
Abstract
Objective:
This study investigated the effects of auriculotherapy on early postoperative rehabilitation after total knee arthroplasty (TKA).
Methods:
A prospective cohort study was conducted from March to September 2024 at Peking Union Medical College Hospital and its affiliated consortium. Patients receiving auriculotherapy postoperatively were compared with a matched non-exposed group (selected by propensity score matching). The primary outcome was the change in knee joint active range of motion (AROM) from postoperative day (POD) 1 to POD 4 (Δ AROM). Secondary outcomes included Hospital for Special Surgery (HSS) scale, patient-controlled analgesia (PCA) use, facial visual analog scale (F-VAS) and Tampa scale of kinesiophobia (TSK) scores, plus swelling measurements.
Results:
Data from a total of 110 patients was collected in this study, with 84 (42 matched pairs) included in the final analysis. Compared with the non-exposed group, the auriculotherapy group showed significantly greater improvements in Δ AROM (40.60 ± 11.69° vs 29.41 ± 13.64°, p < 0.001) and HSS scores (p = 0.004). The auriculotherapy group also pressed their PCA button fewer times (p = 0.047) and exhibited reduced supplemental analgesic use (p = 0.004) and lower TSK scores (p < 0.001). Knee circumference and swelling were significantly reduced in the auriculotherapy group (p < 0.05). Trend analysis indicated significant between-group differences and interaction effects for AROM and kinesiophobia (p < 0.001).
Conclusion:
Based on the findings of this observational study, auriculotherapy is associated with better early functional outcomes in early postoperative rehabilitation of patients after TKA. Randomized controlled trials are necessary to explore its potential effectiveness and underlying mechanisms.
Keywords
Introduction
Total knee arthroplasty (TKA) is a common and effective treatment for end-stage knee osteoarthritis, offering substantial mid- to long-term benefits, such as improved quality of life, pain relief and functional recovery.1,2 However, 16%–20% of patients remain dissatisfied with TKA outcomes 1 year post-surgery.3,4 Orthopedic surgeries, including TKA, are among the most painful procedures globally, often resulting in severe postoperative pain, 5 kinesiophobia, 6 lower limb swelling, 7 and other adverse reactions. These early complications can significantly hinder rehabilitation and affect the ultimate success of TKA. Traditionally, opioid analgesics have been used to manage postoperative pain, 8 but their side effects have led to the increasing adoption of multimodal analgesia and rehabilitation strategies, including acupuncture. 9
Auriculotherapy is a therapeutic modality in which the ear is stimulated by pressure and/or needle penetration, most commonly at one or more traditional auricular acupuncture point locations, with the intention of preventing or treating disease. 10 It has been applied in various traumatic and postoperative acute pain settings.11–13 A recent meta-analysis indicated that auriculotherapy is superior to conventional treatments at reducing adverse reactions and pain after TKA. 14 Although randomized controlled trials (RCTs) have provided evidence for the use of auriculotherapy in TKA, its effectiveness and real-world application still require further validation in complex clinical settings.
Real-world studies (RWS), which utilize real-world data to generate evidence, have become an essential approach in clinical research. 15 Although the research design lacks randomization, which may introduce confounding factors and compromise the validity of causal inferences, RWS can identify associations with potential research value in real-world clinical settings. This approach is particularly well-suited to clinical contexts that emphasize individualized diagnosis and treatment, such as auriculotherapy. Beyond pain management, clinical experience and previous studies suggest that auriculotherapy may offer additional benefits in early TKA rehabilitation, such as improving joint function and quality of life, 16 alleviating postoperative anxiety, 17 and reducing swelling. 18 Verifying these effects through individual RCTs is challenging due to cost, ethics, generalizability and implementation. In practice, auriculotherapy often uses an individualized treatment approach based on the specific patient. By contrast, relevant RCTs commonly establish a fixed protocol for needling location within the treatment plan before the beginning of the experiment, 19 which may limit the full potential of auriculotherapy as compared to usual clinical practice.
Accordingly, we designed a prospective cohort study based on real-world clinical data to investigate known and potential new effects of auriculotherapy in rehabilitation following TKA, and to further examine its potential role in postoperative recovery.
Methods
Study design and ethical considerations
This prospective cohort study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20 Ethical approval was obtained from the Institutional Review Board of Peking Union Medical College Hospital in March 2024 (approval no. I-24PJ0652). In addition, the study protocol was prospectively registered with ClinicalTrials.gov (registration no. NCT06273488) on 15 February 2024 and updated on 9 December 2025.
In terms of reporting standards, we adhered to the STROBE statement for observational studies, while referencing the STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines for intervention-related criteria. 21
Study setting
Participants were recruited from the Department of Orthopedics at Peking Union Medical College Hospital between March and September 2024. Patients scheduled for TKA due to knee osteoarthritis were enrolled. Data collection was conducted at Peking Union Medical College Hospital and its affiliated medical consortium. Follow-up information was obtained through telephone inquiries. The final follow-up of participants was completed in December 2024. Trial data were collected synchronously through clinical visits, electronic medical records and telephone communications.
Participants
Patients were screened for eligibility and enrolled in this study preoperatively. To be included, patients needed to: (1) be aged 50–80 years, regardless of gender; (2) have been diagnosed with Kellgren–Lawrence grade V knee osteoarthritis with a clinical indication for TKA; 22 (3) have intact auricles on both ears; (4) be willing to undergo standardized rehabilitation at a rehabilitation hospital postoperatively; and (5) be capable of understanding the study purpose and be willing to comply with the study protocol and to provide informed consent.
Patients with the following conditions were excluded: (1) severe arrhythmias, heart failure, chronic obstructive pulmonary disease, epilepsy or psychiatric disorders; (2) auricular damage, redness, bleeding, infection or other contraindications to auriculotherapy; (3) preoperative varus deformity >15° or valgus deformity; and (4) other conditions rendering the patient unsuitable for study participation (as deemed by the investigators).
Clinical auriculotherapy protocol
Research personnel contacted participants 2–3 days before surgery to explain the study procedures and obtain informed consent. Our consent form documented participants’ preliminary willingness to receive auriculotherapy. Willing participants were then provided with a detailed explanation of the treatment protocol, which was developed based on nationally certified standards in China and enriched by clinical experience at our hospital. Treatment incorporated both standardized and individualized approaches. Specifically, based on a foundation of fixed traditional acupuncture points (Shenmen, Sympathetic, Heart, Subcortex, Sanjiao, Liver, Kidney and Knee, illustrated in Figure 1), certified acupuncturists supplemented the treatment with personalized point selection tailored to each patient’s specific condition. The selection of additional points was primarily guided by postoperative complications, adverse reactions and significant positive auricular reaction zones. For instance, the Stomach point was added for nausea, while the Heart, Occiput and Subcortex points were added for insomnia, with the total number of acupuncture points not exceeding 11 (additional points ⩽3). The acupuncturist responsible for orthopedic consultations possessed over 10 years of clinical acupuncture experience. All procedures adhered to national standards for ear acupuncture nomenclature (GB/T 13734-2008) 23 and technical specifications (GB/T 21709.3-2021). 24 The auriculotherapy protocol included: (1) two filiform needle treatments within 24–72 h of surgery (15–30 min/session) using 20 × 25 mm disposable stainless steel acupuncture needles (Ande Medical Equipment Co. Ltd, Guizhou, China) that were inserted to a depth of 1–3 mm (alternating ears) and stimulated to maintain de qi sensation; and (2) bilateral auricular acupressure using cowherb seed auricular plasters (Zhongyan Taihe Medical Devices Co. Ltd, Beijing, China) that were applied on postoperative day (POD) 7 and 14 (i.e. 4-d application with 3-d rest intervals). Participants received detailed instructions for the acupressure, which was self-administered three times a day (1 min/session) with additional presses permitted for breakthrough pain. Daily patch monitoring was supported by nurse-led compliance verification through daily rounds and documentation of adherence metrics. If an ear patch was found to be loose, the doctor or nurse was contacted to reapply it. It should be noted that the auricular acupuncture and auricular acupressure treatments in this study were applied at the same set of traditional acupuncture point locations.
