
Abstract
Charles Hewitt Moore, a Fellow of the Royal Society of Medicine, practiced at Middlesex and St. Luke’s Hospitals and was administratively active in The Medical and Chirurgical Society. From 1851 to 1868, he demonstrated expertise in general surgery and the lymphatic system; on pelvic deformity and disease; on the vascular system and aneurisms; on the etiology of cancer; and on the neurophysiology of sleep. He subscribed to two principles of medical investigation: anomalies can reveal new information; and the propagation of untested theory inhibited medical learning and practice. Translator of the German edition of Rokitansky’s Handbook (vol. 3, 1851), Moore wrote twelve papers, three chapters for Holmes’ System of Surgery (1860-1862), and two treatises. Renowned in vascular and cancer surgery, he combined ablation with ZnCl2 against cutaneous and breast cancer. Theorizing that ganglionic nerve tissue was involved in the sleep cycle, he anticipated modern investigations into the sleep-related activity of basal ganglia, the only nerve tissue of that kind in the brain.
Charles Hewitt Moore’s biography exists in the public domain as a composite of fragmentary information on his personal and professional life, the latter being the more substantive of the two (Figure 1). In Part I below, what is known of his personal life, early training, and affiliations, is gathered from obituary notices, biographical sketches, and periodicals. His pioneering contributions to medicine have only been sporadically treated. Part II of this biography will, therefore, present his writings on pelvic anatomy: fractures and distortions; on the management of aortic aneurisms; on the treatment of cancer with chemical coagulation and excision; and on the neurophysiology of sleep. A distinguished surgeon, anatomist, and medical writer, Charles Hewitt Moore developed innovative treatments for refractory diseases.

Charles Hewitt Moore.
Training and affiliations, 1837–1869
Charles’ uncle, Dr. Joseph Moore, of Savile Road, led him to a career in medicine.1–4 Charles began his education at Plymouth New Grammar School, and he entered St. Bartholomew’s Hospital in 1837 when he was 16, as house pupil to Frederic Carpenter Skey (1798–1872), Assistant Surgeon at that institution. 5 Once qualified, he assisted Skey with his anatomy courses at the Aldersgate School of Medicine. On 1 August 1842, at the age of 21, he gained membership to the Royal College of Surgeons. At Aldersgate, after a Clinical Clerkship under Sir George Burrows (1801–1887), he was appointed, in October 1844, House surgeon to John Painter Vincent (1776–1852).6,7 Moore had a penchant for clinical work, his mentors citing, among his many qualities, precision and accurate observation. Burrows affirmed that Moore was one of his best Clinical Clerks.
Once Moore had completed his Clinical Clerkship, he embarked on several post-graduate years in Berlin and Vienna, where he studied under the anatomist, Carl Rokitansky (1804–1878). 8 In this period, Moore would also distinguish himself as a linguist, in 1851 producing a fluent English translation of volume 3 of Rokitansky’s Handbook of Pathological Anatomy. 9 Returning to England in 1846, he was appointed Demonstrator of Anatomy; and, in 1848, Lecturer on Anatomy at Middlesex Hospital, where he served for twenty years as general surgeon and cancer specialist. His numerous writings contain detailed descriptions and 33 case studies. Having been a member of the Royal Society of Surgeons from 1842, he would eventually qualify by examination, on 10 August 1848, as a Fellow of the Royal College of Surgeons.
While a practitioner at Middlesex and at St. Luke’s Hospitals, Moore was administratively active at the Royal Medical and Chirurgical Society of London (RMCS) and a frequent contributor to its Transactions. 10 He was elected Fellow of the RMCS (1857), Librarian (1858), Secretary (1859-62), Council Member (1864-65), Treasurer (1868-69), Member of the Scientific Committee (1866-1869), and Vice President (1866-67); for a period, he served as Curator of Middlesex Hospital Museum (MHM). After resigning this post, in 1869 he accepted a position as Joint-Lecturer in Systematic Surgery at University College Hospital, London. Three months into that appointment, in April 1869, he suffered a stroke and, six weeks later, passed away at the age of 48.
