
Abstract
Background
Periocular acupuncture is a traditional Chinese medical therapy that has been employed for various ocular and systemic conditions.1,2 However, due to proximity to the eyeball, improper technique or an atypical eye structure of the patient may lead to serious ocular complications. 3 Patients with high myopia are at increased risk due to thinner sclera, vitreous liquefaction and peripheral retinal degeneration. 4 Herein, we present a detailed case of multiple retinal breaks and vitreous hemorrhage following periocular acupuncture, with emphasis on the role of serial optical coherence tomography (OCT) in diagnosis, monitoring natural healing and guiding treatment.
Case description
A 51-year-old woman presented to the emergency department with a sudden onset of decreased vision and floaters in her right eye for the preceding 4 hours. The symptoms had begun immediately after undergoing bilateral periocular acupuncture. Her past ocular history was significant for bilateral high myopia (spherical equivalent –15 diopters) and a history of choroidal neovascularization in the left eye, for which she had received an intravitreal anti-vascular endothelial growth factor (VEGF) injection 2 weeks prior.
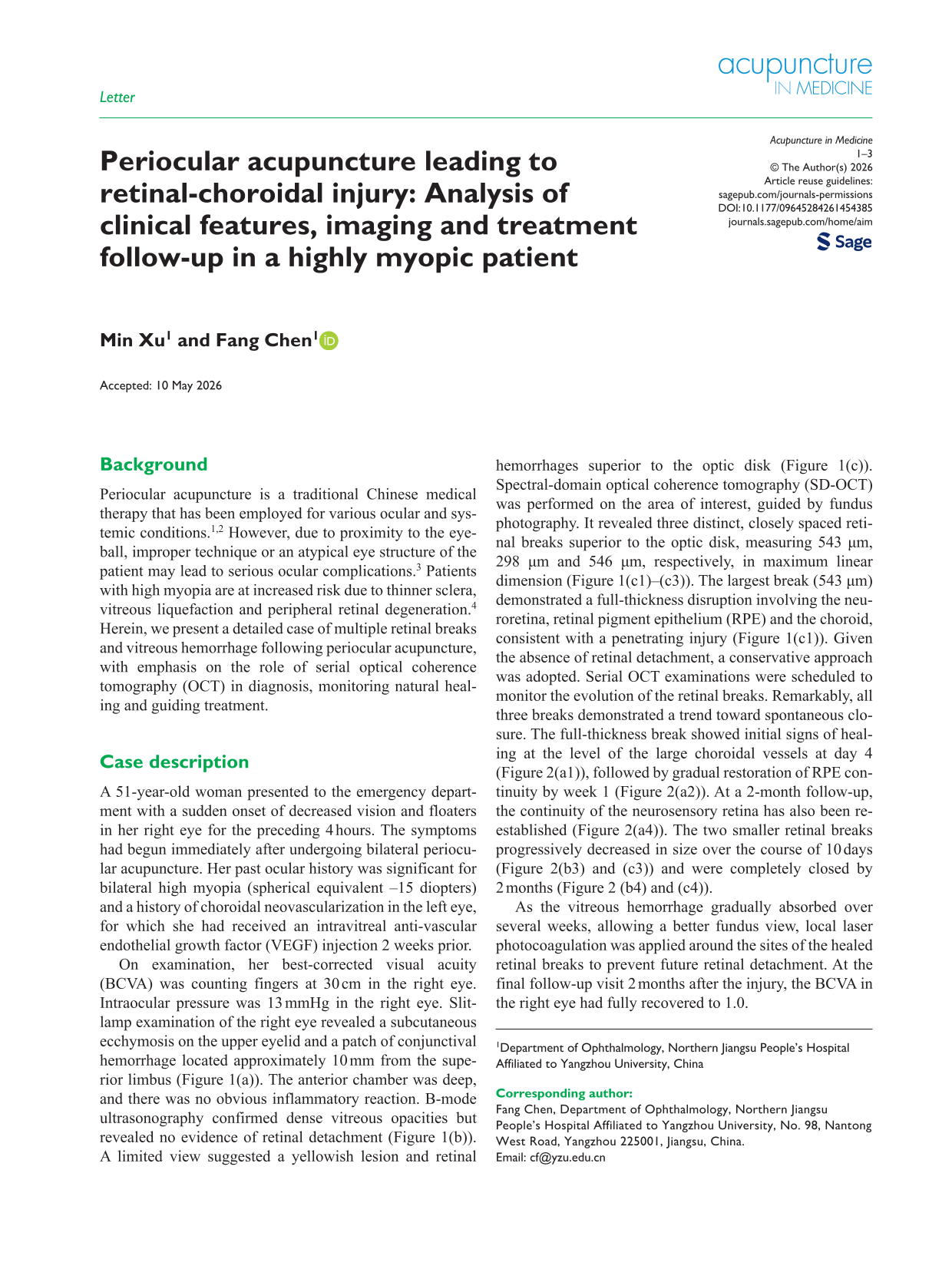
On examination, her best-corrected visual acuity (BCVA) was counting fingers at 30 cm in the right eye. Intraocular pressure was 13 mmHg in the right eye. Slit-lamp examination of the right eye revealed a subcutaneous ecchymosis on the upper eyelid and a patch of conjunctival hemorrhage located approximately 10 mm from the superior limbus (Figure 1(a)). The anterior chamber was deep, and there was no obvious inflammatory reaction. B-mode ultrasonography confirmed dense vitreous opacities but revealed no evidence of retinal detachment (Figure 1(b)). A limited view suggested a yellowish lesion and retinal hemorrhages superior to the optic disk (Figure 1(c)). Spectral-domain optical coherence tomography (SD-OCT) was performed on the area of