
Abstract
Sir Arthur William Mickle Ellis (1883–1966) was born, raised and educated in Toronto, Ontario, Canada. He had a distinguished medical career in North America and Europe which spanned important developments in medical research and education and culminated in appointment as Regius Professor of Medicine at Oxford University. He was a resident physician at the newly created Hospital of the Rockefeller Institute before the start of World War I. Serving with the Canadian Army Medical Corps in England, and responsible for the care of soldiers taken sick with highly virulent cerebrospinal meningitis, Ellis attempted an ambitious therapy and undertook laboratory investigations that impacted management of the disease directly. After the war, he became the Director of the Medical Unit and the first Professor of Medicine in the University of London at the London Hospital, and subsequently Regius Professor of Medicine in Oxford in World War II. As a research-driven academic physician, the career of Sir Arthur Ellis was influenced profoundly by Sir William Osler (1849–1919), the first Canadian to hold the position of Regius Professor in Oxford.
Keywords
Introduction
This article outlines Arthur Ellis's family background and medical education, his early clinical experience in Canada and the United States, including his time as a resident physician at the new Hospital of the Rockefeller Institute for Medical Research in New York. It then considers in detail his service as a medical officer in World War I (WWI) with the Canadian Army in England and France, when Sir William Osler singled him out for special praise and brought him to the attention of London's medical elite. It concludes by summarising his subsequent career in the United Kingdom as Director of the Medical Unit at the London Hospital and Regius Professor of Medicine in Oxford, together with an appreciation of his strengths and weaknesses as seen by his contemporaries.
While in charge of meningitis patients during an outbreak of a highly virulent form of cerebrospinal meningitis (CSM) in wartime England, Ellis used his clinical and laboratory expertise to attempt an ambitious treatment using an epidemic-specific anti-meningococcal serum made in collaboration with the Lister Institute of Preventive Medicine. His subsequent work at a mobile laboratory on the Western Front helped identify different strains of meningococci and led directly to the development of strain-specific sera in England during the war. This aspect of Ellis's career has been mentioned fleetingly in other accounts but is illuminated here by archive records supplemented by a range of primary and secondary sources.
Background, education and early career
Arthur William Mickle Ellis was born on 4 May 1883 in Toronto, Ontario, Canada. He was the second child and eldest son of English-born physician William Hodgson Ellis (1845–1920) and his Canadian-born wife Ellen Maude Mickle. 1
The Ellis family had moved to Toronto in 1863, whereupon William H. Ellis entered the University of Toronto as a student, graduating Bachelor of Arts (BA) with the Gold Medal in Natural Sciences in 1867. He completed his Bachelor of Medicine (MB) degree in 1870, went to England to become a Licentiate of the Royal College of Physicians of London, returning to Toronto in 1871 to become Professor of Chemistry at the Medical Faculty of Trinity College.2,3
In 1878, with the opening of the School of Practical Science, Dr W.H. Ellis became Assistant Professor of Chemistry and then Professor of Applied Chemistry from 1887. When the School became the Faculty of Applied Science and Engineering in 1907, he was made Head of the Chemistry Department and acted as Dean from 1914 to 1919. He was also Lecturer in Toxicology from 1892 and Professor from 1897 to 1913, Public Analyst for the Inland Revenue Department, and forensic advisor to the Attorney General.2,3
Arthur W.M. Ellis obtained his early education at the Church School and Upper Canada College. 4 According to the Canadian census of 31 March 1901, the 17-year-old Arthur was living with his parents, elder sister Ethel and younger brother Harold, and was recorded in employment as a bank clerk. 5
Arthur entered University College, University of Toronto in 1902. 6 He was evidently fully involved in the varsity life, being a member of ‘The Thirteen Club’, which had been formed ‘to promote social intercourse among the members and bring them in contact with prominent men’, partaking in Junior and Senior Arts Hockey and Rugby, and playing for the University Cricket Team. 7 Although acting as Secretary-Treasurer to the latter, his sporting prowess is unclear since a rare scorecard of victory over a touring University of Pennsylvania side reveals that Ellis batted well down the order and was out for a duck. 8
Ellis graduated BA with honours in Biological and Physical Sciences in 1906 and entered the Faculty of Medicine (Figure 1).4,9 In his final year, he served as Class Assistant (Sessional) in the Department of Pharmacy and Pharmacology. 10 Having received the MB in 1908, he was one of several graduates appointed Resident Assistant in the Hospital for Sick Children. 11 After this initial year of clinical training, he served as Resident Staff Officer, Lakeside Hospital, Cleveland, Ohio and Demonstrator in Pathology at Western Reserve University Medical School in 1909–1910. 1
Photograph of Arthur W.M. Ellis. University of Toronto. Torontonensis: The Year Book of the University of Toronto, Volume 8. 1906, p.51.
