
Abstract

Background
Intractable hiccups (IHs) are commonly treated in acupuncture clinics. Persistent hiccups and nausea can serve as the initial, and even isolated, manifestation of area postrema syndrome (APS), which is a core clinical feature of neuromyelitis optica spectrum disorder (NMOSD). APS is observed in up to 30% of patients ultimately diagnosed with NMOSD and constitutes the first presenting symptom in approximately 12% of cases. 1 Early recognition is critical as APS responds to immunotherapy.
Case report
A 36-year-old woman presented for acupuncture on 9 January 2020, with a 1-week history of nausea, vomiting and IH (>10/h). Her symptoms began after body aches and a failed 3-day trial of a proton-pump inhibitor (PPI) for prior non-atrophic gastritis. Initial acupuncture (on 9–10 January 2020) yielded no improvement. Upon return on 13 January 2020, hiccups persisted and new neurological symptoms emerged in the form of dizziness, slurred speech and limb weakness. Physical examination revealed horizontal nystagmus upon right gaze. Neurological assessment indicated right-sided dorsal medullary involvement, characterized by uvular deviation to the left (contralateral to the lesion) and tongue deviation to the right (ipsilateral to the lesion). Limb strength was normal.
Diagnostic workup
Urgent cranial magnetic resonance imaging (MRI) on 13 January 2020 showed a patchy dorsal medullary lesion consistent with area postrema involvement (Figure 1(a)). 1 Serum was positive for anti-aquaporin-4 (AQP4) immunoglobulin (Ig)G antibody. 2 A follow-up brain MRI (on 16 January 2020) showed slight lesion enlargement (Figure 1(b)). Full-spine MRI revealed C4–C5 disc herniation but no longitudinal extensive transverse myelitis. 3
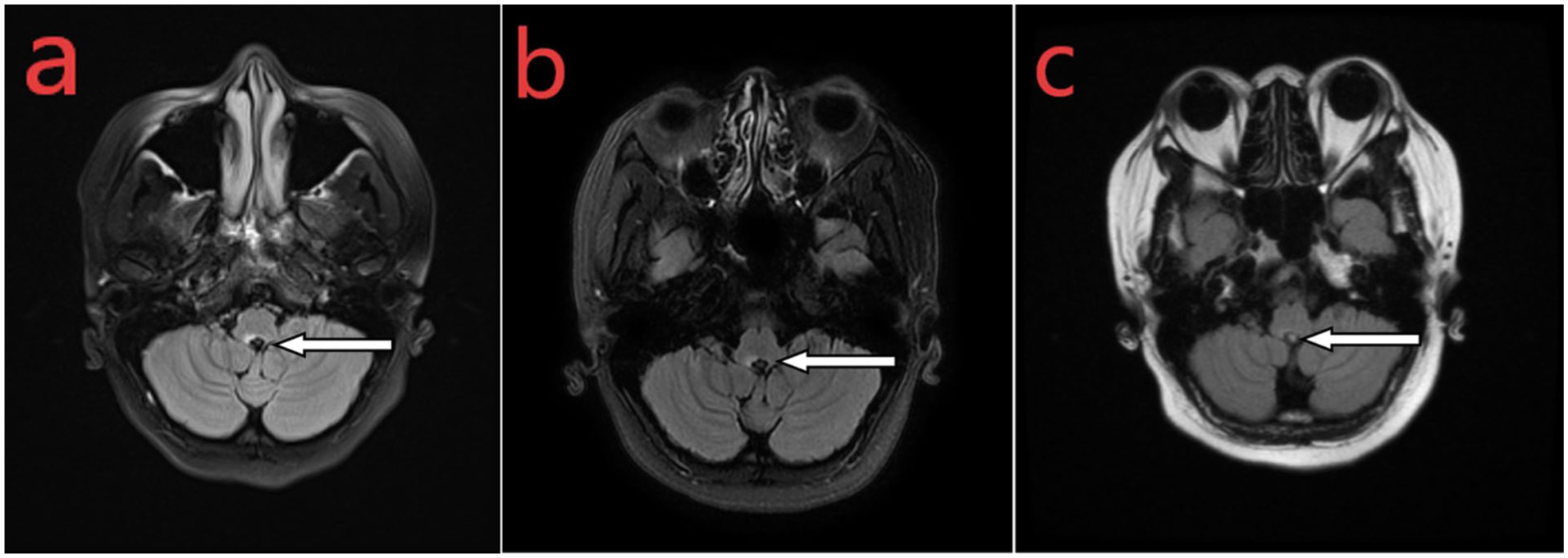
Brain magnetic resonance imaging (MRI) demonstrating the evolution of the medullary lesion. (a) Pre-treatment baseline (13 January 2020): axial T2-weighted image showing a patchy high-signal lesion (arrow) in the dorsal medulla. (b) Follow-up during treatment (16 January 2020): slight lesion enlargement (arrow). (c) Follow-up 2 months post-treatment (23 March 2020): significant lesion reduction (arrow).
Treatment and outcome
NMOSD was diagnosed based on the clinical presentation, MRI findings and AQP4-IgG seropositivity. The patient received a 2-week course of intravenous (IV) methylprednisolone (1 g/day for 5 days) with oral taper, combined with IV immunoglobulin (0.4 g/kg for 5 days), plus supportive care. Her symptoms improved. A follow-up brain MRI (on 23 March 2020) showed significant lesion reduction (Figure 1(c)) and was accompanied by resolution of her hiccups and nausea.
Comment
This case illustrates APS of NMOSD, where a dorsal medullary lesion was believed to have caused IH. Initial attribution to gastrointestinal causes delayed diagnosis by ~10 days. NMOSD frequently presents with “invisible” symptoms like nausea, vomiting and IH due to area postrema involvement, which may precede classic deficits and be misattributed to gastrointestinal disorders.1,4 APS can be the sole initial manifestation. 5
Acupuncture is a valid treatment for symptomatic IH. However, persistent hiccups (>48 h) unexplained by common causes, especially if refractory to a brief PPI trial or initial acupuncture, should raise suspicion for a central nervous system origin. A focused neurological exam at follow-up is essential. Early referral for neurological assessment, brainstem MRI and anti-AQP4 serology is vital to prevent disability.
Conclusion
Acupuncturists must assess for red flags. Unexplained, refractory hiccups warrant consideration of neurological etiologies like NMOSD. Early recognition and referral for definitive testing can significantly improve outcomes.
Footnotes
Acknowledgements
We would like to thank the patient for providing consent for the publication of this case. We are also grateful to colleagues in the Departments of Radiology and Neurosurgery at The 900th Hospital of the Joint Logistics Support Force for their support and assistance in our clinical diagnosis and treatment.
Ethical considerations
This case report is based on clinical practice, and the publication of anonymized case details was conducted with the patient’s informed consent.
Informed consent/patient consent
Informed consent for publication was obtained from the patient. Patient details are anonymized.
Author contributions
D-EH contributed to case management, manuscript draft preparation and data curation. JL contributed to acquisition, analysis and interpretation of imaging (MRI) data. J-QD contributed to study conception, manuscript revision/finalization and project supervision. All authors read and approved the final version of the manuscript accepted for publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this case report are not publicly available due to containing information that could compromise patient privacy. Anonymized data relevant to the case are available from the corresponding author upon reasonable request.