
Abstract
Purpose:
Level 1 evidence supports the use of acupuncture/acupressure (A/A) to manage post-operative nausea and vomiting (PONV). This study aimed to survey healthcare professionals’ attitudes towards A/A, influencing factors and barriers to implementing this effective non-drug intervention into peri-operative care.
Methods:
A validated, anonymous survey with 43 questions was emailed or distributed as a hard copy at meetings to anaesthetists, midwives, nurses, obstetricians, gynaecologists and surgeons at a public hospital in Australia. Descriptive data were presented. Influencing factors were explored using chi-square analysis. Multinomial logistical regression was used to identify the influences of confounding factors.
Results:
A total of 155 completed surveys were returned, reflecting a response rate of 32%. The majority of participants were female (69%), nurses/midwives (61%) and aged between 20 and 50 years old (76%). Eighty-three percent of respondents considered A/A ‘clearly alternative’ medicine or ‘neither mainstream nor alternative’. Eighty-one percent would encourage patients to use acupressure for PONV if it was offered at the hospital. Previous personal use of A/A was the key factor influencing attitudes and openness to clinical use. The key barriers to implementation were perceived lack of evidence and lack of qualified providers and time.
Conclusion:
Hospital-based healthcare professionals strongly supported the evidence-based use of A/A for PONV despite considering the therapy to be non-mainstream and having limited A/A education or history of personal use, providing a positive context for an acupressure implementation study. Significant gaps in training and a desire to learn were identified.
Introduction
Post-operative nausea and vomiting (PONV) affects 30% to 50% of surgical patients, and poorly controlled PONV impacts patients’ recovery and prolongs hospital stay. 1 Modern PONV management encourages multi-modal therapies including pharmacological and non-pharmacological methods.2,3 Systematic reviews and meta-analyses show that acupuncture/acupressure (A/A) is safe and effective at reducing the incidence of PONV in adults following various surgical procedures with different anaesthesia regimes. 4 Needling, pressure or electrical stimulation applied at PC6 (Neiguan), a traditional acupuncture point location above the wrist, reduced the incidence of early post-operative vomiting (at 0–6 h) by two-thirds (relative risk (RR): 0.36, 95% confidence interval (CI): 0.19–0.71) and nausea (0–24 h) by three-quarters (RR: 0.25, 95% CI: 0.1–0.61) when compared with controls, and A/A was particularly effective for patients at high-risk of PONV. 5 Consequently A/A is the only non-pharmacological intervention included in PONV management guidelines,1,2 and one such guideline has been endorsed by the Australian and New Zealand College of Anaesthetists (ANZCA). 1
Despite the evidence, acupuncture in the peri-operative setting has largely remained at the research stage. Although used by individual, interested anaesthetists, 6 to date it has not been implemented systematically. Clinicians involved in peri-operative care from Norway, Germany and the United States have questioned why this safe, simple and effective therapy has not been routinely implemented.5,6
According to the Diffusion of Innovation Theory, 7 positive attitudes towards an innovation, perceived need for change and openness to new ideas are features of early adopters of innovations and facilitate uptake and implementation. 8 A recent survey studied the knowledge and attitudes of 292 anaesthesia providers from the United States towards the use of A/A for PONV 9 and found an overall positive attitude and receptivity to A/A. More than half of the respondents had not used A/A but would consider using it, and more than a third indicated that they would refer patients for A/A. Three quarters of respondents stated that they would like to receive education about A/A.
The authors of this study planned to implement A/A for PONV in a public hospital in Australia. Our previous study showed that over 80% of patients would be willing to receive acupuncture for the management of PONV. 10 The aim of this study was to survey the knowledge of, and attitudes towards, A/A among health professionals involved in the care of surgical patients. Participants included healthcare practitioners involved in peri-operative care at the hospital site where the implementation was planned.
The specific aims of the study were: (1) to survey health professionals’ knowledge of and attitudes to A/A, in preparation for implementing this effective intervention into peri-operative care; (2) to understand the factors that might impact on these attitudes, for instance, profession, gender, age, experience of A/A and personal views of health; and (3) to identify perceived barriers to the implementation of A/A.
Methods
This cross-sectional survey was carried out in a metropolitan hospital located in the northern suburbs of Melbourne, Australia, which has over 300 beds and is a major service provider of acute and subacute specialist health services. At the time of the survey, about 300 elective surgeries were carried out each week and no A/A was offered in the hospital by any health professional, as the hospital did not provide professional indemnity for such activities.
The survey was approved by the Human Research Ethics Committee of the hospital (HREC LR 04.2016), and the approval was endorsed by the Royal Melbourne Institute of Technology (RMIT) College Human Ethics Advisory Network (ASEHAPP 63-16).
Selection criteria of respondents
Eligible participants were health professionals who care for surgical patients, including all anaesthetists, surgeons, peri-operative nurses, surgical ward nurses, obstetrician/gynaecologists and midwives at the study hospital. Both trainee and qualified personnel were included. They were invited by their respective heads of department or nurse unit managers to take part in the survey, either at face-to-face meetings using hard copies or via a Survey Monkey link emailed to them in October 2016. The survey was open for 3 weeks, and a weekly reminder was sent to the eligible participants. The hybrid online and hardcopy method was used to ensure a maximal response.