Only a brief mention of his family life can be found in the biographical literature, one source stating that at a young age he was a widower, caring for two children. 1 One can reasonably infer that this tragedy and his single parenthood did not inhibit his professional life, which spanned two productive decades as a member of the RMCS and as practitioner at the abovementioned Hospitals. Distinguishing himself as a surgeon, Moore endeared himself to colleagues, one of whom described him as amiable, reflective in speech, and always conscientious. He lived his faith, as well, in his activities with the Christian Medical Association. 2
Theory and innovation
Moore’s writings, from 1851 to 1868, demonstrate expertise in the sub-disciplines of general surgery and
The pelvis: Fracture and distortion, 1851 and 1857
Moore learned about pelvic anatomy and disorders through the writings of Sir Astley Cooper (1768-1841), of Guy’s Hospital, through the instruction and writings of F. C. Skey and J. P. Vincent, of St. Bartholomew’s, and through his studies with C. Rokitansky, of Vienna. From Cooper, Rokitansky, and others, he observed how pelvic injuries were classified. Because fractures presented with “a great variety of symptoms,” Cooper grouped them according to “the degree of injury inflicted on the viscera”; a typical case defined each group. 30 On the other hand, Skey and Vincent subscribed to rudimentary guidelines. Skey identified only the most common type of injury: the vertical break “through the acetabulum, or more posteriorly through the ilium,” usually resulting from a fall from great height. 31 Vincent understood the pelvic fracture as a “very common” injury, involving the breaking of prominent bones, such as the crest of the ilium. 32 Although Rokitansky observed J. F. Osiander ‘s (1787-1855) divisions of pelvic abnormality, the former was open to the possibility of an unclassifiable deformity bringing new knowledge to light and of reforming established criteria. 9
Rokitansky’s method– based on authoritative knowledge but open to discovery– informs Moore’s 1851 classic, “Account of a Case of Fracture and Distortion of the Pelvis.” A fractured pelvis on display at the MHM belonged to the stone-sawyer, J. T. Horsfield. Moore observed that the multiple injuries it presented, the result of being crushed by fallen timber, resisted categorization: “Examples are exceedingly rare … in which more than one cause of deformity exists in the same pelvis; and there is … no instance in which so many of the principles of deformity are illustrated as in the accompanying specimen”(Figure 2). 