
Abstract

Background
Sensorimotor representation in the motor cortex is dynamic, distributed and overlapping. This maintains the capacity for significant functional reorganization throughout life following exercise, or after brain injury, which plays an important role in cortical plasticity.
It has been shown that injuries in limbs or facial nerve lesions cause reorganization in the motor cortex. 1 Animal studies on cortical plasticity indicate that the face representation occupied the hand representation in monkeys with therapeutic amputations, and the forelimb representation occupied the face representation in rats with facial nerve lesions. Furthermore, patients with facial nerve palsy exhibited an expansion and lateral extension of the hand motor area toward the face motor area. 2 On the contrary, patients with hemifacial spasm showed a decrease in the ipsilateral hand representation area relative to the contralateral side, and the center of gravity of the hand representation moved to the region of cortical face representation. 3 Thus, altering plasticity may play an important role in the recovery of function. 1
Case report
The subject was a 54-year-old man who had experienced left peripheral facial nerve paralysis caused by trauma 6 months earlier. His symptoms included asymmetry of the left corner of the mouth, absence of nasal labial fold, shallowing of the forehead lines, and numbness of the cheeks on the affected side. He was unable to complete the movements required to wrinkle his forehead, close his eyes, show his teeth, drum his cheeks or whistle. He provided written informed consent. The ethics committee of Guangdong Provincial Hospital of Chinese Medicine approved this study in 2017 (ref. Y2017-171).
Acupuncture treatment
The patient completed four sessions of needling at traditional acupuncture points twice per week for a total of 12 months. Stainless steel acupuncture needles (0.25–0.30 mm diameter, 25 mm length; Huatuo) were inserted at ST2, ST4, ST6 and GB14 on the affected side; 2 Hz electrical stimulation was applied for 30 min using a constant-current electroacupuncture (EA) device with moderately strong current intensity (2 mA).
Measurements
House–Brackmann (H-B) paralysis scale scores and electromyography (EMG) were assessed at baseline (T1) and after 3 months (T2), 6 months (T3), 9 months (T4) and 12 months (T5) of acupuncture to help achieve an objective measure of treatment outcome. The long-term effect of EA on the excitability of the motor cortex was evaluated at baseline and after each session via transcranial magnetic stimulation (TMS; Magstim Company Ltd, UK) detection using a figure-eight coil. Then, acupuncture was administered, and another five TMS detections were delivered again after acupuncture needle removal and respectively compared with the data before acupuncture to observe the immediate effect. Motor-evoked potentials (MEPs) were recorded by EMG at the contralateral first dorsal interosseous (FDI) muscles (abductor pollicis brevis) at rest and the bilateral orbicularis oculi (OO) muscle in the task of a blink. The resting motor threshold (RMT) of the FDI and active motor threshold (AMT) of the OO were identified at the hot spot with the lowest input of current intensity. The lowest intensity induced at least 50 mV in hand representation and 100 mV in face representation (three out of five times). MEPs were measured at 120% motor threshold (MT). The sum of the average MEP amplitudes at each stimulated location was calculated.
