
Abstract
Objective:
To screen for differentially expressed serum microRNAs (miRNAs) in patients with diarrhea-predominant irritable bowel syndrome (IBS-D) compared with healthy participants and explore the mechanism of acupuncture in the treatment of IBS-D based on miRNAs.
Methods:
IBS-D patients that met the Rome III diagnostic criteria and age- and sex-matched healthy participants were enrolled between April 2017 and December 2017. Serum miRNA levels were initially determined using a TaqMan low-density array (TLDA) in pooled samples. Markedly altered miRNAs in IBS-D patients were subsequently validated using quantitative real-time polymerase chain reaction (qRT-PCR) on individual samples. All IBS-D patients accepted the acupuncture therapy for 6 weeks. The disease severity was assessed using the IBS symptom severity scale (IBS-SSS) questionnaire before and after treatment. After acupuncture, the patients’ serum was re-analyzed for altered expression of the miRNAs by qRT-PCR.
Results:
TLDA and qRT-PCR analysis revealed six upregulated miRNAs (miR-1305, miR-575, miR-149-5p, miR-190a-5p, miR-135a-5p, and miR-148a-3p; P < 0.05) and two downregulated miRNAs (miR-194-5p, miR-127-5p; P < 0.05) in IBS-D patients compared with healthy controls. Post acupuncture treatment, total IBS-SSS scores, severity of abdominal pain, duration of abdominal pain, severity of abdominal distention, dissatisfaction with bowel habits and disruption in quality of life decreased significantly (P < 0.001). Furthermore, the upregulated miR-148a-3p levels in IBS-D patients also decreased significantly after acupuncture (P < 0.05).
Conclusions:
The over-expression or reduced expression of several miRNAs may contribute to IBS-D pathogenesis. Acupuncture might downregulate miR-148a-3p through multiple pathways to alleviate or relieve IBS-D symptoms.
Trial registration number:
ChiCTR-IOR-17010860 (Chinese Clinical Trials Registry)
Introduction
Irritable bowel syndrome (IBS) is a chronic, relapsing functional gastrointestinal disorder that is mostly characterized by abdominal pain associated with stool irregularities. IBS is estimated to affect approximately 11.2% of adults worldwide. 1 The main IBS subtype is diarrhea-predominant irritable bowel syndrome (IBS-D), which accounts for one-third of the affected population. 2 The underlying pathogenesis of IBS-D includes visceral hypersensitivity, abnormal brain–gut interaction, alterations in the gut microbiota, intestinal mucosal immune activation, and increased intestinal permeability. 3
MicroRNAs (miRNAs) are small non-coding RNAs with 19–24 nucleotides that are thought to be involved in gene regulation after transcription. 4 Recent evidence suggests that miRNAs may play a regulatory role in the pathogenesis of IBS-D. Research has shown that upregulated miR-29a and downregulated miR-125b and miR-16 are associated with increased intestinal permeability.5,6 Decreased colonic miR-199 was reported to correlate with visceral pain in patients with IBS-D. 7 Another study reported that miR-200a may induce visceral hyperalgesia by downregulation of cannabinoid receptor 1 and serotonin reuptake transporter (SERT). 8 However, previous studies have explored the relationship of only one or two miRNAs with IBS.
Acupuncture is considered to be beneficial for IBS-D and is increasingly accepted worldwide.9,10 Our previous studies have shown that acupuncture has the capacity to improve several symptoms, including abdominal pain, diarrhea, and bloating.11,12 Although several animal experiments have revealed that acupuncture is effective in IBS through the regulation of visceral hypersensitivity, the brain–gut axis, gastrointestinal motility, and immunological function,13–20 the mechanism of acupuncture in the treatment of IBS-D still has not yet been fully described.
This study aimed to examine the different expression profiles of serum miRNA in patients with IBS-D compared with healthy participants using TaqMan low-density array (TLDA) and individual quantitative real-time polymerase chain reaction (qRT-PCR). Furthermore, changes in the expression of miRNAs before and after acupuncture treatment were evaluated. We anticipated that our results would provide a better understanding of the pathophysiological features of patients with IBS-D and further clarify the mechanism of acupuncture in treating IBS-D based on miRNAs.
Methods
Participants
IBS-D patients and healthy participants for this non-randomized clinical trial were recruited from the Jiangsu Province Hospital of Chinese Medicine and surrounding communities. This trial was registered in the Chinese Clinical Trials Registry (ref. ChiCTR-IOR-17010861) on 14 March 2017. Ethical approval was obtained from the ethics committee of Jiangsu Province Hospital of Chinese Medicine (2016NL-079-03). Participants in this trial provided written informed consent.
IBS-D patients were eligible if they: fulfilled the Rome III diagnostic criteria for IBS-D; were 18 to 70 years old; had a duration of symptoms of 6 months or longer; lacked morphological changes and biochemical abnormalities that could otherwise explain the symptoms; had a baseline total IBS symptom severity scale (IBS-SSS) score of 75 points or greater; and agreed to participate and sign an informed consent. The exclusion criteria were diagnosis of an organic intestinal disease, history of abdominal or rectal surgery, history of drug treatment affecting gastrointestinal motility and function, other serious medical conditions, such as cardiovascular disease, endocrine disorders, hepatic dysfunction, cerebral vascular disease, renal disease, cognitive disorders, pregnancy, lactation, and being less than 12 months postpartum.