13 The postmortem, which Moore had performed several years after the accident, revealed that the decedent had suffered from pre-existing conditions: cardiovascular and kidney disease, along with a bone-softening disorder. 33 Factors such as these made a complete evaluation challenging. Before radiographic technology was available, a physician treating a pelvic-ring injury relied on what Moore called “salient characters”—what was seen, felt, or heard (e. g., the sound of bone crepitation). 13 Unlike the Osiander-Rokitansky divisions, the British system did not accommodate anomalies and had only three deformational classes: congenital malformation, pathological deformity, and traumatic injury. Horsfield’s pelvis appeared to correlate with both the second and third categories.
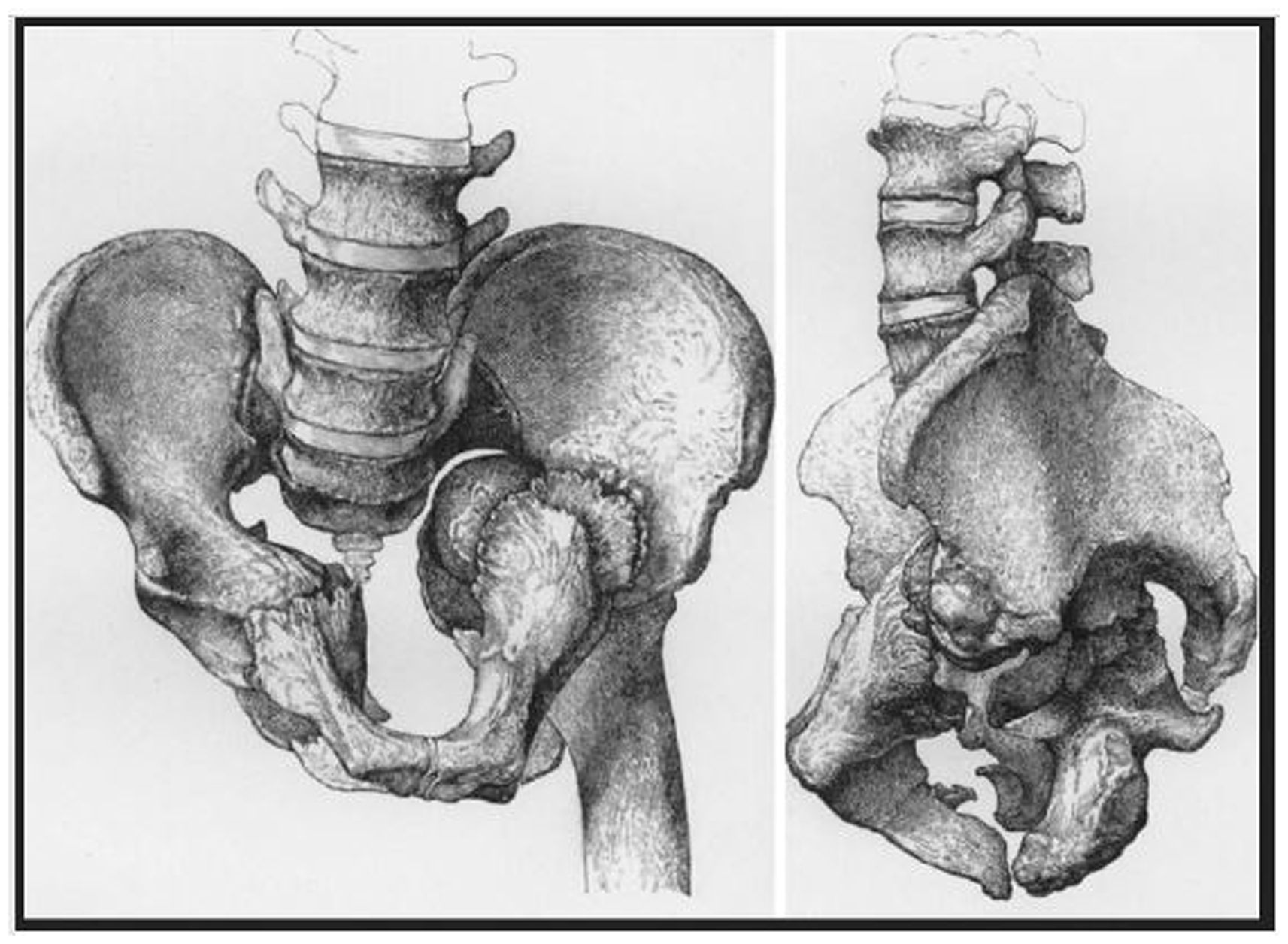
Left side: Front view of pelvis and left femur (Sketch by W. Bagg).
Contrary to expectation, the patient had survived the crushing injury, living for several years with reduced range of motion. The postmortem, however, had found the misshapen pelvis unhealed; and the injury, far worse than originally thought. The head of the left femur had been violently driven up into the pelvis, the limb shortened by two inches, and the hip-joint eroded. Moore’s report describes every contorted feature and verbally reconstructs each shattered bone. From the standpoint of surgery and obstetrics, he noted several points of interest. A surgeon, for example, would doubtless have been interested in the relation of the lower extremities to the injured pelvis and astounded by the fact that the victim recovered from “as severe an injury as any on record.” Moore thought the triangular compression of Horsfield’s pelvis similar to a deformity, of natural origin, which complicated childbirth. The analogue belongs to the sixth subclass of the Osiander-Rokitansky divisions: in a triangular pelvis, the sides become convex, encroach upon the pelvic cavity, and unite at acute angles. 9 While Moore suspected rickets or osteoporosis in the unhealthy condition of Horsfield’s bones, the evidence was inconclusive. Moore’s primary intention was to foreground the anomaly and to determine if it either corrected or augmented conventional knowledge.