interest, guided by fundus photography. It revealed three distinct, closely spaced retinal breaks superior to the optic disk, measuring 543 µm, 298 µm and 546 µm, respectively, in maximum linear dimension (Figure 1(c1)–(c3)). The largest break (543 µm) demonstrated a full-thickness disruption involving the neuroretina, retinal pigment epithelium (RPE) and the choroid, consistent with a penetrating injury (Figure 1(c1)). Given the absence of retinal detachment, a conservative approach was adopted. Serial OCT examinations were scheduled to monitor the evolution of the retinal breaks. Remarkably, all three breaks demonstrated a trend toward spontaneous closure. The full-thickness break showed initial signs of healing at the level of the large choroidal vessels at day 4 (Figure 2(a1)), followed by gradual restoration of RPE continuity by week 1 (Figure 2(a2)). At a 2-month follow-up, the continuity of the neurosensory retina has also been re-established (Figure 2(a4)). The two smaller retinal breaks progressively decreased in size over the course of 10 days (Figure 2(b3) and (c3)) and were completely closed by 2 months (Figure 2 (b4) and (c4)).
Initial clinical presentation of the right eye. (a) Anterior segment photograph showing subcutaneous ecchymosis on the upper lid and a patch of conjunctival hemorrhage (arrow) located 10 mm from the superior limbus. (b) B-mode ultrasonography image revealing numerous point-like echoes in the vitreous cavity consistent with hemorrhage. No retinal detachment band is observed. (c) Color fundus photograph demonstrating dense vitreous hemorrhage obscuring the posterior pole. A suspected yellowish lesion and retinal hemorrhages are noted superior to the optic disk. Optical coherence tomography (OCT) scans corresponding to the suspicious area superior to the optic disk. Three distinct retinal breaks are identified, measuring 543 µm (full-thickness perforation with retinal pigment epithelium (RPE)/choroid disruption) (c1), 298 µM (c2) and 546 µM (c3), respectively.