Survey
The staff survey took approximately 10–15 min to complete and included no identifiable information. Consent was indicated via return of the completed survey. Participants were offered the opportunity to enter into a draw for an iPad Mini to encourage participation.
This anonymous survey had 43 questions modified from a questionnaire previously designed for anaesthetists in the United States, for which face, content and construct validity had already been established. 9 To ensure the validity of the modified survey, we devised a two-step approach. First, the project team screened the questionnaire to map the questions against the purpose of the project to ensure content and construct validity and checked the language to ensure the Australian context. Second, face validity was tested among the project team, and then among 10 health staff members beyond the team, including anaesthetists, nurses, surgeons and women’s health providers. Consequently, section 1 (three questions) was added to ascertain staff attitudes to the use of A/A for PONV. We also added questions to examine staff willingness to provide or encourage patients to use acupressure. Questions about spirituality were removed as the team felt they were irrelevant in the Australian setting. Abbreviations of qualifications were modified to reflect the Australian context. One open-ended text-based question was added to invite comments on barriers. The final survey (Supplemental Appendix 1) had four sections, assessing views about PONV (Q1-3), primary world view of health (Q4-7), attitudes, clinical use and types of evidence (Q8-36) and demographics and specialty (Q37-43).
Sample size and data analysis
The hospital employed about 480 staff involved in peri-operative care, comprising around 60 anaesthetists and fellows, 100 surgeons and fellows, 260 anaesthetic and peri-operative or surgical ward nurses and 60 staff in women’s health. Prior to the conduct of the survey, we expected a 30% response rate, per previous research, 11 or 144 returned surveys.
The chi-square test was applied to test for differences between groups, with a Fisher’s exact test applied on occasions where the counts were <5. Stata version 15.1 (StataCorp, College Station, TX, USA) was used to conduct the statistical analysis, with p < 0.05 indicating statistical significance.
We selected three key behaviours as primary outcomes, prior to the survey data analysis, to assess the willingness for implementation. These questions were as follows: ‘I hope to have AA available to patients in my practice’ (have AA in my practice), ‘Anaesthesia providers and surgeons should be able to advise their patients about AA’ (Advice AA) and ‘If acupressure was available, would you encourage your patients to take up this