In an 1857 paper, “The Mechanism of the Joints of the Sacrum,” Moore argued that a medical theory should be tested exhaustively before being propagated in instructional contexts. 14 Competing approaches to pelvic morphology raised the concern that untested theory might adversely affect medical education. A popular anatomy text, Luther Holden’s (1815-1905) Human Osteology (1855), illustrates Moore’s concern. 34 A Demonstrator of Anatomy at St. Bartholomew’s Hospital, Holden purported to explain how pelvic bones, the spine, and the lower extremities interrelated to each other. His geometrical representation of the pelvic mechanism, however, focused narrowly on the physical characteristics of bones and joints—on aspects such as the arch, axes, the brim, diameters, and angles of obliquity. In excluding the ligaments, so vital to motion and support, he wrongly implied that pelvic function was inherently confined to bones and joints. 34 A representation of pelvic function ignoring the ligaments, Moore pointed out, was fundamentally incomplete and misleading. Bands of connective tissue, the ligaments bind the articular extremities of bones to the pelvis, help support the pelvic ring and upper body, and regulate motion. 35
Another example of Holden’s limited perspective on pelvic anatomy was his description of the sacrum, the joint connecting the lateral halves of the pelvis. Instead of describing it plainly as the lower part of the vertebral column, Holden referred to it as “the broad keystone arch” supporting the weight of the spine; in lieu of connective tissue, he further introduced as explanatory concepts the fulcrum and the lever.
34
Holden’s description was in accord with the principles of Medical Physics. Promulgated by French anatomists of the period, Medical Physics interpreted the pelvic mechanism in terms of bones, energy, motion, and force.
36
Jules Gavarett (1809-1890), a proponent of the theory, likened the sacrum to a multi-purpose “wedge.” In 1858, Gray would also compare the sacrum to a wedge; however, he described the ligaments comprehensively.
35
The Medical Physicists were correct to say that the sacrum connected the lateral halves of the pelvis (i.e., the fused ilium, ischium and pubis), providing balance, support and stability.
37
But their explanation was incomplete without the connective tissues. In reference to Gavarett and associates, Moore asserted that one cannot fully understand the pelvic mechanism without recognizing the interdependency of bones and ligaments: “it is impossible that the anatomy of this part of the body can be completely understood, so long as the precise form and direction of the articulating surfaces, and the use of the ilio-lumbar ligaments, are disregarded or mistaken.”
14
The ligaments were even more important to the pelvic mechanism than were its composite of bones: “The security of the articulations … depends not on the bones, but on the ligaments,” regulators of weight distribution and restrainers of movement.
14
The ilio-lumbar and sacro-sciatic ligaments, for example, tightened in order to support both the spinal curvature and the weight of the torso, as well as to maintain the sacrum as “a firm basis upon which the vertebral bodies may be piled.”
14
Gray and Carter explicitly demonstrate, in word and image, that four classes of ligaments, 12 in all,
As exemplified by his articles on the pelvis, Moore recognized in the MHM exhibit an opportunity for in-depth medical investigation. With respect to the standards of medical literature, in 1857 he contended that instruction in pathological anatomy depended on information that was both accurate and complete.
Aortic aneurism: The wire method, 1858–1866
From 1858 to 1866, Moore wrote extensively on vascular medicine, publishing four papers and two chapters in a compilation.15–20 He is best known for the penultimate paper of this series, “On a New Method of Procuring the Consolidation of Fibrin in Certain Incurable Aneurisms.”
19
Moore’s method was to place coiled wire in a distended artery in order to initiate blood clotting. The wire and clot, which formed
In the 1864 paper, Moore expressed his indebtedness to forerunners. From 1822 to April 1830, the French anatomist and surgeon, Alfred Velpeau (1795-1867), had introduced needles into the blood vessels of dogs to treat aortic aneurisms. 41 Although these experiments were inconclusive, he showed that an extractable needle could initiate blood clots. The British physician, Benjamin Phillips (1805?-1861), conceding that Velpeau had been successful in this regard, downgraded the latter’s experiments as discontinuous, inconclusive, and the cause of “excessive inflammation.” On the basis of five equine experiments (March to May 1830), conducted prior to Velpeau’s, Phillips claimed precedence and to have achieved superior results. His method, however, was never tested on human beings. 42
Moore cited other texts that had contributed to his knowledge on the subject. In chapters for A System of Surgery (1860-62), he described his research on the occlusive danger of foreign objects in the circulatory system.16,17 Sir Stephen L. Hammick (1777-1867), Surgeon General of the Royal Navy Hospital at Plymouth, had presented an undated pathology specimen, Aorta No. 1566 A, to the Museum of the Royal College of Surgeons of England.16,43 A fibrin-encrusted bullet, dislodged from the aorta of a British sailor who had died of a gunshot to the thigh, had apparently circulated up to the ascending aorta where it was found adhering to the wall of the occluded artery. This exhibit exemplified the inherent danger of aneurismal procedures. 16 Moore cited two French accounts that reiterated the danger. M. Legroux, in 1837, attributed cardiac occlusion “to the passage of fibrinous plugs,” originating from a foreign object that had been surgically introduced into the vascular system. 44 In an 1849 paper, M. Laugier described the remarkable case of a man who had died of gangrene, attributed to a fibrin-covered needle found in a ventricle. The lower end of the aorta and the iliac arteries on both sides were filled with an adherent clot that had broken free from a distant operation site.17,45 Hammick’s aorta and the French accounts reinforced Moore’s awareness of the surgical risks.