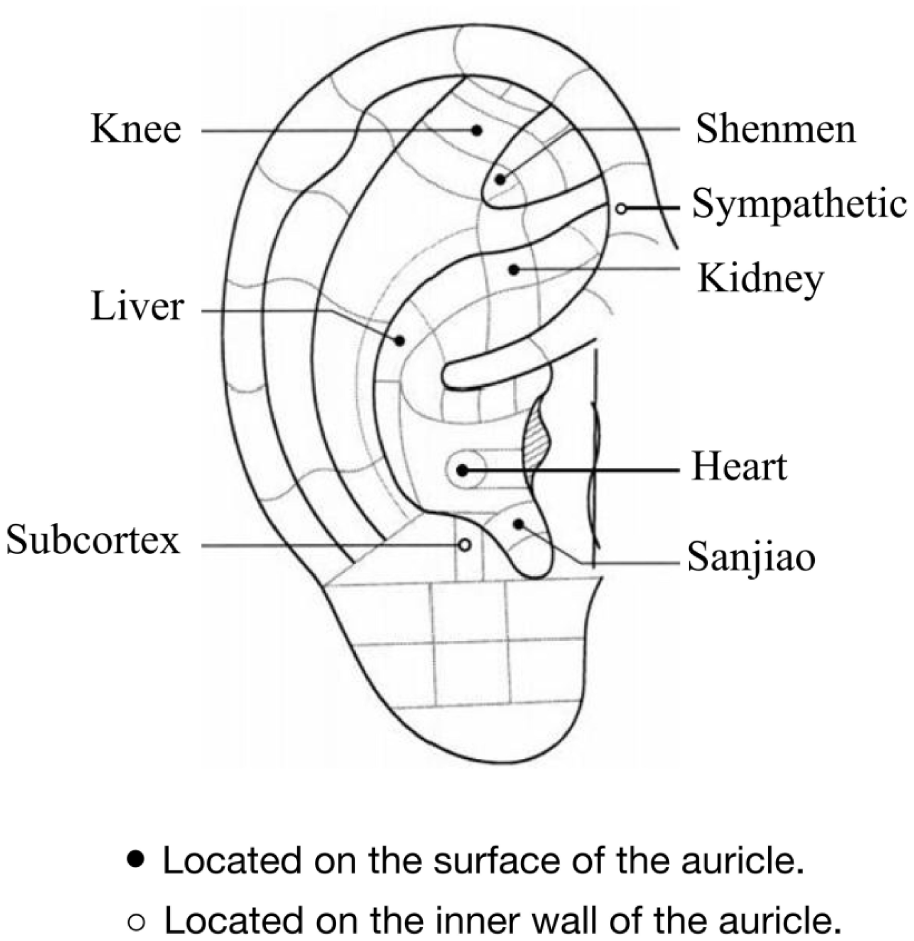
Schematic diagram of fixed traditional acupuncture point selection for auriculotherapy.
Cohort determination
The decision to undergo auriculotherapy was neither randomized nor directed by the investigators. It was influenced by a combination of real-world factors, including patient preference, recommendations from attending physicians and advice from auriculotherapy practitioners. Therefore, not all interested patients ultimately received the treatment. Based on the actual receipt of auriculotherapy treatment after surgery, participants were subsequently categorized into one of two cohorts: the exposed group (those who received at least one session of auriculotherapy) and the non-exposed group (those who received no auriculotherapy). Auriculotherapy was provided free of charge to all participants and the treatment method was consistent with the aforementioned clinical auriculotherapy protocol. This project was supported by the Chinese Academy of Medical Sciences’ Integrated Commissioned Project and the Peking Union Medical College Hospital Sedimentation Research Fund. Crucially, we documented preoperative demographic information, affected limb details, preoperative psychological characteristics, indicators of inflammation and infection in the blood, surgical information and anesthesia information for all patients. The intraoperative anesthesia protocol that was adopted is detailed in the supplemental materials.
Outcome measures
Primary outcome measure
The range of motion (ROM) of the knee joint postoperatively is a key indicator of the success of TKA, as it reflects the ability of patients to resume basic daily activities. 25 Active range of motion (AROM) is defined as the degree of knee flexion achieved without assistance. It is closely related to lower limb pain, kinesiophobia and swelling and better reflects the early functional recovery of the knee joint after surgery. In this study, the change in AROM from POD 1 to 4 (measured by trained personnel to optimize accuracy) was used as the primary outcome measure. Of note, we accidentally listed all our ROM measurement time points (up to 1 month following surgery) as the primary outcome in the trial registration, thus describing the measurement timeline rather than prespecifying any particular time point as primary. The trial registration was corrected on 9 December 2025.
Secondary outcome measures
Secondary outcome measures included the following:
Individual values for AROM of the knee joint on POD 1–4, 7 and 14, which collectively reflect the recovery trend of AROM after surgery. Of note, measurements at 1 month after surgery could not be reliably collected/analyzed due to loss to follow-up.
Pain measurement evaluated using the facial visual analog scale (F-VAS) 26 preoperatively and on POD 1–4, 7 and 14 during early rehabilitation exercises. The F-VAS was added post hoc and incorporated the advantages of the Wong-Baker Faces Pain Scale-Revised (FPS-R) 27 to enhance its suitability for pain assessment in elderly patients.
Anxiety and kinesiophobia measurement. The Tampa scale of kinesiophobia (TSK) 28 was used to assess fear of movement on POD 1–4, 7 and 14, as excessive fear of postoperative pain can impede recovery.
Swelling measurement. Lower limb circumference was assessed at specific measurement points preoperatively and on POD 1–4, 7 and 14. In addition to measuring knee circumference (KC), leg circumference was also measured in axial planes corresponding to different traditional acupuncture point locations, as well as conventional LC measurement sites. Each of the following measurements was repeated three times and averaged: LC-1: at the level of SP10 (Xuehai) and ST34 (Liangqiu) LC-2: at the level of SP9 (Yinlingquan) and GB34 (Yanglingquan) LC-3: 10 cm above the superior border of the patella LC-4: 10 cm below the inferior border of the patella
Additional analgesic use recorded as the frequency of patient-controlled analgesia (PCA) use (defined as the number of times the button was pressed) and the use of supplementary analgesics on POD 1–4 by designated personnel.
Knee function assessment measured using the HSS score on POD 7 and 14.
Auriculotherapy details, including treatment duration, frequency and traditional acupuncture point selection, recorded after each session.
Follow-up information collected via telephone to assess pain levels using a 5-point verbal rating scale (VRS-5) 29 on POD 30 (another post hoc addition).
Adverse events, including nausea, vomiting, dizziness and palpitations (primarily self-reported by patients).
Detailed descriptions of all measurement methods are provided in the supplemental materials.
Potential biases
Patient screening and enrollment were conducted by three orthopedic teams, each possessing over 15 years of experience in TKA. Before surgery, all participants provided written informed consent, which included a commitment to maintain confidentiality of auriculotherapy treatment status. An independent third-party evaluation team, comprised of orthopedic professionals unaware of group allocation, was responsible for the collection and measurement of all clinical data. Standardized tools and uniform procedures were utilized to ensure data objectivity. To monitor blinding integrity, a blinding monitor conducted monthly blinding integrity assessments (where the measurement evaluators’ accuracy in guessing auriculotherapy treatment status was required not to be significantly higher than 50% random probability). All data were managed under tiered access control and statistical analyses were performed by an independent data team. Any instance of outcome assessor unblinding required approval and documentation by the principal investigator.
Sample size calculation
Before beginning the study, we extracted data from 20 patients who had undergone TKA at Peking Union Medical College Hospital between January and February 2024. Among them, 10 patients who received auriculotherapy on POD 4 had an average increase in AROM of 31.8 ± 5.96° (mean ± standard deviation (SD)) compared with POD 1, while 10 patients who did not receive auriculotherapy had an average increase of 28.2 ± 4.78°. Using a significance level (α) of 0.05 and a power (1-β) of 0.8, and assuming a 1:1 ratio between groups, the minimum sample size for the exposed group was calculated to be 36. Thus, it was estimated that a total of 72 participants would be required to detect this estimated difference. Considering a 50% dropout, loss to follow-up and matching failure, we estimated that at least 108 participants should be included, with 54 in the exposed group and 54 in the non-exposed group. Further details of our sample size calculation are provided in the supplemental materials.
Statistical analysis
During the study, efforts were made to minimize data loss. Data collectors were required to meticulously document the reasons for any missing data during phased data collection. This information was used to determine the mechanism of data loss. When data were missing completely at random (MCAR) and the proportion of missing data was <5%, listwise deletion was applied. If data were missing at random (MAR) and the proportion was <5%, regression imputation was used. For missing proportions <30%, multiple imputation was employed. If the proportion of missing data exceeded 30%, the affected variable was excluded from analysis.
All data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 27.0 (SPSS Inc., Chicago, IL, USA). Propensity score matching (PSM) was employed to control for potential confounding factors. These factors included patient demographic information (age, sex, body mass index (BMI)), affected limb details (affected side, year of knee osteoarthritis diagnosis, AROM, F-VAS score, joint stiffness, joint crepitus), preoperative psychological characteristics (self-rating anxiety scale score), indicators of inflammation and infection in the blood (erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)) and surgical information (surgical approach, surgical team, duration of surgery and prosthesis brand). A propensity score was calculated for each study subject, and 1:1 nearest neighbor matching was performed with a caliper value of 0.02. Once matched, the pairs were fixed, and each subject was included only once in the matching process.
