
Abstract
Background:
Postherpetic neuralgia (PHN) is a prevalent and painful complication following herpes zoster infection, impacting patient quality of life and posing significant treatment challenges. Current pharmacological approaches often result in adverse effects. The aim of this study was to develop a clinical prediction model for selecting PHN patients for electroacupuncture (EA) treatment and to determine the prognostic outcomes after two sessions.
Methods:
We conducted a retrospective observational cohort analysis on adults diagnosed with PHN between 2010 and 2017. All participants had undergone at least two acupuncture sessions. Data analysis included demographic, clinical and treatment variables to identify predictors of treatment outcomes. Treatment success was defined using the numeric rating scale (NRS), with failure characterized by an NRS score >3. Predictive modeling and internal validation employed bootstrap resampling.
Results:
Among 243 patients included in the study, the treatment failure rate was 20.6%. Key predictive factors for treatment outcome were the presence of diabetes mellitus, use of carbamazepine and high initial NRS scores. The accuracy of the prediction model was reflected by an area under the receiver operating characteristic (ROC) curve of 0.80 after the first session and 0.88 following the third session, indicating a robust predictive capability.
Conclusion:
In this study, we successfully developed and internally validated a clinical prediction model for EA in PHN patients. We anticipate that this model may guide clinicians in personalized patient care, optimizing the selection process for EA treatment, and predicting treatment response early in the treatment cycle.
Keywords
Introduction
Postherpetic neuralgia (PHN) has emerged as the principal complication following herpes zoster infection, with a prevalence rate of approximately 15% among affected individuals; it can lead to substantial neuralgia, heightened anxiety levels and a reduction in quality of life. 1 The incidence rate of PHN has been quantified at 5 per 1000 patient-years. The diagnosis of PHN typically occurs within a 3-month period following the onset of the herpes zoster rash. Recurrence of herpes zoster infection (shingles) is classically characterized by a dermatomal distribution of vesicular eruptions that is associated with neuropathic pain within the affected dermatome due to the destruction of peripheral nerves. 2 Beyond the physical implications, PHN exacts a significant economic burden, with an estimated per capita lifetime cost of $250 (USD) in developed nations.1,3,4
Therapeutic strategies for PHN often encompass a range of pharmacological treatments, including voltage-gated calcium channel (VGCC) α2-δ ligands, tricyclic antidepressants (TCAs), serotonin-norepinephrine reuptake inhibitors (SNRIs), non-steroidal anti-inflammatory drugs (NSAIDs), weak opioids, capsaicin, local anesthetics (LAs) and intrathecal steroid injections. 5 Despite the plethora of pharmacological options, the associated adverse effects—which are contingent on the mechanisms of action—have led some patients to pursue non-pharmacological treatments with neuromodulation methods, such as scrambler therapy and Chinese acupuncture.
Scrambler therapy, also known as Calmare therapy, is a non-invasive pain management technique that uses a device to deliver a low-frequency electrical stimulation to the nerves. This therapy aims to relieve chronic neuropathic pain by “scrambling” or altering the pain signals sent by damaged nerves to the brain. The process involves attaching electrodes to the skin near the area of pain. The device then delivers electrical impulses that mimic non-painful signals to the nerves, essentially confusing the brain and reducing the perception of pain. Scrambler therapy is often used to treat various types of chronic pain conditions, including neuropathic pain, without the use of medications or invasive procedures.6,7
Ten-session Chinese acupuncture has been posited as an alternative therapeutic avenue for PHN. This modality shares a similar mechanism of action to that of other neuropathic pain treatments,8–12 purportedly inducing peripheral nerve microinjury and muscle relaxation. 10 The 10-session Chinese acupuncture protocol may vary slightly depending on the practitioner and the specific needs of the patient, but it generally involves inserting acupuncture needles at specific traditional acupuncture point locations to promote pain relief. The frequency and duration of the sessions can also vary based on individual responses and the severity of the condition. Acupuncture practices from China, including electroacupuncture (EA) with filiform or fusiform needles, as well as the use of press needles, have gained popularity for managing neuropathic pain globally, especially in cases of PHN. However, the effectiveness of these methods is believed to vary depending on the individual patient. 13
Variability in acupuncture outcomes is notable,8,9 with studies presenting both support for acupuncture and opposition. Physiatrists are tasked with balancing patient preferences and treatment responses, tailoring approaches to individual susceptibilities. There is a notable absence of a predictive model for treatment failure in patients undergoing acupuncture for PHN. Consequently, this study aimed to develop and internally validate a clinical prediction model designed to: (1) select PHN patients for the initiation of acupuncture therapy; and (2) provide prognostic information after two acupuncture treatment sessions.
Methods
The study employed a retrospective observational cohort design, designated PROGRESS 3, which involved a secondary analysis of data sourced from a prior efficacy study related to PHN treatment. 13 The purpose of this secondary analysis was to delve deeper into the factors influencing treatment outcomes, particularly regarding the use of EA treatment for PHN. 14
The cohort comprised adults (age >18 years) who had received a diagnosis of PHN between 2010 and 2017 and who were candidates for acupuncture treatment, having completed a minimum of two EA treatment sessions. The technique employed filiform or fusiform needles inserted at traditional acupuncture point locations, including Jiaji, in the corresponding affected dermatomes, as well as Ah shi points. The needles were then stimulated with electrical current for 20 to 30 min per session. Due to concerns regarding iatrogenic pneumothorax with needle insertion into the thorax and upper back, press needles (0.22 mm in diameter and 1.3 mm in length) were recommended. This type of needle minimizes pain and enhances patient comfort during treatment and can remain in place for 5–7 days. For PHN patients experiencing thoracic pain, using a press needle may offer a safer alternative to mitigate potential complications.
