
Abstract
Objective:
Existing systematic reviews and meta-analyses indicate that acupuncture has similar clinical effectiveness in the prevention of headache disorders (HDs) as drug therapy, but with fewer side effects. As such, examining acupuncture’s use in a pragmatic, real-world setting would be valuable. The purpose of this study was to compare the effects of acupuncture and prophylactic drug treatment (PDT) on headache frequency in patients with HDs, under real-world clinical conditions.
Methods:
Retrospective cohort study of patients with HDs referred to a pain clinic, using electronic health record data. Patients continued with tertiary care (treatment of acute headache attacks and lifestyle, meditation, exercise and dietary instructions) with PDT, or received 12 sessions of acupuncture over 3 months, instead of PDT under conditions of tertiary care. The primary outcome data were the number of days with headache per month, and groups were compared at baseline and at the end of the third month of treatment.
Results:
Data were analysed for 482 patients with HDs. The number of headache days per month decreased by 3.7 (standard deviation (SD) = 2.9) days in the acupuncture group versus 2.9 (SD = 2.3) in the PDT group (p = 0.007). The proportion of responders was 39.5% versus 16.3% (p < 0.001). The number needed to treat was 4 (95% confidence interval = 3–7).
Conclusion:
Our study has shown that patients with HDs in tertiary care who opted for treatment with acupuncture appeared to receive similar clinical benefits to those that chose PDT, suggesting these treatments may be similarly effective of the prevention of headache in a real-world clinical setting.
Keywords
Introduction
Primary headache disorders (HDs) do not have curative treatment options. The stated goals of long-term headache treatment are to: reduce the frequency, severity and disability associated with acute attacks; decrease the reliance on poorly tolerated, ineffective or unwanted acute pharmacotherapies; and avoid the escalation of acute headache medication. 1 Preventive pharmacological therapy may improve functional ability and responsiveness to treatment of acute attacks. Concern for side effects may discourage patients from accepting prophylaxis or may negatively influence patient adherence, causing different problems such as non-regular daily dosing, self-reduction of the prescribed compound or withdrawal of prophylaxis following trivial symptoms. 2 Acupuncture is used for the treatment of headaches and it may be applied as a single modality or as part of a more complex treatment. A total of 9.9% of acupuncture users in the United States stated that they had used acupuncture to treat migraine or other headaches. 3 A study in the United Kingdom reported that some 12% of patients attending a neurology outpatient clinic had already tried acupuncture and 73% would be willing to do so. 4
Sufficient existing evidence supports the use of acupuncture for headache. It is important to move from clinical trials to real clinical practice and to conduct comparative analysis. Real-world data can help inform which treatment is more appropriate for certain patient subgroups that may not have been well-represented in clinical trials and may be a way to see how these treatments measure up outside in routine clinical settings. This manuscript addresses this important clinical need by examining existing data from a pain clinic where acupuncture was incorporated.
We aimed to compare headache frequency associated with acupuncture as part of tertiary care, versus tertiary care with prophylactic drug treatment (PDT), in patients with HDs in a real-world clinical practice setting.
Methods
Design
A retrospective, observational study was conducted according to the STROBE and STRICTA guidelines.5,6 The study was carried out in the Son Llàtzer University Hospital pain clinic, Palma de Mallorca, Spain. Ethical approval was obtained from the Balearic Islands Human Research Ethics Committee in January 2017 (CEI-IB, #IB 3341/16 PI). The study was registered at ClinicalTrials.gov (ID no. NCT03250754) on 16 August 2017.
Participants
Electronic health record (EHR) data from patients with HDs referred to the pain clinic between January 2010 and December 2015 were retrospectively examined. Two researchers independently reviewed the demographic information and clinical diagnoses of these patients and selected those that met the following inclusion criteria: age ⩾ 18 years; clinical diagnosis of headache for over 12 months; and at least two headaches per month. The exclusion criteria were headache caused by somatic diseases and onset of headache or acupuncture treatment within the past year.
According to data from a 2009 clinical audit, three-quarters of the patients with HDs declined new prophylactic therapy because of the risk for adverse events (AEs) and requested non-pharmacological therapies. In light of the results obtained, the proportion of patients with a reduction in the number of headache days of at least 50% after 3 months of treatment was 57% in the acupuncture group and 41% in the PDT group, similar to previous studies.7,8 Data collected in the 2009 clinical audit were not included in this retrospective study. Considering these results and unbalanced design (3:1), 300 patients in the acupuncture group and 100 patients in the PDT group were considered to represent the minimum sample sizes required to detect a difference of at least 16% in the number of days with headache (NDH) between groups (β = 0.2; α = 0.05, two-sided). The pain clinic is visited annually by more than 90 patients with HDs. Patient data were de-identified and then analysed.
Interventions
The usual procedure in the pain clinic included recommendations to stop using abortive medications for headache only if medication overuse headache was diagnosed (regular overuse of one or more drugs that can be taken for acute treatment of headache for more than 3 months, with 10 days per month being enough for diagnosis). Withdrawal of the overused drug was the first step, along with pharmacological and non-pharmacological support. After a washout period of 2 weeks, a new treatment was provided to these patients. 9
All patients with HDs were appropriately evaluated by physicians who were not acupuncture practitioners. Patients were informed about the treatment options: PDT or acupuncture. The recommendations contained in the patient information fact sheet were reinforced at each subsequent visit (see patient information fact sheet in online Supplemental Figure 1, with recommendations for meditation, exercise, dietary instruction and information about the different HDs treatments). If the patient record were to indicate that they had crossed over, those data would be excluded from the current retrospective study.
