understanding of pathways to internalizing symptoms, but their associations and interactions with stressful life experiences also need to be carefully considered. Research on how exposure to stressors affects people and who is likely to be most vulnerable to its adverse effects will be all the more urgent in the coming years, as much of the world’s population will continue to grapple with the lasting effects of a severe, uncontrollable, and chronic stressor in the form of the COVID-19 pandemic. In carefully assessing associations among these ERPs, stressors, and resulting symptom profiles, this line of research should improve prediction, prevention, and intervention, in service of improving outcomes and reducing the burden of these pernicious forms of psychopathology.
Recommended Reading
Dillon, D. G., Rosso, I. M., Pechtel, P., Killgore, W. D. S., Rauch, S. L., & Pizzagalli, D. A. (2014). Peril and pleasure: An RDoC-inspired examination of threat responses and reward processing in anxiety and depression. Depression and Anxiety, 31(3), 233–249. https://doi.org/10.1002/da.22202. An accessible, broad review of reward and threat sensitivity in anxiety and depression.
Hajcak, G., Klawohn, J., & Meyer, A. (2019). The utility of event-related potentials in clinical psychology. Annual Review of Clinical Psychology, 15, 71–95. https://doi.org/10.1146/annurev-clinpsy-050718-095457. A good primer on what event-related potentials are and how they can be used in clinical psychology research.
Ingram, R. E., & Luxton, D. D. (2005). Vulnerability-stress models. In B. L. Hankin & J. R. Z. Abela (Eds.), Development of psychopathology: A vulnerability-stress perspective (pp. 32–47). Sage. https://doi.org/10.4135/9781452231655.n2. A thorough and accessible overview of vulnerability-stress models of psychopathology.