Dr Ellis returned briefly to the University of Toronto as a Fellow in Chemical Pathology, a sessional appointment he held officially until 30 April 1911. 12 During this time, he undertook laboratory research in the Department of Pathological Chemistry, which involved chemical analysis of urine samples from one case of acromegaly and from a patient suffering severe vomiting during pregnancy, and published the findings of his studies.13,14
The Hospital of the Rockefeller Institute for Medical Research
In late 1910, Ellis was appointed full-time Assistant Resident Physician at the Hospital of the Rockefeller Institute for Medical Research, New York City, which had been officially inaugurated on 17 October 1910. Rufus Cole MD (1872–1966), Director of the Hospital, chose talented young doctors with an aptitude for medical research who would have full control of a ward of patients suffering from a disease of interest and would be provided with enough assistance to leave time for them to undertake related research in an amply equipped laboratory. Five diseases were chosen initially for concentrated study: heart disease, ‘intestinal infantilism’ (coeliac disease), lobar pneumonia, poliomyelitis and syphilis.15,16
Syphilis was of especial interest to the Rockefeller Institute for three reasons. First, work in its laboratories had confirmed the discovery of Spirochaeta pallida (Treponema pallidum) in 1905 as the specific cause of the disease. Second, the Institute had by means of a special grant helped fund the experimental work that led to the discovery of the drug salvarsan in Germany in 1910. Third, the Director of Laboratories, Simon Flexner MD (1863–1946), had shown that administration by intrathecal injection into the spinal fluid was the most effective way to deliver anti-meningococcal serum for the treatment of epidemic CSM.15,17
Homer Fordyce Swift MD (1881–1953) was placed in charge of the hospital's studies of syphilis and he and Arthur Ellis collaborated closely in the clinic and laboratory to develop a new intraspinal treatment for syphilis of the central nervous system. The two appear together in a rare photograph of the medical staff of the Rockefeller Institute Hospital (Figure 2). Most of those present were recorded as staff members in 1911, and some had joined the hospital after the beginning of the year, suggesting that the image may date from 1911, rather than the archival date of 1910.18,19
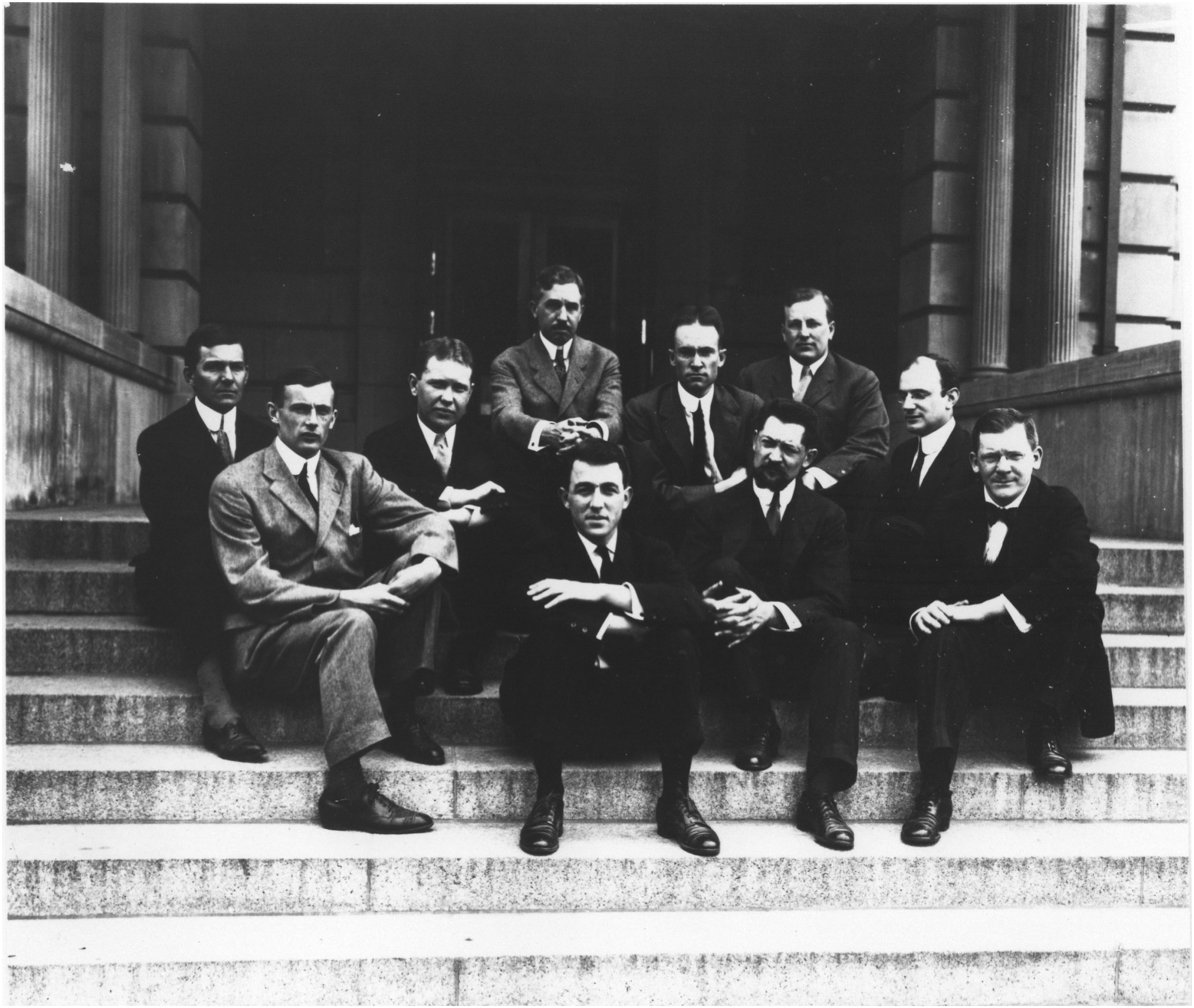
Hospital of the Rockefeller Institute. Group Photo. Dated 1910. Arthur W.M. Ellis (at the front on the left-hand side of the picture), Rufus Cole (in the centre at the back) and Homer F. Swift (second row on the right, facing towards the left). Other personnel listed: Alphonse Raymond Dochez, George Draper, Francis McCrudden, Henry K. Marks, Florentin Medigreceanu, Francis W. Peabody, and George Canby Robinson. Rockefeller Archive Center. DigitalCommons @ RU. https://digitalcommons.rockefeller.edu/hospital-of-institute/22/ (accessed 22 December 2024).