Healthy participants were sex and age matched with the recruited IBS-D patients. The study was performed according to the principles of the Declaration of Helsinki.
Interventions
All patients were advised to follow their routine lifestyles, continue a regular diet and maintain emotional stability during the study period. It was also suggested that they avoid the intake of any food that had previously affected the individual’s symptoms. Patients were asked not to take antispasmodics, antidiarrheal agents, antidepressants, probiotics, or traditional Chinese medicine (TCM) herbs focusing on relieving IBS-D symptoms during treatment. If any related medications were taken, the name and dosage were documented in the case report form. Patients with IBS-D received acupuncture three times a week for 6 weeks for a total of 18 treatment sessions. Disposable, sterile needles with a diameter of 0.30 mm and length of 40 mm (Huatuo, Suzhou, China) were inserted at GV20 (Baihui), Yintang, LR3 (Taichong), ST36 (Zusanli), SP6 (Sanyinjiao), ST25 (Tianshu), and ST37 (Shangjuxu). After insertion, all needles were manually stimulated by lifting and thrusting every 10 min to elicit de qi sensation—a sensation of soreness, numbness, heaviness, and bloating. The needles were retained for 30 min.
Healthy participants in the control group received no treatment.
Sample collection
Every healthy participant and IBS-D patient was asked to provide blood samples on an empty stomach in the morning. The blood from healthy controls was collected only once, while that from the IBS-D patients was collected before and after the treatment. The blood was centrifuged at 2683 g and 4°C for 10 min. Then, the serum supernatant was collected and stored at −80°C until RNA extraction.
RNA isolation, TLDA, and qRT-PCR
For TLDA, total RNA was extracted using TRIzol reagent (Invitrogen, Carlsbad, CA, USA) from two pooled samples from the 23 IBS-D patients or 19 healthy participants (each serum sample was 10 mL) and purified with mirVana miRNA isolation kits (Ambion, Austin, TX, USA) according to the manufacturer’s protocol. The miRNAs were reverse transcribed using Megaplex primer pools (human pools A and B) from Applied Biosystems (Foster City, CA, USA). The reverse transcription reaction products were further amplified using Megaplex PreAmp primers (primers A and B). The expression profile of miRNAs in each sample was determined using Human TaqMan miRNA arrays A and B (Applied Biosystems). PCR was performed using 450 μL of the TaqMan Universal PCR Master Mix No AmpErase UNG (2×) and 9 μL of the diluted pre-amplification product to a final volume of 900 μL. Then, 100 μL of the PCR mix was dispensed to each port of the TaqMan miRNA array. The fluidic card was centrifuged and mechanically sealed, then qRT-PCR was carried out on an ABI PRISM 7900HT sequence detection system (Applied Biosystems) using the manufacturer’s recommended program. The concentrations of the miRNAs were presented as cycle threshold (Ct) values.
For qRT-PCR, the total RNA was extracted from 100 μL individual serum samples using a phenol/chloroform purification protocol. Key miRNAs were selected for validation using qRT-PCR. A TaqMan probe-based qRT-PCR assay was conducted on a 7300 sequence detection system (Applied Biosystems). Briefly, 0.25 μg of total RNA was reverse transcribed using miRNA-specific RT primers, MMLV reverse transcriptase, RT buffer, dNTPs, RNase inhibitor, and RNase-free water under the following conditions: 16°C for 30 min; 42°C for 30 min; and 85°C for 5 min. After synthesizing cDNA, qRT-PCR was performed under the following conditions: 95°C for 5 min followed by 40 cycles of 95°C for 15 s and 60°C for 1 min. RNU6B (Applied Biosystems) was used as the internal control. The miRNA expression levels were calculated using the comparative Ct method (2−ΔCt).
Clinical effectiveness assessment
The clinical effectiveness of acupuncture in this trial was determined using the IBS-SSS. 21 The questionnaire was scored from 0 to 500 and was composed of five 100-point scales that measured the severity of abdominal pain, duration of abdominal pain, severity of abdominal distention, dissatisfaction with bowel habits and disruption in quality of life (QoL). IBS-SSS was assessed at baseline and 6 weeks after treatment.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS Inc., Chicago, IL, USA). For numerical variables, between-group comparisons were assessed using t-tests or Wilcoxon rank-sum tests as appropriate. Chi-square tests or Fisher’s exact tests were used for categorical variables. For TLDA chip analysis, miRNAs with raw Ct scores greater than 37 were excluded. Significance analysis of microarrays (SAM) version 3.02 was used to determine the significant differentially expressed miRNAs. Fold changes were determined by dividing 2−ΔCt of IBS-D patients by that of healthy controls. The miRNAs in the assessed IBS-D samples were considered to be upregulated if the fold change was ⩾2.0 and downregulated if the fold change was ⩽ 0.5 compared with the healthy control group. Pearson’s coefficients were calculated between the change in miRNAs and the change in total IBS-SSS. A two-sided P value of <0.05 was considered statistically significant. Data are presented as mean ± SD unless otherwise stated.
Results
Participant characteristics
A total of 23 IBS-D patients (41.0 ± 12.35 years old; 56.5% male) and 19 healthy participants (36.6 ± 8.73 years old; 57.9% male) were enrolled in the study between April 2017 and December 2017. All 23 patients completed the 6 week treatment, without anyone dropping out. Baseline characteristics were similar between the IBS-D patients and healthy controls (Table 1).