PDT was offered if the patients met the inclusion criteria (accurate diagnosis, non-surgical treatment, no indication for other analgesic techniques or patient’s request) and no exclusion criteria (unclear diagnosis, surgical treatment, indication for other analgesic techniques, major psychiatric disorders, serious deterioration in health, medication intolerance or allergy), in order to treat multiple comorbid medical or psychiatric illnesses at the same time (e.g. patients with sleep disturbance, depression, neck pain, \hypertension and anxiety). Adequate as-needed treatment was given at the same time, with limits on usage to avoid medication overuse headache.
Acupuncture treatment inclusion criteria were: accurate diagnosis; non-surgical treatment; medication intolerance, allergy and/or comorbidity; no indication for other analgesic techniques; complementary treatment; or patient’s request. The exclusion criteria were: unclear diagnosis, surgical treatment, indication for other analgesic techniques, major psychiatric disorders, serious deterioration in health, coagulopathy, fever, or extensive and severe dermopathy. The needles were placed at specific pressure points, usually along a person’s head, neck and extremities. Treatment took about 30 min, and patients were advised to undergo at least 12 sessions, given over 3 months (preferably two sessions in each of the first 4 weeks, followed by one session every 15 days in the remaining 2 months).
Patients received and resolved doubts and questions about recommendations, and dietary instructions. They were informed of the likely benefits and risks of both treatments, before starting any treatment, and provided written informed consent that allowed the clinicians to proceed with the treatment procedures, including data collection. Treatment decision making was based on patient’s choice and fulfilling the inclusion/exclusion criteria.
PDT treatment was defined according to the guidelines of the British Association for the Study of Headache 10 : beta blockers (atenolol) and/or amitriptyline were the first choice for migraine prevention, topiramate and sodium valproate were second-line, and gabapentin was third-line. Amitriptyline was the treatment of choice in tension-type headache (TTH). Cluster headache (CH) prophylactic treatments included verapamil, lithium, valproic acid or topiramate. For trigeminal neuralgia (TN), carbamazepine and oxcarbazepine were first-line therapy, while lamotrigine and baclofen were considered second-line treatments. Anti-epileptics and tricyclic antidepressants were commonly used in occipital neuralgia, cervicogenic headache and post-surgery headache.
Electroacupuncture (EA) therapy was performed by anaesthesiologists with training in medical acupuncture and over 14 years experience.
Two types of needles (Shimmer, Wujiang Shenling Beauty Medical Appliance Co., Ltd., Suzhou, China) were used in all patients (25/30/40 mm x 0.25 mm and 13 mm × 0.20 mm).
Needling was applied at the sites of traditional acupuncture points, which were selected based on the consensus of acupuncture experts based on clinical experience (Table 1).
Framework of traditional acupuncture points that should be selected when administering acupuncture treatments by expert consensus.
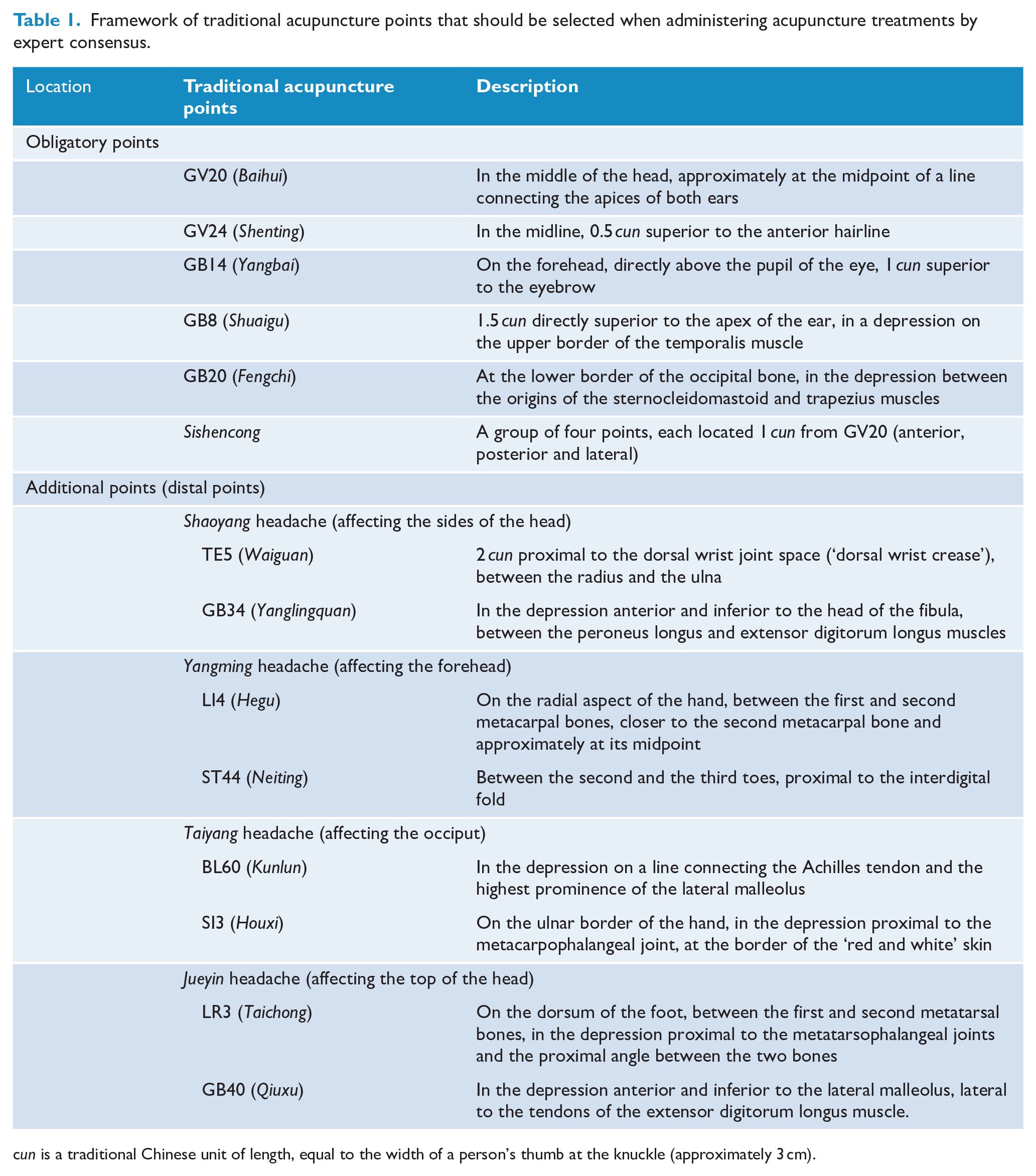
cun is a traditional Chinese unit of length, equal to the width of a person’s thumb at the knuckle (approximately 3 cm).
