
Abstract
Youth mental health problems have increased dramatically in the past decade, whereas the availability of mental health providers has not. This workforce shortage reflects complex dynamics that make it difficult to increase the supply of providers through existing graduate-training pipelines. Task shifting involves transferring the delivery of healthcare services to providers with less specialized training and is one strategy with potential for growing the behavioral health workforce. Here we review evidence that nonspecialist providers can effectively deliver behavioral health services and argue that a bachelor’s-level mental health profession with standardized training in evidence-based practices may be a solution to growing workforce shortages. We describe the undergraduate program at the Ballmer Institute for Children’s Behavioral Health as a model for how to grow the youth behavioral health workforce through the creation of a bachelor’s-level profession with a scope of practice emphasizing the early identification and prevention of mental health problems. The replication of this program at other universities is underway alongside program evaluation and policy work to create the credentialing and billing mechanisms needed to support sustainable employment pathways for a new profession. We invite partnership with universities interested in joining the movement to create a coordinated workforce development solution to the youth mental health crisis.
As many as half of U.S. youth will experience a mental health problem by the time they reach adulthood (Kessler et al., 2012; Merikangas et al., 2010). Over the past decade, youth mental health problems have steadily increased. Rates of depression, anxiety, and suicidal thoughts and behaviors have risen dramatically in adolescents, particularly among females (Centers for Disease Control and Prevention, 2023; Twenge et al., 2018). One in three adolescent girls reports seriously considering suicide in the past year, one in four have made a suicide plan, and suicide deaths among young people have increased more than 50% over the past decade (Centers for Disease Control and Prevention, 2023).
The mental health needs of youth are overwhelming the capacity of the behavioral health workforce. Prior to the pandemic, fewer than half of youth with a mental health problem serious enough to warrant treatment had ever received services for that condition (Whitney & Peterson, 2019). Children with symptoms that did not meet criteria for a diagnosis were even less likely to receive services (Splett et al., 2018). The gap in the need for support and receipt of mental health intervention widened during the pandemic as demand for services increased while the proportion of trained mental health professionals did not (Kuehn, 2022). Nationally, more than half of families seeking behavioral health services for their children report meaningful difficulty obtaining care (Kaiser Family Foundation, 2023). The dramatic erosion in mental health among young people coupled with the shortage of mental health professionals has led numerous health organizations to declare the youth mental health crisis a national emergency.
The Promise of Bachelor’s-Level Providers
The shortage of youth behavioral health providers reflects a range of complex dynamics, including increasing costs of graduate education, wages that are insufficient to incentivize graduate training and repay student debt, and challenges in retaining behavioral health providers in the workforce as a result of increasing caseloads, acuity of behavioral health concerns, and burnout, among many others (Hallett et al., 2024; Pyne & Grodsky, 2020). These factors make it difficult to increase the supply of well-trained behavioral health providers through existing graduate-training pipelines. Addressing the child mental health crisis requires innovative new approaches to train the mental health workforce, identify children and families in need of services, and deliver evidence-based interventions.
Task shifting is one strategy with potential for rapidly increasing the behavioral health workforce. Task shifting involves transferring the delivery of specific healthcare services to providers with less specialized training and has been recommended by the World Health Organization (2008) as a key strategy to expand access to health services. This approach has been widely used globally to address shortages in trained healthcare professionals, including mental health providers. Global mental health provides substantial evidence of the effectiveness of task shifting as a strategy to deliver evidence-based mental health interventions and increase access to high-quality care. In contexts in which a highly trained mental health workforce does not exist, it has been repeatedly demonstrated that nonspecialist providers with no formal training in mental health can effectively deliver evidence-based interventions with appropriate training and supervision (Singla et al., 2017). Building on this evidence, the U.S. mental health system could benefit from a standardized approach to training less specialized providers to address persistent issues with access and equity (Giusto et al., 2024; Singla, 2021).