Following PSM, a multiple linear regression model with stepwise variable selection was constructed to identify significant predictors of the primary outcome. Subsequent between-group comparisons for validation were performed based on data distribution. The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed data are presented as mean ± SD and were compared using the independent samples t-test. Non-normally distributed data are presented as median [interquartile range] and were compared using the Mann–Whitney U test. Categorical variables are presented as n (%) and were compared using the chi-square test or Fisher’s exact test, as appropriate. To mitigate the potential information loss associated with PSM, this study concurrently conducted an inverse probability weighting (IPW) analysis using the same set of covariates. Weighted analyses were subsequently performed to reassess the between-group differences in the primary outcome measure. For data involving multiple time points (repeated measures), a generalized estimating equation (GEE) model was applied. A two-sided p value of <0.05 was considered statistically significant.
Results
Baseline characteristics
To ensure the feasibility of clinical recruitment and enhance the ultimate matching success rate, during the study period, a total of 163 patients with knee osteoarthritis who met the criteria for TKA were recruited. After screening, 130 patients were enrolled based on inclusion/exclusion criteria and informed consent. During follow-up, 20 patients were excluded due to missing primary outcome data, leaving 110 patients (56 exposed and 54 non-exposed) for analysis. After PSM, 42 pairs (84 patients) were successfully matched (Figure 2). Analysis of the matched cohort revealed no significant differences in age, gender or BMI between the two groups (Table 1), indicating successful matching.
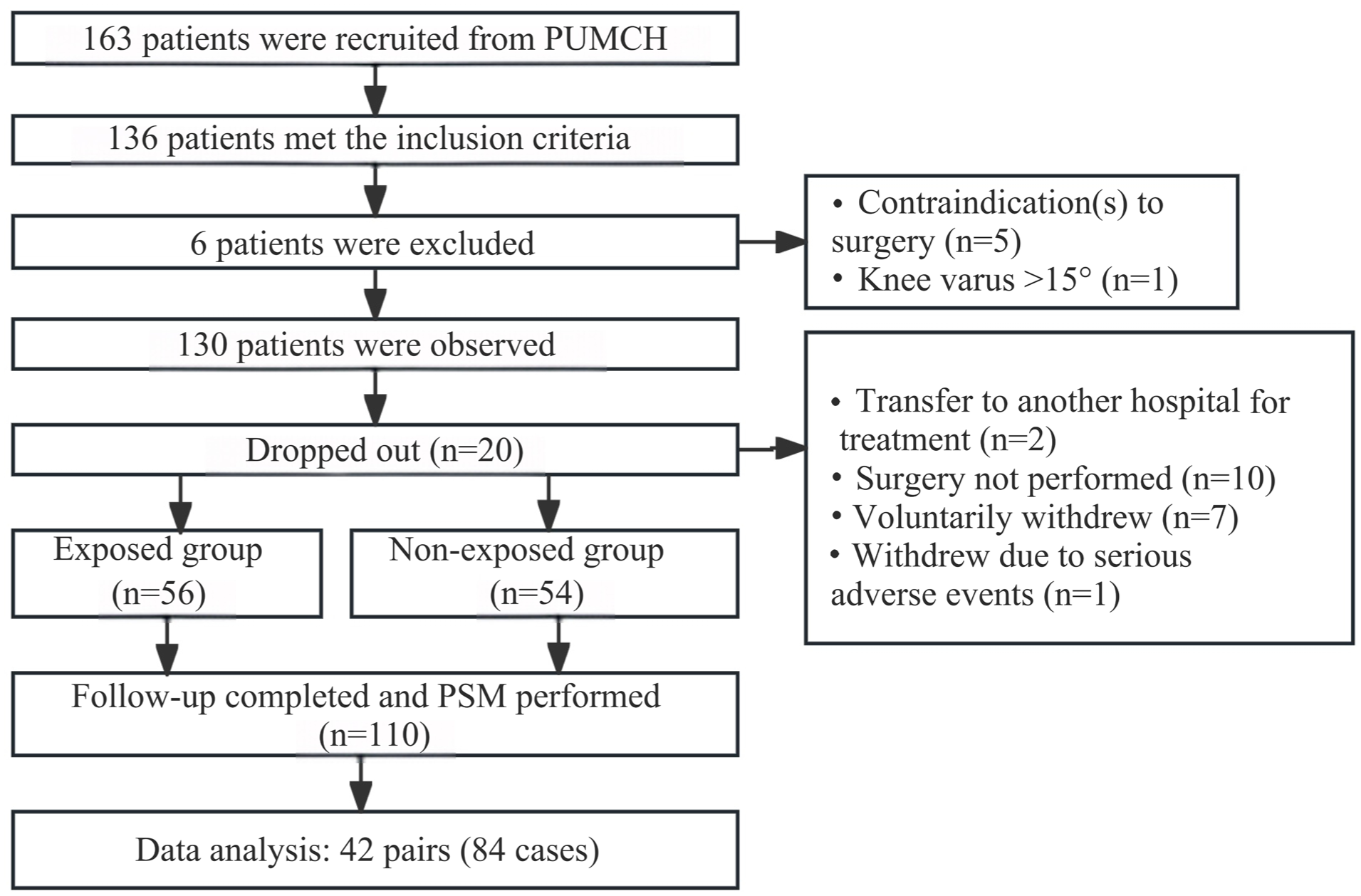
Flowchart of data screening process. PSM, propensity score matching; PUMCH, Peking Union Medical College Hospital.
Demographics and baseline characteristics.
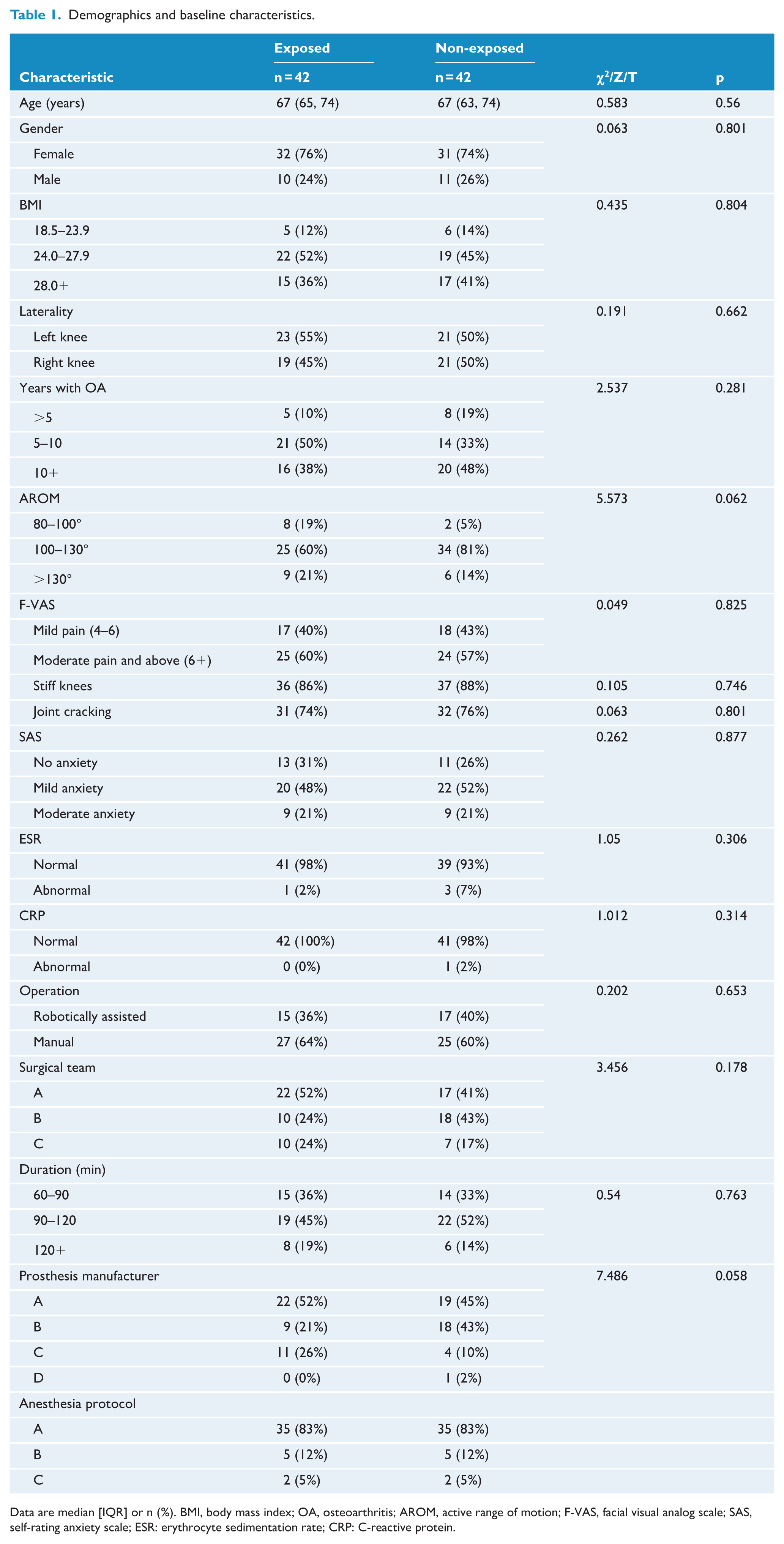
Data are median [IQR] or n (%). BMI, body mass index; OA, osteoarthritis; AROM, active range of motion; F-VAS, facial visual analog scale; SAS, self-rating anxiety scale; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein.