treatment’ (encourage patients to use). Multinomial logistical regression analysis with forward stepwise techniques was conducted to assess and identify factors associated with each of these questions/outcomes. While the results are presented as 5-point Likert-type scale questions, as this is how the questions were included in the survey, for the multinomial regression analysis, the number categories were reduced from 5 to 3, by combining the category of ‘strongly disagree’ with ‘disagree’, and the category of ‘agree’ with ‘strongly agree’. Neutral was retained as a separate category/level. This pooling of responses was conducted due to low response rates in some categories, such as strongly agree or strongly disagree.
Free-text comments were extracted into a Microsoft Excel spreadsheet. Themes were identified and agreed upon by two authors (ZZ and JL) and presented in this article.
Results
Demographic data
Of 480 staff members invited to participate in the survey, 165 responded (70 via online survey and 95 paper-based). Ten were excluded from the analysis as they were incomplete, providing an overall response rate of 32%. Sixty-nine percent of the respondents were female, 80% aged between 20 and 50 years old, 87% trained in Australia and 61% were either nurses (51%) or midwives (10%). The top three surgical specialties were general, obstetrics/gynaecology and orthopaedics (Table 1).
Socio-demographic features of the respondents.
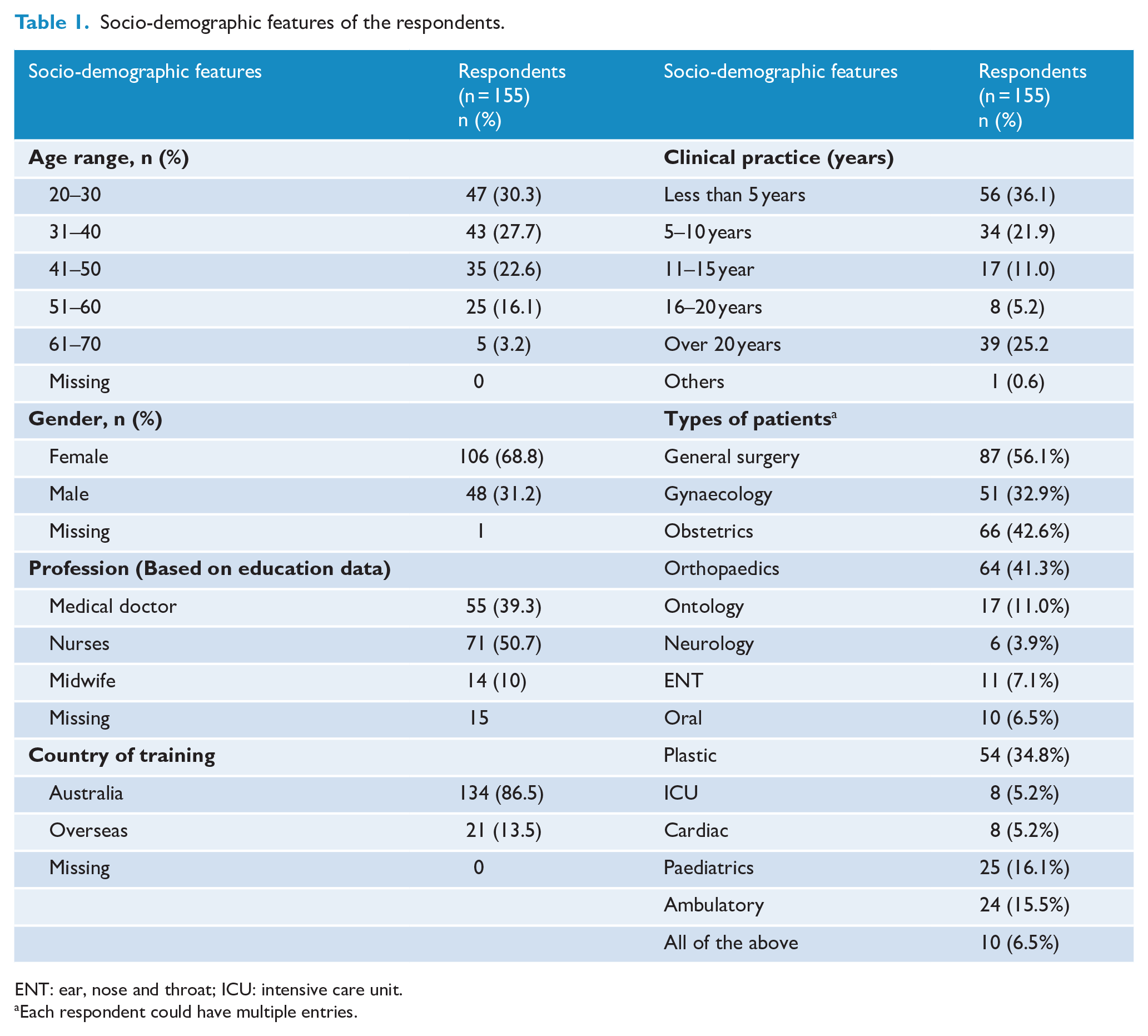
ENT: ear, nose and throat; ICU: intensive care unit.
Each respondent could have multiple entries.
Staff view of PONV management and the use of acupressure at the hospital
Over two-thirds of the respondents agreed that PONV was well managed at the hospital, and that a documented PONV risk checklist should be used. Eighty-one percent agreed that effective non-drug therapies should be used (Supplemental Appendix 2).
Experience of and attitudes towards acupuncture/acupressure
Three questions were designed to understand personal experience of and attitudes to A/A and personal world view of health (Figure 1). Nearly half of the respondents (47%) had not used A/A but would consider using it for their own health. Over half of the respondents (55%) held a combined biomedical and holistic view of health. There was a split between the view that A/A was ‘clearly alternative’ (44%) and ‘neither mainstream nor alternative’ (41%). When asked about the use of A/A for post-operative complications, about 40% of the respondents believed A/A was effective for PONV, post-operative pain or anxiety, whereas 30% believed it had no real impact.
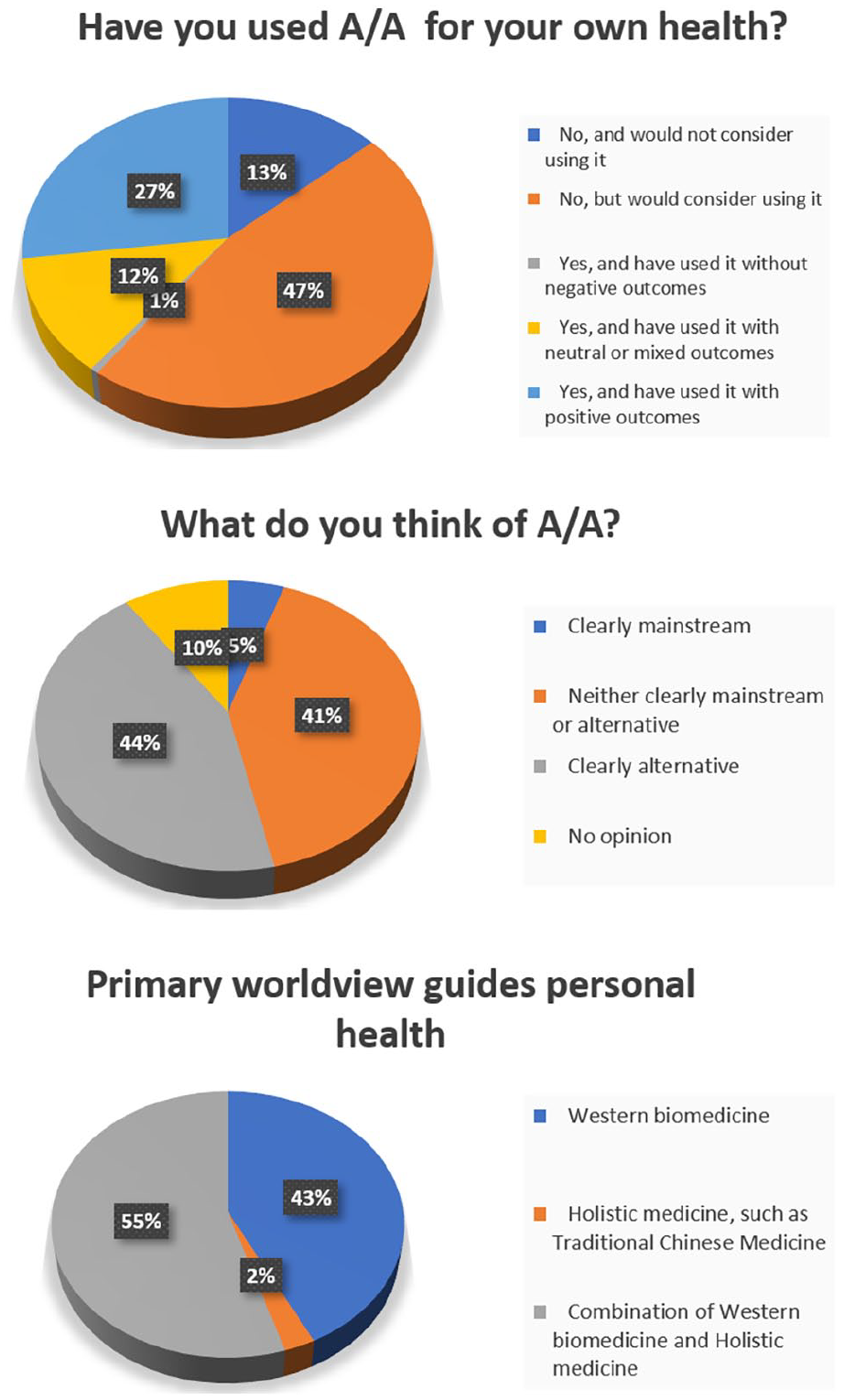
Responses to personal use of acupuncture/acupressure (A/A) and primary world view guiding personal health (n = 155).