The operational definition of treatment failure was a numeric rating scale (NRS) score <3, either at the last visit or upon completion of the 10th session (Figure 1).15,16 Generally, an NRS score of 0 to 3 is considered indicative of a non-burden level, suggesting mild or no pain. Therefore, we defined treatment failure as patients’ NRS scores remaining >3 after treatment. This approach aligns with commonly used thresholds in pain assessment to distinguish between manageable and burdensome levels of pain. 17 The analysis did not exclude participants lost to follow-up after the initial two sessions, assuming that their last recorded NRS scores remained constant. This decision was based on the observation that patients with little or no pain often decline further acupuncture sessions. In addition, it is not typically recommended that patients with consistently low NRS scores undergo additional acupuncture treatment. These patients continued to be monitored by their primary care physicians at Chiang Rai Regional Hospital and were instructed to return to the acupuncture clinic if their pain intensified.
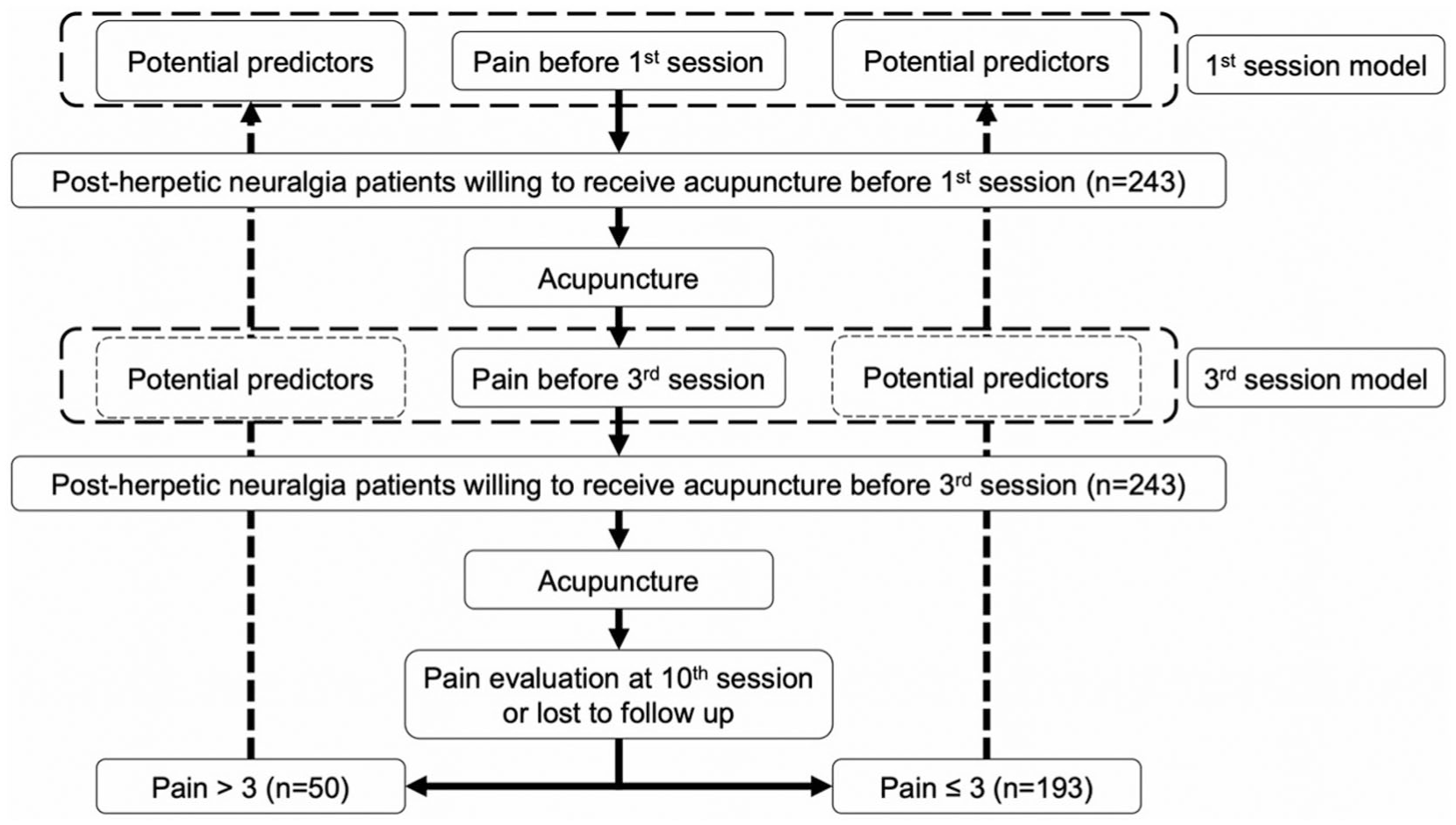
Study flow diagram.
This methodological choice was consistent with the last observation carried forward (LOCF) approach. Given the comparable efficacies of press needles and traditional filiform/fusiform needle EA, these treatment modalities were consolidated for analysis purposes. 13 Potential prognostic indicators were extrapolated from a prior study, 13 and the predictive performances between the first and third treatment sessions were compared.