Multivariate analysis
Multiple regression analysis (incorporating age, gender and other relevant covariates) was conducted to identify factors influencing AROM recovery over POD 1–4. The analysis revealed that treatment group allocation (auriculotherapy exposure vs non-exposure) emerged as a statistically significant predictor of AROM improvement (p < 0.05), as visually represented in Figure 3. The model had a moderate fit (corrected R² = 0.156), indicating that it partially explained the changes in AROM (Table 2).
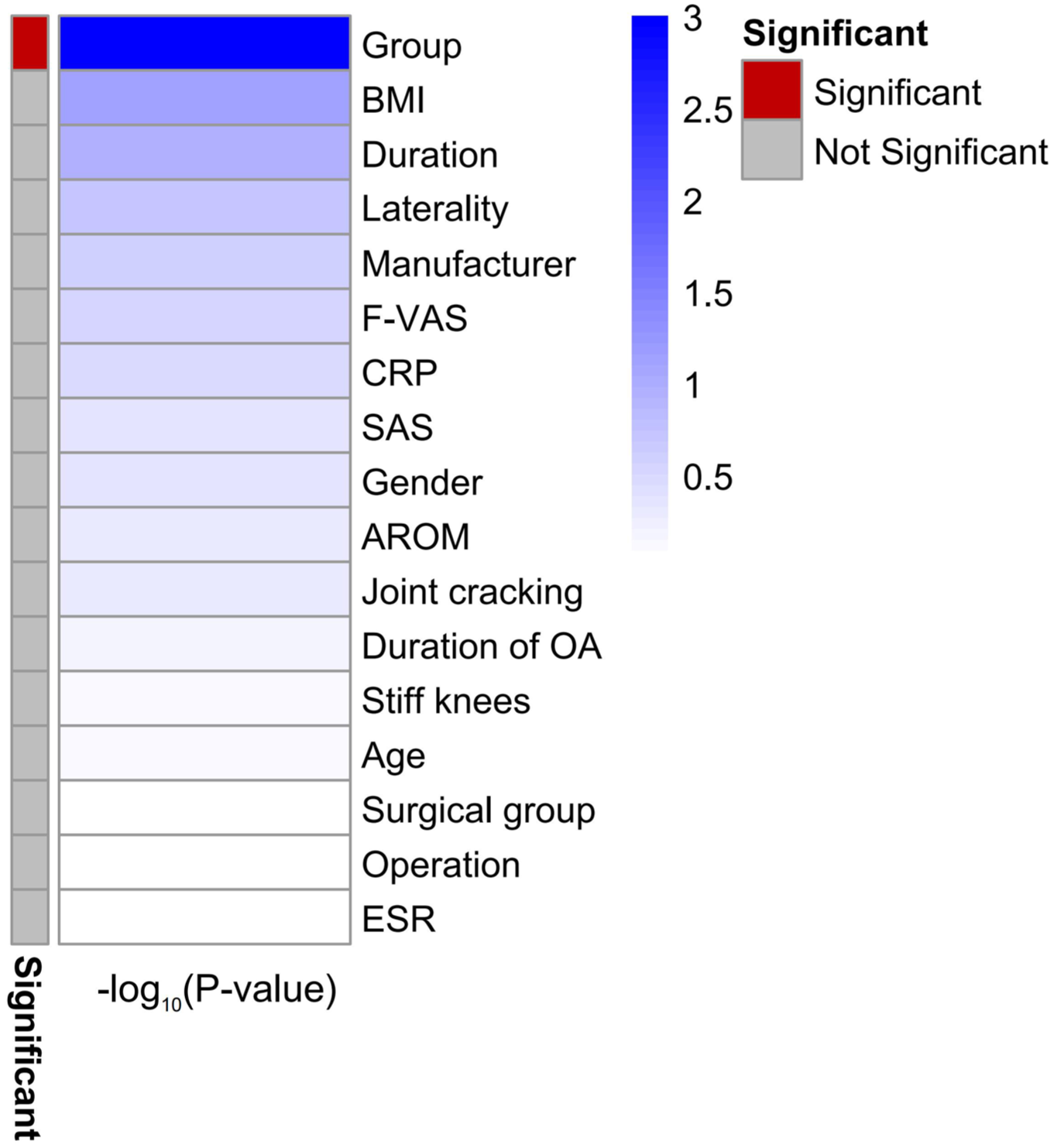
Group allocation was a significant predictor of improvement in active range of motion (AROM).
Regression analysis results for predictors of change in active range of motion.

SE, standard error; CI, confidence interval.
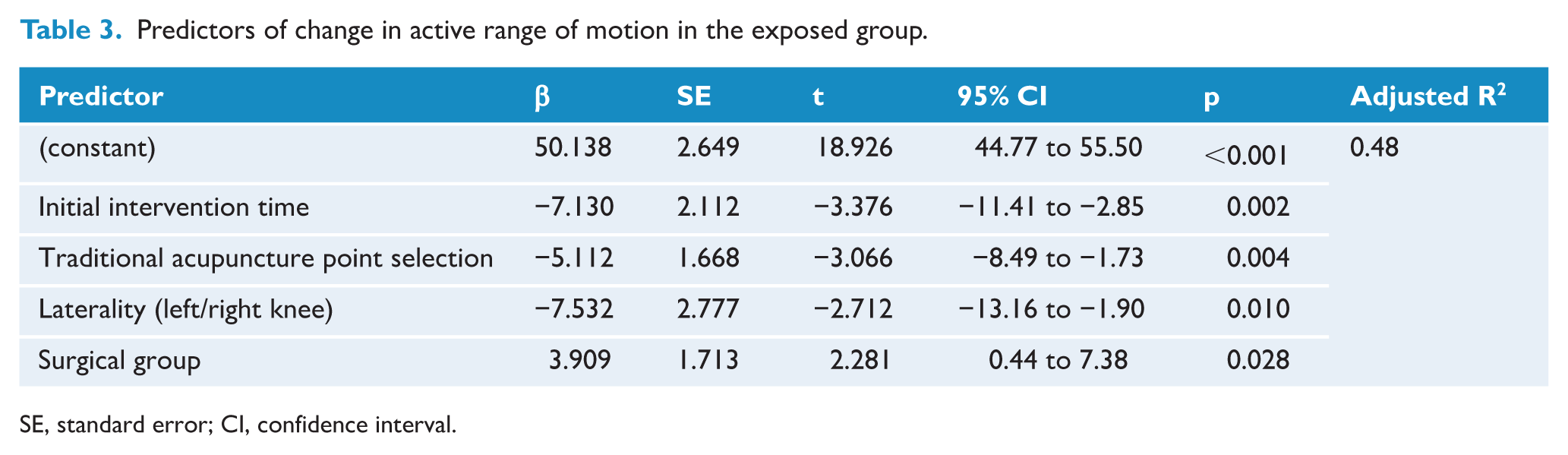
To address variations in auriculotherapy protocols, we conducted a secondary multivariate analysis focusing exclusively on the exposed group (n = 42). As all participants in this group completed the full treatment protocol—comprising two ear acupuncture sessions and two ear acupressure treatments (each involving ⩾3 daily compressions)—treatment compliance was not analyzed as a separate variable. The regression model incorporated auriculotherapy-specific parameters (including time of initial intervention and individualized selection of supplemental traditional acupuncture point locations within standardized auricular zones, illustrated in Figure 4), along with demographic variables (age, gender) and other relevant covariates, to identify predictors of joint ROM changes over POD 1–4. The results showed that the initial intervention time and individualized supplemental point selection served as highly significant predictors of the dependent variable (p < 0.01). A later initial intervention time was associated with a smaller improvement in AROM (β = −7.13, 95% confidence interval (CI): −11.41 to −2.85; p < 0.01). The final model demonstrated strong explanatory power (adjusted R² = 0.48), accounting for nearly half of the observed variance in AROM improvements (Table 3).