Participant characteristics.
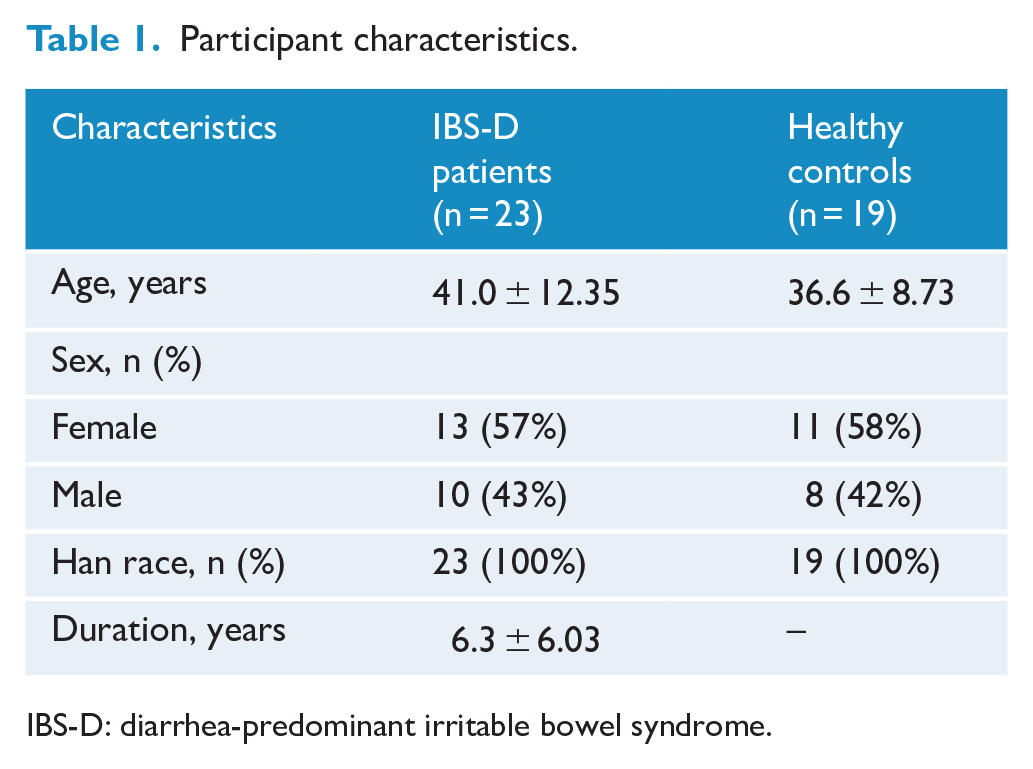
IBS-D: diarrhea-predominant irritable bowel syndrome.
Clinical effectiveness
At the end of the 6-week treatment, the scores of total IBS-SSS, severity of abdominal pain, frequency of abdominal pain, severity of abdominal distension, satisfaction with bowel habits, and interference of IBS with QoL decreased significantly (P < 0.001; Table 2).
Clinical effectiveness assessed by IBS-SSS scores.
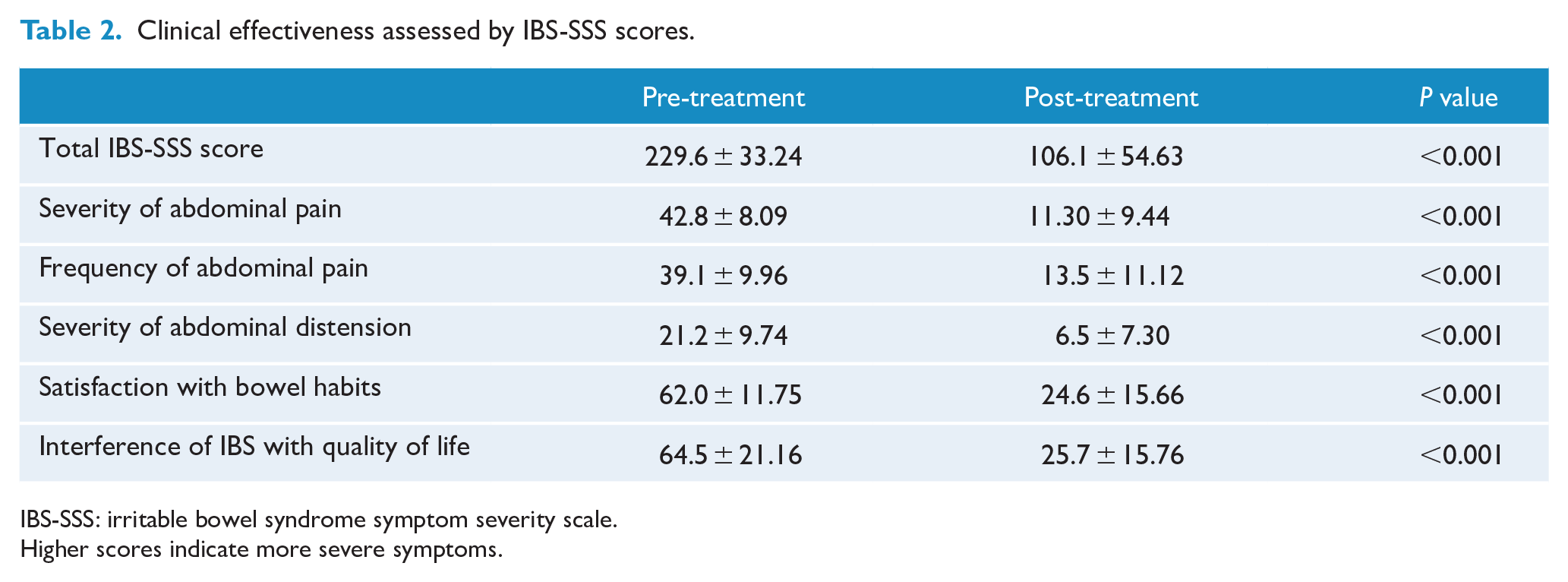
IBS-SSS: irritable bowel syndrome symptom severity scale.