Additional individual point locations were chosen according to traditional syndrome differentiation based on classical meridian theory, according to the headache region: Shaoyang type headache, affecting the sides of the head; Yangming type headache, affecting the forehead; Taiyang type headache, affecting the occiput; and Jueyin type headache, affecting the top of the head. An EA device (model CNMS6-1; Wuxi Jiajian Medical Instrument Co., China) was connected to the needles inserted at distal points, with a dense-and-disperse mode of stimulation and at the maximum tolerable intensity.
The total number of needles was limited to 16 per session.
At GV20 (Baihui), GV24 (Shenting), GB14 (Yangbai) and GB8 (Shuaigu), needles were inserted obliquely under the galea aponeurotica and then turned horizontally with twirling. At all other point locations, needles were inserted perpendicularly then lifted, thrusted and twirled to obtain de qi sensation. The depth of needle insertion varied from 1 to 1.5 cm at the distal point locations.
Data collection
Patients’ data were extracted from the structured EHR and free text. The following information was extracted from each of the onscreen templates: age, sex, visual analogue scale (VAS) for pain, expectations, satisfaction, NDH, sleep quality, acute medication use and AEs of the acupuncture treatment. Data were recorded from patients’ questionnaires completed at baseline and after 1 and 3 months.
Physicians reported clinical diagnoses using the International Classification of Headache Disorders (ICHD) to differentiate between patients with migraine, TTH, trigeminal autonomic cephalgias (CH and Horton’s headache), TN, occipital neuralgia, cervicogenic headache and post-surgery headache (headache for at least 3 months caused by surgical craniotomy, developing within 7 days of craniotomy).
Unstructured free text fields were reviewed in order to extract information about medication and drop-outs; terms for describing AEs, dose and period for the PDT group, drop-outs and reasons for withdrawal were retrieved.
Outcome measurements
The primary outcome was the NDH (days with headache pain lasting 4 h with moderate or severe peak intensity) per month, and groups were compared at baseline and after 3 months. The percent reduction of headache days for each patient and number of treatment responders (defined as those experiencing a reduction of ⩾ 50%) were also calculated. 8
Secondary outcomes included VAS for pain (estimating the average severity of the headaches experienced in the month prior to the visit on a 0–10 scale, where 10 represents ‘very severe pain’ and 0 represents ‘no pain’). Satisfaction with treatment was measured by placing a mark on a 10 cm line that was labelled at each end with ‘not satisfied at all’ and ‘very satisfied’, respectively. Patient baseline and follow-up expectations (asking about ‘expectations of the treatment’ at baseline, using a 0–10 scale, where 10 represents ‘highest expectations’ and 0 represents ‘without expectation’; and asking whether ‘the results of your treatment were what you expected’ at 1- and 3-month follow-up, using a 0–10 scale, where, 10 represents ‘expectations were fully fulfilled’ and 0 represents ‘unfulfilled expectations’), sleep quality (quantified using a 0–10 scale where 10 represents ‘good quality’ and 0 represents ‘poor quality’) and acupuncture-associated AEs (perceived by patients and physicians) were recorded.
Dosage and AEs of pharmacological therapy, and drop-outs and reason for withdrawal, were recorded from unstructured free text fields.