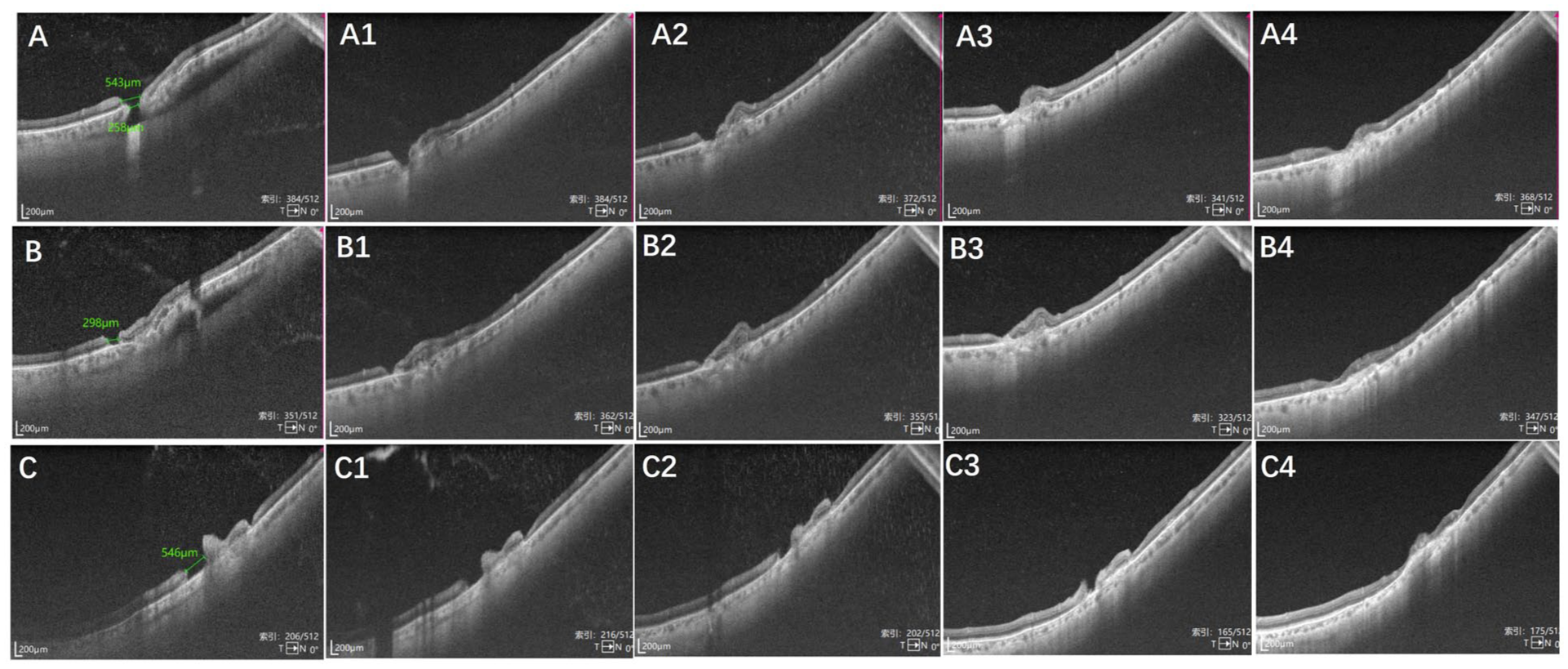
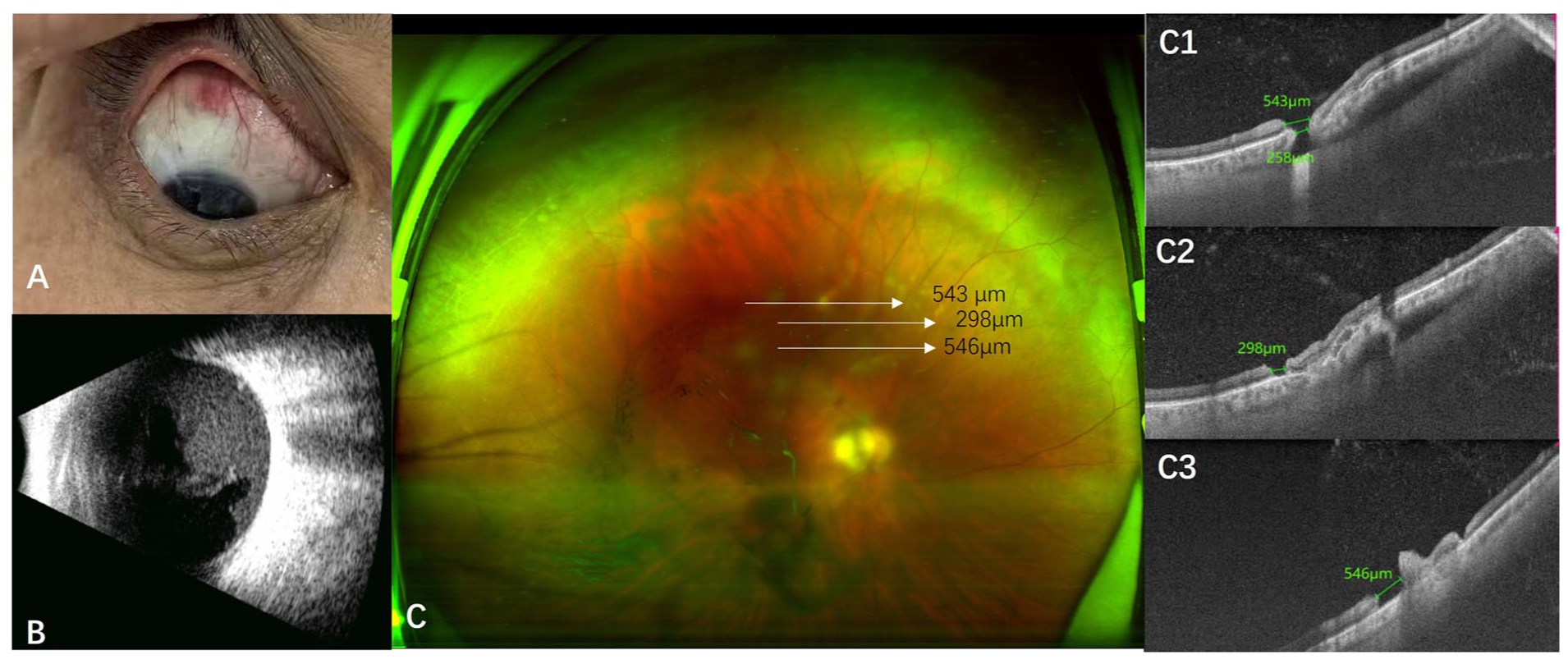
Serial optical coherence tomography (OCT) follow-up of the 543-µm full-thickness retinal break (a), 298-µm retinal break (b) and 546-µm retinal break (c) at 4 days (a1–c1), 7 days (a2–c2), 10 days (a3–c3) and 2 months (a4–c4). With respect to the full-thickness break, at 4 days, initial healing is observed at the level of the large outer choroidal vessels (arrow) (a1). At 1 week, continuity of the retinal pigment epithelium (RPE) layer was partially restored (a2). At 2 months, the continuity of the neurosensory retina was re-established (a4). With respect to the 298-µm and 546-µm retinal breaks, there was a progressive reduction in size at 4 days (b1/c1), 7 days (b2/c2) and 10 days (b3/c3) after the injury, with complete closure of the neurosensory retinal layer by 2 months (b4/c4).
As the vitreous hemorrhage gradually absorbed over several weeks, allowing a better fundus view, local laser photocoagulation was applied around the sites of the healed retinal breaks to prevent future retinal detachment. At the final follow-up visit 2 months after the injury, the BCVA in the right eye had fully recovered to 1.0.
Comment
This case illustrates a serious potential complication of periocular acupuncture—iatrogenic retinal-choroidal perforation and multiple retinal breaks leading to vitreous hemorrhage. The elongated axial length in high myopia is associated with scleral thinning, posterior staphyloma and vitreous syneresis. These structural weaknesses make the globe more susceptible to penetration and the retina more vulnerable to tearing from minor trauma or mechanical disturbance, such as that potentially induced by an acupuncture needle.
