
Abstract
The common law in the United Kingdom dictates that children facing medical treatment should be treated in accordance with their best interests. The Children Act 1989 also demands that the welfare of the child is paramount. However, in light of the creation of saviour siblings after the case of Quintavalle, it is disputed that the donor child is treated in accordance with his/her best interests when undergoing a non-therapeutic procedure for the benefit of another. The Human Tissue Authority (HTA) can, for example, validate a bone marrow harvest on a child created specifically for harvest without the consent of the High Court. The doctrine of substituted judgement was developed in the United States to substitute a previously competent adult decision, but it is proposed that parents of saviour siblings are reviving it in a modified form to install a speculative psychological benefit into the saviour child to satisfy the criteria for a harvest in common law. As a result, there is a glaring discrepancy between the objective jurisdiction of the courts and the validation of non-therapeutic harvesting procedures upon children by the HTA, opening the door to potential legal action.
Introduction
The House of Lords in Quintavalle v. Human Fertilisation and Embryology Authority (and Secretary of State for Health) 1 confirmed the legality of the selection of tissue-typed embryos for the purpose of benefiting another, leading to the creation of ‘saviour siblings’ in the United Kingdom. 2 The Human Fertilisation and Embryology Act 1990 (as amended in 2008) outlaws the selection of embryos for an organ donation (i.e. a kidney or a liver lobe) under section 1ZA(4) schedule 2, but embryos can be selected for their cord blood, other tissue and bone marrow. 3 The largest obstacle for parents is that of consent at the moment of harvest. The law is clear regarding the rights of children, that is, the welfare of the child is paramount under section 1 of the Children Act 1989 and medical procedures must be in the best interests of the child under the common law. 4 The only saviour sibling case known to date – that of Re Y (Mental Patient: Bone Marrow Donation) 5 – confirms that in the absence of a therapeutic benefit there must be an emotional connection between the donor and her family (e.g. a psychological benefit) to validate the harvest. Justice Connell came to this decision using the ‘interfamilial principle’, which pours the interests of several family members into one pot. 6 Re Y was never intended to be applied to children, but the Human Tissue Authority (HTA) has since published a Code of Practice on child bone marrow donations and has incorporated the decision into its formal donation procedure. A substituted judgement, it will be argued, is likely to occur at the point of consent to create a psychological benefit and validate the non-therapeutic harvest. Statements such as ‘she would want to save her brother’ and ‘she would do it if she was older’ are good examples. The literature in support of saviour siblings (the majority) has stated that the donor child can experience a psychological benefit by feeling a sense of altruism, ensuring future relationships, having a sibling to play with and escaping the grief of death. 7 However, it will be argued in this article that these benefits do not exist because (i) the saviour is too young to acknowledge the psychological benefit, (ii) altruism cannot be assumed and (iii) it is pure speculation to suggest that the saviour will support the donation when she is older. The doctrine of substituted judgement will be examined to reveal its origins and how it could be used to substitute the psychological benefit. The appeal courts have not hesitated in the past to use their inherent jurisdiction to overrule parents if the medical treatment proposed is not in the best interests of the child, and it is this objective standard that is missing from the current donation procedure. This discrepancy between the common law (objective) and procedure (subjective) opens the door to manipulation, unlawful medical procedures on children and potential legal action (not to mention psychiatric harm). 8
The law on saviour siblings
Preimplantation genetic diagnosis (PGD) has been used in fertility treatment to screen for genetic disorders in embryos since the first live birth in 1990.
9,10
The Human Fertilisation and Embryology Authority (HFEA) published a relaxed preimplantation tissue typing (PTT) policy in 2004: PTT can be offered in cases where the embryo is not at risk from the condition affecting the existing child and Depending on the needs of the existing child, it can be acceptable to offer PTT with a view to harvesting bone marrow.
11
The House of Lords in the case of R (Quintavalle) v. Human Fertilisation and Embryology Authority (and Secretary of State for Health)
12
had to decide whether the screening of an embryo for a tissue preference was ‘necessary or desirable’ to ensure that it was ‘in a suitable condition’ to be placed in a woman for it to be considered ‘in the course of’ treatment services under section 2(1), section 11(1)(a) and schedule 2 para. 1 of the 1990 Act. Lord Hoffmann spent considerable time canvassing the words ‘necessary’, ‘desirable’ and ‘suitable’ in his judgement, interpreting the word ‘suitable’ as widely as possible to include the personal preference of the mother: ‘Suitable’ is one of those adjectives which leaves its content to be determined entirely by context…one is concerned to discover whether the scheme and background throw light on the question of whether the concept of suitability includes taking into account the particular wishes and needs of the mother…there was no proposal to include in the ‘clearly prohibited’ list the testing of embryos to enable the mother to choose to carry a child with characteristics of her choice.
13
Lord Hoffmann added that if an embryo was ‘suitable’ to the mother, it met the statutory requirements of necessary and desirable too: Thus, if the concept of suitability is broad enough to include suitability for the purposes of the particular mother, it seems to me clear enough that the activity of determining the genetic characteristics of the embryo by way of PGD or HLA typing would be “in the course of” providing the mother with IVF services and that the authority would be entitled to take the view that it was necessary or desirable for the purpose of providing such services.
14
These short statements supported the creation of saviour siblings (e.g. the tissue typing and selection of embryos with a view to harvest) in the United Kingdom.