The predictive models underwent internal validation through bootstrap resampling techniques. Bootstrap resampling is a statistical technique that is used to estimate the distribution of a statistic by repeatedly resampling with replacement from the observed data. This method is particularly useful when the true distribution of a statistic is difficult to determine analytically or when the sample size is small. From the original sample of data, random samples (called bootstrap samples) are drawn with replacement. This means that each observation can be selected multiple times or not at all in each bootstrap sample. The statistic of interest is calculated for each bootstrap sample. By repeating this process many times, a distribution of the statistics is generated. This distribution represents the variability of the statistic and can be used for hypothesis testing, confidence interval (CI) estimation and other statistical inference tasks. 18
The Ethical Committee for Research in Human Subjects of Chiang Rai Regional Hospital approved the study.
Statistical analysis
Categorical variables were summarized by frequencies and percentages and evaluated using Fisher’s exact test. Continuous variables adhering to a normal distribution were described by means and standard deviations and assessed via independent t-tests. Non-normally distributed continuous variables were characterized by medians and interquartile ranges, and the Mann–Whitney U test was applied for analysis. All statistical inferences were framed within 95% two-sided CIs, with p < 0.05 delineating statistical significance. Multivariable logistic regression analyses were conducted with a pre-selection process utilizing a stepwise elimination algorithm informed by clinical relevance and practicality. The potential predictors considered for analysis comprised gender (female), age (elderly, >65 years), diabetes mellitus (DM), pain duration >1 month, utilization of carbamazepine, gabapentin usage, absence of capsaicin gel use, and pain intensity >7 at the first session. All statistical procedures and model development were executed using Stata version 18.0 (StataCorp LLC, College Station, TX, USA).
Results
The study encompassed a total of 243 patients with PHN from January 2010 to December 2017. The treatment failure rate was observed to be 20.6%, with DM, carbamazepine use and initial NRS scores >7 identified as significant differentiators (Table 1). These factors were found to be associated with treatment failure in acupuncture treatment for PHN patients.
Patient characteristics.
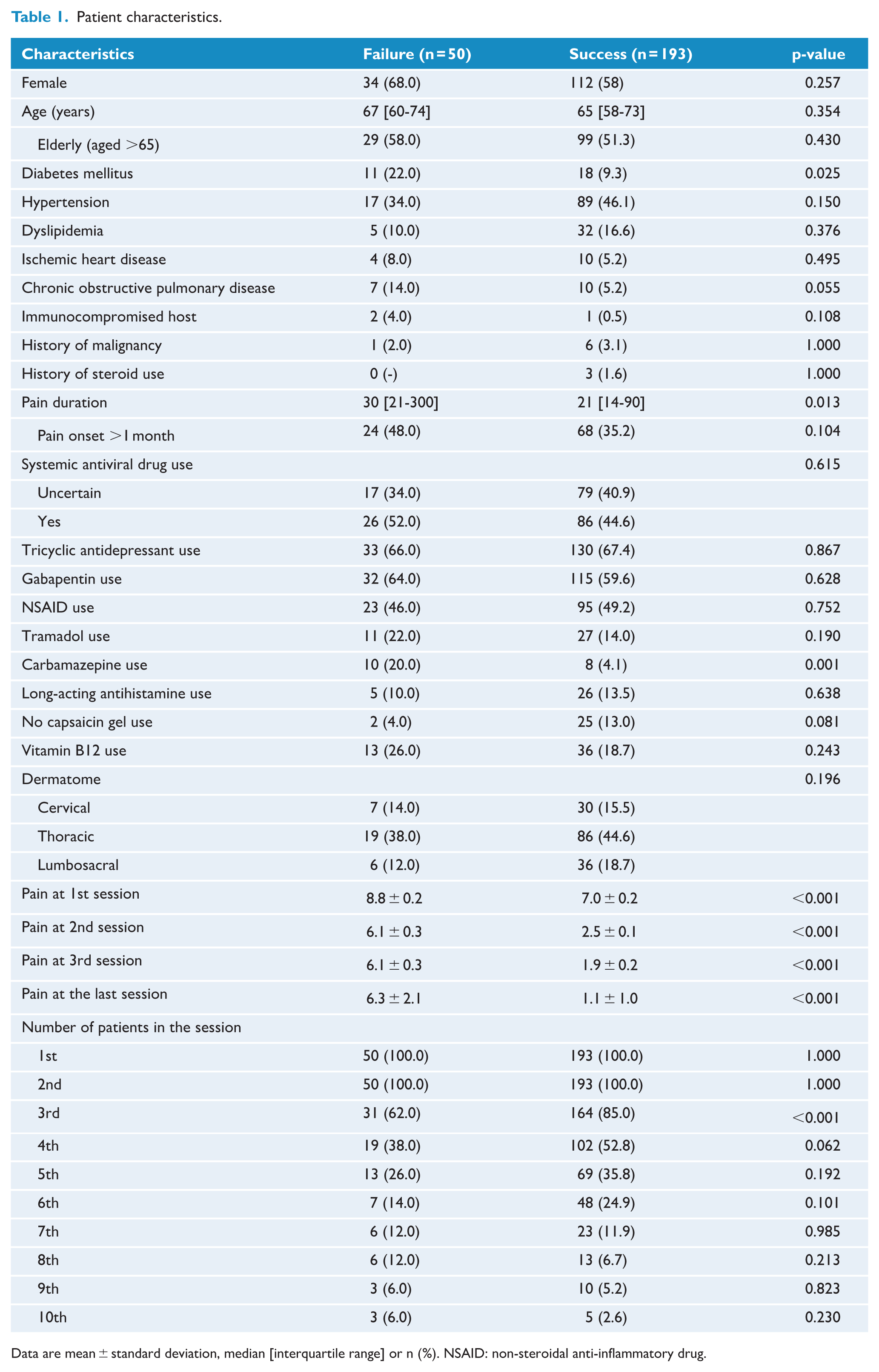
Data are mean ± standard deviation, median [interquartile range] or n (%). NSAID: non-steroidal anti-inflammatory drug.
