
Abstract
Coronavirus disease 2019 (COVID-19) and the national lockdowns of 2020/2021 illustrate how modern public health systems are founded on empirical evidence and contemporary understanding of disease transmission. Duncan Forbes was one of the earliest sanitarians in Britain to propose and implement a new understanding of infectious disease control. Starting his early career in Manchester and Cambridge, his eventual tenure as Brighton's longest-serving medical officer of health (MOH) left an indelible mark by challenging the entrenched tradition of terminal disinfection and by devising his “Brighton methods” for the care of tubercular patients. Forbes led Brighton's public health responses during World War I and the 1918/1919 “Spanish” influenza pandemic. Forbes also strove to improve health and housing in Brighton. His views on limiting access to contraception on the grounds of eugenics are also significant. Analysis of Forbes' work then allowed a discussion of both his legacy and of the applicability of his experiences to our own in tackling COVID-19. Forbes undeniably had a great influence in shaping modern public health practice in Britain and his challenges as MOH bear many similarities, as well as stark differences, to today's experience of COVID-19.
Keywords
Introduction
Preventative measures have formed the bedrock of the national response to Coronavirus disease-19 (COVID-19). These include social distancing, mask wearing, hand washing, increased ventilation and lockdowns. Such interventions have been employed on a global scale and as such have no parallel in human history. The drivers of this pandemic are numerous, however one modelling study predicted that at least 50% of new COVID-19 infections originated from exposure to infectious individuals without symptoms. 1 This risk of asymptomatic transmission therefore necessitates the use of the generalised (rather than targeted) preventative measures mentioned above.
One of the earliest documented instances of the employment of preventative strategies to counter pandemic disease occurred during the 1665 outbreak of bubonic plague in the village of Eyam, Derbyshire. 2 The village underwent a self-imposed quarantine and introduced social distancing measures, which helped to prevent the spread of disease to surrounding areas. 2 Such actions were not enforced on a national scale and subsequent pandemics were also met with little mass preventative action. Reasons for why practices in public health have changed so radically to resemble the response we see today are likely multifactorial, but an evolving understanding of disease transmission and the establishment of epidemiological evidence on empirical research were key.
Many individuals helped usher in these changes, amongst them was Duncan Forbes. The career and work of Forbes, who was Brighton's longest ever serving medical officer of health (MOH), exemplifies this change as he sought to safeguard the health of the town during one of its most trying periods, including its last experience of a major pandemic, the ‘Spanish’ flu. This paper attempts to render a biographical account of his life and delineate his contributions to the field of public health with a focus on his actions during the Spanish flu pandemic and how they relate to our experience of COVID-19.
Early life and education
Census records reveal that Duncan Forbes (Figure 1) was born 7 December 1873 in Perth, Scotland, to another Duncan Forbes and Ann R Forbes.3–5 The 1881, 1891 and 1901 censuses show Duncan Forbes to have grown up at 12 Balhousie St, Perth.4,6,7 Forbes was educated at Perth Academy and at 17 also worked as a dyer's clerk.3,6 He went on to train at Edinburgh University and graduated MB, ChB with honours in 1898. 8 In 1901 Forbes was then accepted to the degree of Doctor of Medicine (MD) and was awarded a Diploma in Public Health (DPH) at the University of Cambridge.3,8
Duncan Forbes as Medical Officer of Health (MOH) for Brighton, exact date unknown. 9 Source: The Keep archives.
Manchester (1902–1906) and Cambridge (1906–1908)
In 1902, Forbes became assistant MOH for Manchester. 8 In his role, Forbes supported the then-MOH, Dr James Niven (1851–1925), in his duties and helped compile annual health reports on the city's population. 10 Niven would later be considered a pioneer in infection control through his much-lauded response to Spanish influenza. 10 It is clear from Manchester's annual medical reports for 1902–1905 that Niven increasingly devolved responsibility to Forbes, such that by 1904 Forbes was single-handedly authoring its sections on smallpox, scarlet fever, diphtheria and phthisis (pulmonary tuberculosis).11–14
A distinctive aspect of Forbes' work during this period was its forward-thinking approach and foundation on scientific principles. This is best exemplified in Forbes' 1903 paper discussing the role of asymptomatic carriers of diphtheria bacilli in transmission on scarlet fever wards. 15 He describes how even patients not exhibiting signs of diphtheria could carry bacteria and thus recommended ‘the covering up of ears and the isolation of such patients…to prevent the accumulation of diphtheria bacilli in wards’. 15 At the time, the ability of asymptomatic carriers to transmit infection was not a widely accepted principle and, indeed, in the 1903 report Forbes himself lamented how it was ‘very difficult to persuade laymen, and at times even medical men, that apparently healthy individuals are infectious’. 12
Between 1906–1908 Forbes served as MOH for Cambridge, where he helped facilitate the introduction of the city's first health visiting service.8,16 Forbes' tenure also saw the lowest infant mortality rate of any previous year (88 deaths per 1000 births), in contrast to a national average of 118. 16
Brighton: early years (1908–1914)
In 1908, Forbes took over the post of MOH for the County Borough of Brighton from Sir Arthur Newsholme (1857–1943).17,18 Newsholme would later record that he had a ‘slight influence’ in securing Forbes' appointment and reveals that he was already well-acquainted with his successor's ‘mental and moral’ qualities. 8 Newsholme himself was one of the pre-eminent figures in public health at the time and was leaving Brighton to take up his post as medical officer to the Local Government Board (LGB), the predecessor of the Ministry of Health. 17
A notable example of Forbes' work during this period is seen in a 1910 paper where he discusses his ‘Brighton methods’ for caring for tuberculosis patients whilst limiting the risk of cross-infection from other wards. 19 These are presented in Figure 2 and suggest an understanding of the risks of asymptomatic transmission. 19 Whilst Forbes did not use the term ‘asymptomatic carrier’ in his paper, his focus on the separation of staff working on different disease wards implies that he appreciated the risk of staff contracting infection and then carrying it on to their respective ward, presumably without symptoms. This emphasis Forbes placed on transmission via people would go on to influence his later work.