Higher scores indicate more severe symptoms.
TLDA chip analysis of serum miRNA profiles
Of the 747 miRNAs tested, 172 miRNAs were differentially expressed; 69 miRNAs were upregulated, and 103 miRNAs were downregulated in the IBS-D group compared with the healthy control group. Twelve of the markedly altered miRNAs (fold change >100 or <0.01) are listed in Table 3.
Markedly altered miRNAs in pooled serum samples from IBS-D patients compared with those from healthy participants as determined by TaqMan low-density array.
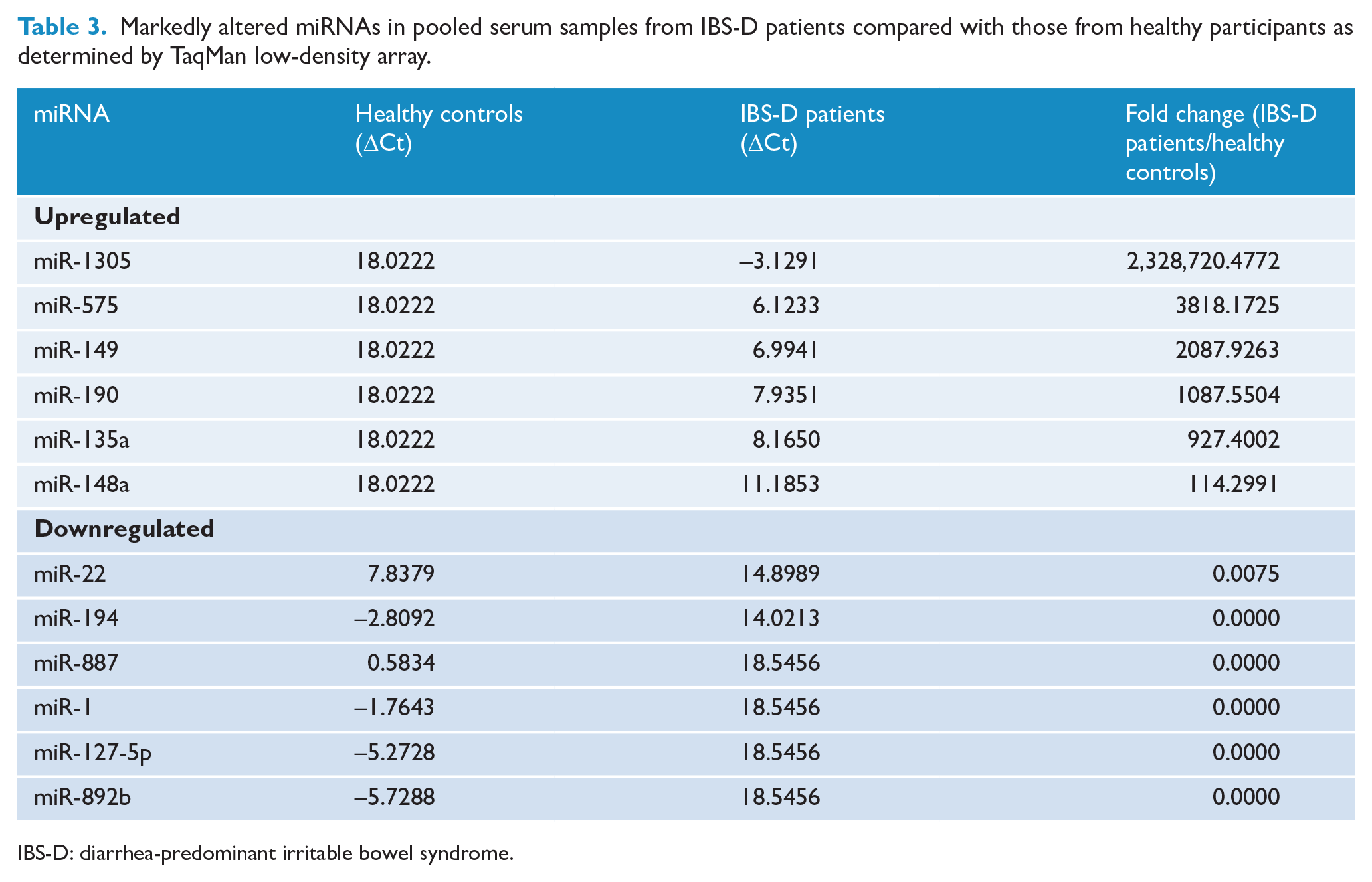
IBS-D: diarrhea-predominant irritable bowel syndrome.