Similar benefits of deploying nonspecialist providers to deliver behavioral health services have also been observed in high-income countries. Meta-analyses demonstrate that non-specialists can effectively deliver interventions for anxiety and depression in the perinatal period (Singla et al., 2021) and behavioral health interventions for a wide range of youth mental health problems (Weisz et al., 1995). Notably, paraprofessionals have been found to be more effective than highly trained clinicians in delivering interventions for youth with externalizing, but not internalizing, problems (Weisz et al., 1995). In the United Kingdom, bachelor’s-level providers have been integrated into the behavioral health workforce through the Improving Access to Psychological Therapies (IAPT) program (Clark, 2018; Wakefield et al., 2021). These frontline providers are trained to deliver brief, structured, “low-intensity” interventions to individuals seeking care for anxiety and depression paired with progress monitoring to ensure that referrals to higher intensity care are provided when problems worsen or fail to respond to initial intervention. This program has increased the reach of evidence-based interventions, has been effective at reducing anxiety and depression in those who receive care, and is one of the most successful approaches ever undertaken to expand access to evidence-based mental health services (Clark, 2018; Wakefield et al., 2021). The IAPT program focused initially on services for adults, and the implementation and evaluation of a similar approach to delivering youth mental health services is underway (Ludlow et al., 2020).
In the United States, college students have played a role in behavioral health service delivery for decades, including for individuals with serious mental illness, children, and other college students. Historical accounts have even introduced the provocative notion that, in some regards, this workforce may be capable of supporting superior behavior change in clients compared with more highly educated and trained professionals (Gruver, 1971). Indeed, interventions delivered on college campuses designed to promote health behaviors and prevent the onset of behavioral health challenges are equally effective, and often more effective, when delivered by college students compared with interventions delivered by more highly trained clinicians (Fromme & Corbin, 2004; Stice et al., 2020). Currently, bachelor’s-level providers deliver mental health services in most states (Medlock & Maxey, 2024), but this workforce lacks standardized training or preparation for these roles. This has led to reasonable skepticism about the possibility of creating a well-trained bachelor’s-level behavioral health workforce. However, after receiving standardized training in evidence-based interventions, bachelor’s-level providers perform as well as those with an advanced degree in terms of intervention fidelity and treatment outcomes (Diebold et al., 2020; McGuier et al., 2021).
A Novel Strategy for Expanding the Youth Behavioral Health Workforce
Multiple lines of evidence suggest that creating a standardized training model for bachelor’s level behavioral health providers is a promising strategy to address persistent challenges in access to evidence-based youth mental health services in the United States. The Ballmer Institute for Children’s Behavioral Health is pursuing this strategy by creating a new bachelor’s-level mental health profession. Providing standardized applied training at the undergraduate level will expand the number of providers who are qualified to deliver services to youth and reduce barriers to obtaining this training. This workforce approach aims to increase access to evidence-based services for youth and improve equity in access to these services. Creating this type of system-level change requires coordinated efforts in the higher education, healthcare, and policy sectors.
A bachelor’s-level profession would serve a distinct role within the behavioral health system. Individuals in this role would be trained to deliver early identification, promotion, and prevention services in community settings in which children and families can easily access care, including schools, pediatric primary care, mental health agencies, and community-based organizations. Rooted in public health models of prevention, this scope of practice aims to expand the types of services available in the behavioral health system to address key gaps. When behavioral health concerns are identified early, preventive interventions are effective, can prevent mental health concerns from worsening over time, and may reduce the need for more intensive services that many children and families are unable to access in our current system (Han et al., 2025; Sandler et al., 2014).
Although our training program focuses specifically on youth behavioral health, a bachelor’s-level provider with a scope of practice emphasizing early identification, prevention, and brief intervention with adults could similarly expand access to services, as has been demonstrated in the United Kingdom through the IAPT program (Clark, 2018).