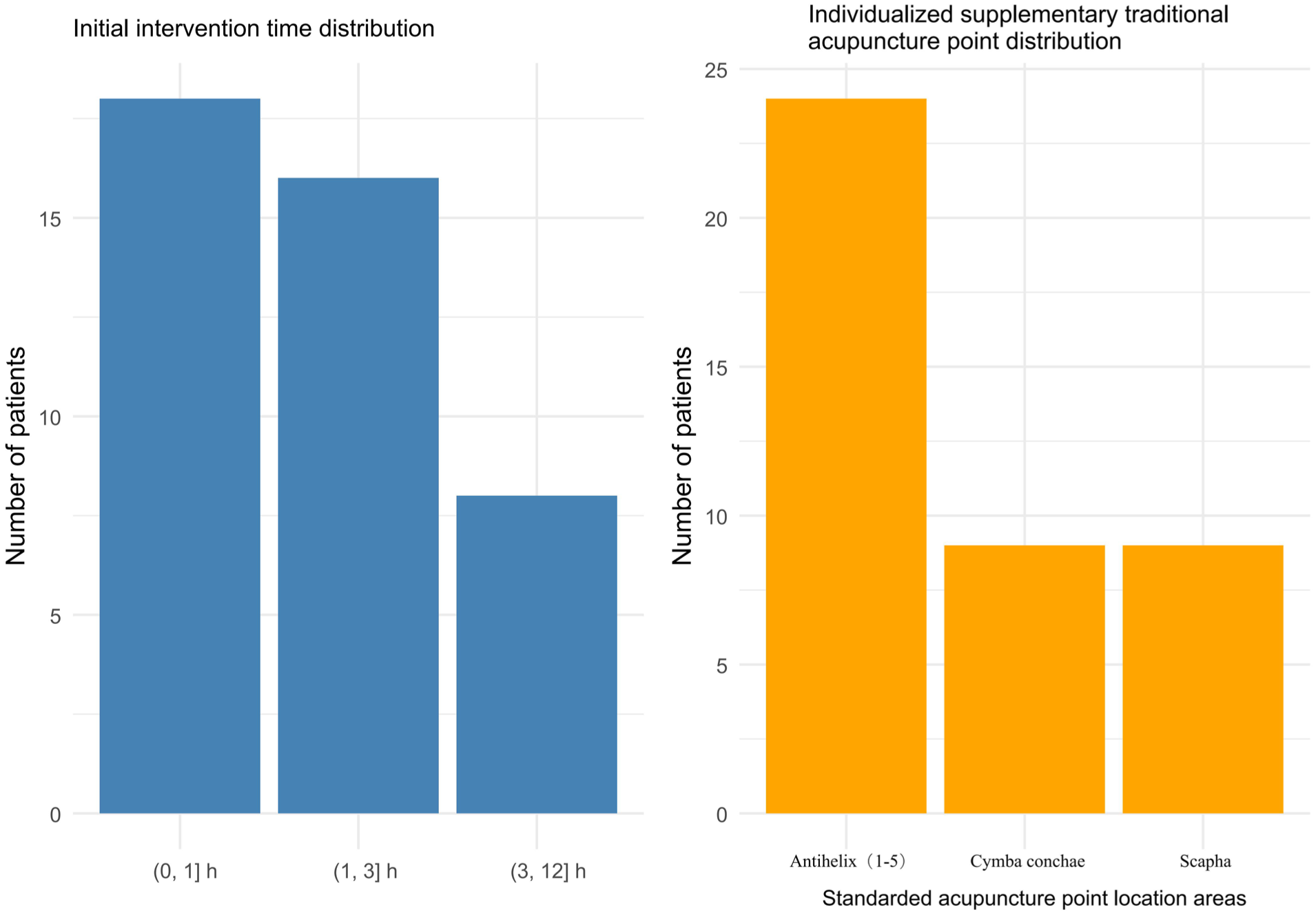
Distribution of initial treatment timing and individualized supplementary traditional acupuncture point selection in the auriculotherapy protocol.
Predictors of change in active range of motion in the exposed group.
SE, standard error; CI, confidence interval.
Comparison of outcomes
The study results showed significant differences in the change of AROM of the knee joint between the two groups from POD 1 to POD 4, with better recovery in the exposed group (40.60 ± 11.69° vs 29.41 ± 13.64°, p < 0.001). IPW analysis also yielded consistent conclusions (p < 0.001, see supplemental materials). The difference in HSS score between POD 7 and POD 14 was also significantly higher in the exposed group compared with the non-exposed group (22.60 ± 11.61 vs 15.46 ± 10.17, p < 0.05). There was no significant difference in F-VAS pain scores on POD 4 (p = 0.82). However, the exposed group had fewer PCA button presses (3.5 [0.0, 12.0] vs 11.0 [0.0, 18.0], p < 0.05), were less likely to use additional analgesics (26.2% vs 57.1%, p < 0.05) and had lower TSK scores (37.5 [36.0, 41.0] vs 48.0 [40.0, 52.0], p < 0.05). Significant differences were observed in KC and LC-1 changes between POD 1 and 4 (p < 0.05). However, no significant differences were found in LC-2 (p = 0.293), LC-3 (p = 0.127) or LC-4 (p = 0.381) changes. Due to data loss exceeding 30% for postoperative CRP and ESR measurements, these indicators were not included in the statistical analysis. The incidence of self-reported adverse events did not differ significantly between the two groups (p = 0.07). Similarly, there were no significant differences in time to ambulation (p = 0.28) or drainage volume (p = 0.16). Telephone follow-up on POD 30 revealed no significant difference in VRS pain scores between the two groups (p = 0.59; Table 4 and Figure 5).
Comparison of short-term postoperative outcomes.
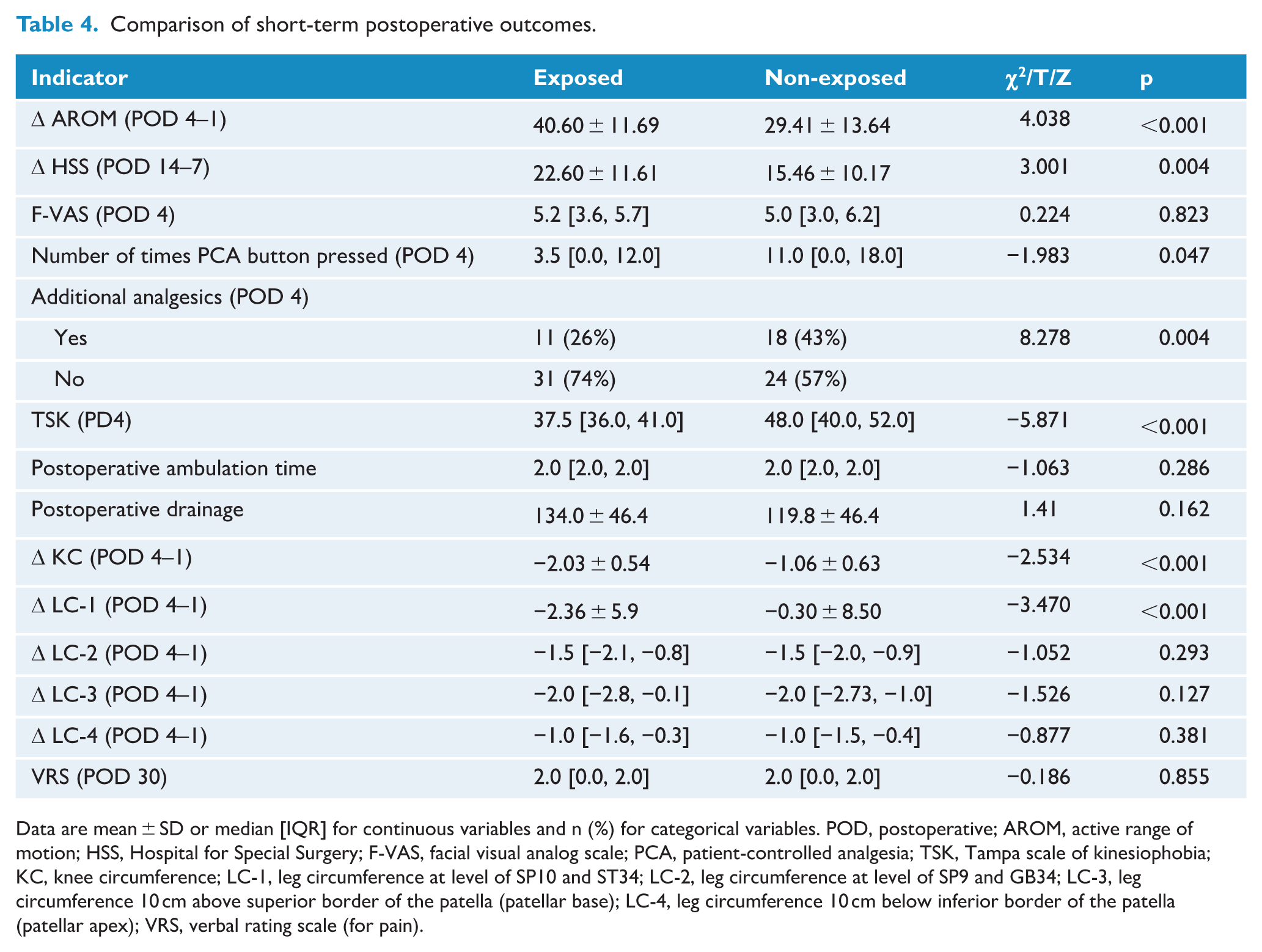
Data are mean ± SD or median [IQR] for continuous variables and n (%) for categorical variables. POD, postoperative; AROM, active range of motion; HSS, Hospital for Special Surgery; F-VAS, facial visual analog scale; PCA, patient-controlled analgesia; TSK, Tampa scale of kinesiophobia; KC, knee circumference; LC-1, leg circumference at level of SP10 and ST34; LC-2, leg circumference at level of SP9 and GB34; LC-3, leg circumference 10 cm above superior border of the patella (patellar base); LC-4, leg circumference 10 cm below inferior border of the patella (patellar apex); VRS, verbal rating scale (for pain).