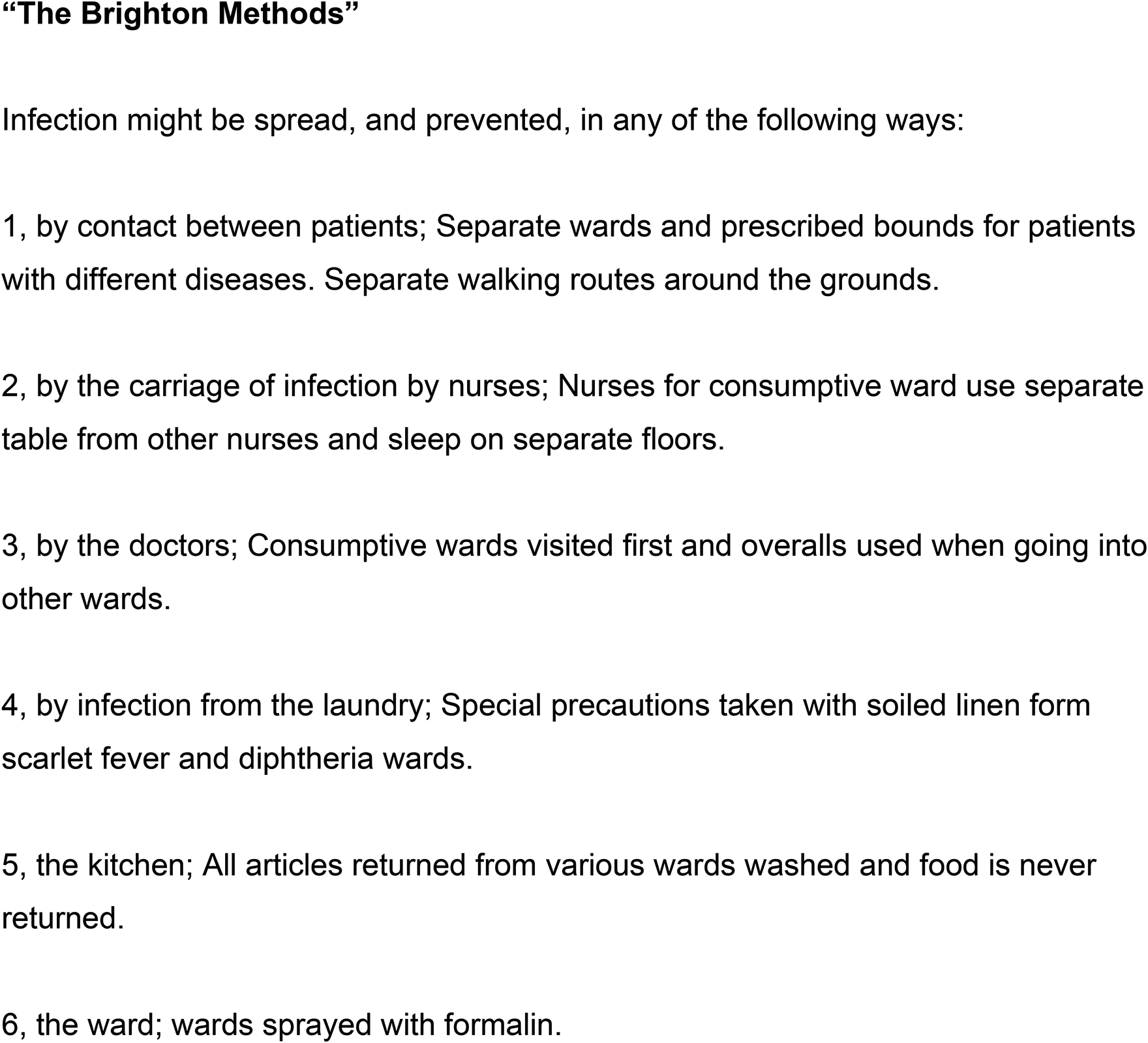
An outline of Forbes' “Brighton methods”, proposed in 1910, for caring for consumptive (tuberculosis) patients in the same facility as other infectious diseases. He lists the different ways infection can be spread and after each semicolon describes the corresponding measures for prevention. 19 Source: Wellcome Collection/Creative Commons By Attribution (CC BY) 4.0.