Scope of Practice
The scope of practice for this bachelor’s-level behavioral health profession encompasses early identification, promotion, and prevention and brief intervention services delivered under the supervision of a licensed mental health provider at the master’s or doctoral level (see Fig. 1). Early identification services designed to identify signs and symptoms of mental health problems focus primarily on universal and targeted screening (Rapee et al., 2025; Wissow et al., 2013). Services to promote behavioral health are designed to support wellness in all youth regardless of their level of risk and are sometimes referred to as “universal interventions” or, in schools, “Tier 1 services.” These services include strategies to increase mental health literacy and facilitate the adaptive development of competencies in domains such as identity, relationships, emotion awareness and regulation, and decision-making. Prevention and brief intervention services involve delivering brief evidence-based interventions to prevent the onset and progression of mental health concerns, reduce symptoms, and improve functioning. Bachelor’s-level providers are trained to deliver brief cognitive and behavioral practices—often referred to as the “common elements” of evidence-based practice—that are known to have beneficial effects on a wide range of common mental health concerns (Chorpita et al., 2007; Fitzpatrick et al., 2023; Weisz et al., 2012). A final key element of the scope of practice involves risk identification and referral through the use of evidence-based tools to evaluate the severity of mental health symptoms and the presence of clinical risk, track progress after interventions, and engage in appropriate referral practices to higher intensity interventions (e.g., psychotherapy) for youth with more severe clinical concerns. Training emphasizes delivering early identification, promotion, and prevention services in community settings in which children and families routinely access care, including schools, the healthcare system, and community-based organizations that provide youth services such as mentoring programs.
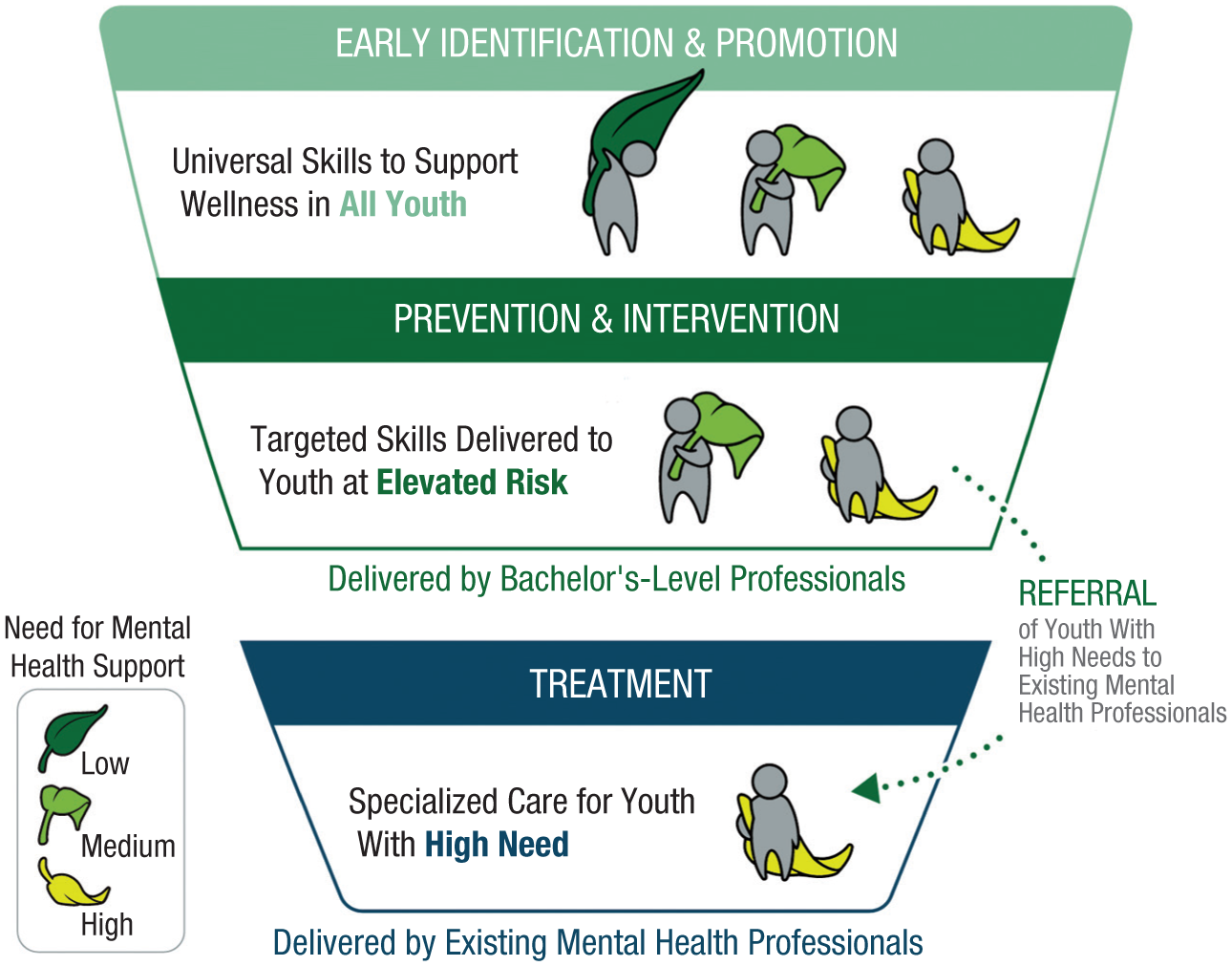
Scope of practice for a new bachelor’s-level mental health profession.