Statistics
Data are presented as means ± standard deviations, medians (interquartile ranges) or numbers (percentages), unless otherwise specified. Intra-group data (at baseline, and 4 and 12 weeks) were analysed using analysis of variance (ANOVA) for repeated measures and post hoc Bonferroni tests for each group. For inter-group (acupuncture vs PDT) comparisons, an analysis of covariance (ANCOVA) for repeated measures, using age and baseline values as the covariates, was performed. For baseline and continuous variables, the optimal cut-off values associated with a greater than or equal to 50% decrease in headache days after 3 months were determined using receiver operator characteristic (ROC) curve analysis with the Youden’s index (maximum (sensitivity + specificity − 1)). Binary logistic regression was used to estimate the odds ratios (crude and adjusted by age and sex) of baseline variables using as dependent variable a decrease of more than 50% in headache days at 3 months (with respect to headache days at baseline).
A two-tailed p-value less than 0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 23.0 (SPSS Inc., Chicago, IL, USA).
Results
Participants and baseline characteristics
A total of 448 EHRs were reviewed. There were 446 participants meeting all the inclusion criteria, of which 342 (76.7%) formed the acupuncture group and 104 (23.3%) formed the PDT group (see online Supplemental Figure 2: Flowchart of patient inclusion). Six patients did not fulfil the inclusion criteria, 26 received other treatments (e.g. trigeminal nerve radiofrequency ablation, pulsed radiofrequency for occipital neuralgia) and 3 were excluded for other reasons (data errors).
Seven patients in the acupuncture group discontinued the intervention due to myocardial infarction (n = 1), surgical interventions (n = 2), inability to take time off work (n = 2) and missed appointments (n = 2). Eight patients in the PDT group discontinued the intervention due to AEs, and one patient missed appointments.
The two cohorts were comparable in terms of characteristics at baseline and types of HD (Table 2). A significant imbalance between the two groups was observed only with regard to age. There was a trend towards a difference in the percentage of females and in sleep quality.
Demographics and characteristics at baseline.
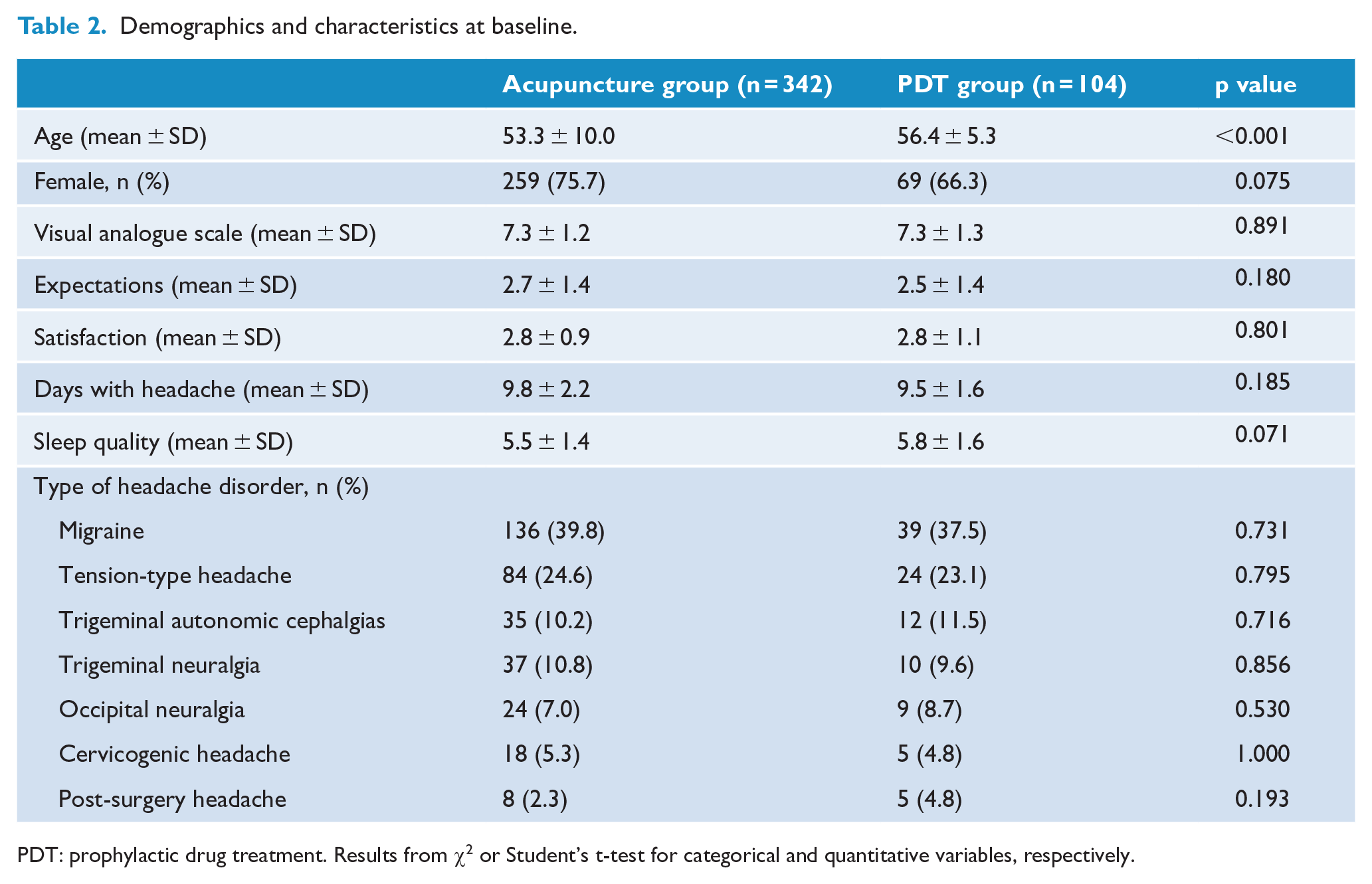
PDT: prophylactic drug treatment. Results from χ2 or Student’s t-test for categorical and quantitative variables, respectively.