Swift and Ellis determined that salvarsan injected into the vein of a patient failed to reach the sub-arachnoid space around the brain and spinal cord in therapeutic amounts; when injected directly into the spinal canal, however, the drug proved too irritating to the nervous system. They devised a new method by first injecting salvarsan intravenously, drawing serum after a few hours while the drug was still in the circulation, and then injecting the ‘salvarsanized’ serum intrathecally, which was better tolerated. The Swift-Ellis treatment proved beneficial in cases of tabes dorsalis and some other types of neurosyphilis and remained in use until the advent of penicillin in the 1940s.15,20
Their productive collaboration resulted in a series of jointly authored publications with Swift tending to feature as first author on the principally clinical papers and Ellis on papers of a more experimental nature.21–28 Ellis also published on studies of syphilis as sole author.29,30
He further collaborated with other researchers at the Rockefeller Institute, notably the cancer pathologist James B. Murphy MD (1884–1950) and the pioneering clinical chemist Donald D. Van Slyke PhD (1883–1971).31–33 Having fulfilled his early promise, in July 1914, the 31-year-old Arthur Ellis was promoted Associate Resident Physician. 34
No. 1 Canadian General Hospital
After Britain declared war on Germany on 4 August 1914 the Dominion of Canada began mobilising its military forces. Ellis signed his attestation papers on 23 September to serve in the Canadian Over-Seas Expeditionary Force (CEF) then assembling at Valcartier Camp, Quebec. 35 Commissioned Captain in the Canadian Army Medical Corps (CAMC) he joined No. 1 Canadian General Hospital. On 30 September the hospital staff sailed from Quebec City bound for England on the SS Scandinavian (Figure 3). 36

Officers, No. 1 Canadian General Hospital. SS Scandinavian, October 1914. Captain A.W.M. Ellis is standing in the back row, second from the right. Cameron K. History of No. 1 Canadian General Hospital, 1914–1918. Sackville, New Brunswick: Tribune Press, 1938.
The hospital staff joined the first Canadian contingent on Salisbury Plain and took on the duties of camp hospital at the end of October. The work began in tents at West Down North Camp and the tent hospital continued to operate until December. The main hospital was set up in Bulford Manor during November but additional accommodation was required there and at Netheravon because of the number of sick resulting from particularly wet and flooded conditions on the Plain at the time. Moreover, a cottage hospital was established at Bulford especially for the treatment of meningitis patients.37,38
Lieutenant-Colonel George G. Nasmith CAMC (1877–1965), a sanitary advisor in charge of water purification, left a vivid record of the times in his memoir On the Fringe of the Great Fight. Nasmith recalled one occasion he and Ellis were dining in ‘The Silver Grill’ in Salisbury when a civilian sneeringly insulted the Canadians. Confronting the man: Captain E– got worked up to the point of explosion as he watched the fellow unconcernedly keep on eating. ‘You snivelling cur, I’ve a good mind to rub your face in that gravy, by G– I will rub it in that gravy!’ exploded the Captain, and in the instant he seized the dinner-plate in one hand and the fellow's head in the other and brought them quickly together, rubbing the man's chin and nose briskly round and round in the mixture of congealing gravy and potatoes.
The first case of CSM among the Canadian troops on Salisbury Plain was recorded on 18 October and two further cases which occurred in the same month were all sent to Tidworth Isolation Hospital. The next four cases, manifesting between 8 November and 3 December, were admitted to No. 1 General Hospital and recovered or seemed to improve. By contrast, after 12 December there arose a spate of 14 new cases of CSM with more pronounced virulence and six patients died during the month, raising serious concern about the outbreak. 40
Lieutenant-Colonel Nasmith travelled to London to seek help from experts at the Lister Institute of Preventive Medicine in identifying the contacts of meningitis cases who were potential carriers of meningococcus. 41 The Institute was an independent institution focused on research, instruction and treatment relevant to the prevention and cure of infectious diseases. Its Serum Department pioneered the production of diphtheria antitoxin in the United Kingdom in 1894, developed other serum products including anti-meningococcal serum, and had become an established supplier to the U.K. market vital to the war effort. 42
The Director of the Lister Institute agreed to loan an experienced bacteriologist, Dr Joseph A. Arkwright MD (1864–1944), who had expertise in cultivating meningococci from epidemic and sporadic cases of CSM.43,44 A few days after Christmas, the Canadians urgently brought down the necessary apparatus to establish a diagnostic laboratory, amounting to 780 pounds of excess baggage, by passenger train. 41 The laboratory was established under the charge of Captain Allan C. Rankin CAMC (1877–1959) in Cottage No. 3 at Bulford Manor which housed the wards dedicated to CSM patients under the care of Captain Ellis. 45
Sir William Osler and CSM
Sir William Osler (1849–1919) took a special interest in Arthur Ellis and his work with CSM. During his long career, Osler published more than 1400 works, of which nearly 200 papers, reviews, editorials and monographs dealt with neurological disorders. His writings documented the evolution of the general medical understanding of meningitis, the occurrence of sporadic and epidemic forms of the disease, introduction of lumbar puncture which Osler advocated in the investigation of the problem, and the identification of distinct types of meningitis associated with different types of infections. 46
In 1882, Osler had encountered CSM in a child while performing autopsies in Montreal. 47 In subsequent discussion of cases at meetings of the Canada Medical Association and Philadelphia Neurological Society he noted the problem of misdiagnosis and stressed the importance of post mortem examination.48–50 At Johns Hopkins Hospital, Baltimore, he presented and lectured on cases admitted to the hospital.51–55 He contributed chapters to medical text-books and delivered the Cavendish Lecture to the West London Medico-Chirurgical Society in 1899.56–58 Later, he lectured to Edinburgh students following an epidemic of the disease. 59 He would also publish on the subject during the war.60,61
As Regius Professor of Medicine in the University of Oxford, Osler had been appointed Honorary Colonel in the Oxford Regiment and would become attached in an honorary capacity to several hospitals treating Canadian troops (Figure 4). These included: the Queen's Canadian Military Hospital at Beachborough Park, Shorncliffe, near Folkestone in Kent; the Duchess of Connaught's Canadian Red Cross Hospital at Taplow; and the Daughters of the Empire Canadian Red Cross Hospital for Officers in London. It is not surprising that Osler should have taken a keen interest in the epidemic of CSM unfolding on Salisbury Plain.62–65

Detail of photograph of William Osler in uniform at Cliveden, dated 20 March 1916. National Library of Medicine. http://profiles.nlm.nih.gov/101743406X60 (accessed 22 December 2024).