In November 1863, a patient with an aortic aneurism consulted the surgeon, Charles Murchison (1830-1879). 19 When the condition worsened, the patient agreed to undergo the procedure. Technically, the operation was successful; however, despite short-term improvement, on 12 January 1864, as noted above, the patient succumbed. Reminiscent of J. T. Horsfield’s demise, that of the aortic patient was attributed to pre-existing atheroma of the aorta and to both kidney and liver disease.
Since Moore’s method was on trial, it was inevitably blamed for the death. He defended its legitimacy by virtue of six points: (1) the procedure, rather than hastening death, had forestalled it; (2) the wire coils were deposited in the aneurism without complications; (3) the wire neither punctured the chest wall nor had fragments detached from the main clot (as per Aorta No. 1566 A, Legroux, and Laugier); (4) the minute puncture of the aneurism had healed and bled slightly; (5) within one post-operative hour, good results were reported: the aneurism ceased to beat; its size diminished; the pulse subsided; a large mass of fibrin, as predicted, adhered to the coils; and the heart rate was normal (standard medicines being ineffective); (6) as intended, the reinforcing adhesion was firm and inseparable from the wall of the aneurism. Moore concluded that the wire was not dangerous. On the contrary, if performed cautiously, the procedure tended toward cure. The operation itself, he claimed, had not been the cause of death; rather, as it had been for J. T. Horsfield, co-morbidities were to blame. Without manifest fault, Moore argued that the method should not be abandoned, especially since post-operative results evidenced its short-term value. 19
Moore’s method which had introduced wire permanently into an aneurism would be modified but not abandoned. From 1872 to 1886, surgeons in Britain, Italy, and the United States would treat fourteen aneurisms, located in various arteries, with wire, needles, silk, horse hair, and even watch-springs. 40 Despite limited success, the method continued to be applied from 1907 to 1921, operators employing a range of wire alloys, gauges, and apparatuses. 39 On a parallel track, surgeons, as early as 1824, had tested electric current to induce blood coagulation. 40 Alfonso Corradi (1833-1888), of Pavia, in 1870, initiated clotting in an aortic aneurism by combining Moore’s procedure with electricity. 46 What came to be known as the Moore-Corradi technique, by 1938 had shown inconsistent results–that is, until Arthur Blakemore (1897-1970) and Barry G. King, of New York, perfected the technique.40,47 In 1953, Blakemore described an improved method, using ligation, inserted wire, and 100 volts of direct current, to treat an aortic aneurism. 48 Moore’s innovation in vascular surgery inspired a century of technical development in the management of aortic aneurism.
Cancer: The knife-ZnCl2 method, 1862–1867
Moore attended at the cancer wards of Middlesex Hospital, alongside Campbell De Morgan (1811-1876), Alexander Shaw (1804-1890), John Pattison (d. 1876), and others. He published six papers, a chapter in a compilation, and one treatise on the subject.21–28 His chapter on cancer, in Holmes’, System of Surgery (1860), surveyed what was known about the disease and current treatment options. 22 Using the nomenclature of the day, Moore enumerated five types of cancer (Scirrhous, Medullary, Melanotic, Epithelial, and Osteoid); its general etiology, including comments on metastasis; its biological characteristics and the influence of heredity; and five modes of treatment (surgery, diet, escharotics, compression, and ligation). Moore included numerous case studies in his essays and in his treatise, Rodent Cancer. He described treatment for four kinds of cancer: urological (1852) 21 ; oral (1862) 23 ; breast (1867) 22 ,25,27; and skin (1862, 1866, and 1867).22,26,28 Their most well-known treatment modality, used for skin and breast cancers, was surgical excision and zinc chloride (ZnCl2). Sir D’Arcy Power (1855-1941) rightly stated that Moore was “a pioneer of the modern operation to prevent recurrence after operation for cancer of the breast and so to cure the disease.” 49
In 1865, Moore used ZnCl2 routinely against breast cancer, as a solid, paste, lotion, and injectable.26,50 In April and May 1867, he called for its aggressive use; hence, where surgery was not possible, solid ZnCl2 was applied to the edges of the skin as a paste on open wounds or as a wash on visibly healthy surfaces 27 ; however, he cautioned that strong concentrations of the agent were risky. For breast cancer, he was wary of using concentrated strengths in the range of 20 to 40 grains per fluid ounce of water; the cancer had to be destroyed but not at the expense of healthy tissue. 27 The effectiveness of this regimen, in the long-term, was indeterminable since patients had to be closely monitored and their histories followed for years.