Predictive factors were selected in the first treatment session model using a parsimonious stepwise backward elimination process. Baseline characteristic differences were identified, including gender, age, DM, duration of pain exceeding 1 month, carbamazepine use, gabapentin use, capsaicin gel use and initial session NRS score >7 (Tables 2 and 3). The predictive models, formulated through logit linkage, demonstrated notable cut-off points that balanced clinically acceptable rates of false positives and false negatives (Figure 2). The third-session model exhibited superior discriminatory capacity in predicting treatment failure compared to the initial model, incorporating pain intensity prior to the third acupuncture session (Figure 3). Prevalence-based cut-off points delineated high-risk and low-risk patient cohorts (Table 4).
Univariable analysis of the first treatment session model.
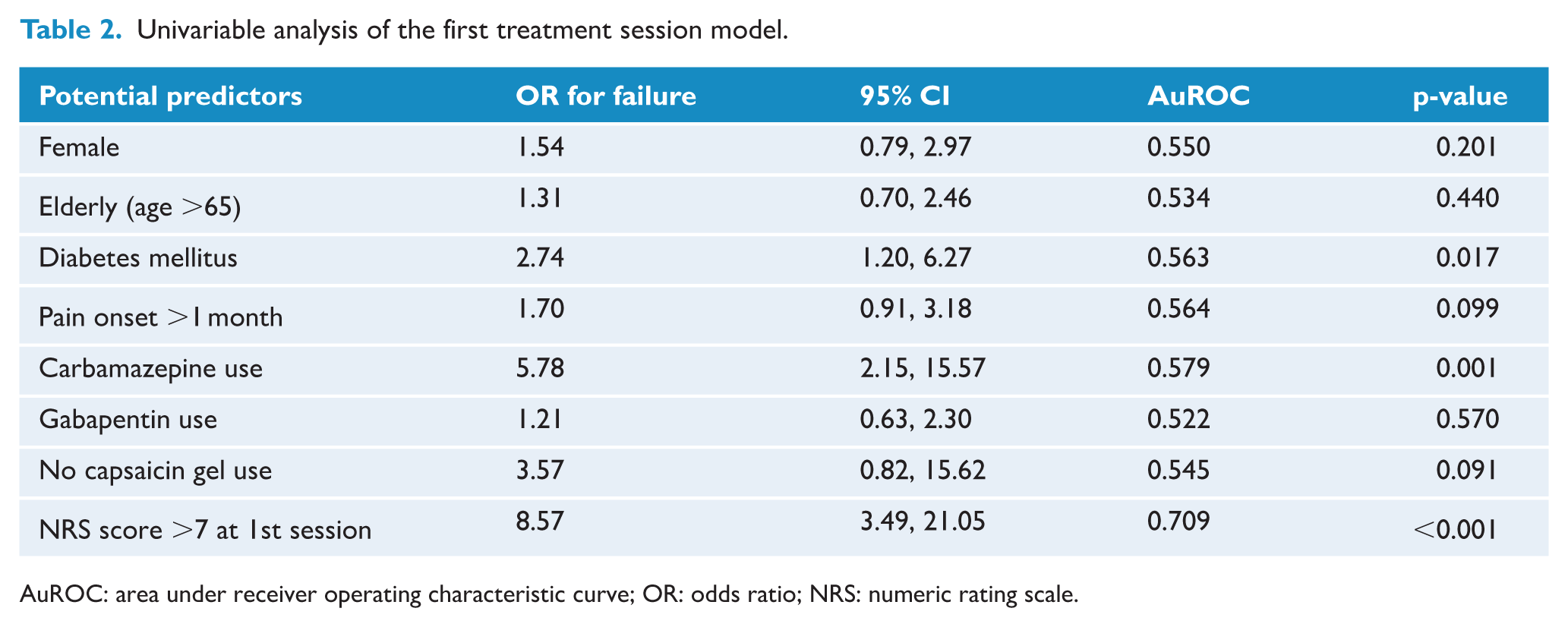
AuROC: area under receiver operating characteristic curve; OR: odds ratio; NRS: numeric rating scale.
Multivariable analysis.