15
Parliament has now inserted tissue typing for the purposes of saving a sibling into the Human Fertilisation and Embryology Act 1990 with an insertion into the amending 2008 Act: Schedule 2: Activities that may be licenced under the 1990 Act. Paragraph 1ZA(1): A licence … cannot authorise the testing of an embryo, except for one or more of the following purposes: (d) in a case where a person (‘the sibling’) who is the child of the persons whose gametes are used to bring about the creation of the embryo (or of either of those persons) suffers from a serious medical condition which could be treated by umbilical cord blood stem cells, bone marrow or other tissue of any resulting child, establishing whether the tissue of any resulting child would be compatible with that of the sibling.
Once born, a saviour sibling is in desperate need of welfare protection. The speculative risks of a cord blood donation include multiple birth and prematurity (risks inherent to in vitro fertilization),
16
prolonged efforts to achieve a vaginal birth to increase the amount or quality of cord blood, rapid umbilical cord clamping, raising the new born above the mother to increase placental blood volume, being used as a commodity, a risk of abandonment if there is no match, a lack of self-worth (i.e. value is entangled in a sibling) and psychological harm.
17
The speculative risks of bone marrow donation include puncturing the hipbone 100 times to remove approximately two cups of marrow, pre-harvest screening, anaesthesia (allergy, deprivation of oxygen, brain damage, heart attack and stroke), bone fracture, bone infection, rupture of an artery, skin scarring, hypertension, anaemia, broken needles, blood transfusion, pain, fear of operations, fear of losing a body part, spite, resentment, refusal (if harvested repeatedly), force, manipulation, exploitation, guilt, rejection and being treated as an insurance policy.
18
In light of these risks, the consent procedure for donation between young siblings is expected to be rigorous. The courts have overruled parents if their views on medical treatment have not corresponded with the best interests of their child. In the relevant trail of case law, caution was first exercised in R v. Gyngall when overruling parental responsibility: in exercising the jurisdiction to control or to ignore the parental right the court must act cautiously, not as if it were a private person acting with regard to his own child, and acting in opposition to the parent only when judicially satisfied that the welfare of the child requires that the parental right should be suspended or superseded.
19
The first notable medical case was Re B (A Minor) (Wardship: Medical Treatment) in which the court authorized a surgical procedure on a child against the wishes of the parents: While great weight ought to be given to the views of the parents they are not views which necessarily must prevail. The judge was much affected by the reasons given by the parents and came to the conclusion that their wishes ought to be respected. In my judgment he erred in that the duty of the court is to decide whether it is in the interests of the child that an operation should take place … the fact of the matter is that this court now has to make the decision. It cannot hide behind the decision of the parents or the decision of the doctors; and in making the decision this court’s first and paramount consideration is the welfare of this unhappy little baby.
20
In Re K.D. (A Minor) (Ward: Termination of Access), Lord Oliver described the authority of the court in clear terms: when the jurisdiction of the court is invoked for the protection of the child the parental privileges do not terminate. They do, however, become immediately subservient to the paramount consideration which the court always has in mind, that is to say, the welfare of the child.
21
The focus on the child in a medical context continued in Re J (A Minor) (Wardship: Medical Treatment) in which Lord Donaldson described the decision-making process as exclusively that of the court: the parents owe the child a duty to give or to withhold consent in the best interests of the child and without regard to their own interests. The court when exercising the parens patriae jurisdiction takes over the rights and duties of the parents, although this is not to say that the parents will be excluded from the decision-making process. Nevertheless in the end the responsibility for the decision whether to give or to withhold consent is that of the court alone.
22
In agreement, Balcombe LJ described the purpose of wardship in terms of the ‘reasonable parent’ to ensure objectivity: In deciding in any given case what is in the best interests of the ward, the court adopts the same attitude as a responsible parent would do in the case of his or her own child; the court, exercising the duties of the Sovereign as parens patriae is not expected to adopt any higher or different standard than that which, viewed objectively, a reasonable and responsible parent would do.
23
This opinion is directly applicable to parents of saviour siblings who may be subjective in their decision to harvest. This was confirmed as the correct approach in Re Z (Identification: Restrictions on Publication) by Sir Thomas Bingham who added that sometimes even the view of the reasonable parent may not accord with the objective view of the court: I would for my part accept without reservation that the decision of a devoted and responsible parent should be treated with respect. It should certainly not be disregarded or lightly set aside. But the role of the court is to exercise an independent and objective judgment. If that judgment is in accord with that of the devoted and responsible parent, well and good. If it is not, then it is the duty of the court, after giving due weight to the view of the devoted and responsible parent, to give effect to its own judgment. This is what it is there for.
24
The subsequent decision in Re T (A Minor) (Wardship: Medical Treatment) also made it clear that even the most loving motives of parents (i.e. in saving their own child) were not immune to being set aside: [The cases above] are uncompromising in their assertion that the sole yardstick must be the need to give effect to the demands of paramountancy for the welfare of the child. They establish that there are bound to be occasions when such paramountancy will compel the court, acting as a judicial parent, to substitute the judge’s own views as to the claims of child welfare over those of natural parents – even in a case where the views of the latter are supported by qualities of devotion, commitment, love and reason.