Comprehensive documentation with serial OCT can provide unique insights into the natural history of such injuries. Notably, even a full-thickness perforation demonstrates capacity for self-repair, healing in an “outside-in” manner from the choroid toward the neurosensory retina. This observation suggests that, in the absence of persistent traction or subretinal fluid, some traumatic retinal breaks may close spontaneously, possibly mediated by RPE proliferation and glial cell migration. However, the presence of multiple breaks and vitreous hemorrhage signifies a high-risk eye for subsequent rhegmatogenous retinal detachment. Therefore, despite the observed healing, prophylactic laser retinopexy was arguably a prudent intervention to create chorioretinal adhesions and reduce long-term detachment risk in this case.
This report highlights several important clinical implications. First, practitioners performing periocular acupuncture must be aware of this potential vision-threatening complication, especially in patients with high myopia or other ocular comorbidities. Second, OCT is an indispensable tool for detecting subtle retinal breaks not visible on clinical examination and for monitoring their progression. Finally, management should be individualized. While immediate vitreoretinal surgery may be required for cases with retinal detachment, this case demonstrates that a period of observation with close OCT monitoring can be a valid initial strategy for injuries without detachment, as spontaneous resolution may occur.
Footnotes
Acknowledgements
All authors would like to thank the patient.
Author’s note
Min Xu is now working at Southern University of Science and Technology Hospital (Nanshan, Shenzhen), Shenzhen 518000, China.
Ethical considerations
Informed consent was obtained from the patient to publish this case report.
Patient consent
Consent for publication was obtained from the patient.
Author contributions
All authors attest that they meet the current ICMJE criteria for authorship.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The authors are willing to share the data generated by this case.