This scope complements existing mental health professions, including at the bachelor’s level, such as the baccalaureate social worker (BSW). The Council on Social Work Education (CSWE) describes BSW training as preparing graduates for “generalist practice positions (such as casework)” (CSWE, n.d., para. 2), whereas clinical work requires a master’s in social work and postdegree supervised hours. Training a prescribed set of practices is not aligned with social work’s historically generalist focus (Howard et al., 2007), and most social work programs do not emphasize training in evidence-based practices (Spensberger et al., 2020). In contrast, this new bachelor’s-level provider will be trained with relative depth in a limited number of specific common elements of clinical practice that have scientific support across primary, secondary, and tertiary intervention. Additionally, students are trained in the process of evidence-based practice, with an emphasis on formulating clinical questions, identifying and evaluating evidence, and applying evidence in conjunction with information about individual backgrounds, values, and preferences. Graduates of this new program will not be trained in a range of practices that are cornerstones of other professions, such as case management and advocacy—key to the practice of social work; administration and scoring of cognitive, academic, or neuropsychological assessments key to the clinical and school psychology scope of practice; provision of academic or career advising as in school counseling; or diagnosis of mental disorders or prolonged psychotherapy, which requires training in psychology, counseling, or social work at the master’s or doctoral level.
Training Bachelor’s-Level Providers
In building this novel program, we brought training components typically present only in graduate degree programs into an undergraduate program. These components include 2 years of specialized training in applied skills in early identification, promotion, prevention, and brief intervention and risk identification and referral; 700+ hours of supervised applied practice in community settings, such as schools and the healthcare system; and competency evaluations to ensure that students are developing the applied skills the program was designed to provide.
Curriculum
The child behavioral health curriculum spans five professional domains: early identification and progress monitoring, applied practice (promotion, prevention, and brief intervention), risk evaluation and referral, culturally responsive and inclusive practices, and professionalism and ethical behavior. The training program also includes a sequence that covers self-care and wellness and a range of skills to support professional development.
Training in early identification and progress monitoring focuses primarily on behavioral health screening as well as the routine assessment of behavioral health symptoms (i.e., measurement-based care), which is associated with improved youth mental health outcomes and recommended as part of evidence-based practice (De Jong et al., 2021; Ehrenreich-May et al., 2025). Students are trained to administer, score, and interpret evidence-based behavioral health screening and progress monitoring tools that can be used in different settings.
Training in applied practice encompasses promotion, prevention, and brief intervention. Promotion courses include training in mental health literacy along with three broad domains that have been shown in meta-analyses to prevent the onset of youth mental health problems: self-regulation skills, interpersonal skills that form the foundation of healthy relationships, and skills to promote health behaviors with strong links to mental health (e.g., sleep, physical activity, and adaptive digital media use; Korczak et al., 2017; Scott et al., 2021; Skeen et al., 2019). Training in prevention and brief intervention centers on a transdiagnostic, common elements approach. Rather than learning specific “branded” interventions, students are trained on a set of common elements that are present in numerous evidence-based interventions for a wide range of mental health problems (Chorpita et al., 2007; Fitzpatrick et al., 2023). The common elements included in our training program include relaxation and calming skills; problem-solving; motivational interviewing; behavioral principles of reinforcement as applied both with youth and in behavioral parent training; opposite action—which encompasses behavioral activation and graduated engagement in avoided situations; and flexible thinking.