Confirmation of the TLDA results using individual qRT-PCR
To confirm the TLDA results, qRT-PCR of miRNAs was carried out using individual serum samples. Of the 12 miRNAs, six miRNAs (miR-1305, miR-575, miR-149-5p, miR-190a-5p, miR-135a-5p, and miR-148a-3p) were upregulated (P < 0.05), while two miRNAs (miR-194-5p and miR-127-5p) were downregulated (P < 0.05) in IBS-D patients compared with the healthy controls (Figure 1).
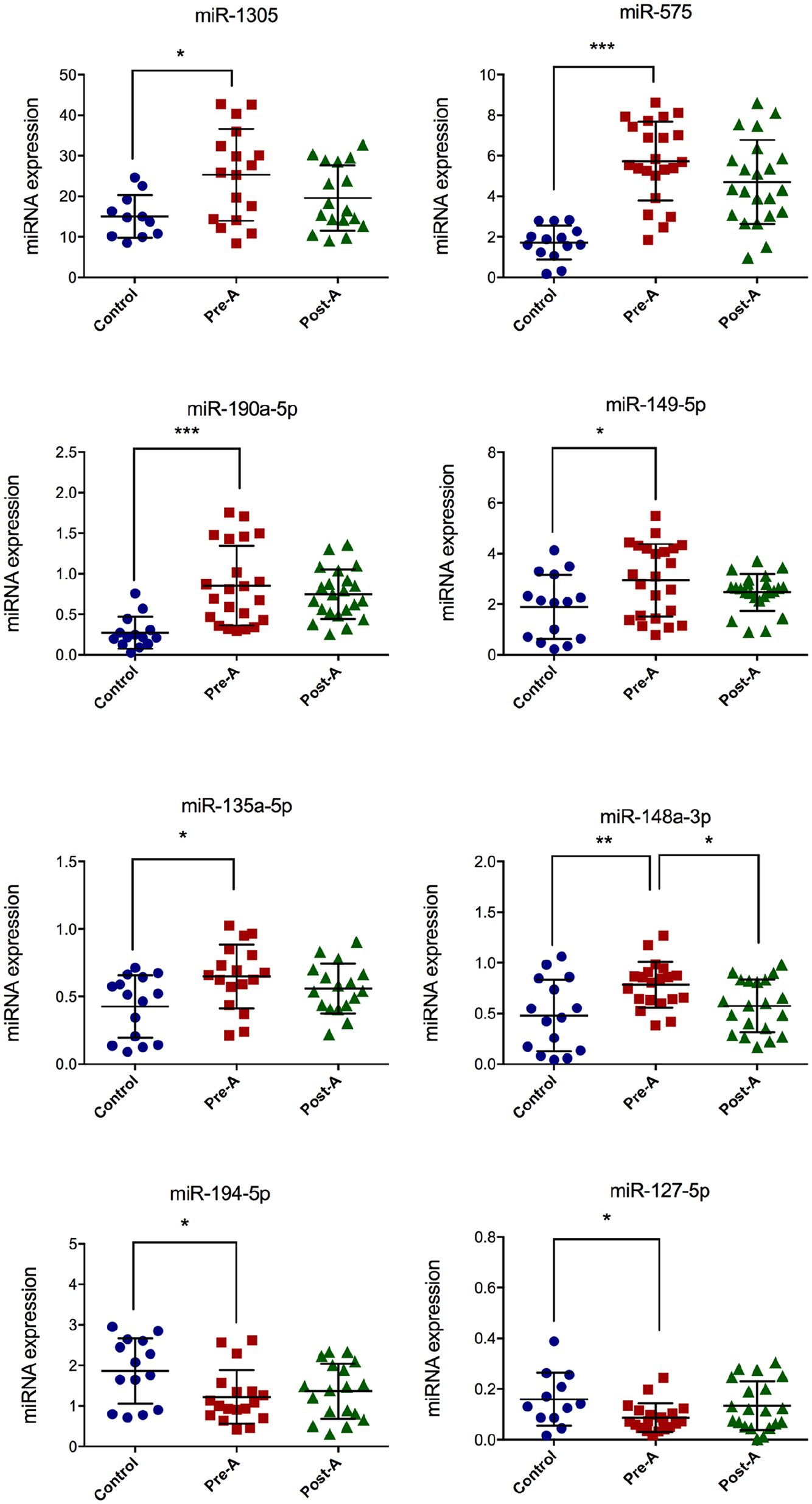
The expression of markedly altered miRNAs assessed by qRT-PCR. The miRNA expression levels were calculated using the comparative Ct method (2−ΔCt). Control, healthy control; Pre-A, before acupuncture treatment; Post-A, after acupuncture treatment. *P < 0.05; **P < 0.01; *** P < 0.001.
Differential expression of serum miRNAs related to acupuncture treatment
The serum samples of IBS-D patients after acupuncture treatment were also assessed by qRT-PCR. The results showed that the upregulated miR-148a-3p in IBS-D patients decreased significantly after acupuncture (P < 0.05). However, the other seven differentially regulated miRNAs showed no significant difference after acupuncture treatment (P > 0.05; Figure 1).
Correlation coefficients of change in miR-148a-3p and total IBS-SSS
Before acupuncture treatment, Pearson’s correlation analysis showed that miR-148a-3p was weakly positively related to the total IBS-SSS score (r = 0.52, P < 0.05). However, there was no significant correlation between the change in miR-148a-3p and the change in total IBS-SSS (r = 0.41, P > 0.05; Figure 2).