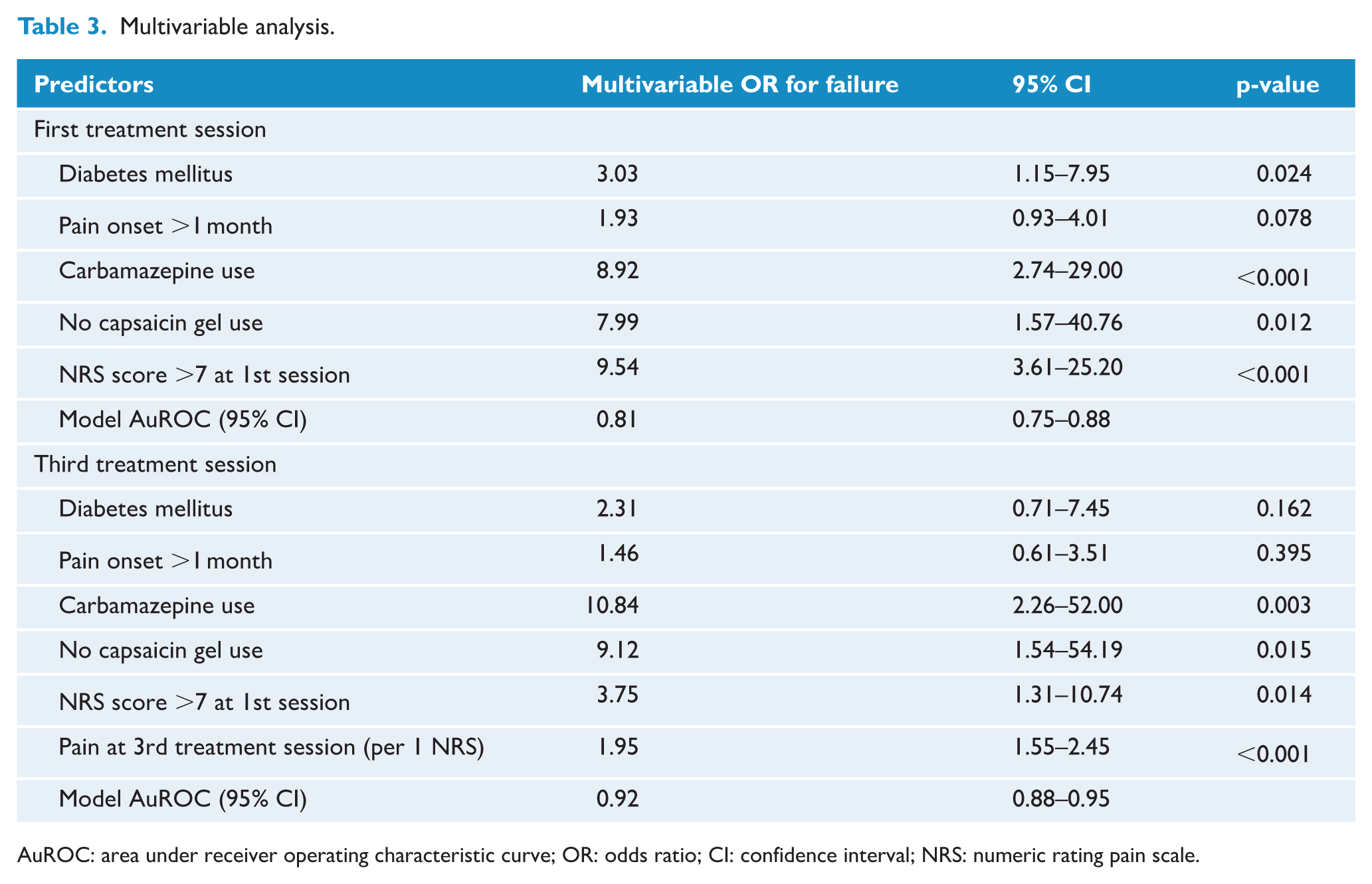
AuROC: area under receiver operating characteristic curve; OR: odds ratio; CI: confidence interval; NRS: numeric rating pain scale.
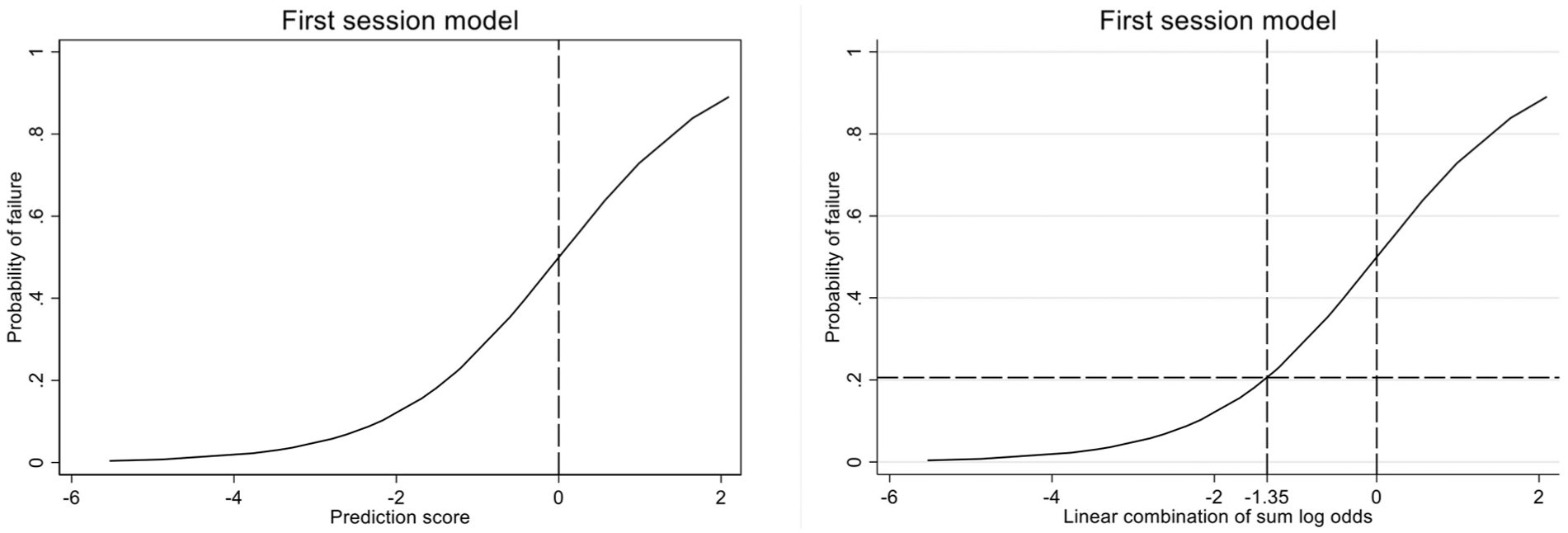
Risk curve with prevalence-based cut-off point.