Attitudes towards integrating acupuncture/acupressure into clinical practice
Ten questions were designed to assess attitudes towards the use of A/A in clinical practice. Overall, the attitudes to A/A were positive with a small portion of respondents holding negative views (Table 2). For instance, 59% (n = 90) believed that A/A could be integrated with the best conventional care for clinical use, and 63% (n = 97) indicated that they would like to make A/A available in their practice.
General attitude to acupuncture and acupressure (n = 155).
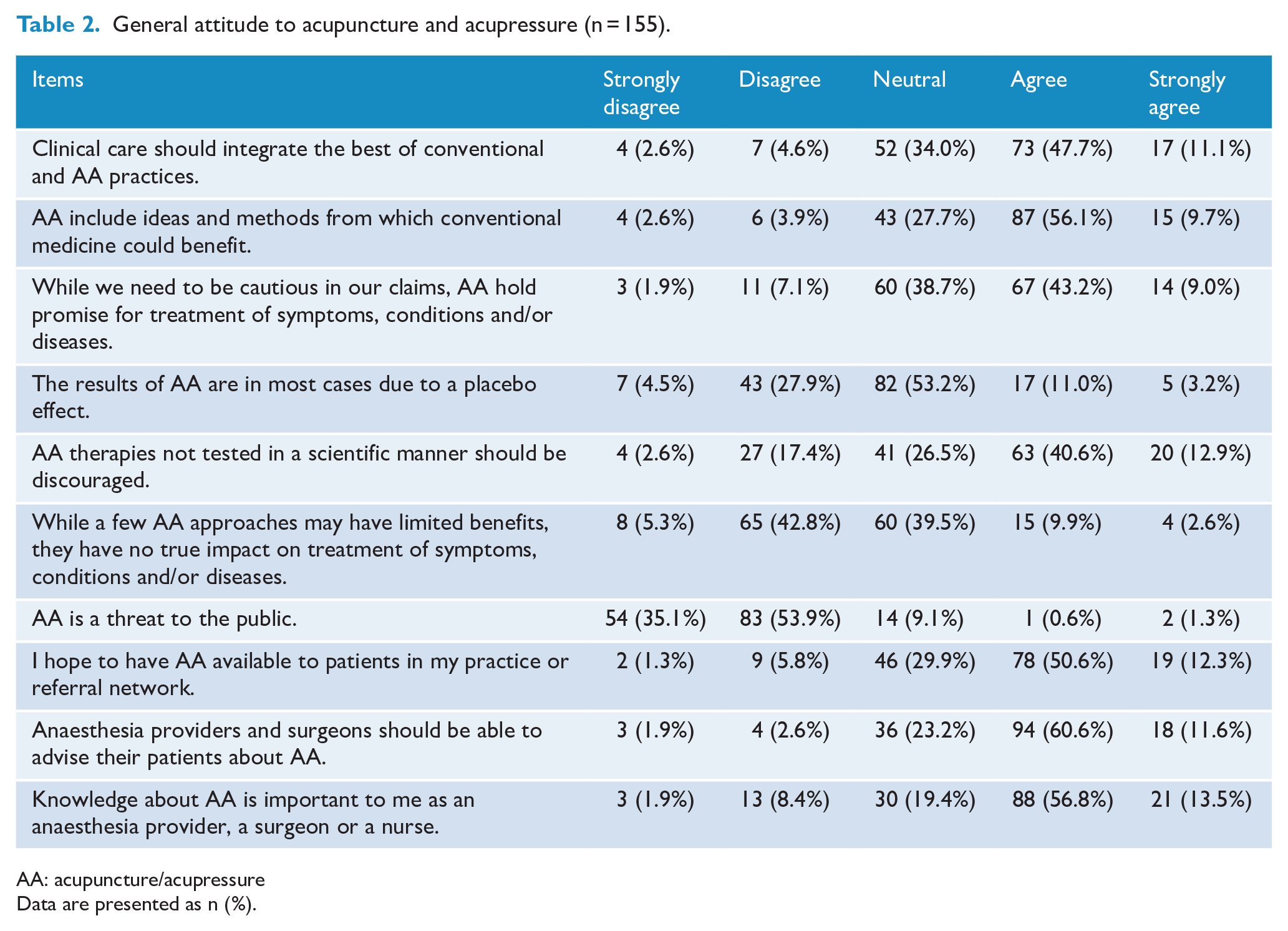
AA: acupuncture/acupressure
Data are presented as n (%).