Moore confirmed that combining ablation and ZnCl2 was warranted in advanced cases of rodent cancer, which he demonstrated in his treatise (Figure 3). 28 The adjective “rodent,” derived from the Latin verb rodo (“to gnaw”), figuratively conveyed the erosive effects of advanced basal cell carcinoma. 51 Moore remained circumspect about outcomes. In the case of a patient named Mary H., for example, whom facial skin cancer had disfigured, he was gratified to have prolonged her life, to have saved her vision, and to have provided cosmetic prosthesis. 24
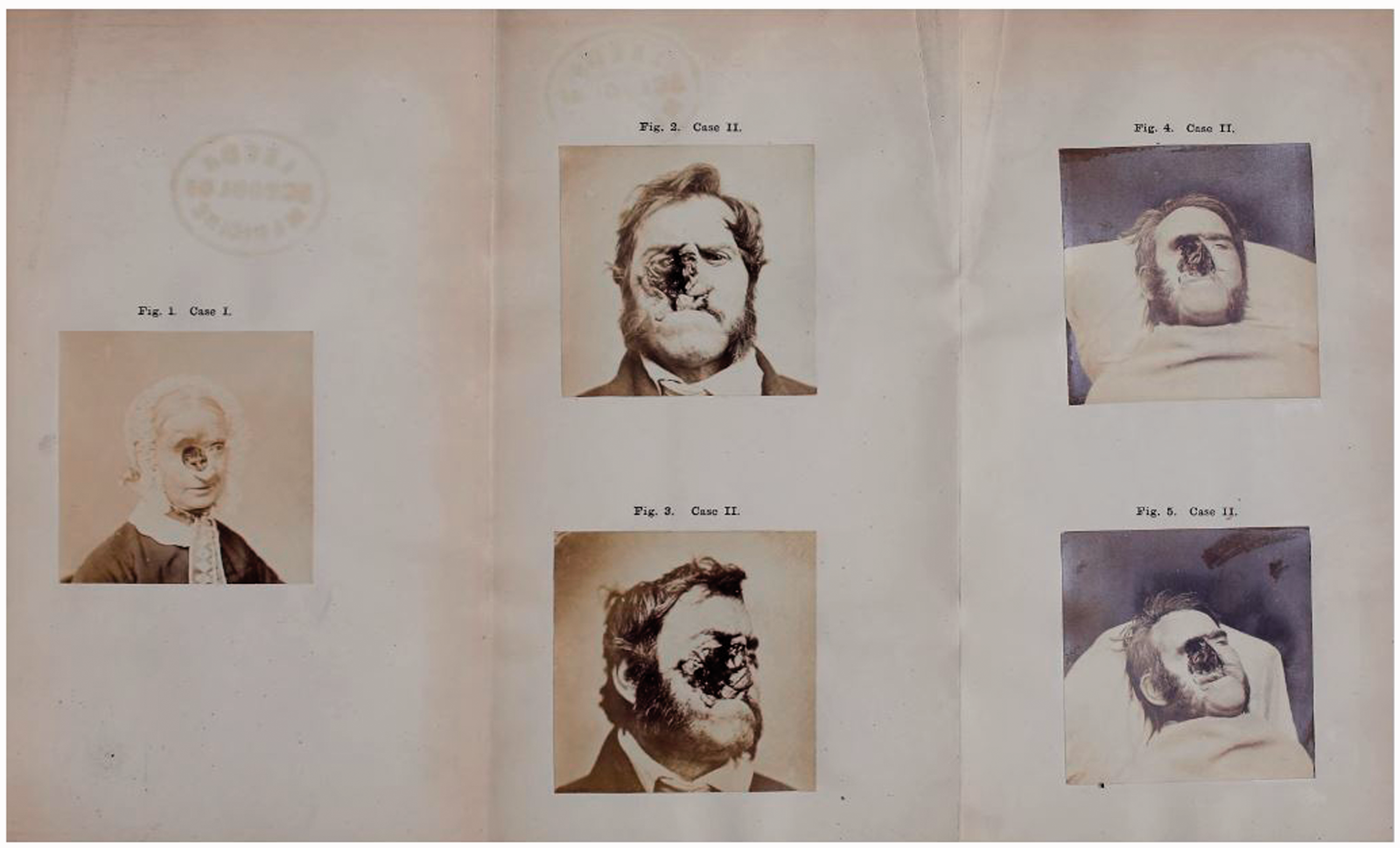
Rodent cancer patients at Middlesex Hospital.