Brighton: The First World War (1914–1918)
The years 1914–1919 posed two major challenges to public health: the First World War and Spanish flu. The annual health report for 1914 gives the first indication of the difficulties ahead as Forbes remarks that the inspection service was ‘handicapped’ as three out of five of the district inspectors had already been enrolled for military service. 20 Staff shortages would only worsen, with 1915 seeing seven out of 17 of the male members of the health department and six out of seven of the sanitoria staff leaving for active duty. 21 Consequently, Forbes conceded in his 1915 report that ‘only absolutely necessary work’ was undertaken by his department. 21 This is tangible in the progressive shortening of the annual health reports, with the 1913 paper having 179 pages, 1914 having 148, 1915 having 92 and 1918 only 58.20–22
Furthermore, the inspection of military billets fell under the remit of the local MOH office and as the war wore on and more troops came to be stationed in Brighton, ever more inspections had to be conducted by an already undermanned department. In 1914, 597 inspections were completed but this rose to a staggering 2,142 the following year.20,21 The disease burden of such an influx of people into the town was also a critical factor in stretching the local health services, as thousands of military personnel were treated in Brighton between 1914 and 1916. 23 This increasing burden is most starkly evident in the rising number of military deaths occurring in Brighton's hospitals during the war, rising from 15 in 1914 to 124 in 1915 and eventually 162 in 1918.20–22
Between 1914 and 1916, numerous sites in Brighton were converted into hospitals to care for Indian soldiers wounded on the Western Front. 23 These sites included the Royal Pavilion, where the accommodation of thousands of troops brought unique challenges in meeting the diverse religious needs of the Indian army at the time. 23 Numerous provisions were made to accommodate them including a tented Gurudwara and space on the eastern lawn to pray. 23 Dietary provisions were also essential and Forbes mentions in the preface of the 1915 health report that ‘a separate slaughterhouse was built for the Indian troops’. 21 The efforts of Forbes and his department did not pass unnoticed and he was awarded an MBE in 1918 for services rendered during the war. 24
Brighton's epidemic (1918–1919)