Perceived barriers integrating acupuncture/acupressure into the Western medical hospital setting
Five multiple choice questions and one open-ended question asked about potential barriers to the use of A/A in a modern Western medical hospital setting. As shown in Figure 2, the top two reasons were a perceived lack of scientific evidence (79%, n = 122) and lack of availability of credentialled providers (73%, n = 113). Over 50% selected a lack of reimbursement and equipment as barriers. Thirteen respondents provided written text, citing a lack of education or knowledge about A/A and its effectiveness (n = 7), the difference in medical paradigms or the dominance of the biomedical model (n = 3) and patients’ willingness or choice (n = 2) as potential barriers.
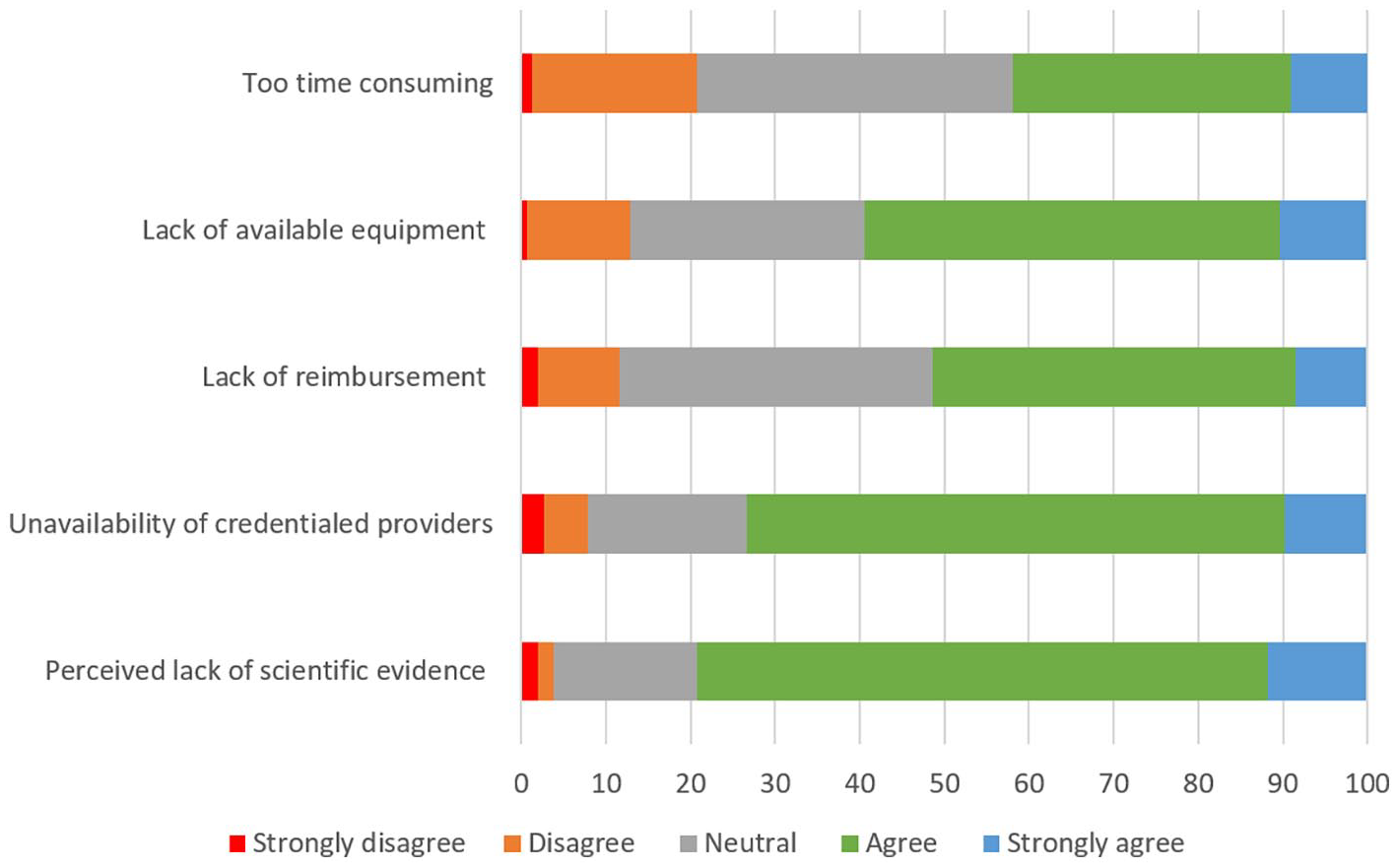
Perceived barriers to integrating acupuncture/acupressure into the Western medical hospital setting (n = 155).