Baseline pain VAS score was not significantly different between patients with the different types of headache (see online Supplemental Table 1: Demographics and characteristics at baseline for diagnostic groups).
Equivalence statistical testing was performed to compare drug and acupuncture arms at baseline in addition to null-hypothesis significance tests 11 (see online Supplemental Table 2).
Primary outcome
Between baseline and week 12, the NDH per month decreased by a mean ± SD of 3.7 ± 2.9 days in the acupuncture group versus 2.9 ± 2.3 days in the PDT group (p = 0.007). Values are baseline and age-adjusted (Table 3).
Outcome measurements.
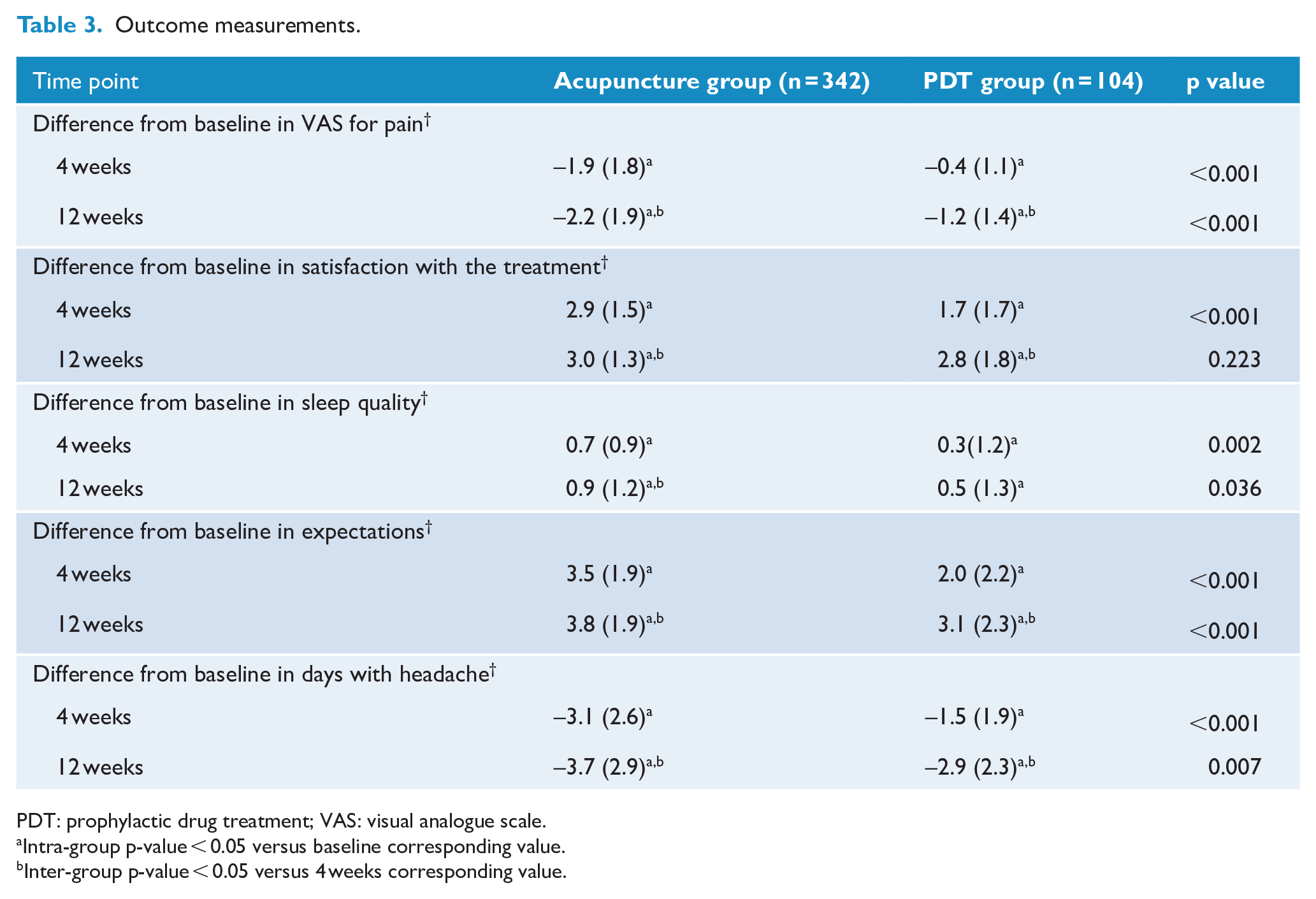
PDT: prophylactic drug treatment; VAS: visual analogue scale.
Intra-group p-value < 0.05 versus baseline corresponding value.
Inter-group p-value < 0.05 versus 4 weeks corresponding value.
