
Abstract
Objectives
Self-sampling for human papillomavirus (HPV) is being considered as an additional cervical screening method in Ireland. As sample takers play a central role in cervical screening and their support would be essential to the successful delivery of any HPV self-sampling programme, this survey aimed to assess sample takers’ views on HPV self-sampling.
Methods
An anonymous, online survey of HPV sample takers registered with CervicalCheck was conducted. Survey questions focused on sample takers’ views on the introduction of HPV self-sampling in Ireland, advantages and disadvantages for them and the role sample takers might play in delivering self-sampling.
Results
Of the 200 sample takers who completed the survey, 175 (87.5%) were nurses and the remainder doctors. Two-thirds (67%, 95% confidence interval: 60.5–73.5%; n = 134) supported introducing HPV self-sampling, 9% (5.0–13.0%; n = 18) did not, and 24% (18.1–29.9%; n = 48) were unsure. The reasons respondents supported introducing HPV self-sampling included a potential to increase screening uptake and provide a better experience for participants. Those opposed were concerned self-sampling would represent a missed opportunity for clinical examination of the cervix, to counsel patients about screening, and discuss other health concerns, while a minority reported concerns about the accuracy of self-sampled tests. No clear differences in views were observed by professional role.
Conclusions
Most respondents supported HPV self-sampling as an additional cervical screening method, but some were concerned about the potential reduction in important clinical encounters and accuracy of self-sampled tests. The benefits and limitations of HPV self-sampling should be carefully considered before introducing any self-sampling programme in Ireland.
Introduction
Self-sampling for human papillomavirus (HPV) is an alternative method to clinician-collected HPV testing for cervical cancer screening and is currently being considered for introduction as an additional cervical screening method in Ireland. 1 HPV self-sampling has been introduced in a number of countries worldwide and the World Health Organization (WHO) recommends it as an additional option to improve cervical cancer screening coverage.2–4
There are potential benefits of implementing HPV self-sampling in a cervical screening programme. In particular, these include the potential to increase the uptake of cervical screening and to reach individuals who delay or drop out of cervical screening.5,6 International evidence has shown high acceptability of HPV self-sampling among screening participants.7–9 Reasons for this high acceptability may include less pain or physical discomfort associated with HPV self-sampling compared to clinician-collected samples, ease of use, convenience, ability to perform the test in private and less embarrassment or anxiety.2,9 There are clear limitations associated with HPV self-sampling, however, and these include the loss of opportunity for healthcare professionals to counsel participants about the benefits, risks and limitations of cervical screening, the risk of participants not attending follow-up after a positive self-sampled HPV test, and potentially inferior sensitivity of self-sampled HPV tests compared to clinician-collected HPV tests.10–14
It is important to assess the views of healthcare professionals involved in performing cervical screening tests, hereafter referred to as sample takers, on HPV self-sampling. Sample takers represent a key stakeholder group who play an integral role in screening; their support would be essential for the successful delivery of any HPV self-sampling programme and negative attitudes could lead to issues with implementation and adherence. 15 Additionally, sample takers may have an important role in promotion of HPV self-sampling to their patients and may be able to identify potential facilitators and barriers to the introduction and implementation of HPV self-sampling.
The aim of this study was to assess HPV sample takers’ views on the possible introduction of HPV self-sampling in Ireland, and to identify what they perceived to be the advantages, disadvantages, and challenges associated with implementing it.
Methods
Setting
This study was conducted in Ireland, where CervicalCheck, the national population-based cervical cancer screening programme, has been in operation since 2008. Women and people with a cervix aged 25–65 years are eligible for free HPV screening tests every 3 or 5 years. Samples positive for HPV are triaged by reflex cytology; participants with abnormal cytology are directly referred for colposcopy and participants with normal cytology are referred for repeat HPV screening after 12 months. 16 Participants in the programme can arrange an appointment to have a free test with a CervicalCheck registered sample taker of their choice. Sample takers are practice nurses, midwives, general practitioners (GPs), GP registrars or other types of doctors. At the time when the study was conducted, 61% of all sample takers registered with CervicalCheck were nurses or midwives, 94% were female, 31% were based in Munster, one of the four provinces of Ireland, with the remainder being split between Dublin (25%), the rest of Leinster (23%), and Connaught and Ulster (21%). At the time this study was conducted, decisions about who would be offered HPV self-sampling in the future in Ireland had not been made by decision-makers within the health service or the government's health department. There was no preferred model of delivery being proposed by any of the key stakeholders involved in cervical screening. Indeed, the concept of HPV self-sampling was novel to many stakeholders involved in delivering cervical screening prior to this time.
Survey design
An anonymous, online, cross-sectional survey of HPV sample takers registered with CervicalCheck was conducted in 2023. The survey instrument was informed by a literature review of health professionals’ attitudes towards HPV self-sampling, as well as discussions with key stakeholders within the National Screening Service (NSS), the overarching national population screening organisation.