‘The boys have had a deuce of a time at the Salisbury Camp – soaked in rain & knee deep in mud. Finley was here for a few days & Ellis from Toronto this week end’ wrote Osler at the start of January 1915. 66 ‘I have been away for a week – at the Can. Hospital Folkestone and at the Canadian Camp Salisbury Plain investigating an outbreak of cerebrospinal meningitis’. 67 He commented on the epidemic in a letter to Princess Louise on 21 January and praised the medical staff: ‘One doctor in particular, a young Canadian from the Rockefeller Institute, New York, who fortunately is an expert in matters relating to the serum treatment of the disease’. 68 And in two other letters in January: ‘I spent three days there last week at Bulford’. and ‘Ellis of the Rockefeller is doing splendid work with it’. 69
A special meeting was arranged at the Royal Society of Medicine (RSM) in London on 26 February 1915 to discuss the epidemiology of CSM. 70 In the Chair was the President of the Section of Epidemiology and State Medicine, Charles J. Martin FRS (1866–1955), Director of the Lister Institute. 71 The proceedings were opened by William Osler, who had been a member of the Lister Institute's Governing Body since 1906, a position he took over from his predecessor as Regius Professor, Sir John Burdon Sanderson (1828–1905) and one he would continue to hold until 1916. 72 Among the invited speakers was Captain Ellis who described his work in treating patients with a new serum prepared with the help of the Lister Institute's Serum Department. 73
Serum treatment of CSM patients
By the time of the RSM meeting, 40 cases of CSM had occurred among the troops of the CEF on Salisbury Plain with 26 deaths, a mortality exceeding 60%. Various anti-meningococcal sera made in horses had been used for treatment, including products from Burroughs Wellcome & Co. and the Lister Institute in Britain and from the American firms H.K. Mulford Co. and Parke Davis & Co. One patient had received more than 20 intrathecal injections with sera from all these manufacturers yet still carried the meningococcus in his spinal fluid two and a half months after the onset of his illness.73,74
Reasoning that the commercially available sera had failed because the appropriate strains of meningococci had not been used in their manufacture, Ellis and his colleagues began to culture samples which had been isolated from the cerebrospinal fluid of three of his patients at Bulford on 6 January 1915. 73 With the intention of making a new serum for the prevailing epidemic, he sent these isolates to the Lister Institute to include in the mix of meningococci previously obtained from multiple cases of both epidemic and sporadic CSM that were used to inoculate horses in the typical production of so-called ‘polyvalent’ anti-meningococcal serum. 75