Peri-operative use of acupuncture/acupressure and training
Five questions asked about the experience of using peri-operative A/A, related education and willingness to utilise it. More than two-thirds of respondents (67%, n = 103) did not practice A/A and 30% (n = 46) would recommend a complementary and alternative medicine (CAM) provider to patients. After being told A/A that ‘acupuncture and acupressure have been shown to be effective for PONV and postoperative pain in systematic reviews and are included in the guidelines for those two conditions’ and education would be provided for practising A/A, 67% (n = 102) of respondents indicated they would use it. In addition, 85% of respondents (n = 131) would encourage patients to use acupressure for PONV if the hospital provided it. At the time of survey, 69% of respondents (n = 110) had not had any education in A/A, and only 6% (n = 9) felt sufficiently trained to personally provide the intervention. Ninety-four percent (n = 139) of respondents indicated that they would like to receive education in A/A.
Importance of evidence types
Finally, respondents were asked to rate the importance of eight types of evidence that they considered essential for recommending or using A/A (Supplemental Appendix 3). The top three were systematic reviews or clinical guidelines (85% considered these to be either essential or somewhat essential), randomised controlled trials (81%) and proven mechanisms (77%).
Exploring factors influencing attitude and practice
Profession and gender significantly influenced participants’ belief in, attitude towards, personal use of and willingness to be educated in A/A, as summarised in Table 3. For instance, nearly half of the female respondents (45%) considered A/A neither alternative nor mainstream, and had used A/A for personal health (48%), whereas the majority of males (58%) considered it clearly alternative, and had not used A/A but would consider it. In addition, females (70%–80%) and nurses (70%–80%) were more likely than males and doctors, respectively, to consider A/A knowledge and availability important, more willing to advise patients on its use, and less likely to consider the results of A/A as being due to placebo effects. Similarly, females were more positive towards providing acupressure if taught (71%), or recommending their patients use acupressure (89%) than males. There was no difference in the view (mainstream vs alternative) or provision of acupressure among the different professions.
Profession, gender and age differences in attitudes to A/A and view of A/A practice (n = 155).
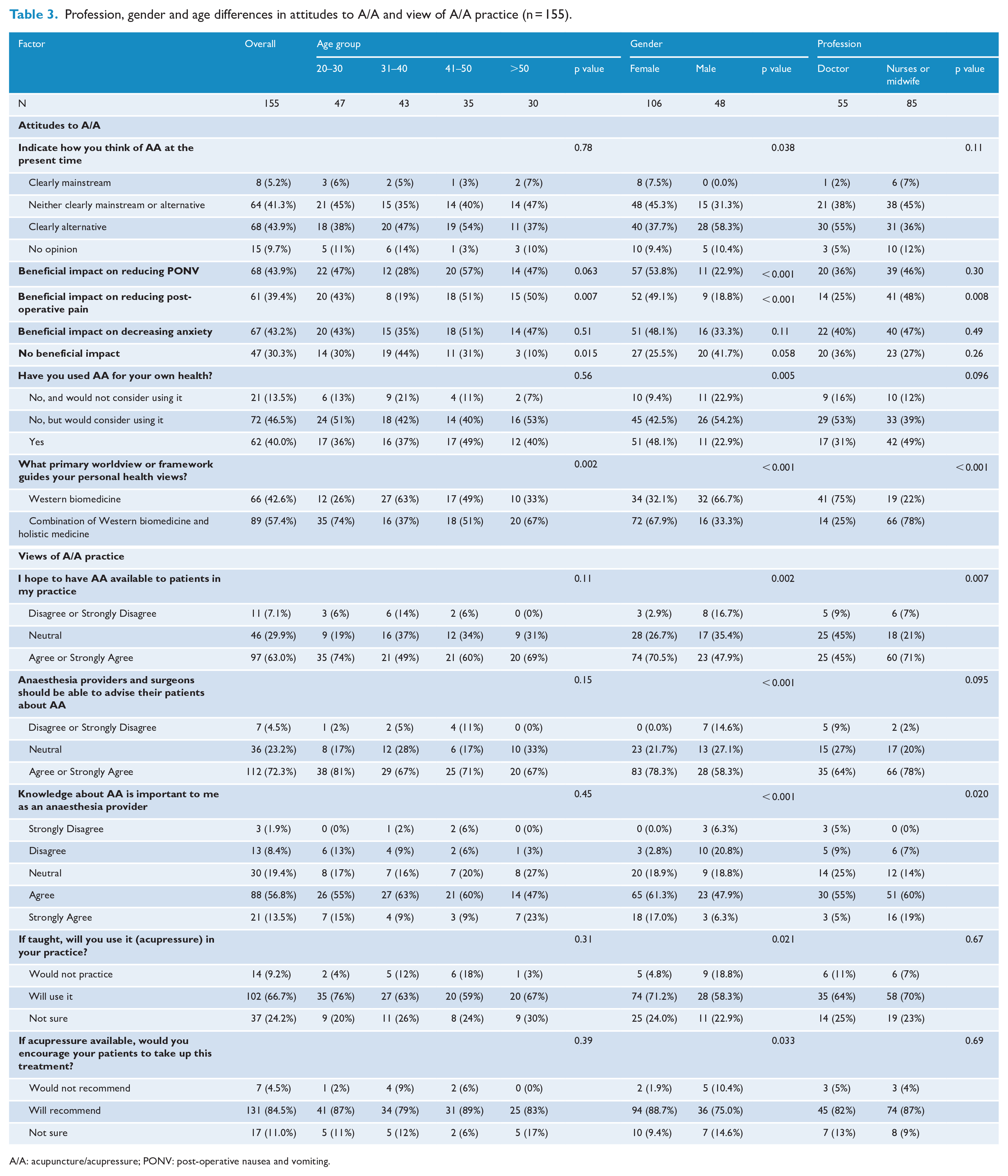
A/A: acupuncture/acupressure; PONV: post-operative nausea and vomiting.