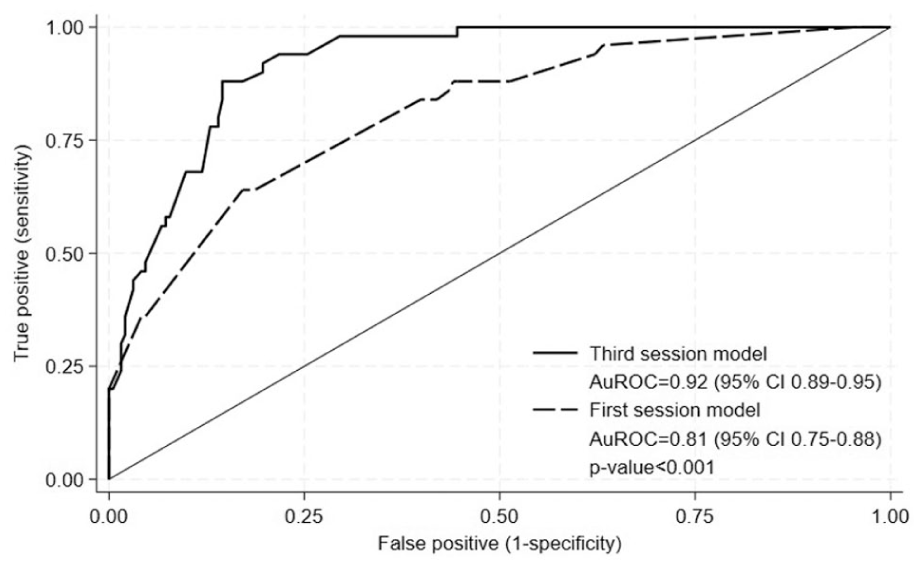
Comparative receiver operating characteristics curve of the first- and third-session models. Abbreviations: AuROC: area under receiver operating characteristic curve; CI: confidence interval.
Prediction model diagnostic classification properties.
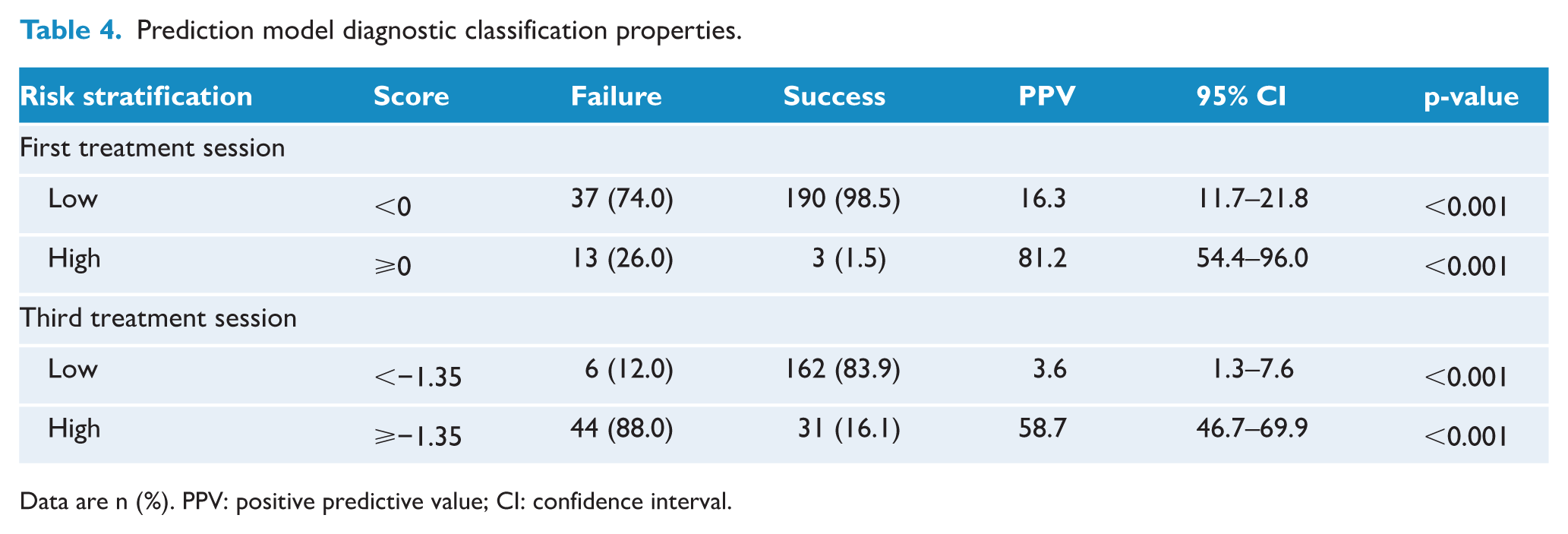
Data are n (%). PPV: positive predictive value; CI: confidence interval.
Internal validation of the first-session model through 200 bootstrap resampling replications yielded an area under the receiver operating characteristic (ROC) curve of 0.80 (95% CI: 0.74–0.87), with heuristic shrinkage of 0.913. The third-session model achieved an area under the ROC curve of 0.88 (95% CI: 0.84–0.94), with a similar shrinkage factor (0.910). Calibration plots for both models suggested adequate fit (Figure 4). The third-session model outperformed the initial model in decision curve analysis, providing enhanced guidance for post-treatment decision-making (Figure 5). A standard deviation bar plot correlated increasing NRS scores with an escalated likelihood of treatment failure (Figure 6).