The percent reduction of headache days was 36.6% (SD = 27.36) in the acupuncture group and 29.1% (SD = 22.10) in the PDT group (p < 0.001). The proportion of responders was 39.5% in the acupuncture group and 16.3% in the PDT group (p < 0.001); number needed to treat was 4; 95% confidence interval was 3 to 7 (Figure 1).
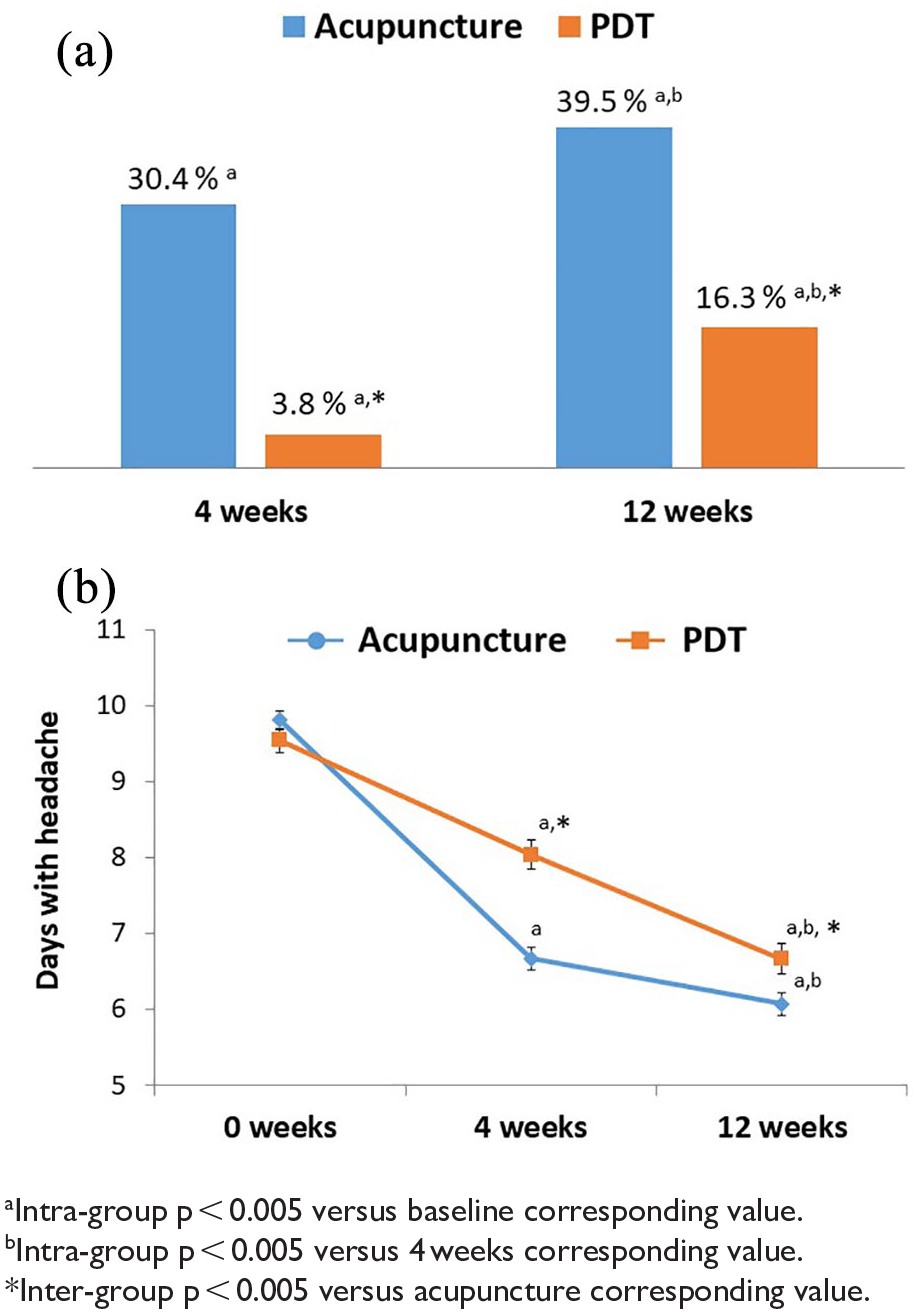
(a) Percentage of responders and (b) days with headache (mean ± SD).
Secondary outcomes
VAS for pain, assessment of satisfaction with treatment, expectations and sleep quality assessment scores were significantly in favour of the acupuncture group (vs the PDT group) at weeks 4 and 12.
The proportion of patients with acute medication intake reduced significantly in the acupuncture group compared with the PDT group at 4 and 12 weeks (39.5% vs 2.9% and 50% vs 5.8%, respectively; p < 0.001).
After adjusting by age, sex and acupuncture, sleep quality > 5, expectations > 2, headache days per month > 7.5, headache intensity (VAS for pain) < 7.5 and satisfaction with the treatment > 2.5 were the baseline patient characteristics associated with a > 50% decrease in headache days after 3 months (Figure 2).