Training in risk evaluation and referral focuses on evidence-based approaches to clinical risk identification (e.g., self-harm, suicidal ideation, and violence exposure) and response (e.g., safety planning), as well as appropriate referral and care coordination practices for youth with high clinical risk. Training in culturally responsive and inclusive practices focuses both on understanding sources of behavioral health disparities—with a focus on exposure to trauma, adversity, and discrimination—and practices to work effectively with youth with diverse identities, abilities, and backgrounds. Training in ethics and professional practice emphasizes professional skills needed in the behavioral health field, including ethical and legal standards, foundational helping skills, documentation, consultation, and collaboration.
In addition to this specialized coursework, all students complete general education requirements that are standard for a bachelor’s degree. To be successful in specialized child behavioral health training, students require awareness of individual and cultural differences and foundational skills in writing and oral communication, critical thinking, and evaluating research evidence. In applied training, students routinely make complex decisions, apply ethical standards, and engage in varied forms of communication, all features that require the broad training that a bachelor’s degree comprises in addition to the specialized training provided in the child behavioral health curriculum.
Practicum experiences and supervision
Child behavioral health students acquire at least 700 hours of supervised applied practice across several practicum placements. All students complete a practicum in which a faculty member from our program is embedded alongside the student to model service delivery and provide direct, timely supervision. This allows students to observe licensed clinicians delivering services as an initial step and ensures intensive support from faculty who are well trained in their scope of practice when students begin delivering services themselves. After this initial practicum experience, students complete a year-long practicum placement in their final year of training. Placements occur in a wide range of settings, including early learning centers and preschools; pediatric primary care, community mental health, and other healthcare settings; and community-based organizations that provide mentoring and behavioral health services to youth. Students are supervised by a site supervisor (i.e., a licensed behavioral health professional) and complete group supervision each week with a faculty member from our program.
Competency-based evaluations
Competencies are assessed in all courses and practica to ensure students not only have acquired knowledge about core professional domains but also have developed relevant applied skills. Competency evaluations largely involve the direct observation of skills, either live or through a recording, but sometimes include other types of assignments that are appropriate for demonstrating a skill (e.g., interpretation of a screener). Our competency evaluation framework was developed to align, where possible, with the Ensuring Quality in Psychosocial and Mental Health Care framework from the World Health Organization (Kohrt et al., 2025). Competencies are scored on a standardized scale across professional domains, with students expected to reach the “Meets Expectations” level for each skill.
Feasibility
The integration of clinical training into an undergraduate major increases the number of specialized credit hours required. However, many universities offer similar types of pre-professional bachelor’s programs that require applied training; nursing is perhaps the best example. Bachelor’s-level nursing programs exist at many universities. These programs typically include a larger number of in-major credit hours than other majors and similarly emphasize training in specific skills required to enter an applied healthcare profession. The requirement for applied training makes these programs more specialized than a typical undergraduate major. Yet national data suggest that nursing is one of the most popular undergraduate majors (National Center for Education Statistics, 2024). Although we have not typically trained mental health professionals at the bachelor’s level, there is good evidence spanning decades that this type of pre-professional training is feasible to deliver at the undergraduate level in other healthcare fields.
Building a New Profession
We intend for the child behavioral health training program (CBH-TP) to become a national model for creating a bachelor’s-level behavioral health workforce. To do so, we need to demonstrate that our training program is effective and has a positive community impact. We are currently evaluating multiple elements of the program to ensure we are providing high-quality training to students and delivering services that are benefiting the schools and communities in which our students are practicing. The design encompasses an evaluation of the training program (i.e., student outcomes, including the development of key competencies and intervention fidelity), the effectiveness and acceptability of services delivered by students (i.e., youth and family outcomes, including symptom change, skill development, and perceived satisfaction and quality of services), and the impact on the community settings in which students are integrated (i.e., implementation outcomes, including reach and fit of services) and was informed by relevant stakeholders at multiple levels, including partnering schools and practicum sites, our community advisory board, and our national behavioral health advisory board. This evaluation will allow for continual refinement of the training model to produce the largest community impact.