25
There appears to be a subtle message in the case law that parents may not always be entirely objective when doing the best for their child. There may, for example, be a meshing of interests, or the parents may be serving their own needs through their child. A definitive passage by Wilson in Re C (A Child) (HIV Test) – in which a couple wished to control the medical treatment of their baby to suit their own desires – addressed this issue directly: This case is not at its heart about the rights of the parents. And if, as he in effect suggested in his evidence, the father regards the rights of a tiny baby as subsumed within the rights of the parents, he is wrong. This baby has rights of her own. They can be considered nationally or internationally. Under our national law I must determine the case by reference to her welfare.
26
This passage is directly applicable to parents of saviour siblings, that is, the desire to save an older child must not be confused with an adjoining ‘right’ to take advantage of the younger child.
27
The trail of case law finishes at An NHS Trust v. MB, in which Holman consolidated the modern best interests test for children: (x) The views and opinions of both the doctors and the parents must be carefully considered. Where the parents spend a great deal of time with their child, their views may have particular value because they know the patient … although the court needs to be mindful that the views of any parents may, very understandably, be coloured by their own emotion or sentiment. Their own wishes, however understandable in human terms, are wholly irrelevant to consideration of the objective best interests of the child. (iv) The matter must be decided by the application of an objective approach or test. (v) That test is the best interests of the patient.
28
This brings us full circle to Quintavalle. Lord Brown stated that embryo selection for ‘purely social purposes’ would be eradicated using inherent jurisdiction: in the unlikely event that the authority were to propose licencing genetic selection for purely social purposes, Parliament would surely act at once to remove that possibility … failing that, in an extreme case the courts’ supervisory jurisdiction could be invoked.
29
This statement is interesting for two reasons. Firstly, because the embryo does not suffer from the same genetic condition as the existing child, the embryo is selected for purely social purposes (i.e. to meet the desires of the mother). Secondly, because the embryo is selected for purely social purposes, according to Lord Brown it may be subject to wardship once born. 30 In view of the high risks and speculative benefits to the saviour child and the subjectivity of the parents, wardship would be a good option for saviour siblings.
To summarize, the common law is overwhelmingly clear, that is, the best interests of the child must prevail. It is accepted that best interests includes many factors – such as comfort and environment – but these must flow directly to/from the child herself not a third party (i.e. the plight of a sick sibling is not relevant). 31 In practice, therefore, a saviour sibling is entitled to be made a ward of court if her embryo is selected for harvesting purposes (as a result of the passage by Lord Brown in Quintavalle), allowing the court to objectively consider her best interests without the interference of distressed parents or sick siblings. The question to be asked by the HTA is simple, At the exclusion of other parties, according to the objective standard at common law, is it in the best interests of this child to be harvested? The answer should be just as simple, that is, in view of the high risks and lack of benefits, it is not in his/her best interests.
However, the doctrine of substituted judgement (examined below) may have been revived by parents. It is currently possible to override the objective common law by substituting a psychological benefit into the saviour child. It is time to examine the doctrine to reveal how it may be manipulated to provide consent for a non-therapeutic procedure on a child.
The doctrine of substituted judgement
The old jurisdiction of parens patriae (translating to ‘parent of the State’) first emerged in De Prerogativa Regis where the Crown delegated its duty to guard infants, idiots, lunatics and their property to the Chancellor.
32,33
The law used to distinguish between two categories of incompetent adult – the idiot and lunatic – on the grounds that the lunatic (derived from ‘luna’ meaning ‘moon’) had waxing and waning incompetence that could be substituted, whereas the idiot was born insane and remained insane until he/she died. Parens patriae therefore allowed the courts to act on behalf of idiots and lunatics who were ‘incapable to take care of themselves’.
34
The doctrine of substituted judgement began to emerge in ex parte Whitebread, in which Lord Eldon stated of his decision: [it] is not because the parties are next of kin of the lunatic, or as such, have a right to an allowance but, because the Court will not refuse to do, for the benefit of the lunatic, that which it is probable the lunatic himself would have done.
35
The idea of substituted judgement travelled across the Atlantic three decades later to the Court of Chancery of New York and was adopted in re Willoughby.
36
In English law, parens patriae was eventually cast aside following the revocation of the Royal Warrant on 1st November 1960, allowing the new Mental Health Act 1959 to deal with the affairs of adult patients under Part VII. This did not include the power to make medical decisions, so a best interests test was constructed in Re F (Mental Patient: Sterilisation).
37
In regards to children, wardship took hold in the form of welfare under the Children Act 1989. Substituted judgment was pushed out of the U.K. jurisdiction.
In the United States, however, the historical development of substituted judgement is far more interesting. It was called upon to help in the historic adult saviour sibling case of Strunk v. Strunk.
38
In looking to validate a non-therapeutic kidney donation, the Court of Appeal of Kentucky took inspiration from the English approach: The English courts [took] a broad view of the inherent power of the equity courts with regard to incompetents … the rule in these cases is that the chancellor has the power to deal with the estate of the incompetent in the same manner as the incompetent would if he had his faculties … the right to act for the incompetent in all cases has become recognised in this country as the doctrine of substituted judgment and is broad enough not only to cover property but also to cover all matters touching on the well-being of the ward. The doctrine has been recognised in American courts since 1844.
39
The psychiatrist gave strong evidence that if the sick brother died, it would have an ‘extremely traumatic effect’ on the incompetent donor. It was also thought that should the parents subsequently die, the donor would no longer have the ‘concerned, intimate communication so necessary to his stability and optimal functioning’.