As the concept of HPV self-sampling was novel to many cervical screening stakeholders when the survey was being conducted, survey respondents were given information at the beginning of the survey about how HPV self-sampling tests work and their effectiveness. Other than HPV self-sampling being framed as an ‘additional test’ in the survey questions – implying that it would not fully replace standard clinician-collected HPV testing – respondents were not provided with any information on how it might be implemented in practice, at whom it might be targeted, how it would supplement clinician-collected HPV testing, and in what scenarios it might replace clinician-collected HPV testing.
The survey consisted of 18 questions in total (16 closed and two open). Questions focused on sample takers’ views on whether HPV self-sampling should be introduced in Ireland, the perceived advantages and disadvantages of HPV self-sampling for sample takers, and the potential challenges associated with implementing it in the Irish context. Other questions focused on the location in which self-sampling should be performed and the role sample takers should play in a HPV self-sampling programme. Demographic information was also collected, specifically age group, working location and professional role. Information on respondents’ sex was not collected, as it was judged that this could have made respondents identifiable. All questions were mandatory.
The survey was pre-tested on two individuals who met the eligibility criteria to participate in the final survey. Feedback provided information to further refine the survey. The survey was self-administered via the Smart Survey platform (https://www.smartsurvey.co.uk/) and took approximately ten minutes to complete (survey available in the online supplemental materials).
Survey dissemination
The survey was disseminated via email in July 2023 to all sample takers who were registered with CervicalCheck and had previously indicated a willingness to be contacted by the NSS (n = 1549). The survey was promoted in the June 2023 edition of the sample takers’ Cervical Screening Newsletter, a quarterly newsletter produced by CervicalCheck, and at an educational webinar run by CervicalCheck for sample takers. The survey was available to complete online between 10th and 26th July 2023.
Data analysis
Responses were analysed in Stata 17 (StataCorp. 2021, College Station, TX, USA: StataCorp LLC). Counts, proportions and their 95% confidence intervals (CIs) were calculated to describe the quantitative data. As all questions were mandatory, missing data did not represent an issue during analysis. In addition to being asked whether they thought HPV self-sampling should be introduced or not, respondents could provide free-text responses to explain their answers. These free-text responses were analysed using Braun and Clarke's thematic analysis framework to identify themes and subthemes. 17 A subgroup analysis was performed whereby responses were analysed according to professional role (nurses and midwives vs doctors), as previous research has indicated that CervicalCheck sample takers’ behaviours and views on cervical screening may vary according to their professional role. 18 Chi-squared tests were performed to compare responses between subgroups. All p-values reported are two-sided and statistical significance of p < 0.05 was assumed throughout.
Consent to participate and ethical considerations
Prior to survey participation respondents were provided with information outlining the purpose of the survey and the role of the NSS in conducting it. They were made aware that the survey was anonymous, of their right to not participate, and their right to withdraw from the survey at any point. They had to provide their written consent to participate. Ethics approval for the survey was granted by the Royal College of Physicians of Ireland's Research Ethics Committee in June 2023 (RCPI RECSAF 189) and conformed to the principles embodied in the Declaration of Helsinki.
Results
Characteristics of survey respondents
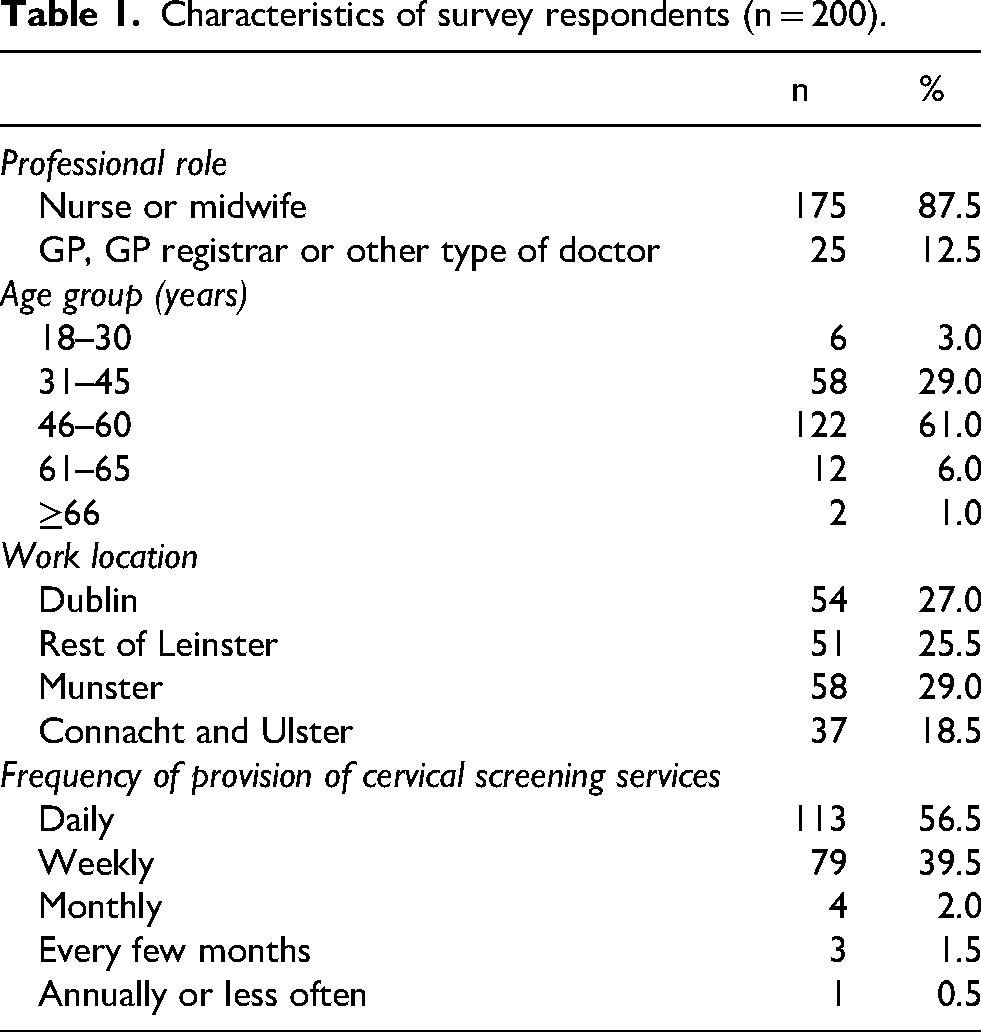