The cancer research of Moore and his colleagues belongs to a tradition of zinc-chloride research in medicine, traceable to the chemist, Sir Humphry Davy (1778-1829) and to his younger brother, John (1790-1868), an Edinburgh-trained physician. 52 Moore and colleagues had demonstrated the potential value of combining ZnCl2 and ablation. In 1932, F E Mohs, MD (1910-2002), preceded by a number of researchers, introduced the fixed-tissue method of cutaneous surgery in which ZnCl2 was used to devitalize basal or squamous cell cancers. In 1953, modifying the procedure by eliminating ZnCl2, Mohs devised a more efficient, fresh-tissue method of excision. The employment of zinc chloride as an anti-cancer modality continues to inspire research today.53,54
Sleep: The neurovascular theory, 1868
Moore was familiar with three mid-nineteenth century theories on the mechanism of sleep: the vascular theory, which held that sleep and arousal were directly related to blood volume and to the arterial pressure of the cerebral arteries; the chemical theory, which proposed that oxygen or carbon-dioxide concentrations regulated sleep; and the neural theory, which posited that sleep and arousal were controlled by the action of nerve-cell bodies. In 1891, the German anatomist, W. G. von Waleyer-Harz (1836-1921), would call these cells neurons.55,56
Contemporary debates conditioned Moore’s thinking. In one area, his theorizing anticipated the modern neurophysiological understanding that sleep and wakefulness were regulated in the brain, and that nerve impulses led to the release of hormones and chemicals.57 In his 1868 treatise, 57 On Going to Sleep, Moore formulated a unique neurovascular theory. He postulated that ganglia, small masses of nerve tissue, relayed impulses to cerebral arteries and were, therefore, essential to the sleep-wake cycle. 29 In 1858, Gray had identified fifty-four such structures. 35 Moore, however, misidentified the cervical ganglia, those found in the neck, as the relay points for the nerve impulses that were responsible for sleep. Twentieth-century neuroscientists, such as Henri Piéron (1881-1964), would discover that sleep is regulated by cerebral rather than cervical activity58; thus, the sleep-wake cycle is a function of the Central (brain and spinal cord), not of the Peripheral, Nervous System.
Moore’s idea that ganglia of some kind were involved in sleep and wakefulness was, in fact, an intuitive advance in the understanding of the neurophysiology of sleep. Neuroscientists are currently investigating whether the basal ganglia, located in the midbrain of both hemispheres, are molecularly involved in the sleep process.60,61 Basal ganglia are the only structures of the kind found in the brain 57
Through the study of pelvic anatomy and function, Moore formulated an investigative method. In 1851 he demonstrated through detailed examination how an anomaly could reveal new medical insights 62 ; and, in 1857, on the pelvic mechanism, how incomplete representations could inhibit medical learning and practice. An innovator in both vascular and cancer surgery, he developed methods, instrumentation, and pharmacological agents, to improve conventional treatments. In 1868, he contributed a neurophysiological explanation, based on contemporary theories, on the alternations of sleep and wakefulness. He proposed that ganglionic nerve tissue was essential to the physiology of sleep. Although Moore wrongly implicated cervical nerve tissue in the process, his insight that ganglia of some kind were involved anticipated modern investigations into the sleep-related activity of basal ganglia, the only tissue of the kind in the brain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.