40
The harvest was ordered on the grounds that the court was free to substitute consent, with a subtle emphasis on best interests: ‘Jerry [is] greatly dependant on Tommy, emotionally and psychologically, and his well-being would be jeopardised more severely by the loss of his brother than by the removal of a kidney’.
41
A few years later, a kidney transplant was required between identical twins in Hart v. Brown.
42
The Connecticut Superior Court explored the substituted judgement doctrine, stating that it had the equitable power to act on the donor’s behalf.
43
The court decided to substitute consent, after it was testified that Margaret Hart ‘desired to donate her kidney so that her sister may return to her’.
44
However, the court showed caution by completing a ‘close, independent and objective investigation of [the parents’] motivation and reasoning’ and decided that in the rare event that the doctrine was enforced, the ‘need must be urgent, the probabilities of success should be most favourable, and the duty must be clear’.
45
This stricter approach was tested only a few months later in Re Richardson.
46
The Court of Appeal of Louisiana were strongly influenced by the best interests of the donor, stating that ‘a minor [has a] right to be free in his person from bodily intrusion to the extent of loss of an organ unless such a loss be in the best interests of the minor’.
47
It was decided by the judges, in light of the lower success rate, the alternative of dialysis, the extra complications, the 11-year lifespan of the donation and the lack of urgency that the harvest could not be ordered on the grounds that it did not support the best interests of the patient: Surgical intrusion and loss of a kidney clearly would be against Roy’s best interest…neither [the] parents nor the courts can authorise surgical intervention for the purpose of donating one of his kidneys…[it must be] clearly established that the surgical intrusion is urgent, that there are no reasonable alternatives, and that the contingencies are minimal.
48
It was becoming clear that the best interests principle was underpinning the doctrine of substituted judgement in a strange merger, for example, if the interests of the donor were not met by a non-therapeutic harvest, the court would not substitute the judgement. In the next case of Re Pescinski,
49
the Supreme Court of Wisconsin separated and rejected both the doctrine of substituted judgement and the best interests principle on the grounds that there was ‘absolutely no evidence’ that the donation was of a benefit to the donor and the doctrine was ‘nothing more than an application of the maxim that equity will speak for one who cannot speak for himself.’
50
The court was of the opinion that it required statutory authority to approve the harvest and decided it could not find any: an incompetent particularly should have his own interests protected. Certainly no advantage should be taken of him. In the absence of real consent on his part, and in a situation where no benefit to him has been established, we fail to find any authority for the county court, or this court, to approve this operation.
51
Justice Day dissented on the grounds that a judgement could be substituted using the following five-part test: (i) the recipient will die without the transplant; (ii) reasonable steps were taken to find another source; (iii) there must be a close blood connection such as siblings; (iv) the court must be convinced that if competent, the donor would have consented and (v) the donor is in good health.
52
The next case, Little v. Little, adopted elements of the dissenting test above, but ironically used them to support the best interests principle.
53
The Texas court reviewed the previous case law and noted that substituted judgement was often underpinned by considerations of best interests: It is clear in transplant cases that courts, whether they use the term ‘substituted judgment’ or not, will consider the benefits to the donor as the basis for permitting an incompetent to donate an organ. Although in Strunk, the Kentucky court discussed the substituted judgment doctrine in some detail, the conclusion of the majority there was based on the benefits that the incompetent donor would derive rather than on the theory that the incompetent would have consented to the transplant if he were competent.
54
The Texas court ordered the harvest on the grounds that the best interests of the donor were met. The decisive factors included a close relationship between the siblings, an understanding of welfare, happiness in the donor, both parents consented, the dangers were small, the alternatives were investigated and the benefit to the sick sibling was significant: There is uncontradicted testimony relating to increased happiness. Studies of persons who have donated kidneys reveal resulting positive benefits such as heightened self-esteem, enhanced status in the family, renewed meaning in life, and other positive feelings including transcendental or peak experiences flowing from their gift of life to another.
55
The Texas court was not happy about the state of the law and restricted its approach to parent and sibling relationships, also calling for proper legislation. 56 The doctrine of substituted judgement was expressly rejected 5 years later in a bone marrow case named Re Doe. 57 The risks and benefits to the donor and recipient were weighed up (including the alternatives), but the determining factor in support of harvest was that the recipient was the sole family member involved in the care and placement of the donor. It was therefore in his best interests to donate. 58
The doctrine of substituted judgement was used in other areas of medicine in the United States, where it was honed into shape, namely to order blood transfusions in the face of parental objection,
59
the amputation of a leg
60
and the sterilization of an individual.
61
The doctrine was particularly useful in withdrawal of treatment cases. In the leading case of Re Longeway, for example, the doctrine was available to refuse medical treatment as long as the guardian could ‘attempt to establish, with as much accuracy as possible, what decision the patient would make if the patient were competent to do so’.
62
The court took the opportunity to lay down two ground rules to clarify the correct use of the doctrine: (i) the guardian was required to ‘determine if the patient had expressed explicit intent regarding this type of medical treatment prior to becoming incompetent’ and (ii) if this was not possible, ‘the patient’s personal value system must guide the [guardian]’, including philosophical, religious and moral views, life goals, values about the purpose of life and attitudes towards sickness, medical procedures and death.