Before Brighton and the wider world could recover from the war, a new crisis had emerged. Spanish flu, caused by the H1N1 influenza virus, arrived in Brighton in July 1918 in its herald wave. 25 A recrudescence followed in October and November in the form of its second wave, the most lethal. 25 The pandemic finally ebbed away following a third wave in February and March of 1919. 25 In total, 526 fatalities in Brighton would be directly attributed to the three waves of the pandemic, although the true figure was likely higher due to difficulties in diagnosing influenza at the time (the influenza virus only being discovered in 1933). 25 For context, 603 deaths were attributed to influenza from 1890 to 1899, a period that included the Russian flu pandemic. 25
To contextualise Forbes' actions as MOH during Spanish flu, it is useful to contrast them with those of Niven and Newsholme, men Forbes knew personally from his earlier career. In 1918, Niven was working as MOH for Manchester and Newsholme as medical officer to the LGB, directing the national response from London. 26 Figure 3 illustrates the points at which each first initiated action in respect to their local epidemics and shows the monthly all-cause death rate per 1000 of the population. All-cause death rate was used to capture influenza deaths incorrectly attributed to pneumonia or bronchitis. 27
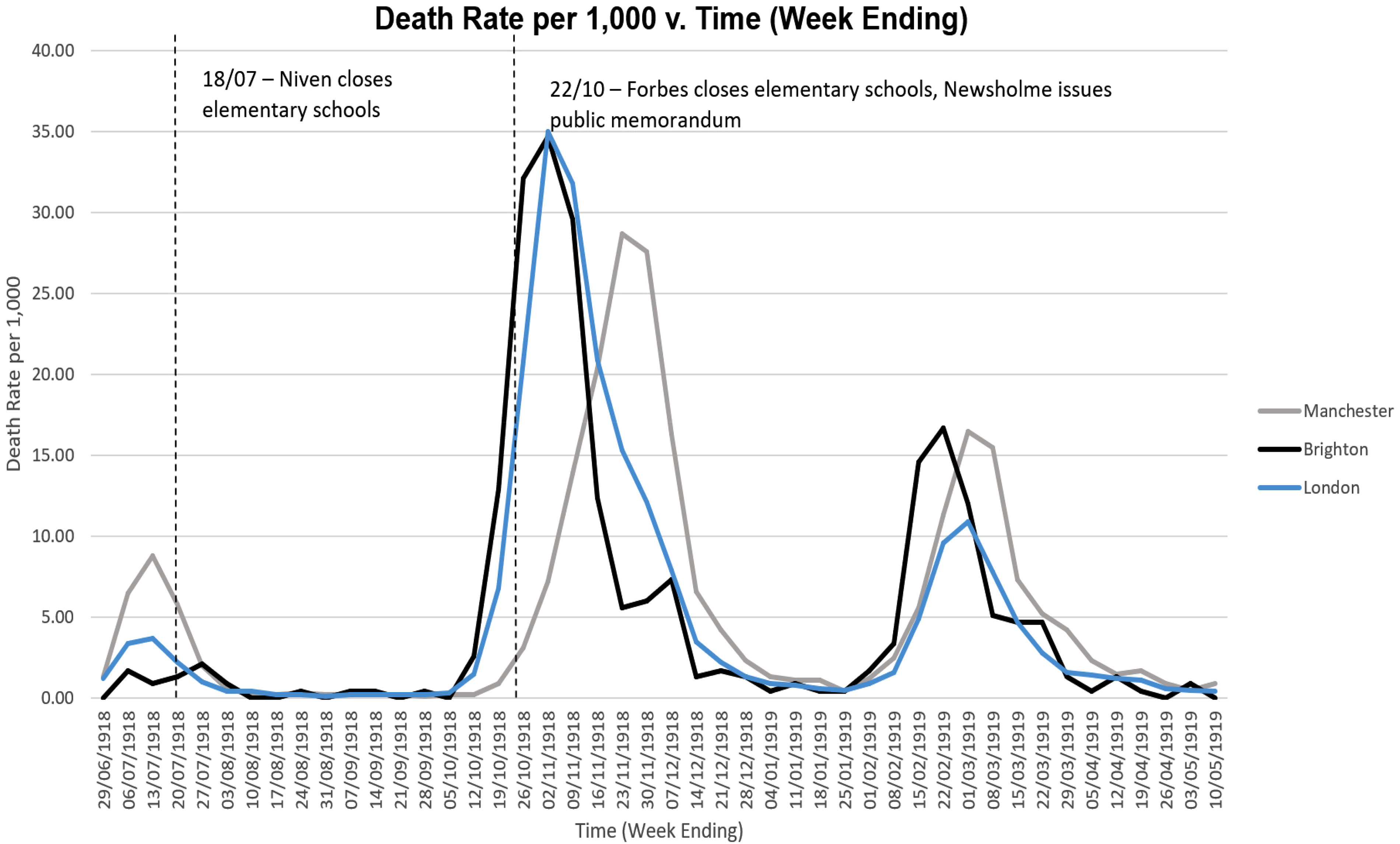
Figure 3 shows that Forbes' first action as MOH was to close elementary schools on 22 October 1918. 22 Other actions taken by Forbes in October included: promoting ventilation of trams, appealing to cinemas to keep their halls ventilated, spraying disinfectant on the floors of public buildings and distributing 5000 advisory pamphlets. 22 These pamphlets were distributed around Brighton and offer wider insight into Forbes' strategy for influenza prevention (Figure 4). In them, Forbes writes that ‘In mild cases constitutional symptoms are absent and the patient seems to suffer from an ordinary cold and is able to be about’. 22 He goes on to say ‘these mild cases are highly infectious and spread the disease’. This final sentence was the only text in the leaflet that was underlined, hinting at the importance Forbes placed on the ability of apparently healthy individuals to spread infection. 22
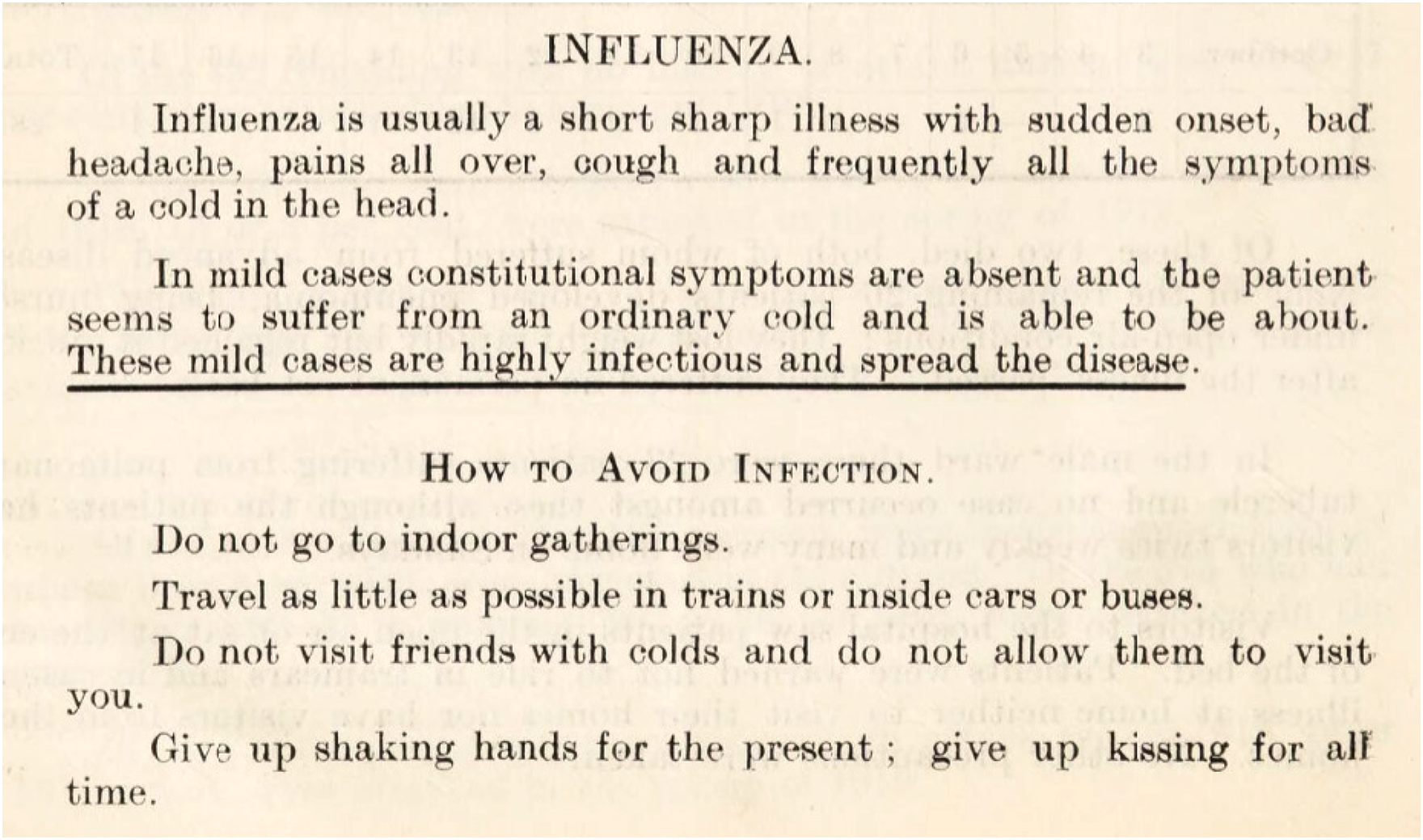
One of the thousands of copies of a leaflet distributed to the public in Brighton by Forbes in 1918. Noticeable is the emphasis placed on transmission by individuals without constitutional symptoms as well as the focus on measures to prevent infection and transmission. 22 Source: Wellcome Collection/CC BY 4.0.