The combined holistic and biomedical view was more frequently held in those aged 20–30 (74%) or >50 (76%), than those between 31 and 40 (37%) or 41 and 50 (51%). There were differences according to age, gender or profession type in perceived barriers to integration, views on PONV management and use of acupressure at the surveyed hospital (Table 3).
Sixty-one percent of those who had prior education of A/A believed that A/A reduces PONV (p = 0.003), compared with only 36% of those without A/A education (data not shown). Those who had prior education were also more likely to have used A/A for personal health (59% with education vs 31% without, p = 0.001). Both groups were equally keen to refer patients to A/A if the service were available (88% with education and 83% without education, p = 0.449) or personally provide (75% with education and 63% without education, p = 0.139).
There were overlaps between gender and profession, as the majority of nurse respondents were female. In addition, 76% of those who had used A/A for personal health held a combined world view, compared with 54% for those who had not used A/A but would consider it, and 14% (3 of 21) of those who would not consider using it (p < 0.001). In addition, those who had prior A/A education were more likely to have used A/A for personal health. Multinominal logistic regression was used to explore the influencing factors, including gender, profession, age, A/A use for personal health, world view and prior A/A education. When considering the three key behaviours and factors independently associated with them, gender, profession, world view and prior A/A education were found not to be significantly associated with the response. The only variable associated with all three key behaviours was previous personal use of A/A. Those who had not used A/A and would not considering use it were as follows: 51 times less likely to have A/A in their practice (RR: 51.34, 95% CI: 3.91–673.92, p = 0.003) than those who used A/A; 42 times less likely to advise A/A use (RR: 42.40, 95% CI: 3.94–456.03, p = 0.002); and seven times more likely to select ‘not sure’ if they would recommend acupressure even when the service was available (RR: 6.59, 95% CI: 1.52–28.49, p = 0.012). Those who held a Western biomedical view were three times more likely to select ‘neutral’ (RR: 3.17, 95% CI: 1.39–7.23, p = 0.006). The impact of health view was far less prominent (Supplemental Appendix 4).
Discussion
In this survey, the attitudes of doctors and nurses involved in the care of surgical patients were overwhelming positive towards the use of peri-operative A/A. Eighty-eight percent of health professionals at the study site were willing to support their patients to take up evidence-based use of A/A for PONV, despite over 85% considering the therapy non-mainstream and only 40% having prior personal experience of A/A. Perceived lack of evidence and lack of credentialed providers were the two key barriers to incorporating A/A. Previous personal use of A/A had a positive impact on three key behaviours related to implementation: considering A/A in their practice, advising patients about A/A and encouraging patients to take up acupressure for PONV if available. Successful implementation of A/A for PONV needs to capitalise on these positive attitudes, enhance awareness of evidence and provide training.
Strengths and limitations of the study
This study was based on a validated US survey on a similar topic. 9 The survey was modified for the Australian healthcare context, with a view to implementation. The validity of the modified survey was tested prior to use. All health professionals involved in PONV management were surveyed, with a response rate over 30%, and a small amount of missing data.
The key limitation of the study is being a single hospital-based survey. The surveyed hospital had a history of having general practitioners delivering acupuncture to patients over 10 years prior. This might have created a positive image of A/A and skewed the results, and the data might not represent the overall Australian context, although the positivity was similar to the US data. The second possible weakness is the use of a mixed method of online and paper-based surveys, which increased opportunity to complete the survey, but did not prevent individuals from completing it more than once. However, it was clear from the contact details provided for the prize draw that no one had entered the draw twice.
Ten incomplete surveys were excluded from the final analysis. Demographic data were placed at the end of the survey, therefore those data were not available for comparison. However, within the completed questions, there were no differences in answers between complete and incomplete surveys. The incomplete surveys were therefore deemed to have had a minimal impact on the overall findings.
Comparisons with previous research
To our knowledge, there has been only one other survey examining this topic. 9 The trends in our findings are similar to that previous study in the world view for health and personal use of A/A. Our Australian cohort had relatively less education in A/A and were more willing to learn. About 70% of Australian respondents had never had A/A education, compared with 44% in the US cohort. In both countries, about 85% of those surveyed considered A/A as either ‘clearly alternative’ or ‘neither clearly mainstream nor alternative’. Over one-third in both cohorts had used A/A, and about 50% had not but would like to try. Fewer respondents in the Australian cohort (30%–40%) believed that A/A would be useful to reduce post-operative anxiety (30%), pain (39%) and PONV (40%), compared with 60%–85% in the US cohort. However, it is important to note that the US survey focused on anaesthetists and anaesthesia providers, whereas surgeons, nurses, midwives and obstetricians were also included in the Australian cohort.