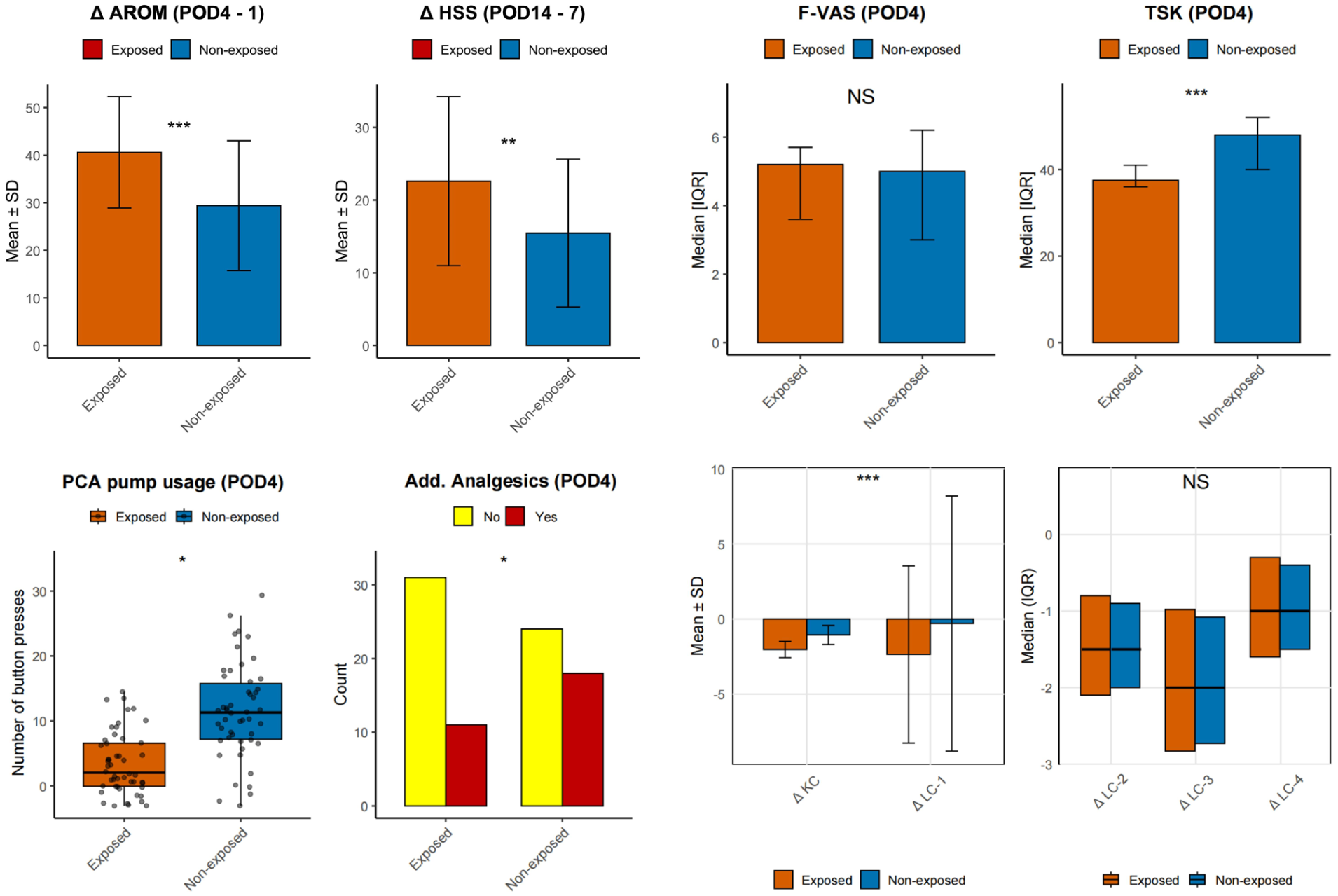
Comparison of short-term postoperative outcomes.
Trend comparison between groups
We compared the trends between groups using repeated measures analysis across multiple time points. The results showed significant time-by-group interaction effects for AROM, F-VAS score, KC, LC-1, LC-2, LC-3, LC-4 and TSK scores on POD 1–4, 7 and 14 (p < 0.05). This indicates that the improvement trends in these indicators differed between the exposed and non-exposed groups over time, suggesting that auriculotherapy influenced the trajectory of recovery. The between-group main effects for AROM and TSK scores were highly significant (p < 0.001), indicating significant differences in the changes in knee function and fear of pain between the two treatment groups. In addition, the time main effects for AROM, F-VAS, KC and TSK scores were significant across measurement time points (p < 0.05), reflecting clinically relevant changes associated with the postoperative rehabilitation process (Table 5 and Figure 6).
Results of generalized estimating equation analysis for time, group and time-by-group interaction effects on postoperative outcomes.
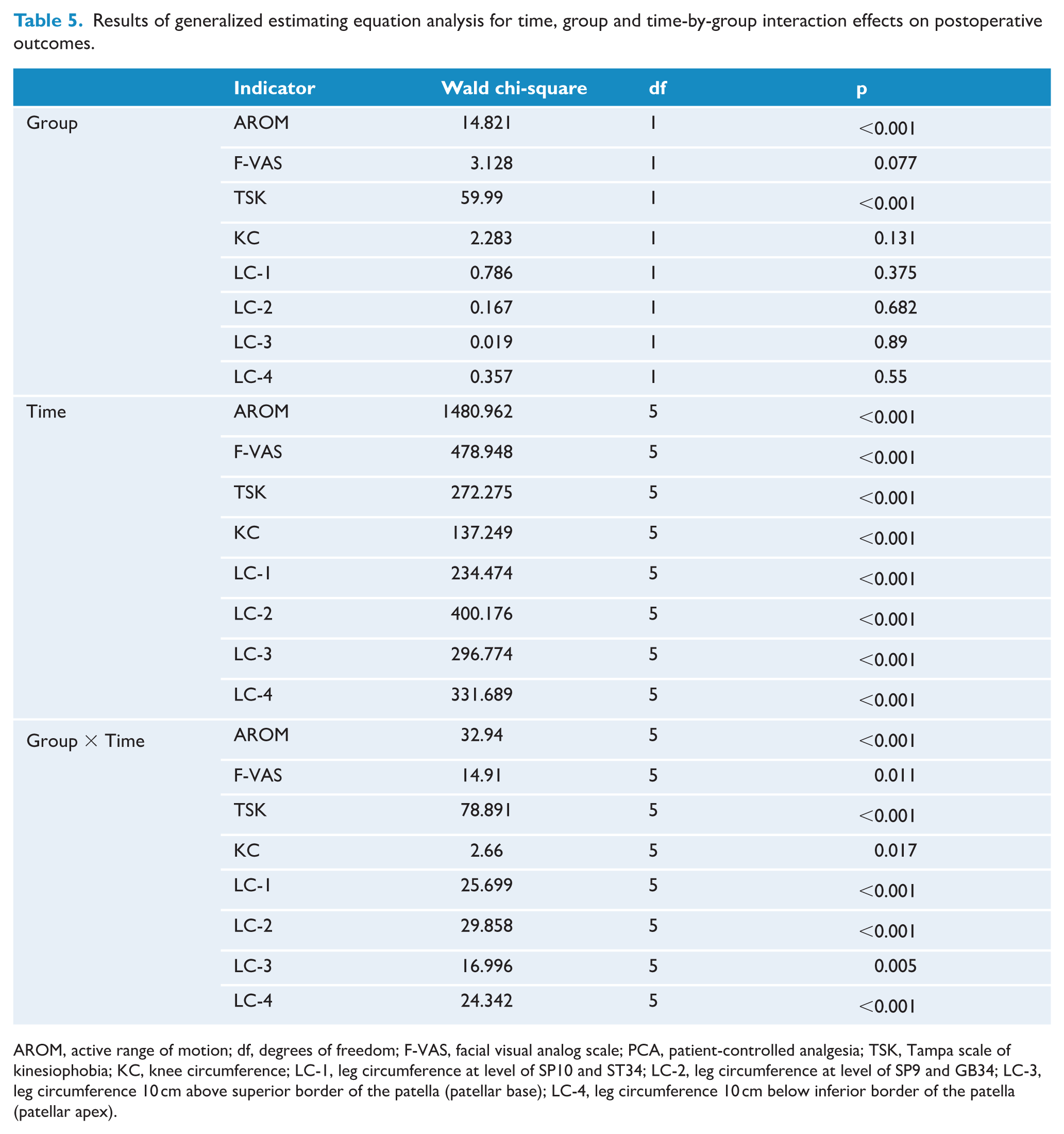
AROM, active range of motion; df, degrees of freedom; F-VAS, facial visual analog scale; PCA, patient-controlled analgesia; TSK, Tampa scale of kinesiophobia; KC, knee circumference; LC-1, leg circumference at level of SP10 and ST34; LC-2, leg circumference at level of SP9 and GB34; LC-3, leg circumference 10 cm above superior border of the patella (patellar base); LC-4, leg circumference 10 cm below inferior border of the patella (patellar apex).