Given the scarcity of the disease before the war, the Serum Department had only a single horse in use to make immune serum for treating CSM – ‘Tasmania’ – which had been bled only infrequently, and not since May 1914. 76 A new round of bleeding began on 28 January 1915, a period of about three weeks after inoculation, when 6000 cc (cubic centimetre or ml) of immune blood plasma was isolated and converted into a new batch of serum (M8). 77 Part of this preparation was output two days later in 350 bottles, each containing 10 cc of the anti-meningococcal serum. 78 During a further two weeks before release, the batch of serum would have been tested for sterility and the horse observed to ensure it stayed healthy. 79
Army medical case sheets show that 31-year-old Private Robert Carter, 11th Battalion, Canadian Infantry, taken sick on 25 November 1914, was the patient who had failed to respond to repeated serum treatments (Figure 5). On 11 February 1915, he was injected with 40 cc of ‘Serum made by Lister Inst. Polyvalent to which recently strains from this epidemic (Carter, Kennedy, Palmer) added’ and received further injections on a number of days following. 80 Ellis noted that clinical improvement set in immediately, the spinal fluid tested negative for meningococcus after three days and fever abated after four, suggesting that ‘even when the outbreak did not yield to stock sera, one could in a few weeks produce a serum from the organism isolated from the cases from which efficient results could be expected’. 73
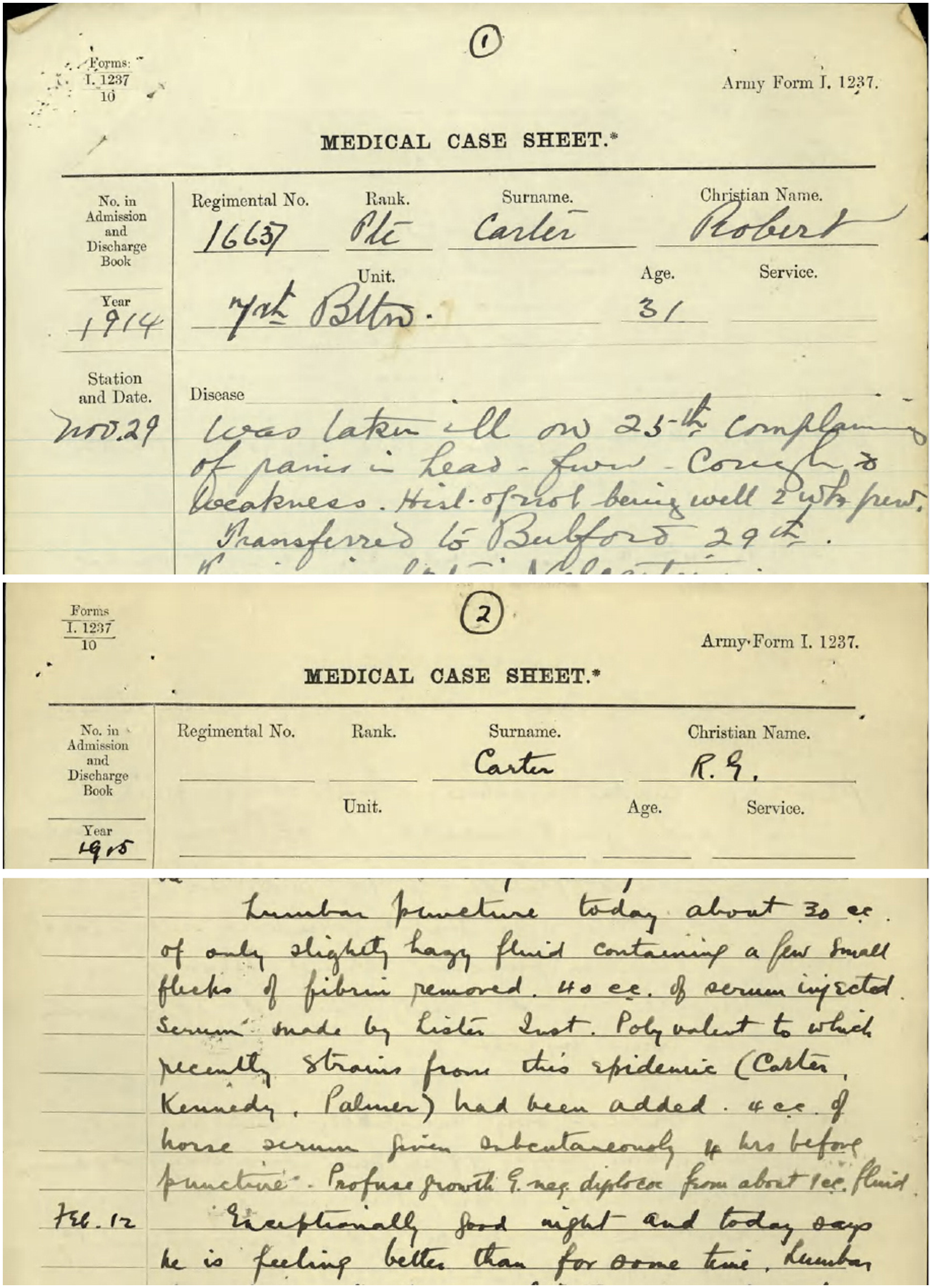
Extracts from medical case sheets in the service file of private Robert G Carter, recording the use of specially prepared Lister Institute serum. Library and Archives Canada. https://central.bac-lac.canada.ca/.item/?op=pdf&app=CEF&id=B1549-S013 (accessed 22 December 2024).
One day before the RSM meeting was held, however, Bulford Hospital closed following the move of the 1st Canadian Division to the Front and its patients were transferred to other hospitals. It is not known if Private Carter received any further serum injections but his death from ‘cerebrospinal meningitis (chronic)’ was recorded at Salisbury Isolation Hospital on 26 March. 80 He was buried with honour at Stratford-sub-Castle (St Lawrence) Churchyard. 81
However, surviving records also show that Private Frank Cobbin, taken ill on 31 January and treated at Netheravon, received two 30 cc doses of the special Lister serum on 11 and 12 February. He recovered gradually and was put on leave in March. Persistent neurological after-effects led him to be discharged from duty in 1916, although he later re-enlisted.82,83
No. 5 (Canadian) Mobile Laboratory
Early in February 1915, the Canadian government had decided to add a mobile laboratory to its medical establishment. Among the allocated staff were two of the most experienced and popular officers of No. 1 Hospital, namely Captains Ellis and Rankin, under the command of Lieutenant-Colonel Nasmith. 84