Perceived lack of evidence and lack of credentialed providers were the top two barriers identified in both surveys. In implementation science, knowledge of the new intervention is essential for uptake. 8 There is a significant amount of evidence supporting the effectiveness and safety of A/A for PONV and post-operative pain. ANZCA has endorsed the PONV guideline, in which A/A was the only non-pharmacological intervention included. 1 This recommendation has been in place since the first edition of the guidelines in 2003. 12 The ANZCA guidelines on acute pain management have also cited systematic review (level 1) evidence supporting acupuncture for acute pain and post-operative pain since 2005. 13 It appears that the information has not been disseminated to the end users.
Interpretation of the findings
We found women, nurses, those holding a combined Western medicine and holistic view and those who were willing to use A/A for personal health were more positive towards A/A and were more likely to offer A/A to their patients. Faircloth 9 also found that more women have used acupuncture for personal health than men (45% of females vs 31% of males). Indeed, in the literature, female healthcare practitioners 14 and women in general15,16 are more positive towards CAM than men are. We found age was not a strong influence, but nurses were more positive towards A/A than doctors. This differed from Faircloth’s study, in which there was no difference between doctors and nurses. In Faircloth’s sample, 46% were nurses and 49% were female, in comparison with 60% and 69%, respectively, in our survey. Most of the nurses surveyed were female, so the difference in profession was perhaps driven by gender.
After using multinomial logistic regression to adjust for the possible overlaps among various factors, we found that the only factor strongly impacting attitudes was previous personal use of A/A for personal health. Faircloth did not explore this relationship. Our finding is consistent with previous international and Australian research. In the literature regarding CAM use, Stewart et al. 17 surveyed midwives, obstetricians and anaesthetists caring for pregnant women and found midwives who had training in CAM, had personal use of CAM or had been in practice longer were more willing to recommend CAM use to their patients. Similarly, after logistic regression, only personal use of CAM was a key indicator, with those who had used CAM for personal health being eight times more likely to recommend CAM to pregnant women than those had no personal use. Personal use leading to a recommendation for CAM to patients has been consistently found in other surveys, most of which have targeted nurses.18,19
Generalisability, gaps in knowledge and relevance to implementation
The results suggest a supportive environment for the implementation of acupressure for PONV at the study site. Either doctors or nurses could be suitable to deliver acupressure in our implementation study, as the majority of both professions were willing to accept and practise this intervention. To address the key barriers, we have developed a knowledge translation plan and training plan. The knowledge translation plan includes outreach, education seminars, flyers in the team room and personal contact. The training plan includes a short video message from the lead surgeon, nurse manager, reports of overseas experiences and a step-by-step flow chart. It may also be useful to invite healthcare professionals to experience acupuncture or acupressure prior to the implementation. Overall, this survey could be useful for those who are interested in implementing A/A in hospitals.
This study identifies a significant gap between a lack of knowledge or training in A/A among healthcare professionals and their desire to learn. Less than one-third had prior education and over 90% indicated they would like to have more education. Given A/A is one of very few effective non-pharmacological interventions for PONV and post-operative pain, it is necessary to embed the education in undergraduate or post-graduate training of doctors and nurses and provide opportunities for those students to experience A/A for their personal health. In addition, registered Chinese medicine practitioners could deliver A/A in an acute setting with additional training.
Conclusion
Healthcare professionals involved in peri-operative care in an Australian hospital have positive views of integrating A/A into clinical practice and a strong desire to learn more about it. The survey results have guided the development of implementation strategies for incorporating A/A into the routine management of PONV. To facilitate broader implementation of PONV, further understanding of practitioners’ view through a national survey is warranted.
Supplemental Material
sj-docx-1-aim-10.1177_09645284221085282 – Supplemental material for Health professionals’ attitudes towards acupuncture/acupressure for post-operative nausea and vomiting: a survey and implications for implementation
Supplemental material, sj-docx-1-aim-10.1177_09645284221085282 for Health professionals’ attitudes towards acupuncture/acupressure for post-operative nausea and vomiting: a survey and implications for implementation by Zhen Zheng, Wanda S Stelmach, Jason Ma, Juris Briedis, Raphael Hau, Mark Tacey, Jeannette Atme, Debra Bourne, Julie Crabbe, Catherine Fletcher, Paul Howat, Jenny Layton and Charlie C Xue in Acupuncture in Medicine
Supplemental Material
sj-docx-2-aim-10.1177_09645284221085282 – Supplemental material for Health professionals’ attitudes towards acupuncture/acupressure for post-operative nausea and vomiting: a survey and implications for implementation
Supplemental material, sj-docx-2-aim-10.1177_09645284221085282 for Health professionals’ attitudes towards acupuncture/acupressure for post-operative nausea and vomiting: a survey and implications for implementation by Zhen Zheng, Wanda S Stelmach, Jason Ma, Juris Briedis, Raphael Hau, Mark Tacey, Jeannette Atme, Debra Bourne, Julie Crabbe, Catherine Fletcher, Paul Howat, Jenny Layton and Charlie C Xue in Acupuncture in Medicine
Footnotes
Acknowledgements
We would like to thank all participants who completed the survey and all the managers who promoted the survey.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The project was embedded in an NHMRC TRIP project, in which an acupressure wristband was implemented for preventing and managing PONV. No other conflict of interests is to be declared.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by a Translating Research into Practice Fellowship (TRIP, APP1110446) from the National Health and Medical Research Council (NHMRC) to Zhen Zheng; an RMIT University Postgraduate Scholarship to Jenny Layton, and an RMIT University Seeds Grant and Internal funding from the School of Health and Biomedical Sciences, RMIT University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.