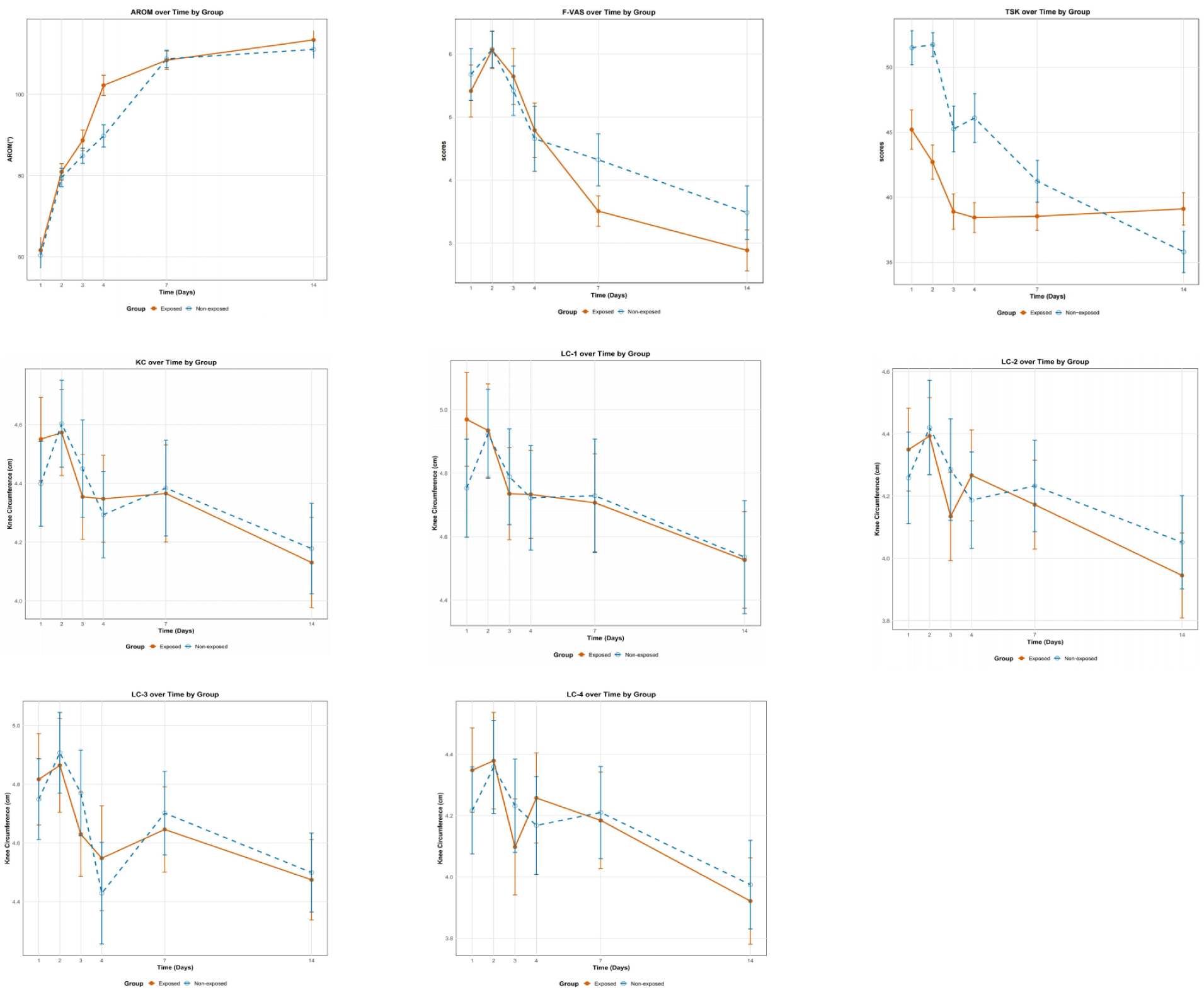
Trends in postoperative outcomes over time (presented as mean ± 95% confidence interval).
Discussion
This prospective cohort study evaluated 84 TKA patients (42 auriculotherapy-treated vs 42 controls) to assess the effects of auriculotherapy on postoperative recovery. Our findings demonstrate that auriculotherapy served as a significant predictor for improved knee joint AROM during the critical early postoperative period (POD 1–4). There was a significant inverse correlation between the timing of postoperative auriculotherapy initiation and AROM recovery (β = −7.13, 95% CI = −11.41 to −2.85; p < 0.01). Specifically, earlier auriculotherapy intervention was associated with greater improvements in AROM, a clinically important relationship that has not been sufficiently addressed in previous literature. Longitudinal trend analysis revealed consistent AROM benefits in the auriculotherapy exposed group across all measured timepoints (POD 1–4, 7 and 14), with parallel improvements in HSS scores from POD 7 to 14 (all p < 0.05). Based on the results of this study and the existing literature, auriculotherapy may promote early functional recovery after TKA through multimodal mechanisms such as pain regulation, inflammatory regulation, emotional balance and promotion of musculoskeletal function. The clinical significance of this finding and the possible related mechanisms will be further analyzed in the following sections.
Pain management and kinesiophobia
Chronic postoperative pain can seriously impair knee joint function and quality of life after TKA and also cause a heavy economic burden. 30 Early postoperative pain intensity and pain-related motor phobia are considered independent predictors of chronic postoperative pain. 31 Auriculotherapy, as a non-pharmacological treatment, can effectively alleviate postoperative acute pain and reduce the consumption of analgesics and opioids, 32 and thus reduce drug-related adverse reactions. 33 The analysis of this study revealed that, during the acute phase (POD 1–4), the application of auriculotherapy was associated with statistically significant reductions in pain intensity, decreased usage of PCA and additional analgesic medications, and a decline in the incidence of related adverse reactions. Furthermore, the treatment was significantly correlated with an improvement in kinesiophobia, as evidenced by a reduction in the TSK score (p < 0.05). This association with psychological improvement persisted until POD 14 (p < 0.001 for both interaction and between-group effects). However, no statistically significant associations were observed between the auriculotherapy treatment and the between-group comparisons of the F-VAS scores within the first 15 days postoperatively or the VRS-5 score on POD 30 (P > 0.05). These findings suggest that short-term auriculotherapy stimulation may potentially be associated with improvements in postoperative subacute pain levels and psychological state, although its long-term association with pain indicators was not confirmed in this study.