63
The court deemed the best interests principle to be unsuitable in withdrawal cases because it ‘lets another make a determination of a patient’s quality of life, thereby undermining the foundation of self-determination and inviolability of the person upon which the right to refuse medical treatment stands’.
64
The doctrine of substituted judgement was strictly narrowed as a result of Longeway; it could only be applied to patients who had enjoyed previous competence, had already made the relevant decision, or had expressed a view about that kind of decision. The leading saviour sibling case of Curran v. Bosze emerged at this perfect time.
65
The Illinois Supreme Court had a difficult decision to make, that is, it could rule to test for compatibility under the doctrine of substituted judgement on the grounds that the twins would want to be tested (as Bosze contested, supported by Strunk, Hart and Little) or it could apply the principle of best interests and refuse the test on the grounds that there was no benefit (as Curran contested, supported by Richardson and Pescinski). The decision in Longeway was delivered by the exact same court only months previously, leaving the newly defined rules of substituted judgement fresh in the minds of the judges. Bosze had to discharge a heavy burden of proof to engage the doctrine, for example, he had to find clear and convincing evidence that the twins, if competent, would choose to be tested for compatibility. He could not.
66
The Illinois Supreme Court agreed with Nancy Curran that the doctrine of substituted judgement was inapplicable to minors: It is not in the best interest of either Allison or James to undergo the proposed bone marrow harvesting procedure… it is not possible to discover the child’s likely treatment/non-treatment preferences by examining the child’s philosophical, religious and moral views, life goals, values about the purpose of life and the way it should be lived, and attitudes toward sickness, medical procedures, suffering and death … at the age of three and a half, it is very difficult if not impossible to predict what a specific individual will do in a specific circumstance at a specific point of time in the future.
67
The court also noted, in response to considerations of best interests underpinning every previous legal decision, that a clear best interests test was required for any subsequent incompetent donation cases. The new (and current) test reads as follows: (i) the consenting parent must understand the risks and benefits of the procedure; (ii) there must be emotional support from the person with parental responsibility and (iii) there must be an existing close relationship between the donor and the sick child, per Justice Calvo: the psychological benefit is grounded firmly in the fact that the donor and recipient are known to each other as family. Only where there is an existing relationship between a healthy child and his or her ill sister or brother may a psychological benefit to the child from donating bone marrow to a sibling realistically be found to exist.
68
The expert testimony for Curran stated that the twins had only met Jean Pierre twice and did not know him as their brother. The psychological benefit to the twins (the only kind of benefit that could be gleaned from such a procedure) was therefore minimal, difficult to predict and fairly insignificant. There was simply no existing close relationship between the donors and the sick sibling to satisfy the best interests test. 69
The doctrine of substituted judgement was removed from child donors with the passing of Curran v. Bosze, but it was made clear that to invoke the doctrine the patient must have enjoyed previous competence and their former views on the matter at hand must be convincingly shown. In agreement, the UK and the US courts do not allow a parent, a court or any other authoritative body (such as the HTA) to substitute the judgement of a child for the purposes of harvest. This is surely correct, because a child cannot form a competent opinion, has no life experience and cannot maturely weigh the risks. The typical precursors to parental consent for a bone marrow transplant, therefore, such as ‘she would want to do it’ or ‘she would feel good in future’ cannot be used to scaffold a required psychological benefit. A speculative benefit that is even remotely framed in the perspective of the child – such as ‘she would enjoy a sister to play with’ – is ruled out because it substitutes a judgement that does not exist. The best interests test reigns supreme, that is, there must be an actual connection between the saviour and the sick, and it must be strong enough to foster a psychological benefit in the present.
The best interests test in Curran v. Bosze travelled back over the Atlantic to underpin our very own bone marrow decision in Re Y (Mental Patient: Bone Marrow Donation). 70 It was not applied altogether correctly (examined below), but it does confirm that an incompetent donor must experience a psychological benefit to ensure his/her best interests. Herein lies the problem. A saviour sibling created specifically for harvest under the 1990 Act cannot glean any benefit from a bone marrow donation. There is no altruism, no consent, no relationship and no understanding in an infant or a toddler. The only avenue open to the parents to justify the harvest in common law is to substitute their own speculative psychological benefit into the child.
Manipulating the doctrine: Saviour siblings and substituted judgement
In Re Y (Mental Patient: Bone Marrow Donation), an incompetent adult was a tissue match to her older sister.
71
Justice Connell stated the legal issue clearly: the taking of blood tests and the harvesting of bone marrow from the [donor], who is incapable of giving informed consent, would amount to assaults upon the [donor] and would therefore be illegal unless shown to be in the best interests of the [donor] and therefore lawful.
72
The facts in Re Y did not support a bone marrow harvest on an incompetent adult patient because there was no clear benefit to the donor. Connell J was forced to turn to case law in similar jurisdictions to validate the procedure, and he stepped upon the three-part test in Curran v. Bosze. It was created in the context of child donors but this did not matter – it was the only relevant authority to be found: (i) the consenting parent must understand the risks and benefits of the procedure, (ii) there must be emotional support from the person with parental responsibility, and (iii) there must be an existing close relationship between the donor and the sick child.