Outcome
After the acupuncture treatment, the patient was able to complete the movement of his face symmetrically. The treatment outcomes are presented in Figure 1(a). The long-term effect and the immediate effect of acupuncture are presented in Figure 1(b) and (c), respectively.
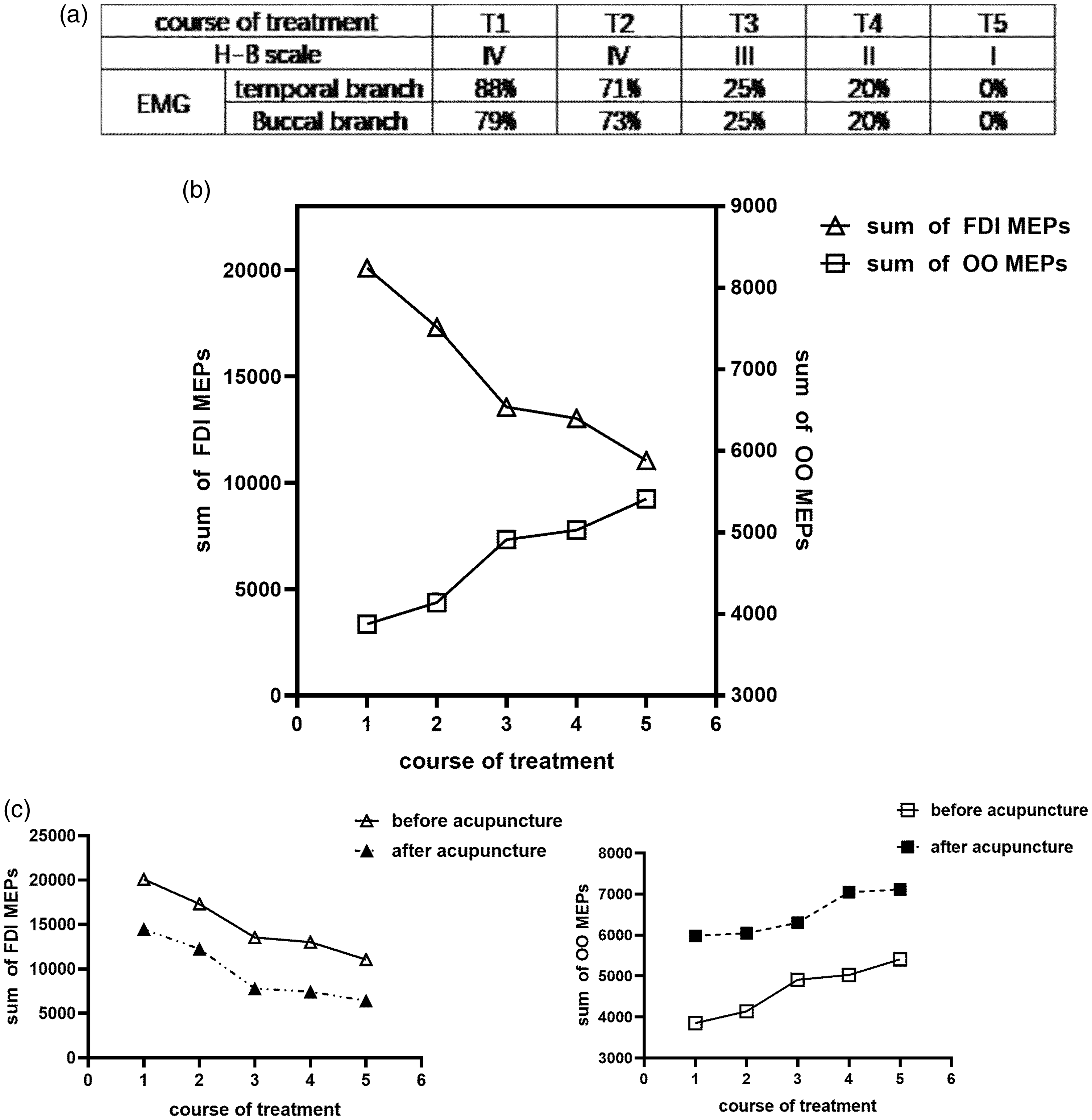
(a) Changes in House–Brackmann (H-B) paralysis scale scores and electromyography (EMG) following each acupuncture treatment session. (b) Changes in the sum of motor-evoked potentials (MEPs) following each treatment session. (c) Changes in the sum of orbicularis oculi (OO) and first digital interosseous (FDI = abductor pollicis brevis) muscle MEPs before and after acupuncture. Acupuncture induced an increase in the sum of OO MEPs (p < 0.005) and a decrease in the sum of FDI MEPs (p < 0.05).H-B scales: the House–Brackmann paralysis scales; EMG: electromyography; OO: orbicularis oculi muscle; FDI: abductor pollicis brevis muscle; MEPs: motor-evoked potentials.
Commentary
In the present study, we observed that EA on the affected side could: (1) improve symptoms of the sequelae of facial paralysis; (2) completely restore the function of the facial nerve; and (3) induce changes in excitability in the contralateral motor cortex (increased excitability in face representation and decreased excitability in hand representation). These results suggest that somatosensory stimulus-induced plasticity between the face and hand representations in the motor cortex may correlate with the improvement in facial paralysis.
Plasticity between different representations can be induced in healthy subjects by central or peripheral stimuli. Repetitive TMS (rTMS) of face or hand representations induced an inhibitory effect on upper arm representations in a transient ischemic nerve block (INB) model established in the proximal forearm of healthy subjects. 1 Moreover, somatic stimulation in the lower limb can produce changes in upper limb muscle representation in the motor cortex. 4
Furthermore, recent studies have suggested that plasticity between different representations may play an important role in the recovery of function. The best treatment options for facial pain caused by trigeminal nerve lesions involve stimulation of the face representation area of the cerebral motor cortex by rTMS, but not the facial representation area corresponding to the painful zone. 5
In summary, the plasticity between different representations induced by somatic stimuli may provide a new treatment strategy for functional recovery in neurological diseases. The effects observed in this case need to be verified in a large sample and further evaluated by controlled clinical studies.
Footnotes
Authors’ note
The views expressed in the submitted article are not an official position of the institution or funder.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Key Research and Development Program of China (grant no. 2019YFC1709100 and 2019YFC1709102), National Natural Science Foundation of China (grant no. NO81873381), and Guangdong Provincial Hospital of Traditional Chinese Medicine Science and Technology Research Projects (grant no. YN2019ML12).