He also advised avoiding the following: indoor gatherings, travel inside trains, cars or buses, interacting with those who exhibit symptoms and shaking hands. 22 He then implores readers to give up kissing ‘for all time’. 22 Forbes warns of the danger in ‘bringing people together in stagnant air as they are brought together in public halls…where the fan is not kept running during the performance’. 22 Accordingly, he goes on to suggest electrical fans as a means of adequately ventilating public venues. 22 This emphasis on ventilation as a means of prevention is consistent throughout the report. 22
A particular focus on limiting the activities of children is also noticeable, with Forbes writing that the power to close schools should also be extended to ‘all children's meetings and gatherings’. 22 He also writes of the need for powers to ‘require theatres and cinemas to refuse admission to children’, whilst presumably still allowing entry to adults. 22 Whilst not explicitly stated in his report, this suggests that Forbes placed particular importance on children as vectors of transmission.
An influenza vaccine was also offered from 15 February 1919. 22 At the time, a vaccine was theorised to be an effective prophylactic as it was believed that influenza was caused by Bacillus influenzae. 28 Forbes described the vaccine as protecting against ‘B. influenzae’, ‘pneumococci’ and ‘streptococci’ species. 22 He writes that the vaccine was mostly offered to teachers, the district nurses and the town hall staff. 22 A total of 70 of these were inoculated along with 56 members of the public. 22 Forbes wrote that of the 126 people vaccinated in total ‘nine developed influenza within five days of inoculation and none thereafter’. 22 Forbes uses this as evidence of an ‘increased susceptibility to infection following immediately after inoculation’ but to a ‘lessened susceptibility thereafter’. 22
Forbes challenges orthodoxy
Following a case of infectious disease, it was common practice in the early 1900s to disinfect the patient's home. 29 Known as ‘terminal disinfection’, this involved the systematic disinfection of clothes, bedding, surfaces and household items. 29 The practice was born from the observation that following a case of infectious disease and removal of the patient to hospital, that disease still occurred in households beyond the period of incubation of the causative organism. 29 It was thus attributed to articles of clothing or items which were missed on initial disinfection. 29 This belief system was bolstered by Koch's discovery that certain microbes could survive for prolonged periods outside the body and still cause infection in animals. 29 Another potentiating factor was the influence of traditional sanitary philosophy in public health at the time. 29 This belief system strongly linked ‘filth’ with disease and so terminal disinfection remained an attractive intervention.
In 1906 Charles Chapin (1856–1941) presented a paper to the American Medical Association on ‘The Fetich of Disinfection’ in which he called for a re-evaluation of the practice based on his findings as medical officer for Providence, Rhode Island. 30 Chapin discontinued terminal disinfection for diphtheria in 1905 and his statistical analysis showed that there had been no appreciable rise in cases as a result. 30 His work was met with scathing criticism as it represented not just an isolated change in practice, but also an emerging movement to base clinical practice upon objective epidemiological science rather than anecdotal evidence. 30
In 1910, Forbes too ceased the orthodox practice of terminal disinfection for cases of scarlet fever and diphtheria in Brighton by no longer disinfecting bedding or mattresses. 29 Forbes arrived at this decision due to the nascent understanding of the impact of asymptomatic carriers on transmission. 29 This development shifted the focus from objects and the external environment as the route of infection and towards asymptomatic people as the vector of communicable disease. These actions made Forbes one of the earliest sanitarians in the UK to abandon the orthodoxy of terminal disinfection. 31 He published his first results in 1920 showing that the change in practice had not led to an increase in cases. 32 He then went further and in 1921 became one of the first in the UK to cease the spraying of patients' rooms with formalin, instead advising that homeowners conduct a ‘spring clean’ after being provided with instructional leaflets. 29 In his 1926 paper, Forbes acknowledged the controversial nature of his change in practice and also writes of the opposition he faced. 33 This, along with the fact that the majority of sanitary authorities were still practising terminal disinfection at this time, shows that Forbes was indeed going against the grain of established practice. 32 In 1939, Forbes was able to publish his results, shown in Table 1. 29 The most profound benefit of the work of Chapin in the US and Forbes in the UK lies in the new age of evidence-based public health practice they helped to usher in.29,30 Their work signified a shift from traditional and seemingly common-sense practice, towards policy based on published evidence and analysis.
Table adapted from one published in Forbes' 1939 paper showing the number of primary cases of scarlet fever and diphtheria which were followed by subsequent cases in the same house, expressed as cases per thousand.