73
Connell J preferred the third prong of the test and validated the harvest in Re Y on the following grounds: In this situation, the [donor] would clearly be harmed by the reduction in or loss of contact with her mother. Accordingly, it is to the benefit of the [donor] that she should act as donor to her sister, because in this way her positive relationship with her mother is most likely to be prolonged. Further, if the transplant occurs, this is likely to improve the [donor’s] relationship with her mother who in her heart clearly wishes it to take place and also to improve her relationship with the plaintiff who will be eternally grateful to her … it is relevant to ask the question, why subject the [donor] to this process? To this the answer, in my judgment…is because it is to her emotional, psychological and social benefit.
74
Connell J was of the opinion that the harvest was in the best interests of the donor, but this decision was out of step with Curran v. Bosze in two ways. Firstly, like the twins in Curran v. Bosze, the donor in Re Y could not derive a psychological benefit from the bone marrow donation because she was not connected to the recipient. Connell J admitted this in his judgement: She is severely mentally and physically handicapped … it was apparent that [she] did not understand what was being said to her. Likewise, she did not understand what was being said when told that her older sister is very unwell. The [donor] understands her own basic needs but cannot understand the needs of others … she did not understand what was being said when told that her older sister is very unwell … it is not possible accurately to describe the relationship between the plaintiff and the [donor] as particularly strong.
75
Even more strangely, he also admitted that the donor did not even know who her mother was, ‘her mother holds a special place in the [donor’s] world even if the [donor] does not appreciate that this lady is in fact her mother’. 76 It was made clear in Curran v. Bosze that a solid relationship must be present between the donor and the donee for a tangible psychological benefit to be evidenced in sibling donation cases, 77 but Connell J explicitly turned away from this criteria by framing the main benefit around a third party (the mother) who was unknown to the donor.
Secondly, the heart of the matter in Curran v. Bosze was the best interests of the twins, but the focus in Re Y appeared to be on the plight of other family members: [The patient’s] most regular visitor and the family member with whom she has the closest relationship is undoubtedly her mother. More recently, the mother has had a coronary bypass operation and at the present time she suffers from angina and gets tired very easily. It is clear that her health is precarious and her condition is significantly exacerbated by her anxieties concerning the health of the [sick sister]. If the plaintiff dies, this is bound to have an adverse effect upon her mother who already suffers from significant ill-health. One lay witness took the view that this event would prove fatal to the mother.
78
Connell J was clearly forced to expand the test in Curran v. Bosze to include third parties because the facts in Re Y did not lend themselves to harvest. This is the crux of the interfamilial principle, that is, the needs of third parties are incorporated into the best interests test to scaffold a ‘general’ psychological benefit in a case where none exists. It would be highly unordinary for the courts to validate a non-therapeutic procedure on a child by throwing the best interests of the parent, the sick and the saviour into one big pot, but as a result of Re Y, the parents of saviour siblings can now place their own aspirations on the table – phrases such as ‘they would support each other throughout life’ and ‘she would love to save her brother’ – and could find that they are adopted over the best interests of the child. This is a modified version of the doctrine of substituted judgement, that is, the subjective views of the parents are substituted into the child. There is no other way to validate this kind of harvest in law.
The decision in Re Y confirms that an incompetent donor can be harvested for bone marrow if a psychological benefit can be evidenced and grievances of third parties can be used to underpin this. The case was decided in the context of incompetent adults and Connell J stated that it would not be useful in ‘more intrusive’ cases such as organ donation (at p. 116), but the decision appears to have influenced the HTA. It has published a Code of Practice on bone marrow donations from children and it states the following regarding consent: Paragraph 82: A person with parental responsibility can consent to storage and use of bone marrow for transplantation on behalf of the child, if the donation is assessed as being in the child’s overall best interests, taking into account not only the medical but also emotional, psychological and social aspects of the donation, as well as the risks.
79
The phrases ‘overall best interests’ and ‘emotional, psychological and social aspects’ are a clear insertion of the interfamilial principle in Re Y: A non-therapeutic donation would never ordinarily be in the best interests of a child unless the plight of the family was included in the test. The Code of Practice also makes it clear that the High Court is only required to validate the harvest if there is a disagreement: Paragraph 37: In cases where a child is not competent to consent to donation themselves and there is a dispute between those with parental responsibility, or between them and the clinicians looking after the child, or there is a doubt as to best interests of the child, the court should be asked to rule in advance. The court ruling should be in place before referral to the HTA.
80
The decisions to harvest marrow from a child, therefore, is taken behind closed doors. A decision can be made on the child’s behalf by a person with parental responsibility. 81 The consent of only one parent is required. 82 There will be interviews with an accredited assessor (AA), the donor (or the parents of the donor) and the recipient, and then it will be up to the HTA to decide whether the harvest should go ahead. 83 The substituted judgement occurs here. The distressed parents – knowing that there is no therapeutic benefit to the saviour yet aware of the fate of the sick – will present a collection of speculative familial benefits to the HTA (i.e. a sense of altruism, ensuring future relationships, having a sibling to play with, experiencing closer family connections, escaping the grief of death and the interfamilial principle) to help sway the decision in favour of harvest. It is highly unlikely, in this balance of benefits and burdens, that the harm to the saviour will outweigh the risks to the sick, especially if the parents agree on harvest. It should also be remembered that since Quintavalle, the parents may have created the donor child specifically for the purpose of harvest, making their desire to harvest overwhelmingly strong.