Previous studies have shown that auriculotherapy may achieve a pain-relieving effect by reducing pro-inflammatory cytokines and activating endogenous opioid systems.34,35 Auriculotherapy may also affect pain perception by enhancing patients’ sense of control (e.g. through self-selection of traditional acupuncture point locations and active acupressure), reducing the use of PCA and supplementary analgesics, and alleviating kinesiophobia. The results of this study suggest that auriculotherapy has a unique dual time-effect feature of “analgesia-anti-fear” in rehabilitation after TKA. Recent studies have shown that transcutaneous auricular vagal nerve stimulation (taVNS) may be a mechanism of action for the analgesic and anti-anxiety/depression effects of auriculotherapy. 36 Vagal nerve stimulation can regulate hippocampal inflammation, thereby reducing pain sensitivity and depression-like behavior in animal models. 37 This mechanism may underlie the observed reduction in pain sensitivity among patients in the auriculotherapy group herein. Although this study did not evaluate inflammatory biomarkers, these mechanisms would be worth exploring in future experiments through dynamic inflammatory factor detection and observation of brain function by functional magnetic resonance imaging (fMRI). In addition, acupuncture has been shown to induce neural plasticity, 38 and long-term auriculotherapy may lead to neural circuit remodeling, affecting the transmission and processing of pain signals. Increasing the frequency and duration of auricular stimulation may improve postoperative chronic pain.
Lower limb swelling
Postoperative lower limb swelling is a common complication after TKA, which is typically caused by the surgical procedure itself, as well as perioperative blood loss. 39 This swelling can lead to a decrease in quadriceps muscle strength, which is not conducive to early rehabilitation training, 40 and increases the risk of adverse events such as deep vein thrombosis.
The choice of surgical approach influences intraoperative bleeding and duration. Both bleeding and soft tissue damage can potentially contribute to postoperative swelling. Existing evidence shows that the medial patellofemoral approach involves cutting the medial thigh muscle, leading to muscle tissue damage and increased bleeding, 41 and increasing the degree of swelling. In theory, the inferior approach to the medial thigh muscle may preserve more vascular and neural structures, reduce tissue damage and bleeding,42,43 and thus reduce swelling. However, the associated increase in operative time may offset these advantages. Recent cohort studies have yielded conflicting results regarding related bleeding indicators and the two approaches show no significant difference in their long-term impact on TKA function.44,45 Since all patients in this study underwent the classic medial parapatellar approach, differences between surgical approaches were not compared. Nevertheless, this factor should be considered when interpreting swelling data in future studies.
Traditional methods for measuring lower limb swelling often involve using a tape measure to assess the circumference at specific points, such as 10 cm above and below the patella and at the patellar center (KC).46–48 However, individual differences can reduce the reliability of measurements taken 10 cm above and below the patella. To address this, we not only used these traditional methods but also selected SP10 and SP9 as reference points for measurement. These points were located using the “bone measurement method” combined with anatomical landmarks, 49 which helps minimize the impact of individual differences. This study found that auriculotherapy demonstrated a significant correlation with changes in KC at the patellar center and LC-1 (at the level of SP10 and ST34) from POD 1 to 4. This suggests auriculotherapy may help reduce post-TKA lower limb swelling. The lack of significant differences observed with other measurement methods might be because the areas around the patella and between the quadriceps muscles (LC-1 distribution area) are the most common sites of swelling after TKA. Swelling around the patella may arise from soft tissue injury, bleeding and inflammatory reactions, while that in the quadriceps muscles could be due to direct traction or incision during surgery. We speculate that the high sensitivity of these areas to swelling after TKA might explain the more pronounced differences in lower limb circumference between the two groups, indicating a potential role for auriculotherapy in reducing postoperative swelling.
It is well known that concealed blood loss and inflammation caused by surgery are important causes of lower limb swelling after TKA. 50 Prior studies have shown that auriculotherapy can inhibit the release of pro-inflammatory factors (such as tumor necrosis factor (TNF)-α and interleukin (IL)-1) through the cholinergic anti-inflammatory pathway, mediated by the vagus nerve, reduce concealed blood loss after TKA, 51 and thus alleviate postoperative joint cavity and soft tissue inflammation. This may not only directly relieve pain but may also improve joint swelling by reducing inflammatory exudates. However, studies on this aspect are relatively scarce, and the mechanism by which auriculotherapy promotes the reduction in lower limb swelling still needs further exploration.
Limitations of the study
As a single-center prospective cohort study, our results may have been influenced by hospital-specific medical conditions, surgical skills and patient population characteristics. Conducted at a renowned tertiary hospital in Beijing, China, this study ensured internal validity through standardized protocols for surgery and auriculotherapy, which were performed by senior experts. However, these protocols—along with postoperative management and patient compliance—may differ from practices in other regions or primary healthcare institutions, thereby limiting the generalizability of our findings. Furthermore, the non-randomized, patient-driven decision to receive auriculotherapy may have introduced selection bias, further constraining external validity. Although PSM was used to control for known covariates (such as age, BMI and preoperative pain score), it cannot completely eliminate the influence of unknown confounding factors. As an observational study, the aim of this research was to preliminarily explore the potential application patterns of auriculotherapy in real-world clinical settings and their association with rehabilitation outcomes, given it cannot establish a causal relationship. Future research should include high-quality RCTs and adopt a multicenter design to cover different regions, healthcare resource levels and patient populations, to further validate our conclusions and improve external validity.
Inconsistency of auriculotherapy schemes
Although we recorded and preliminarily analyzed key auriculotherapy parameters—including initial treatment time, frequency and traditional acupuncture point selection—and derived relevant conclusions, the current findings remain limited due to insufficient data granularity. Specifically, the existing data set does not permit an in-depth comparative analysis of different auriculotherapy protocols. To address this gap, future studies should incorporate larger sample sizes and systematically evaluate diverse auriculotherapy regimens following TKA. Such research is critical for establishing evidence-based, standardized auriculotherapy protocols to optimize postoperative knee rehabilitation.
Limited follow-up duration
Our study followed patients for only 30 days postoperatively, which precluded assessment of the long-term impact of auriculotherapy on functional recovery and chronic pain. Future research should extend the follow-up period to observe the long-term effects of auriculotherapy.
Insufficient exploration of biological mechanisms
Although we hypothesized that auriculotherapy may promote postoperative recovery through neuroregulation and anti-inflammatory effects, the absence of inflammatory biomarkers in our data set limited our ability to analyze these mechanisms. Future studies should incorporate the measurement of biological markers to elucidate the mechanisms underlying the effects of auriculotherapy.
Conclusion
This cohort study provides preliminary empirical evidence for the potential role of auriculotherapy in early postoperative rehabilitation after TKA. Timely treatment in auriculotherapy may be more conducive to the recovery of knee function. Auriculotherapy may promote the early recovery of knee function after TKA through various clinical mechanisms, such as relief of pain and reduced fear of movement, swelling and use of analgesics. However, due to limitations in research design, sample size and available data, further validation through high-quality RCTs is needed in the future to confirm the clinical effectiveness of auriculotherapy.
Supplemental Material
sj-pdf-1-aim-10.1177_09645284261434605 – Supplemental material for The role of auriculotherapy in early postoperative rehabilitation after total knee arthroplasty: a prospective cohort study
Supplemental material, sj-pdf-1-aim-10.1177_09645284261434605 for The role of auriculotherapy in early postoperative rehabilitation after total knee arthroplasty: a prospective cohort study by QinDong Mi, Fei Bao, XiaoLong Zhao, DeFang Zan, YuHao Liu and YunXi Xu in Acupuncture in Medicine
Footnotes
Acknowledgements
The authors would like to extend our special thanks to Professor Jin Jin’s team, Professor Lin Jin’s team and Professor Weng Xisheng’s team from the Department of Orthopedics at Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, for their strong support of this study. We are deeply grateful for their professional guidance and selfless assistance in research design, data collection and clinical practice. In addition, we sincerely appreciate the support and cooperation of all the medical staff and patients in the orthopedic ward of Peking Union Medical College Hospital. Their hard work and active participation provided a solid foundation for the successful implementation of this research.
Ethical review
Ethical approval was obtained from the Ethics Committee of Peking Union Medical College Hospital in March 2024 (approval no. I-24PJ0652).
Consent to participate
All participants provided informed consent.
Author contributions
QinDong Mi: Conceptualization, Methodology, Formal analysis, Investigation, Writing—Original Draft, Writing—Review and Editing. XiaoLong Zhao: Investigation, Data collection, Writing—Original Draft. DeFang Zan: Investigation, Data collection. YuHao Liu and YunXi Xu: Methodology, Formal analysis, Visualization, Review and Editing. Fei Bao: Conceptualization, Supervision, Investigation, Funding acquisition, Writing—Original Draft, Writing—Review and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article:This work was supported by the Sedimentation Research Funding Integration Entrustment Project of Peking Union Medical College Hospital (grant no. ZC201903189).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.