Although all the necessary arrangements were made in good time, the orders for Nasmith and colleagues to proceed to France were not issued for three weeks by mistake, delaying their departure until 21 March so they became known as ‘The Lost Canadian Laboratory’. Officially, No. 5 (Canadian) Mobile Laboratory was attached to No. 7 Clearing Hospital and initially located in a spacious, well-appointed, 18th-century room in the Hôtel de Ville at Merville. The laboratory carried out a wide range of routine chemical, bacteriological and clinical analyses. At the same time, in spite of essential work, occasional disruption of supplies and bombs dropping nearby, Ellis continued to conduct research.85,86
In his experiments, Ellis prepared monovalent sera by immunising rabbits against single strains of meningococcus, examined the capacity of such sera to agglutinate 46 different isolates and identified two main types – designated Type I and Type II – that were widely distributed and equally prevalent. He noted the parallel with earlier work identifying multiple strains of pneumococcus by Cole and his colleagues at the Rockefeller Hospital and explicitly suggested that better results could be obtained with the serum treatment of CSM if ‘monovalent horse serum of appropriate type, and therefore known to be active against the infecting organism, were employed in place of the polyvalent serums at present in use’. 87
The same two main meningococcal types were identified by studies carried out independently and published simultaneously by the Lister's Arkwright using samples from British Forces in France and various epidemic foci in England, including Salisbury Plain. 88 The disease had first appeared among British troops on the Plain on 13 November, casting suspicion on the CEF as some cases had occurred in Quebec and during transportation, although British military cases occurred in England earlier. 89 The Canadians were understandably sensitive to suggestions their troops introduced the disease or were responsible for its spread.90,91 Work at the Royal Army Medical College further identified two rarer strains, Types III and IV. 92
By January 1916, the Lister Institute had begun to inoculate two horses with Ellis's strains of meningococci: one with Type I (M.4) and one with Type II (M.12). Samples of blood were repeatedly taken, and their neutralising potency determined against the immunising strain in each case; by April, the agglutinating strength of each horse serum had risen six-fold. 93 The serum subsequently drawn from these horses was handled, bottled and labelled (‘El’ for Ellis) separately from regular batches of pooled serum processed during the same period (Figure 6). 77 The War Office judged the Lister monovalent sera efficacious and requested large quantities of sera against each of the four Types for the winter of 1917–1918. 94
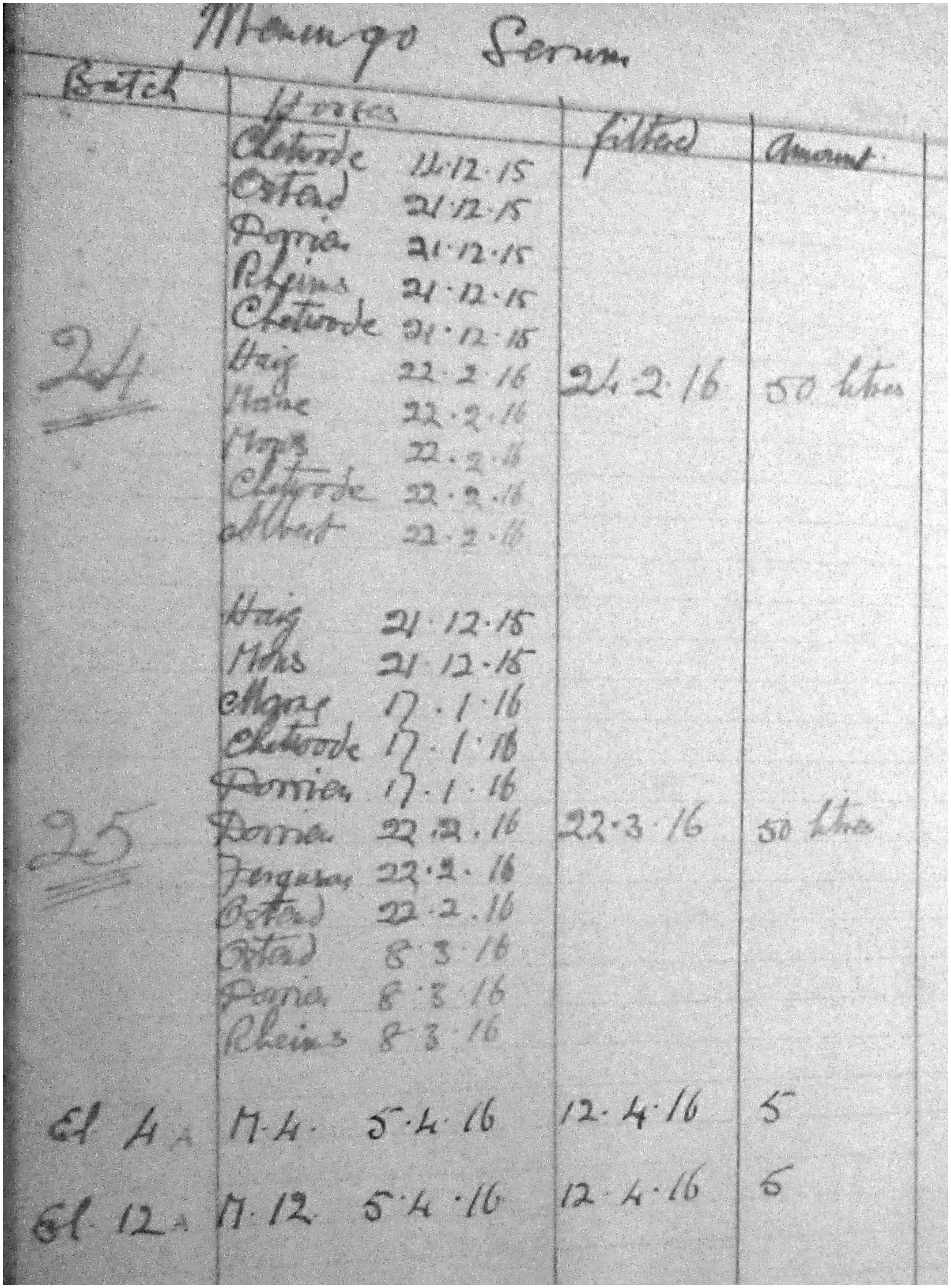
Detail of page from Lister Institute Serum Department batch processing book, showing typical 50-L batches of pooled anti-meningococcal serum from multiple horses and special 5-L batches from individual horses inoculated with meningococcal strains M.4 and M.12 isolated by Ellis. Lister Institute. Anti-toxin batch, September 1914–February 1918. Wellcome Collection Archives. SA/LIS/I.35/1.