The Code of Practice does confirm that if a clinician has serious concerns, the child will become a ward of court: Paragraph 109: If the court is asked to consider the matter, the welfare of the prospective donor child will be the court’s paramount consideration and not the welfare of the recipient. The “welfare checklist” which is set out in the Children Act 1989 will be considered by the court in determining the application.
84
It is deeply regrettable that only in the event of a disagreement will the objective jurisdiction of the High Court be called upon to defend the best interests of the saviour child.
There is plenty of support for the interfamilial principle in the literature. The fiercest supporter by far is Lainie Friedman Ross, who believes that the interests of the donor child can be overridden to allow the parents to instil good traits in their children: To hold parents to a best interest of the child standard is incompatible with the family as an intimate group with goals that do not maximise the best interest of each child member…this threatens both the parents’ interest in raising a family according to their own vision of the good life and the children’s interest in having sovereign parents. [The donor’s] persistent dissent can be overridden because her parents can justify treating her as the type of person who will come to accept good samaritanism and family obligations as integral to her own wellbeing. Parents can override their child’s present identity, goals and interests if they conflict with the future person they want their child to become.
85
This view looks remarkably like forced altruism in the form of a substituted judgement. Jansen suggests that it is favourable instead to bind the interests of both parties: when an intimate attachment exists between a child organ donor and a prospective recipient, then the wellbeing of the former is bound up with the latter. This makes it possible for the organ donation to serve the best interests of both the donor and the recipient.
86
It cannot be beneficial for the saviour to have her interests bound up in the plight of the sick because they have completely separate interests, that is, the saviour needs protection from harm, whereas the sick wishes to inflict harm. However, this idea was spotted closer to home in the PTT Report (2004) by the HFEA: ‘if a medical procedure, such as a bone marrow transplant, would save the life of a sibling, it is likely to be in the best interests of the child, since to lose a sibling is psychologically damaging’. 87
A direct application of the interfamilial principle can be found in one of the oldest saviour sibling cases from the United States named Masden v. Harrison.
88
The procedure was validated on the grounds that the death of the sick brother would have a negative psychological impact on the donor brother: I am satisfied from the testimony of the psychiatrist that grave emotional impact may be visited upon Leonard if the defendants refuse to perform this operation and Leon should die, as apparently he will … such emotional disturbance could well effect the health and physical wellbeing of Leonard for the remainder of his life. I therefore find that this operation is necessary for the continued good health and future wellbeing of Leonard and that in performing the operation the defendants are conferring a benefit upon Leonard as well as Leon.
89
This approach is understandable. Crouch and Elliott lead the way in a list of speculative benefits available to parents when the moment comes to consent using the interfamilial principle: First, the donation can have an instrumental value to the donor: in donating, the donor may save the life of a sibling and will therefore have a sibling to grow up with and to share a life with, each of which brings with it certain identifiable social and emotional benefits to the donor. Second, ceteris paribus, growing up in a household unaffected by the tragic loss of a sibling or child is possibly more conductive to psychological stability and general mental health than growing up in a family that has been struck by loss. Third, even if the donation is ultimately unsuccessful, the donor may receive some comfort from the recognition that everything possible was done to help the sibling, and that the role played in the medical treatment was crucial, even if unsuccessful.
90
Sheldon and Wilkinson discuss additional benefits that are particular to tissue-matched saviour siblings under the 1990 Act: It could surely be argued that [a selected sibling] would benefit from [the existing child’s] company and may well derive pleasure from knowing that she has saved [his] life. In contrast, imagine the psychological impact on [a randomly selected sibling], born into a bereaved family, later to discover that she was a huge disappointment to her parents because of her inability to save [the existing child’s] life (or, more emotively, that her tissue incompatibility was the cause of his death). Is it not possible that the new child’s capacity to save its sibling’s life is something which would endear it greatly to its parents?
91
These are emotive arguments, but there are three insurmountable barriers facing parents when proposing these interfamilial benefits as justification to harvest a child: (i) they are completely speculative, (ii) a young child does not understand the concept of altruism and (iii) the lack of knowledge and understanding on the part of the donor renders the benefits defunct. Ladd suggests that because altruism is an adult concept, the saviour must consent as an adult: siblings do not owe each other anything, and this is why organ donation, if it is to take place at all, must be voluntary on the child’s part … child assent is required because parental consent without child assent would amount to requiring of a child a degree of altruism that we do not ever require of adults.