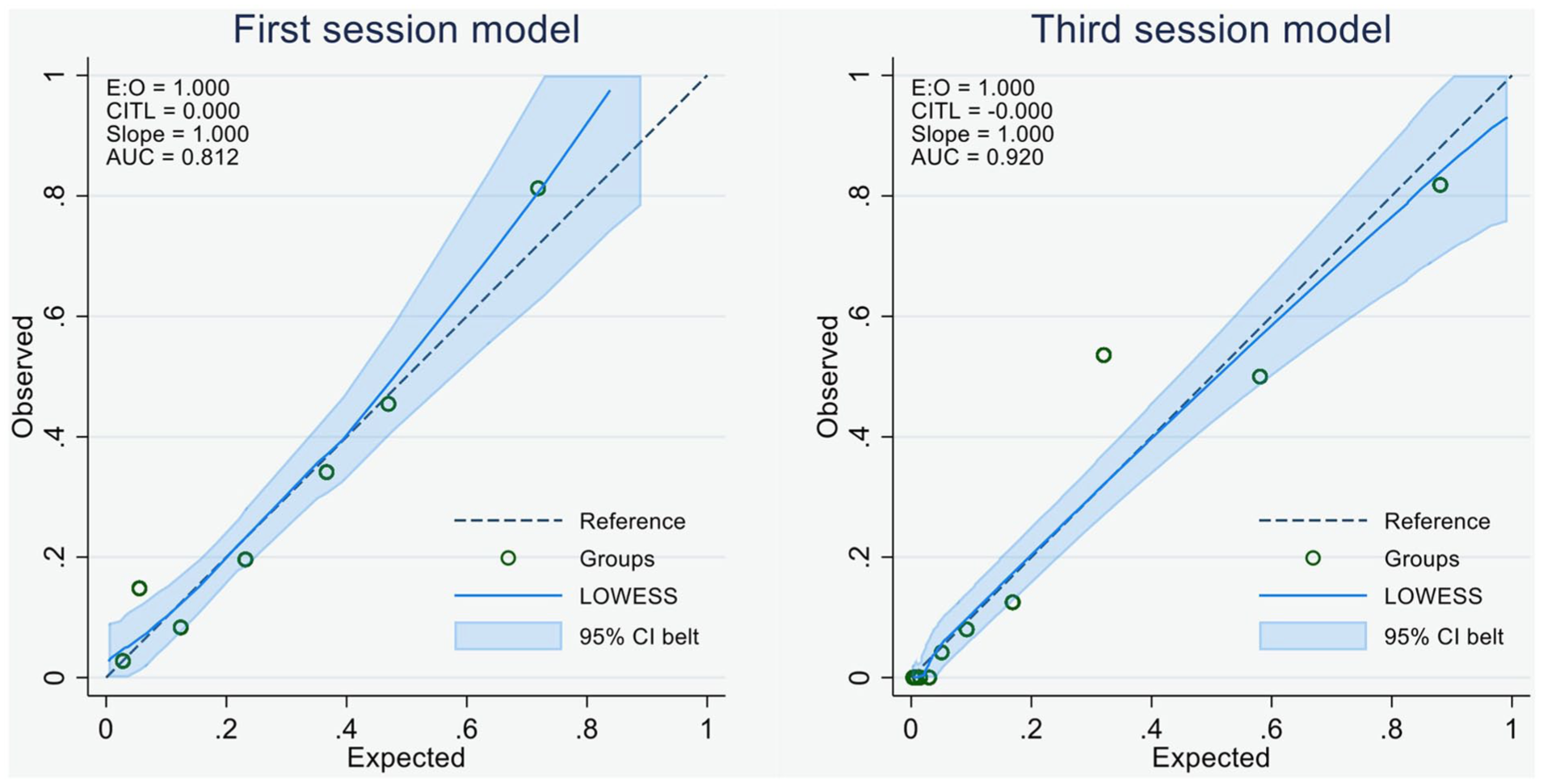
Calibration plot. Abbreviations: E: O: expected:observed ratio; CITL: calibration-in-the-large; AUC: area under the curve; LOWESS: locally weighted scatterplot smoothing; CI: confidence interval.
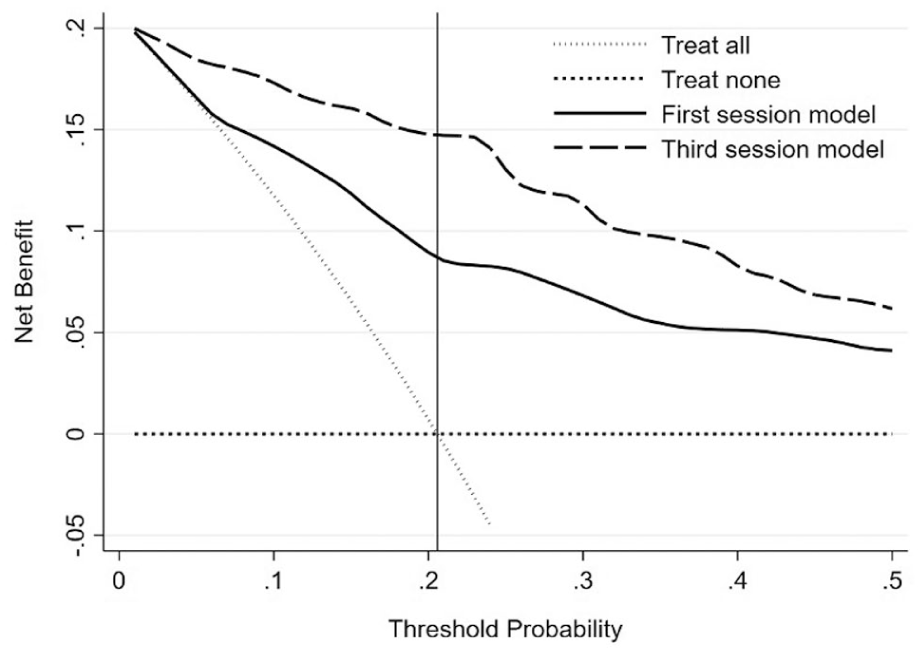
Comparative decision curve analysis.