It is unclear to what extent Ellis had the opportunity to stay in contact with Sir William Osler during the time of his military service in France; however, his army records show that he was granted 10-days’ leave from his duties from 29 April 1916, returning to duty on 9 May. 35 It is probable that he travelled to England on this occasion since he appears to have met with Osler who, writing to a Canadian acquaintance in early June, enclosed ‘a snapshot taken with Arthur Ellis’, the whereabouts of the photograph being unknown today. 95
Ellis was made officer commanding No.5 (Canadian) Mobile Laboratory from November 1916 and promoted Major a month later and became Assistant Advisor in Pathology to the 4th Army in April 1918.35,96 He spent most of January 1919 recovering from influenza at the Michelham Convalescent Home in Mentone, France. On returning to England in early February, he was attached to the Petrograd Red Cross Hospital for Officers in London. In July, he returned to Canada on the RMS Carmania and was struck off the strength by reason of general demobilisation. 35 Ellis was mentioned in despatches three times in 1917, 1918 and 1919 and awarded the Order of the British Empire (Military Division).97–100
The London Hospital
After WWI, medical teaching in London was reorganised following the recommendations of the Haldane Commission in 1913. Between October 1919 and May 1920, medical and surgical professorial units were created at four London teaching hospitals: St Bartholomew's, St Thomas's, University College Hospital and the London Hospital. 101 The directors of these units were to be whole-time professors of medicine in the University of London, combining clinical work, experimental studies and medical teaching. 102 The units provided integration of bedside teaching and ongoing research and were staffed by full-time clinicians employed by the university rather than the individual medical school. 103
The new model was based in major part on the productive fusion of medical science and clinical teaching in the United States which had originated in Germany. 104 In the late 19th century, the American physician William H. Welch (1850–1934) had introduced the German system at the Johns Hopkins Hospital. The idea was then brought to England by Osler when he was appointed Regius Professor in Oxford and it was he who urged that a professor of medicine needed the set-up of a full-time unit if he was to treat his patients and teach his students properly as well as advance medicine by research. 105
On returning to London in 1919, Ellis had worked for a time as a chemical pathologist at Guy's Hospital with a grant from the Medical Research Council. He joined the London Hospital in 1920, first as Assistant Director of the Medical Unit and then, in 1924, he was appointed Director of the Unit and the first Professor of Medicine in the University of London at the London Hospital (Figure 7). The principal interest of Ellis's ‘school’ would be renal disease, especially the correlation of clinical and pathological features, and the relationship of hypertension and kidney disease. 1

Aerial photograph of the London Hospital site, from north–west, c.1925. The image shows the front of the main hospital block facing onto the Whitechapel Road with the stand-alone Medical School building located at the south–western corner of the main complex of buildings on the right-hand side of the photograph. Barts Health NHS Trust Archives and Museums. RLHLH/P/2/1/2.
Ellis had taken the MRCP in 1920, was elected FRCP in 1929, and nominated Croonian lecturer in 1941. 106 His three lectures on the ‘Natural history of Bright's disease’, published in the Lancet but not delivered in person owing to World War II (WWII), were the culmination of 20 years of personal observation and a decade of combined clinical and pathological study at the London Hospital, involving analysis of some 600 cases, with 200 post-mortems, made by the same observers. 107
On the basis of this work, nephritis was classified into two distinct pathological types: type-I, of typically acute onset, was in most cases reversible and occurred particularly after infections in young patients; type-II, of more gradual onset, was in most cases progressive and tended to occur in older patients. This clinical distinction in the natural history of nephritis was widely accepted and Ellis thought it especially helpful in the teaching of students and determining the prognosis in individual cases. 108
According to Ellis's long-term colleagues, Dr Clifford Wilson (1906–97), one-time Assistant Director of the Medical Unit, and Dr Horace Evans (1903–63), later Baron Evans of Merthyr Tydfil: Ellis was not concerned to show that any individual lesion of the glomerulus was specific for a particular type of nephritis; he attempted rather to demonstrate that the pattern and progress of histological change had a separate natural history in the two types, which corresponded to the clinical picture.
109
On the night of 21 October 1940, Arthur Ellis was one of the staff having dinner at the hospital when a succession of explosions caused them to dive under the table for cover. He had remained on site in charge of the resuscitation ward where each bed had been fitted up with an oxygen tube, an electric heater and a sphygmomanometer. His team, which consisted of a first assistant and four students, kept pulse, respiration and blood-pressure charts. Ellis's clinical judgement was considered invaluable and his personal interest in people rendered him popular among his colleagues. 111
Subsequently, Ellis became an Adviser in Medicine to the Ministry of Health in 1941–1942 and Director of Research in Industrial Medicine for the Medical Research Council in 1942–1943. In 1943 he was appointed Regius Professor of Medicine in Oxford. In the same year he was appointed Consulting Physician to the London Hospital and to the Radcliffe Infirmary, Oxford. He remained Regius Professor until his retirement in 1948 at the age of 65 when he was appointed Emeritus Professor. He was knighted in 1953. 112
The professor
Arthur Duncan Gardner (1884–1978), who succeeded Ellis as Regius Professor, recalled first meeting him as a medical officer in the CAMC when given lunch with his unit in Christ Church, Oxford by Sir William Osler ‘who had taken Ellis warmly under his wing’. In Gardner's estimation, Ellis was ‘obviously a very competent, quick, humorous, and friendly man doing an unselfish job with happy equanimity’. 111 It had been Osler's influence that led Ellis to take up clinical medicine in England after demobilization. 1
According to Walter Russell Brain (1895–1966), Lord Brain of Eynsham, one-time Assistant Physician to the London Hospital, when Ellis helped found the Medical Unit, it was widely regarded as an experiment which many thought might not succeed. But he left it with ‘an established tradition of distinction of work and personnel, and he himself was by that time one of the most influential figures in the hospital’. 112 A photograph of Arthur Ellis taken in the 1940s is shown in Figure 8.

Photograph of Arthur William Mickle Ellis, OBE DM FRCP LLD, c.1940s. Barts Health NHS Trust Archives and Museums. RLHMC/P/3/53.