92
Altruism is clearly not available as a psychological benefit to a young saviour sibling because its very nature requires understanding, capacity and voluntariness. The parents cannot substitute it. Altruism was discussed in Curran v. Bosze, and it was believed that it could be as much as 20 years before the psychological benefits could be measured. 93 It was also suggested that altruism should be present at the time of the act as a motivating factor – not used at a future point to retrospectively justify an action – and motivation and intention could not be supplied after the act. 94 It can be concluded that a saviour sibling specifically created for harvest under schedule 2 paragraph 1ZA(1)(d) of the HFE Act 1990 cannot be harvested for bone marrow in law because there is no physical or psychological benefit at the time of harvest. The HTA, however, has been exercising its powers behind closed doors to authorize harvesting procedures on minors, and its own statistics show the following 95 :
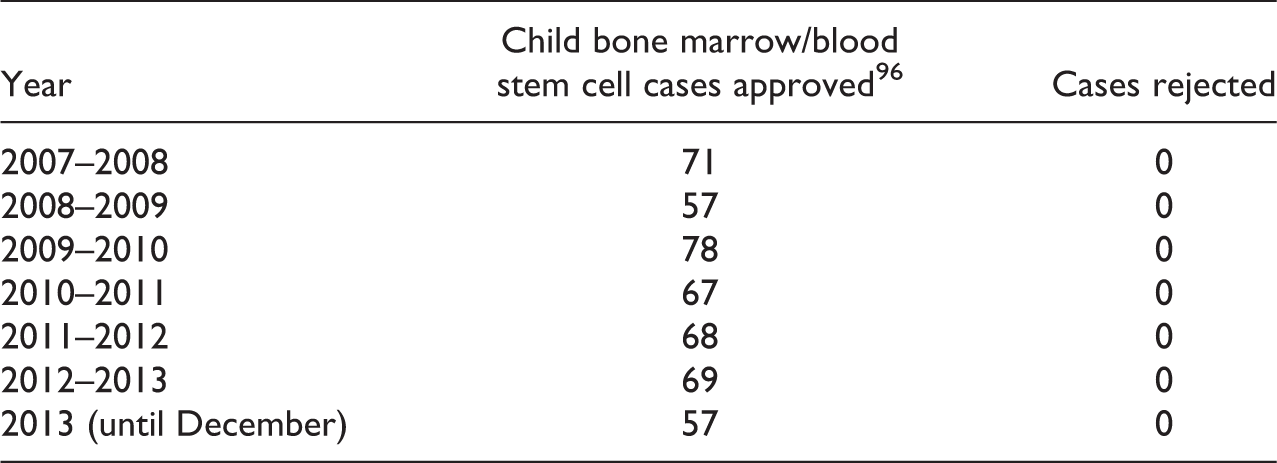
The most alarming feature of the statistics above is the permanent zero in the ‘cases rejected’ column. The substituted judgement doctrine – using a combination of speculative altruism and the interfamilial principle – is clearly working for the parents. A saviour sibling has not yet been warded in a high-profile case, but should it occur in the near future, this evidence suggests that the judges are very likely to be persuaded by the emotive pleas of the parents in a modified substituted judgement, leading to our very own Re Y for minors.
Conclusion
The HTA does not adhere to the common law, which clearly states that an objective standard must be met when determining the best interests of a child. The need for an objective test is only increased when the parents are seeking to serve their own interests. A speculative emotional or social benefit, substituted in the form of consent by the parents, should not be acceptable. The HTA has ensured that safeguards are in place in their Code of Practice to ensure that the saviour sibling is not exploited. For example, a senior person in the bone marrow team must be satisfied that an adult donor cannot be found.
97
There must also be no signs of coercion or reward: Paragraph 89: Children will also often experience feelings of responsibility or duty when faced with the prospect of being a donor. In some circumstances children may experience feelings of guilt or a fear that love may be withdrawn if they do not proceed with donation. In trying to determine whether a child has been coerced into donating, it is important for the [Accredited Assessor] to discuss any feelings of pressure or duty the child holds and explore their origins. Paragraph 90: If there is any doubt about whether the child is donating because of the promise of a reward, or the child is being coerced to donate through any other means, the AA should seek guidance from other AA’s and raise their concerns within their report to the HTA.
These safeguards are of little use to babies or toddlers who are specifically created for harvest using PGD/PTT. A baby cannot be coerced or induced by a reward and a toddler will have no understanding of the procedure. The parents are perfectly positioned to strongly influence the bone marrow team on what the child ‘would do’ if she was competent. Lord Hoffmann in Quintavalle assumed that once born, the saviour sibling would be able to rely on the law for protection: ‘the [HFE] authority is in my opinion entitled to assume that a child conceived pursuant to its licence will, after birth, receive the full protection of the law’. 98 There was no further elaboration on this point, but if he was referring to wardship, it is clearly not invoked. It does not help that our only authority on sibling donation –Re Y (Mental Patient: Bone Marrow Donation) – adopted the interfamilial principle and merged the interests of the mother (who was frail) and the sick sibling (who had no relationship to the donor) with the donor to ensure that a psychological benefit was evidenced. Re Y concerned an adult patient, so its decision should not have been incorporated into the HTA Code of Practice on bone marrow donations from children.
The doctrine of substituted judgement is the only avenue parents have left to fulfil the psychological benefit requirement under common law, but it has been revealed that the lack of knowledge and understanding on the part of the child renders any psychological benefit defunct. The current process, to put it bluntly, allows the best interests of the child to be trumped by the desires of the parents – the very threat that the jurisdiction of wardship was created to avoid.
The conundrum for distressed parents is clear. A saviour sibling is a freshly born baby (or a toddler if the sick sibling can wait that long) with no emotional connection to the family and no desire to donate. There is no benefit to be gained from a non-therapeutic procedure except for speculative benefits in a substituted judgement. It is proposed that to authorize a non-therapeutic procedure on a young child ‘in-house’ using only the consent of the parents in the form of a substituted judgement with no court involvement is breaking the law – just because the Human Fertilisation and Embryology Act 1990 made the creation of saviour siblings legal under schedule 2, para. 1ZA(1)(d), does not mean they can be legally harvested. Their Lordships in Quintavalle failed to identify this issue when bringing the practice into law.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.