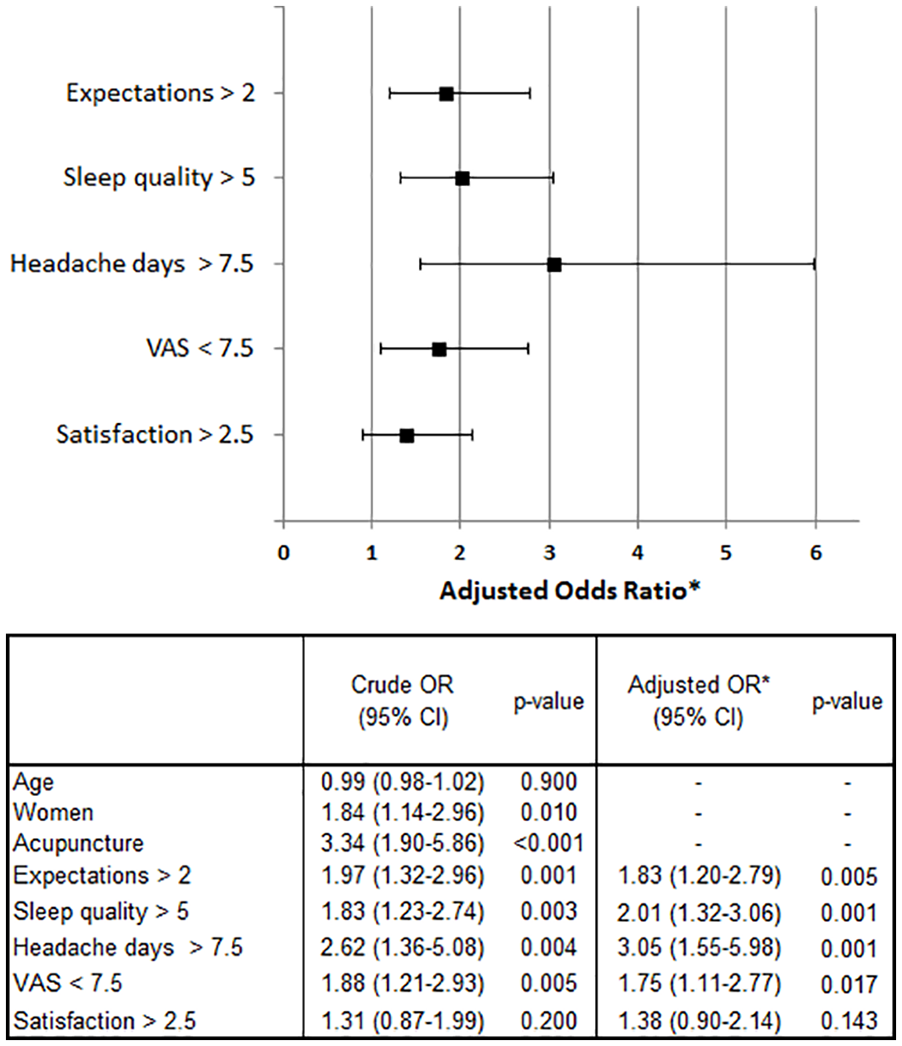
Binary logistic regression was used to estimate odds ratios (crude and adjusted by age and sex) of baseline variables using a >50% reduction in headache days after 3 months as the dependent variable. VAS, visual analogue scale.
Safety
Ninety-six patients (34 (9.9%) in the acupuncture group and 62 (59.6%) in the PDT group) reported AEs during the treatment period. Most AEs in the acupuncture group were related to the local insertion of the needle; 15 had minor local bleeding, 6 described local pain, 4 complained of local paraesthesia after needle insertion at the sites located on the head, 2 reported local infection, 3 suffered vasovagal syncope and 4 individuals experienced facial flushing, swelling, dizziness and loss of strength, respectively. All AEs were reported as mild or moderate, and no one discontinued prematurely the treatment because of needling related side effects.
One or more AEs were observed in 62 (59.6%) of the 104 patients with PDT treatment. The drugs, doses used in the regimens and the AEs of the different HDs are shown in online Supplemental Table 3. The AEs observed most frequently included dizziness (21%), dry mouth (21%) and weight gain (14.5%). Eight patients prematurely discontinued the treatment because of AEs.
Discussion
We have demonstrated that patients with HDs in tertiary care who chose treatment with acupuncture showed similar improvements in symptoms compared with patients who chose PDT. As such, the study demonstrates that acupuncture treatment can be incorporated within a pain clinic and that it is acceptable to a large percentage of patients with many types of refractory HDs.
This was a retrospective, non-randomised, observational study. Nonetheless, the study analysed a large number of patients in a tertiary hospital clinic under real-world conditions. Real-world evidence (RWE) is considered to better represent routine practice compared with the idealised conditions of a randomised control trial (RCT). Data from RWE studies can complement findings from RCTs and can provide valuable information about practice patterns and patient characteristics in a real-world setting.
In our study, acupuncture practitioners did not use Western diagnoses of headaches; HDs were treated according to ‘meridian’ diagnoses, traditional syndrome differentiation based on meridians in the headache region and localisation of the pain. HDs, from the point of view of traditional Chinese medicine (TCM), have differing treatments depending on pain localisation, in the same way the Western approach is based on the ICHD with different lines of treatment for each HD.
First, we wanted to compare the results of both approaches to the treatment of HDs as a whole. Second, we wanted to compare the results of both approaches according to the different types of headache included in the ICHD. Analysing HDs collectively could certainly be pragmatic from the Western medicine perspective as the physiopathology of the different types of HDs is very different, but TCM has its own diagnostic system. Following this premise, one in four of the patients with HDs treated with acupuncture, regardless of their classification, showed significant improvements in clinical outcome measures.