Writing in an obituary notice in the Lancet, Clifford Wilson observed that one of Ellis's lifelong convictions was that ‘a professor should be no less skilled in the art of medicine than his colleagues’. 113 Another colleague, Leslie J. Witts (1898–1982), had the highest regard for his ability: ‘Although he started his professional career as a pathologist, he made himself one of the best clinicians in London’. 102 In this ambition he was successful, attracting talented students and qualified doctors alike to his unit from his own hospital and elsewhere. 1
Each week, Ellis spent several afternoons in the wards, examining his patients with the ward sisters who were devoted to him. 102 Archibald Clark-Kennedy (1893–1985), who started at the London as a house physician, observed that he ‘took every history most carefully and examined each patient minutely, according to strict routine, and then wanted plenty of time to think his findings over’. His clinical clerks had to be prepared to ‘stand long, waiting round the bed, while he examined the patient in complete silence and only at long last made up his mind’. His opinion was thought as good or better than any other obtainable at the Hospital. 114
Ellis was no great lecturer but impressed on all who worked with him that more errors of diagnosis arise from failure to observe than from inability to interpret. He taught by example rather than by precept; he excelled in instruction at the bedside and in the personal training he gave to the members of his staff and abhorred intellectual dishonesty and authoritarianism in the teaching and practice of medicine. 1 He insisted on straight thinking, often combined with plain speaking, and gained respect and emulation from generations of students. 113
It has been claimed that Ellis was essentially a stop-gap appointment as Regius Professor during the war and left little imprint on the post. 115 He had a constructive mind which made him a valuable member of scientific committees. 106 But he was a poor speaker, nervous and with a hereditary tremor, and not a good chairman. 102 Controversy over the formation of an undergraduate clinical school affected his health, especially towards the end of his tenure, and his wife's chronic illness further restricted his ambitions. 112 Nevertheless, he carried on his clinical work and teaching with patience and enthusiasm. 1
Ellis was a man of complete integrity, great wisdom, a warm heart, quick, rich humour and unstinting helpfulness in any kind of trouble and was tremendously loyal both in his professional and private life.105,111 At all times, however, with kindness and consideration, he put first the interests of patients who throughout his career held him in great respect and affection.1,113
A career in perspective
Arthur Ellis was evidently a bright student who followed in his father's footsteps, training in medicine and displaying a talent for chemical analysis applied to clinical problems. With his experimental instincts, the young doctor was a prime candidate to join the original cadre of resident physicians at the recently inaugurated Hospital of the Rockefeller Institute, a product of the growing importance of laboratory research in the understanding of patients’ ailments and their rational treatment. Ellis' research productivity during his three years in New York suggests he grabbed the opportunity wholeheartedly and was a valued colleague.
It was a matter of chance that Captain Ellis found himself in the unenviable position of being responsible for the care of patients with CSM at the start of a deadly outbreak of epidemic disease. This assignment was not entirely unexpected given that he was an expert in treatment of patients by intrathecal administration of serum, a skill learnt at the prestigious institute that had developed anti-meningococcal serum. And it was certainly not coincidental that the CAMC should have turned to the Lister Institute for assistance owing to its bacteriological expertise and long history of serum manufacture.
No luck was involved in Ellis's determination to help his patients by trying to develop a new, potentially epidemic-specific serum. Given the barely adequate time for immunising a horse, the few patients he was able to treat and the limited follow-up possible, the most promising outcome that could have been expected was the observed evidence of biological activity as assessed by the clearance of meningococci from the cerebrospinal fluid and the simultaneous improvement in clinical symptoms, which stock sera had apparently failed to achieve. Ellis appears to have been the first in England to put this approach into practice during the war.
Ellis's laboratory expertise was put to good use when he transferred to the Western Front. Not content with carrying out his military duties, he found the time and resources to continue studying samples of meningococci isolated from cases of epidemic CSM. Although his identification of two major strains was not unique, and had been preceded by other workers, the outcome was uncertain at the time and the circumstances under which he carried out this research are remarkable. Types I and II became known as the Group A and B meningococci, respectively, in modern nomenclature. 116
Ellis clearly recognised the importance of strain specificity, based on advances in pneumonia treatment at the Rockefeller, and the potential of monovalent sera to outperform polyvalent sera in the clinic. The evidence suggests that his work was instrumental in the Lister Institute developing type-specific sera on behalf of the War Office. Although the opportunity to trial monovalent sera during the war was limited, the long-term legacy of such investigations was the proof-of-principle necessary for the later creation and continued elaboration of specific vaccines for the global control of meningococcal meningitis. 117
While Regius Professor at Oxford, Ellis wrote to his former colleague at the Rockefeller Hospital, G. Canby Robinson (1878–1960): I can never be sufficiently grateful for the luck which brought me to the Rockefeller and to the companionship and friendship of the group that you and Rufus had collected. They were good days in every way and I agree with you that subsequent records suggest that we did not waste our time. I have often thought what a remarkable act of faith it was that we should all have been there consciously attempting to fit ourselves for full-time posts in medicine, when no such jobs existed anywhere.
118
Footnotes
Acknowledgements
I would like to thank Kate Jarman and Ginny Dawe-Woodings of Barts Health NHS Trust Archives and Museums, London for their help in locating original photographs of Sir Arthur Ellis and the London Hospital, provision of high-resolution digital scans for publication, and permission to reproduce them. Lily Szczygiel of the Osler Library of the History of Medicine, McGill University, Montreal, Canada kindly provided access to the letters of Sir William Osler. I am grateful to the library and archives staff of the Wellcome Collection for their helpful assistance and to the Lister Institute of Preventive Medicine for permission to reproduce archive material. I appreciate greatly the advice and encouragement I received from John and Ruth Ward of the Osler Club of London, and helpful correspondence with Christopher Boes and Charles Bryan of the American Osler Society, and with Judith Curthoys at Christ Church Oxford.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.