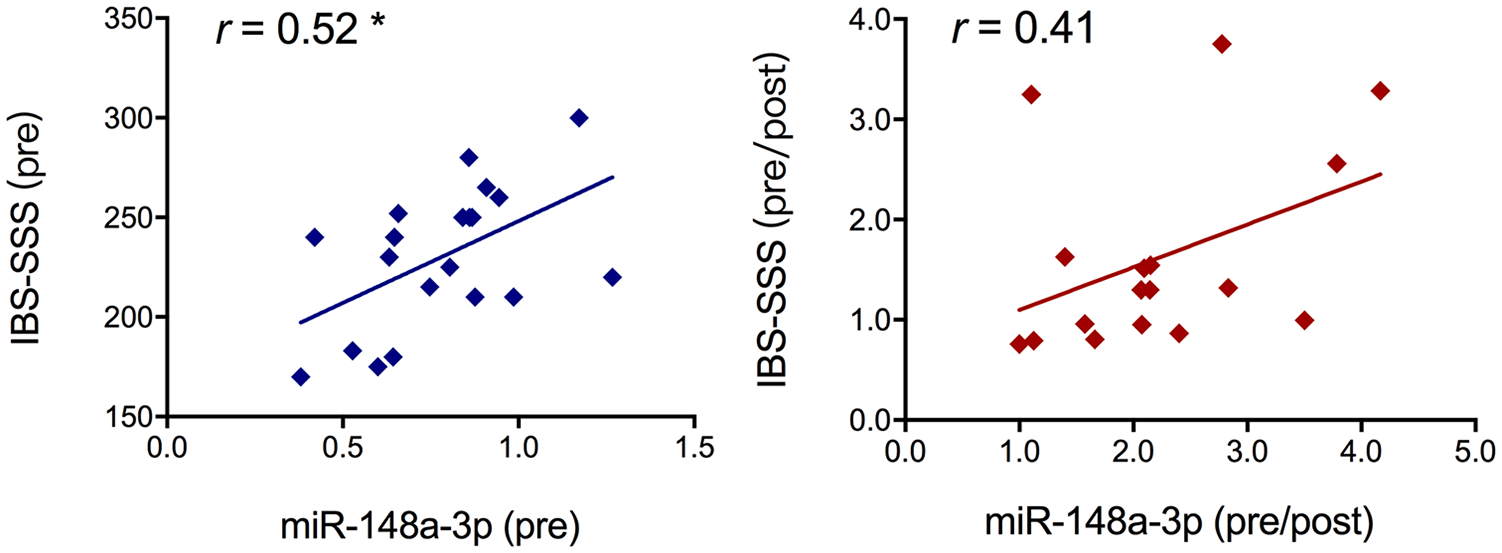
Scatterplot of serum miR-148a-3p expression versus irritable bowel syndrome symptom severity scale (IBS-SSS) scores (left panel) and change in miR-148a-3p versus change in IBS-SSS scores (right panel). The figure shows the regression line with r values indicating Pearson’s correlation coefficients. Pre, before acupuncture treatment; Post, after acupuncture treatment; *P < 0.05.
Prediction of miR-148a-3p target genes and enrichment analysis
Single miRNAs can regulate many target genes after transcription and ultimately act as modulators of multiple cellular pathways. To predict the target genes of miR-148a-3p, we carried out an online search for “miRNA targets” using TargetScan and miRDB. To gain insights into miR-148a-3p, we carried out a function and pathway analysis using the GO (Gene Ontology) and KEGG (Kyoto Encyclopedia of Genes and Genomes) databases on the online software DAVID (Database for Annotation, Visualization and Integrated Discovery). As demonstrated in Supplemental Figure S1, the annotations of genes were divided into three domains, namely biological processes, molecular function, and cell components. GO analysis indicated that for the biological processes annotation, the target genes were mainly enriched in neuron recognition (GO:0008038), axonal fasciculation (GO:0007413), cell migration involved in sprouting angiogenesis (GO:0002042), phosphatidylinositol dephosphorylation (GO:0046856), and sprouting angiogenesis (GO:0002040). KEGG pathway enrichment analysis showed that these candidate genes were enriched in multiple signaling pathways, such as transforming growth factor (TGF)−β, p53, insulin, B-cell receptor, gonadotropin-releasing hormone (GnRH), and adipocytokines (Figure 3).