Creating stable employment pathways for graduates requires partnerships with school districts, mental health agencies, primary-care practices, and community-based organizations as well as policy changes. Specifically, legislation is required to create a credentialing pathway for new providers to deliver services within their scope of practice and develop a payment model to allow services to be billed to healthcare payers. In Oregon, we approached this policy work by cultivating relationships with legislators whose priorities included child health and building a coalition of support for expanding the youth behavioral health workforce through a bachelor’s-level profession. This coalition included behavioral health employers, mental health and youth advocacy groups, healthcare organizations, and community-based organizations that support children and families. A process for garnering broad stakeholder input on the scope of practice and training requirements for a new bachelor’s-level provider was formalized as H.B. 4151 (Or. Legis. Assemb., 2024). The taskforce created by that legislation and the government agency overseeing the process both formally recommended the creation of a new bachelor’s-level provider type to the Oregon legislature. Legislation defining the scope of practice, training requirements, and licensing pathway for this new provider was passed with broad bipartisan support (S.B. 1547; Or. Legis. Assemb., 2026).
We are actively working with other states to create structures to support this bachelor’s-level behavioral health profession. The Nevada legislature has also enacted legislation (S.B. 165; Nev. Legis. Assemb., 2025) creating a bachelor’s-level provider mirroring the license created in Oregon that supports several state universities to replicate the CBH-TP. Notably, several other states (California, Washington, Utah, and Wyoming) have recently created credentialing pathways for bachelor’s-level behavioral health providers, signaling growing momentum to create a bachelor’s-level profession. Although these credentials differ somewhat in the services that can be offered, all require ongoing supervision by a mental health professional at the master’s or doctoral level.
To support other universities interested in launching training programs, we are building a toolkit of technical assistance materials to support the dissemination and scaling of the CBH-TP that will include details on building a curriculum, creating applied training experiences, program evaluation, and pursuing the policy work needed to support this profession over the long term—including legislative language that can be used across states to create a credentialing pathway. We will release an open-source version of our curriculum in summer 2026. We are eager to partner with other universities interested in building programs to provide support and ensure alignment across contexts.
Conclusion
The CBH-TP aims to grow the behavioral health workforce through a bachelor’s-level profession that emphasizes early risk identification and prevention of youth mental health problems. Recent credentialing legislation has formalized this new profession, establishing it as a critical rung in the continuum of roles in behavioral health care. Growing a reputable bachelor’s-level behavioral health profession in the United States will require a systematic and coordinated approach within and across sectors. To that end, we are actively developing partnerships with schools, behavioral health employers, community-based organizations, and other universities to build momentum in a movement to ensure all youth have access to evidence-based behavioral health support.
Recommended Reading
Clark, D. M. (2018). (See References). Reviews the Improving Access to Psychological Therapies program in the United Kingdom, including the implementation of a bachelor’s-level behavioral health workforce.
Fitzpatrick, O. M., Cho, E., Venturo-Conerly, K. E., Ugueto, A. M., Ng, M. Y., & Weisz, J. R. (2023). (See References). Meta-analysis of five common elements of youth mental health interventions demonstrating that each element is associated with beneficial treatment outcomes across a range of common youth mental health problems, with stronger benefits for interventions that incorporate more of these common elements.
Giusto, A., Jack, H. E., Magidson, J. F., Ayuku, D., Johnson, S. L., Lovero, K. L., Hankerson, S. H., Sweetland, A. C., Myers, B., & Fortunato dos Santos, P. (2024). (See References). Reviews partnerships that bring key service-delivery principles in global mental health—including task sharing through lay providers to deliver evidence-based mental health interventions—to address inequities in access to mental health services in the United States.
McGuier, E. A., Rothenberger, S. D., Friedman, A., & Kolko, D. J. (2021). (See References). Demonstrates equivalent intervention fidelity and treatment outcomes for providers with and without advanced degrees after receiving training in an evidence-based intervention.
Singla, D. R., Kohrt, B. A., Murray, L. K., Anand, A., Chorpita, B. F., & Patel, V. (2017). (See References). Reviews global mental health approaches to mental health service delivery, including task-shifting approaches utilizing lay providers to deliver evidence-based mental health interventions.
Footnotes
Acknowledgements
We would like to acknowledge the creativity, thought leadership, and substantial work contributed to the creation of the Ballmer Institute by faculty and university leaders at the University of Oregon and the faculty and staff of the Ballmer Institute.
Transparency
Action Editor: Kristina Olson
Editor: June Gruber