We found that acupuncture was similarly effective to PDT for HD prophylaxis. Our findings were congruent with those of previous clinical trials.12,13
Safety is an important consideration in the management of chronic conditions such as HDs. Acupuncture showed mild adverse effects in the treatment of HDs, similar to other studies 7 ,8,14 and no patients discontinued the treatment.
Over half of the PDT patients had AEs, necessitating changes in treatment or prompting premature discontinuation of treatment.
Another important finding of this study is the determination of an optimal cut-off basal value for discriminating patient responders from non-responders. These results are consistent with the idea that those patients with a positive attitude, high expectations and better sleep quality respond better to treatment. 15
Patient perceived quality of life and state of anxiety and depression were not measured in this study. For this reason, it would be difficult to determine the effectiveness of the treatment without acknowledging the possible influence of different emotional states.
Although the data indicate that acupuncture is more than a placebo, factors in addition to the specific effects of needling are important contributors to therapeutic effects. 16 However, it is important not to forget that it is becoming clear that any treatment is significantly modulated by placebo effects in clinical settings. 17 On the contrary, the placebo effect in episodic migraine prophylaxis is usually in the 20%–40% range, and in some trials, it has been even higher. 18
The strengths of our study are the design19,20 with a large sample size, thorough statistical analysis, the evaluation of treatments under conditions approximating usual care and the description of the acupuncture intervention. 21
Weaknesses include the non-randomised design (which, despite contributing to the high external validity of the data, reduces its internal validity), the use of self-reported questionnaires rather than a diary format (recognizing that, in routine care situations with large number of patients, formal diaries may not be practical) and treatment decision making based on patients’ choice (which could have introduced bias towards acupuncture treatment).
Conclusion
In summary, given a choice between acupuncture and PDT, a substantial majority of patients chose acupuncture and, in so doing, achieved similar clinical outcomes as did those patients who chose PDT. Given the risk profile of most PDTs, using an arguably safer treatment paradigm while attaining similar clinical results is an important finding. We suggest that future studies with a greater number of patients, and powered for subgroup analysis by type of HD, might shed further light on the effects of acupuncture in neuralgias, especially those that do not respond to conventional treatments.
Supplemental Material
sj-doc-3-aim-10.1177_0964528420987571 – Supplemental material for Treatment of headache disorders with acupuncture: a 6-year retrospective study
Supplemental material, sj-doc-3-aim-10.1177_0964528420987571 for Treatment of headache disorders with acupuncture: a 6-year retrospective study by Javier Mata, Pilar Sanchís, Pedro Valentí, Beatriz Hernández and Jose Luis Aguilar in Acupuncture in Medicine
Supplemental Material
sj-doc-4-aim-10.1177_0964528420987571 – Supplemental material for Treatment of headache disorders with acupuncture: a 6-year retrospective study
Supplemental material, sj-doc-4-aim-10.1177_0964528420987571 for Treatment of headache disorders with acupuncture: a 6-year retrospective study by Javier Mata, Pilar Sanchís, Pedro Valentí, Beatriz Hernández and Jose Luis Aguilar in Acupuncture in Medicine
Supplemental Material
sj-doc-5-aim-10.1177_0964528420987571 – Supplemental material for Treatment of headache disorders with acupuncture: a 6-year retrospective study
Supplemental material, sj-doc-5-aim-10.1177_0964528420987571 for Treatment of headache disorders with acupuncture: a 6-year retrospective study by Javier Mata, Pilar Sanchís, Pedro Valentí, Beatriz Hernández and Jose Luis Aguilar in Acupuncture in Medicine
Supplemental Material
sj-jpg-2-aim-10.1177_0964528420987571 – Supplemental material for Treatment of headache disorders with acupuncture: a 6-year retrospective study
Supplemental material, sj-jpg-2-aim-10.1177_0964528420987571 for Treatment of headache disorders with acupuncture: a 6-year retrospective study by Javier Mata, Pilar Sanchís, Pedro Valentí, Beatriz Hernández and Jose Luis Aguilar in Acupuncture in Medicine
Supplemental Material
sj-png-1-aim-10.1177_0964528420987571 – Supplemental material for Treatment of headache disorders with acupuncture: a 6-year retrospective study
Supplemental material, sj-png-1-aim-10.1177_0964528420987571 for Treatment of headache disorders with acupuncture: a 6-year retrospective study by Javier Mata, Pilar Sanchís, Pedro Valentí, Beatriz Hernández and Jose Luis Aguilar in Acupuncture in Medicine
Footnotes
Acknowledgements
The authors would like to thank Dr Gemma Rialp and Dr Mike Cummings for performing critical review of the manuscript. They did not receive compensation for their contributions.
Contributors
JM, PS and PV conceived the study. JM, PV and BH were in charge of subject recruitment, treatment and data collection. JM and PS had full access to all the data in the study and take responsibility for data analysis. JM and JLA drafted the manuscript. All authors read the manuscript and approved the final version accepted for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Data availability
doi:10.17632/kvfc3jxz2k.2
Trial registration
NCT03250754 (ClinicalTrials.gov) – observational study
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.