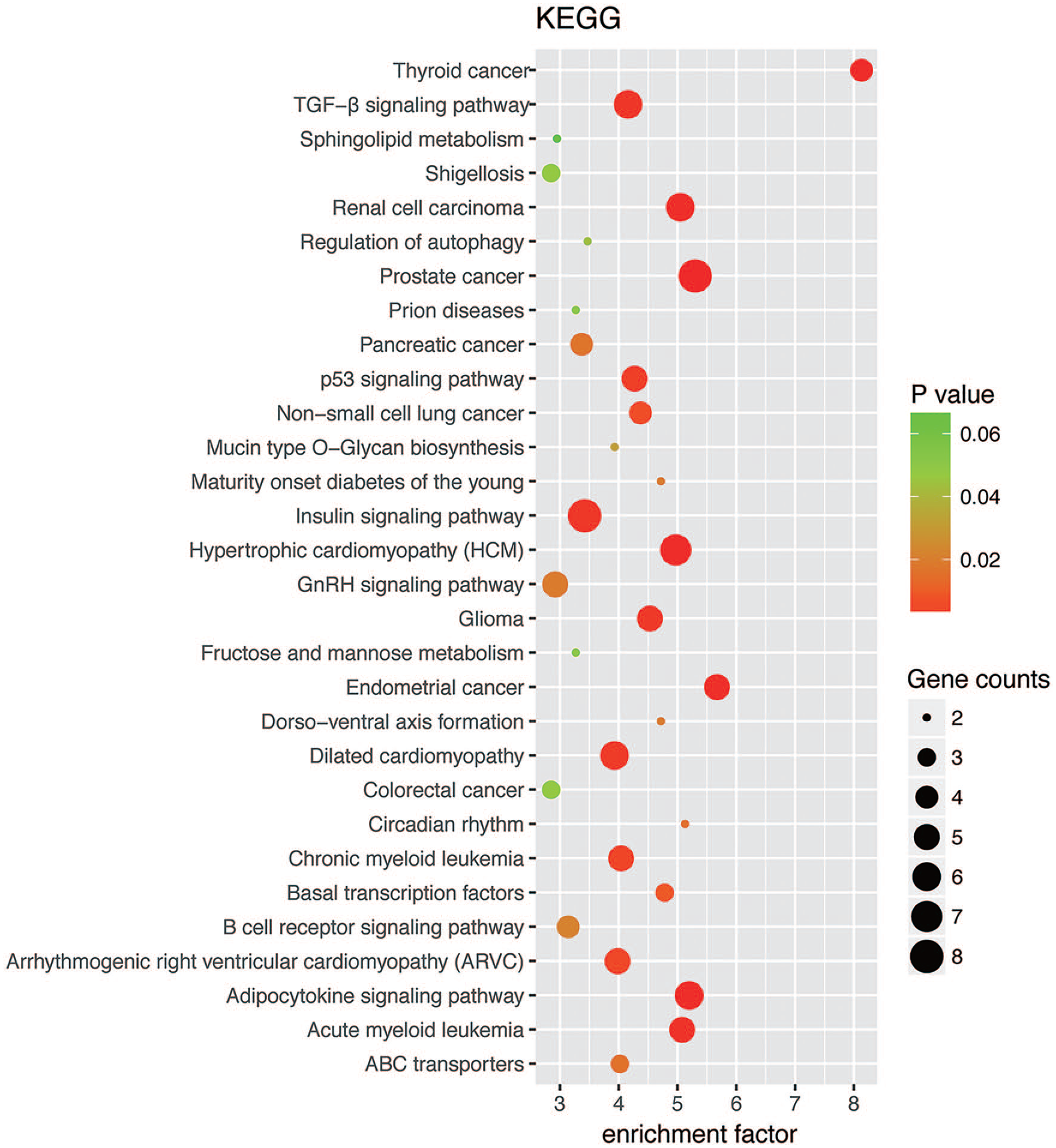
Statistics of KEGG (Kyoto Encyclopedia of Genes and Genomes) database enrichment.
Discussion
In this study, TLDA chip and individual qRT-PCR analyses indicated that eight miRNAs were differently expressed in IBS-D patients compared with age- and sex-matched healthy participants; the expression of six miRNAs was upregulated (miR-1305, miR-575, miR-149-5p, miR-190a-5p, miR-135a-5p, and miR-148a-3p), while that of two miRNAs (miR-194-5p and miR-127-5p) was downregulated. Acupuncture appeared to be effective at improving IBS-D symptoms, given the associated reduction in total IBS-SSS scores. After acupuncture treatment, the upregulated miR-148a-3p also decreased significantly.
The over-expression of miR-1305 has been demonstrated to induce differentiation of pluripotent stem cells. 22 We speculated that high levels of expression of miR-1305 might be associated with the mechanism of IBS-D pathogenesis by disrupting the balance of pluripotency and decreasing cell survival. MiR-575 has been reported to be an oncogene that promotes gastric cancer progression. 23 It has been reported that miR-149-5p and miR-190a-5p are associated with several kinds of cancer.24–26 However, the correlation between miR-1305, miR-575, miR-149-5p, miR-190a-5p, and IBS-D needs to be studied in the future.
Previously, it was shown that over-expression of miR-135 inhibits the transcription of genes associated with the 5-hydroxytryptamine (5-HT) signaling system, reduces the expression of SERT (a transporter for uptake of synaptic 5-HT) and increases the 5-HT content between synapses, thus alleviating depression. 27 Changes in the central and gastrointestinal 5-HT signaling system could lead to visceral hypersensitivity in IBS. 28 A lack of SERT could lead to increased activation of the 5-HT receptor and enhanced effects of 5-HT and cause gastrointestinal dysfunction. 29 Furthermore, IBS patients may also display emotional symptoms such as anxiety or depression. Based on these findings and our results, we speculate that miR-135 functions upstream of the 5-HT signaling system, which is closely related to IBS pathogenesis.