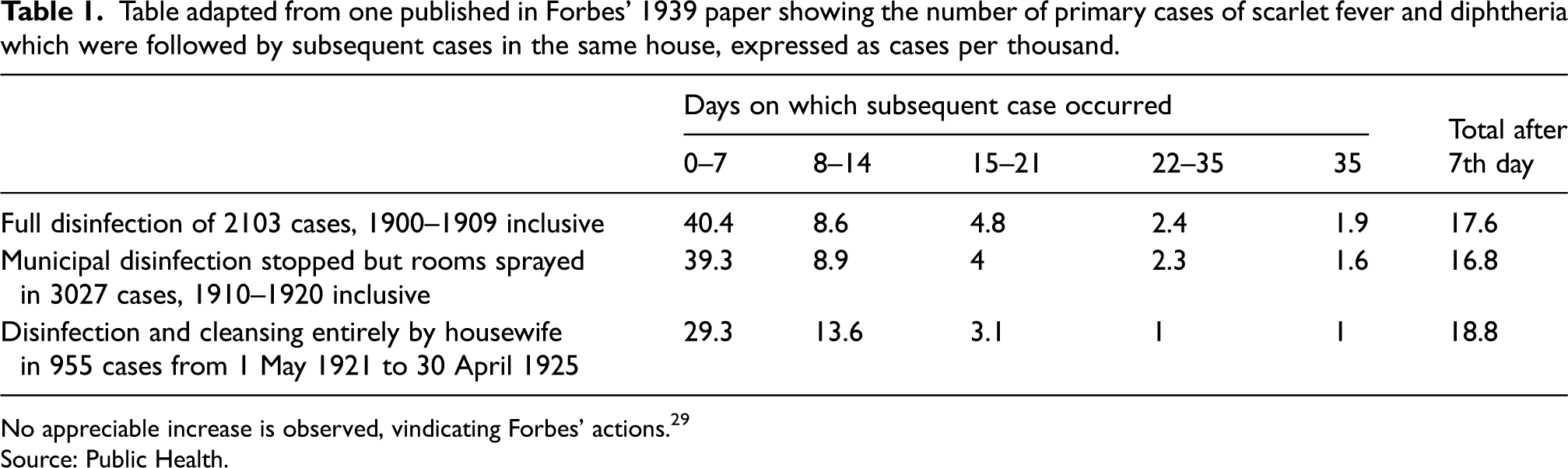
No appreciable increase is observed, vindicating Forbes’ actions. 29
Source: Public Health.
Later work and later years
Forbes demonstrated himself to be in many ways a forward-thinking public health doctor. In other regards, however, he was indeed a physician of his own time. This is best demonstrated by correspondence written by Forbes and published in Public Health in 1924 on the emerging practice of contraception. 34 Referring to the effects of contraception on ‘The British Race’ Forbes stated that it is ‘to be regretted that any steps should be taken likely to accelerate the present steady fall in our birth-rate’. 34 He also wrote of the cumbersome process of contemporary female contraception which involved douching before and after inserting the ‘instrument’, and how this may result in its use exclusively by the ‘intelligent’ classes. 34 He argued that this may risk future generations being ‘bred to an even greater extent from the ignorant and careless which, from the point of view of eugenics, is unsound’. 34 Referring to marriages between individuals with transmissible defects, Forbes writes that ‘the state should prevent such marriages as far as possible, and when such have taken place should sterilise the man’. 34 From this it can be inferred that Forbes was a believer, at least in part, in eugenics.
Forbes does, however, concede that contraception may be useful in women in whom further childbearing could be dangerous and went on to establish Brighton's first contraceptive clinic in 1931.34,35 However, consistent with his own position and that of the prevailing moral attitudes of the time he writes that these clinics were not meant for ‘all and sundry’ and that services would only be rendered to women in whom ‘further pregnancies would be detrimental’.35,36
Forbes' tenure during the 1930s oversaw an extensive programme of slum clearance and further development of the estates of Moulsecoomb and Whitehawk to provide new housing for the people of Brighton. 31 It is apparent that Forbes came into direct conflict with his contemporaries over the design and situation of the new houses, with Forbes expressing a strong preference to house workers centrally in Brighton, closer to the major industrial sites. 31 He also expressed a desire for building larger houses. 31 This appeared to be in opposition to guidance from the Ministry of Health, who Forbes believed had a preference for constructing large numbers of smaller houses at the cost of ‘healthiness and amenity’. 31 Forbes' tenure also oversaw the clearance of 1339 slum dwellings and the building of 4030 new homes, 31 which contributed significantly to the expansion of Brighton.
Fittingly, in his final health report for 1938 Forbes once again took the opportunity to criticise government policy in multiple domains including food supply, vaccination and business regulation. 31 He finally retired in 1939, making his tenure the longest of any MOH for Brighton. 31 However, his propensity to court controversy did not end there. In relation to the Second World War, The Argus newspaper reported on his suggestion that those aged 65 years and over and not engaged in essential work should be sent to Canada or the United States to lessen the strain on domestic food supply.24,35 Forbes would not live to see whether his suggestion was adopted; he died on 25 July 25 1941 following an operation in London. 24
Forbes' legacy
Work during Spanish flu
A 2018 BBC documentary on the Spanish Flu discussed the actions of both Niven in Manchester and Newsholme at the LGB. 26 The documentary constructs a narrative with Niven playing the protagonist and Newsholme the antagonist. This is in part due to the consensus which has arisen that Niven was among the first to act in containing the influenza outbreak whilst Newsholme's failure to intervene was ‘a mistake’. 26 In comparing Forbes' response to theirs, it is possible to contextualise his actions. Figure 3 attempts to objectively capture their actions chronologically and shows that school closures were the first intervention undertaken by both Forbes and Niven.22,27,37 What is also noticeable is the swiftness of Niven's response in closing schools just as the first wave was abating, whereas Forbes only closed schools when the second wave reached exponential growth. This probably resulted in the closures having little effect on the local epidemic in Brighton.