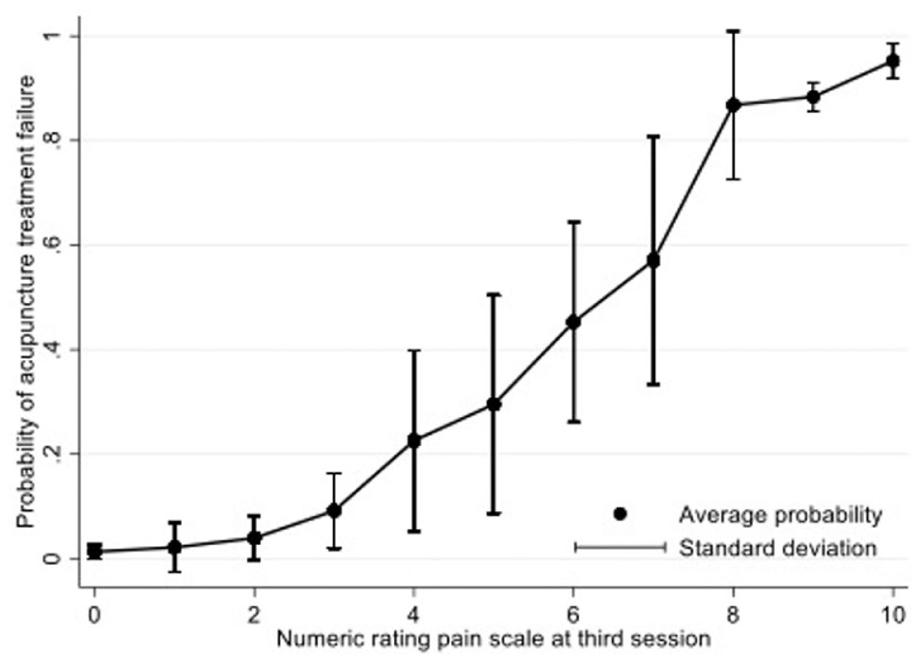
Acupuncture treatment failure average probability with standard deviation.
Discussion
The findings of this study contribute significantly to the extant literature concerning the prognostic factors affecting outcomes and efficacy in managing PHN. Specifically, our analysis revealed an association between treatment failure in acupuncture treatment for PHN patients and the presence of DM, utilization of carbamazepine and higher initial NRS scores. These results align with previous investigations, highlighting the pivotal role played by DM in delaying nerve healing processes and predisposing to the development of PHN.19–21 The chronic hyperglycemic state characteristic of DM is known to induce enduring vascular abnormalities, particularly within the microcirculatory system, which is critical for peripheral nerve function. 22 This correlation emphasizes the necessity of accounting for comorbidities, such as DM, when assessing prognostic indicators for PHN outcomes and devising tailored acupuncture treatment plans.
Carbamazepine utilization has waned among healthcare providers owing to the potential for severe cutaneous adverse drug reactions. 23 Typically, physicians reserve carbamazepine as an adjunctive therapy for PHN patients who exhibit inadequate responses to gabapentin and TCAs. Consequently, PHN patients who were prescribed carbamazepine in our study were deemed more likely to be experiencing more severe and persistent forms of pain. This hypothesis suggests a heightened likelihood of treatment failure with acupuncture in these patients.
The use of capsaicin gel, available over-the-counter and used on an as-needed basis, showed a reverse relationship with treatment failure. The mechanism of action of capsaicin, which reduces pain sensitivity by desensitizing sensory neurons, underscores the intricate balance between patient-driven symptom control and treatment outcomes. 24 There is potential for capsaicin to complement acupuncture in alleviating pain for PHN patients, but scientific evidence is required to substantiate this hypothesis.
Severe neuropathic pain, as measured by a NRS score >7, signifies complex pain mechanisms. This level of pain severity goes beyond being a symptom; it mirrors the underlying pathophysiology that could forecast the difficulty of PHN. 25 Starting a multimodal treatment approach early could help prevent treatment failure in these PHN patients.
The discriminative capability of the predictive models was enhanced by including pain assessments conducted before the third session of acupuncture. This suggests that early treatment responses are pivotal in predicting long-term outcomes, supporting the notion of dynamic treatment planning. Adherence to treatment until the third session allowed for more informed prognostication, which may have implications for optimizing treatment strategies and resource allocation.
Strengths
The strengths of this study begin with the utilization of routine clinical practice data, which reflects real-world settings and provides insights that are immediately applicable to patient care. The selection of prognostic factors was based on pragmatic criteria, focusing on variables readily assessable in primary care settings before referring patients for specialized acupuncture treatments. The consistency in acupuncturist expertise and the uniformity of the dataset from which both models were developed add to the robustness of the findings. The clinical endpoint (NRS for pain) is a widely accepted and practical measure for pain assessment, further underscoring the applicability of the experimental results.
Limitations
Despite the aforementioned strengths, the retrospective nature of the study design introduces inherent limitations. The inability to capture NRS scores for patients lost to follow-up could introduce bias, and the focus on only two acupuncture techniques might limit the generalizability of the results to broader acupuncture practices.
Conclusion
In summary, our study provides a validated predictive model for the treatment of PHN with acupuncture, emphasizing the importance of individualized patient care and the need for dynamic treatment strategies responsive to early indicators of treatment success or failure.
Footnotes
Acknowledgements
The authors wish to thank the committee of Chiang Rai Regional Hospital Research Unit.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.