In contrast to the aforementioned miRNAs, the expression of miR-194-5p and miR-127-5p was found to be reduced in IBS-D patients. A recent study indicated that laryngeal cancer was correlated with downregulation of miR-194-5p. 30 It was reported that there was a significant reduction in miR-127-5p expression in the osteoarthritic cartilage compared with normal cartilage; in addition, miR-127-5p has been reported to suppress the interleukin (IL)-1β-induced activation of nuclear factor (NF)-κB. 31 Although, to our knowledge, there are no studies exploring the relationship between miR-127-5p and IBS-D, we speculate that the downregulation of miR-127-5p may fail to suppress the inflammatory process, which might contribute to IBS-D pathogenesis.
As an important component of TCM, acupuncture has been used to treat IBS and alleviate its symptoms for several decades. A systematic review indicated that, in comparative Chinese trials, patients reported greater benefits from acupuncture than from pharmacological therapies. 9 Acupuncture could reduce overall IBS symptom severity and improve health-related quality of life. Although this was not a randomized controlled investigation, the results of our study are broadly consistent with these findings; acupuncture appeared to be effective at improving IBS-D symptoms and was associated with reduced total IBS-SSS scores. Notably, after acupuncture treatment, the upregulated miR-148a-3p in IBS-D patients decreased significantly. The expression levels of miR-148a-3p prior to acupuncture were positively correlated with total IBS-SSS scores, and therefore, might be indicative of the severity of IBS. However, the acupuncture-induced change in miR-148a-3p was not significantly correlated with the change in total IBS-SSS scores. Nonetheless, considering the small sample size of our study, we cannot rule out the possibility that, given a big enough sample size, there might be a significantly positive correlation between the changes in miR-148a-3p and markers of clinical efficacy.
To obtain insights into the role of miR-148a-3p, we carried out GO analysis, which demonstrated that the target genes were associated with complex biological processes, such as neuron recognition and axonal fasciculation. KEGG pathway enrichment analysis showed that these candidate genes were enriched in multiple signaling pathways, such as TGF−β, p53, insulin, B-cell receptors, GnRH, and adipocytokine. To our knowledge, there have been no reports indicating a relationship between IBS-D and any of aforementioned signaling pathways. Abnormal TGF-β signaling activities have been connected to a variety of diseases, such as cancer, fibrosis, and inflammation. 32 We hypothesized that acupuncture might downregulate miR-148a-3p to suppress inflammation via the TGF−β signaling pathway. KEGG pathway enrichment analysis also showed that miR-148a-3p could regulate the nucleotide-binding oligomerization domain (NOD)-like receptor and Toll-like receptor (TLR) signaling pathways. Several studies have indicated that these receptors play an important role in the pathogenesis of IBS.33,34 The decreased expression of NOD-like receptor pyrin domain-containing protein 6 (NLRP6) expression, along with increased expression of IL-1β and IL-18 was associated with IBS colonic inflammation. 35 The expression of TLR4 was upregulated in the colonic mucosa of IBS patients and rat models of visceral hypersensitivity.36,37 Electroacupuncture could ameliorate the visceral hypersensitivity of IBS model rats by down-regulating TLR4 expression. 37 Taken together, we speculate that acupuncture might regulate miR-148a-3p through multiple pathways to alleviate IBS symptoms. Further studies are needed to explain the specific mechanism of acupuncture in the regulation of miRNAs to treat IBS.
Conclusion
This study revealed an association of some miRNAs with the pathogenesis of IBS-D. The symptoms of patients with IBS-D appeared to be improved by acupuncture therapy, which may promote downregulation of miR-148a-3p. Further studies are required to clarify the specific mechanism underlying the regulation of miR-148a-3p by acupuncture in the treatment of IBS-D.
Supplemental Material
sj-docx-1-aim-10.1177_09645284211027892 – Supplemental material for Regulation of serum microRNA expression by acupuncture in patients with diarrhea-predominant irritable bowel syndrome
Supplemental material, sj-docx-1-aim-10.1177_09645284211027892 for Regulation of serum microRNA expression by acupuncture in patients with diarrhea-predominant irritable bowel syndrome by Jing Guo, Gao Lu, Lu Chen, Hao Geng, Xiaoliang Wu, Hao Chen, Yang Li, Mengqian Yuan, Jianhua Sun and Lixia Pei in Acupuncture in Medicine
Footnotes
Contributors
All authors contributed to the study concept and design. G.L., C.L., H.G., X.W.,and M.Y. were responsible for acquisition of the clinical data. J.G. did the main statistical analysis. H.C. and Y.L. contributed to the literature review and interpretation of the data. J.G. and G.L. contributed to drafting of the report. J.S. and L.P. provided administrative, technical and material support, and supervised the study. All authors revised the text for intellectual content and have read and approved the final version of the manuscript accepted for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Project of Jiangsu Provincial Administration of Traditional Chinese Medicine (grant no. JD201506); Jiangsu Postgraduate Practice Innovation Program (grant no. SJCX21_0737); National Natural Science Foundation of China (grant no. 81804193); Leading Talents of Traditional Chinese Medicine in Jiangsu Province (grant no. SLJ0206); Special Project on the Inheritance of Ancient Books and Special Techniques of Chinese Medicine of the State Administration of Traditional Chinese Medicine (grant no. GZY-KJS-2020-07).
Ethical approval
Ethics Committee of Jiangsu Province Hospital of Chinese Medicine (2016NL-079-03).
Patient consent
Ethical consent was obtained from the participants.
Provenance and peer review
Not commissioned; externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.