One explanation of Forbes' actions is that the death rate in the first wave for Brighton was lower than for Manchester (Figure 3), and so Forbes would have had less impetus to mandate school closures at such an early stage. On the same day Forbes closed Brighton's schools, Newsholme issued a memorandum on how the public could avoid infection and what to do if symptoms appeared. 38 Newsholme's memorandum does not mention or recommend school closures, suggesting that Forbes may have been acting on his own initiative. 38 The fact that the closures occurred on the same day as the memorandum does, however, suggest that its publication may have influenced Forbes to act.
Generally, the measures employed by Forbes were preventative in aim, standing in stark contrast to those proposed by Newsholme, who wished to keep people in work and using trams so as not to disrupt the war effort. It was for this same reason that Newsholme chose not to publish a memorandum earlier in July 1918 as the ‘relentless needs of warfare justified incurring this risk of spreading infection’. 39 Therefore, Forbes' philosophy as MOH departed significantly from that of his predecessor. Moreover, Forbes takes an almost confrontational tone in his 1918 report on the epidemic where he laments that the necessary powers to enforce closure of schools and premises had not been forthcoming. 22 He goes on to call for the LGB to issue an ‘authoritative statement’ as to the proper use of disinfectants, hinting at a perceived lack of leadership from the board. 22 Here Forbes walks a similar line to Niven, who also bemoaned the voluntary basis under which schools could be closed and who also favoured preventative measures to contain infection. These included minimising social contact by avoiding gatherings, ensuring adequate indoor ventilation and isolating the sick, mirroring what Forbes wrote in his pamphlets. 37
In his role as MOH, Forbes advised against the use of public transport whereas Niven did not. Therefore, it could be argued that Forbes went even further than Niven in this area of prevention.22,37 This again departs from Newsholme who was a noted sceptic of preventative measures, declaring in his address to the Royal Society of Medicine that he knew of ‘no public health measures which can resist the progress of pandemic influenza’. 39 Forbes’ pamphlets also convey an appreciation of the risks posed by asymptomatic transmission. By physically underlining his warning to the people of Brighton that even mild cases were ‘highly infectious and spread disease’, even when ‘constitutional symptoms are absent’, he again reflects the actions of Niven, who made similar warnings in his leaflets.22,37
In summary, whilst it is indisputable that Forbes' actions chronologically resemble those of Newsholme, and so likely made little difference due to their timing, the actions themselves ultimately went further than what was advised by the LGB. Moreover, from the contents of his pamphlets Forbes showed himself, alongside Niven, to be an early practitioner of preventative public health measures who appreciated the danger posed by asymptomatic transmission.
Further contributions to public health
Forbes contributed significantly to the existing body of public health literature. In this regard, among his most seminal work was his early change in practice in relation to the orthodoxy of terminal disinfection. In assessing and changing his methods based on data, Forbes showed himself, alongside Chapin, to be an early proponent of evidence-based practice in public health. This similarity between the work of Forbes and Chapin was not lost on Newsholme, who wrote in Forbes' obituary that he ‘knew them both intimately; and it is right that the names of Chapin and Forbes should be remembered in this practically important research’. 8 Whilst this remains an endorsement of Forbes' legacy, it must also be remembered that the precise date when Forbes changed his practice is unknown. Therefore, it is impossible to gauge whether Forbes changed his practice independently, or whether he was following Chapin's lead. However, as Chapin's seminal work on the issue, The Sources and Modes of Infection, was published in the same year (1910) as Forbes reformed his practice, 30 it appears likely that Chapin influenced Forbes to act. Nonetheless, this still places Forbes in the vanguard of a paradigm shift in British public health that would go on to shape the field to the present day. Additionally, Forbes' ‘Brighton methods’ for the care of tubercular patients lend further credence to a legacy of pioneering practice, as they clearly show an appreciation of the risk of asymptomatic transmission of disease. This is exemplified in his aim of separating nurses working on different wards, to prevent the carriage of infection to other parts of the hospital by assumedly asymptomatic staff. 19
Relevant to any discussion of Forbes' legacy is his apparent support for eugenic policies. Of note are his comments regarding the sterilisation of males with transmissible defects, although there is no evidence that he ever instituted such practices as MOH. Nonetheless, these writings may have contributed to the persistence of a now discredited belief system. 34 Whilst these views would rightly not be acceptable today, it should also be remembered that they were mainstream among medical practitioners during this period. 40
Contributions to Brighton
From the beginning of Forbes' term in 1908 to the end of his term in 1939, the town's infantile mortality rate decreased from 111 to 61 per 1000, a staggering reduction considering that this period saw both a world war and a devastating pandemic. 31 As it relates to Brighton, his frequent clashes with policymakers are also relevant. This is because at the centre of Forbes' concerns lay the people of Brighton, especially the poorer classes. Indeed, his disagreements with government over nutrition and housing primarily stemmed from concern that current practice disadvantaged the poor. 31 This care and dedication Forbes showed for the town's people may be reflected in his being awarded an MBE in 1918, the bestowing of the 1931 presidency of Brighton's Medico-Chirurgical Society, as well as the very fact that he remained in his post for 30 years.24,41 These factors along with his influence in slum clearance demonstrate his undeniable influence on the development of modern-day Brighton.
Applicability of Forbes' work to managing COVID-19
Similarities
Many parallels exist between Forbes' experiences and those of today. For example, Forbes’ difficulty in convincing ‘laymen’ of asymptomatic transmission endures and has proven a challenge in managing COVID-19.1,12 Forbes' focus on increased ventilation to tackle influenza in 1918 is also mirrored in our contemporary experience, as Brighton and Hove Council in October 2020 advised premises to ensure good ventilation when re-opening to the public to ‘help reduce the risk of coronavirus spreading’. 42
A striking similarity is also seen in the knee-jerk reaction of closing primary schools. This was the first measure instituted by Forbes as well as one of the earliest by the UK government in 2020.22,43 This is of relevance, as in both cases, these actions were of questionable efficacy. In 1918, this was due to the closures being too late and in 2020 due to the epidemiology of COVID-19 infection, which appears to affect children aged 0–10 years at a far lesser rate than adults. 43 In both cases however, an assumption appears to have been made from the outset that young children represent a virulent vector of transmission. This is evidenced by Forbes' relentless focus on measures to limit the activities of children in 1918 and in 2020 by media portrayals of children as ‘super-spreaders’, despite multiple studies attesting to the contrary.22,43,44 These assumptions may have proved damaging to control efforts, by drawing Forbes' focus away from other target groups. Similarly in 2020, numerous authors, including The Royal College of Paediatrics and Child Health in an open letter to government, considered the protracted closure of schools to have been more damaging to the long-term well-being of children than it was beneficial to the population.45,46 This may be more relevant to children aged 0–10 years as data pertaining to older children and teenagers indicates higher levels of transmission. 47
Forbes' views on vaccination are also relevant today, as he wrote in one paper concerning the mandating of smallpox inoculations that ‘unfortunately, compulsion is anathema in England…it is quite impossible to enforce general and repeated vaccinations’. 48 This theme has persisted to the present day with Prime Minister Boris Johnson echoing Forbes' words in early December 2020, ensuring parliament that COVID-19 vaccines would not be mandatory, adding that compulsion was ‘not part of our culture or ambition’. 49 The implementation of vaccination in Brighton by Forbes in 1918 also mirrors aspects of today's ongoing roll-out. An example is the priority Forbes gave to frontline workers such as nurses, which closely mirrors the COVID-19 vaccination programme. 22
Differences
In 1918, only 0.1% of Brighton's population were inoculated. 22 Additionally, the vaccine targeted bacteria to prevent a viral illness, whereas the COVID-19 vaccinations target the coronavirus itself. The slight efficacy observed by Forbes may be explained by the fact that by inoculating against bacterial strains, the vaccine may have prevented the secondary bacterial pneumonias that often killed following influenza. 28
Further divergence is seen in Forbes' emphasis on largely asymptomatic transmission, contrasting with initial government policy in early 2020 not to test all patients leaving hospitals and going in to care homes. 50 The health secretary defended this decision as ‘asymptomatic transmission was not known’, despite this decision likely contributing to the spread of COVID-19 in care homes. 50 This assumption that asymptomatic transmission would not occur was borne out of observations of other coronaviruses, where transmission is generally symptomatic. 51
Advising premises to keep their halls adequately ventilated, Forbes wrote of the importance of keeping fans ‘running during the performance’. 22 In July 2020, a widely publicised study found that in an air-conditioned restaurant in Guangzhou, droplet transmission and subsequent infection was consistent with airflow direction. 52 Other studies have reported similar findings and since influenza is also spread via droplet transmission, it is possible that Forbes’ measures to provide indoor air movement with no commensurate social distancing increased transmission. 53 Forbes' instructions certainly contrast with COVID-19 advice from the World Health Organization, which stresses the risk of fans spreading infection. 54
In 1918, peak mortality occurred in the 25–35 years age range, whereas with COVID-19 the ≥ 70 years age group are most severely affected.25,55 Ultimately, the major complicating factor in 1918 was the co-occurrence of the First World War. This defined all elements of the national response, as demonstrated by Newsholme's reluctance to disrupt the war effort. As such, the war effort may be the critical factor in why a generalised lockdown resembling our contemporary experience did not occur in 1918.
Conclusion
Whilst Forbes' work during Spanish flu likely did little to contain the outbreak, it certainly demonstrated several hallmarks of pioneering work and practice. This is also tangible through his work in challenging the long-established tradition of terminal disinfection, placing him at the forefront of a public health revolution in this country. However, his promotion of eugenics forms a more uncomfortable part of his legacy and contrasts with his advocacy for the poor of Brighton evident, for example, in his work to eradicate slums. In conclusion, his significant contributions to empirical study and preventative medicine in public health should rightly be placed alongside those of Niven and Chapin.
Finally, in comparing the responses to Spanish flu and COVID-19, what is most striking is the far-reaching effects of flawed assumptions made in both pandemics in relation to both child and asymptomatic transmission. Herein lies another target for future research and pandemic containment strategies, as finding ways of determining key characteristics of emerging pathogens earlier on would reduce the need for basing public health responses on unproven assumptions, and risking the devastating consequences this can have. Accordingly, in the EU's executive summary on future pandemic preparedness, it is stated that ‘crucial scientific questions should be clarified as quickly as possible…to rapidly inform effective and safe public health measures’. 56 Doing so would help to ensure that when the next pandemic strikes, broad assumptions do not cloud the collective response.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.