Of the 1549 sample takers invited by email to participate in the survey, 200 (12.9%) completed it. Most respondents were nurses or midwives (87.5%, n = 175). The remainder were GPs, GP registrars or other types of doctors (12.5%, n = 25; Table 1). Sixty-one percent (n = 122) of respondents were aged 46–60 years and 96% (n = 192) performed sample taking for cervical screening on a daily or weekly basis. Respondents’ work locations encompassed all regions of Ireland.
Characteristics of survey respondents (n = 200).
Views on introducing HPV self-sampling
Two thirds of respondents (67%, 95% CI: 60.5–73.5%; n = 134) supported introducing HPV self-sampling as an additional cervical screening method in Ireland, while 9% (5.0–13.0%; n = 18) did not, and 24% (18.1–29.9%; n = 48) were unsure. From the analysis of the free-text responses in which respondents could expand on their views, four key themes were generated.
Theme 1: The potential for HPV self-sampling to improve cervical screening uptake
Many respondents were in favour of introducing HPV self-sampling due to its potential to increase screening uptake. Views on why HPV self-sampling could increase screening uptake included its ability to surmount the logistical barriers to screening. One respondent stated that ‘I feel it may increase uptake for people who find it difficult to take time for the screening in surgery’, while another stated ‘It may increase the uptake as clients don’t have to schedule an appointment for GP or take time off work’. Some respondents expressed the view that HPV self-sampling could increase screening uptake as it addressed important psychological barriers, such as fear, embarrassment, and self-consciousness regarding screening. As one respondent summarised ‘It would encourage better uptake from people who are afraid to come for screening. Better than not being screened at all’.
Theme 2: Better participant experience associated with HPV self-sampling
Among the respondents who favoured the introduction of HPV self-sampling in Ireland, many highlighted its potential to provide a better experience for participants than clinician-collected HPV tests. Some respondents saw HPV self-sampling's lack of invasiveness as its key benefit, which could provide screening participants with a superior experience to a HPV test collected by a clinician. One respondent stated ‘Some women find smear tests unbearable. If HPV is negative there is no need for a smear’, while others noted that the reduction in pain and discomfort associated with a self-sampled test could be particularly beneficial to post-menopausal women: ‘An initial swab would be easier for the older post-menopausal women who often find the speculum uncomfortable’. Some respondents remarked that HPV self-sampling may be perceived by participants as less daunting than a clinician-collected HPV test, as it would not only allow participants to avoid a pelvic exam, but many women and people with a cervix have become accustomed to self-testing for sexually transmitted infections (STIs). As one respondent commented ‘a lot of women are more comfortable taking HVS [high vaginal swabs] themselves for other testing and I think this would be the same’.
Theme 3: Missed opportunities arising from the potential reduction in clinical encounters
Respondents opposed to introducing HPV self-sampling identified the potential missed opportunities to talk to and examine women and people with a cervix as a key potential drawback. Some expressed concern that HPV self-sampling could represent a missed opportunity to counsel participants about cervical screening and discuss other health concerns, with one respondent stating ‘Woman [sic] will miss out on counselling and the opportunity to discuss so many issues that regularly turn up with the intimacy that's involved with this consultation’. Another respondent highlighted the specific women's health issues that would not be discussed with screening participants if home-based self-sampling were introduced, by saying ‘… we very often, actually in almost all our patients, will provide the opportunity for them to discuss contraception, HRT [Hormone Replacement Therapy], STI testing, discloses [sic] of sexual assault, domestic violence’. Indeed, as one respondent concisely summarised ‘… [CervicalCheck] is an excellent service that provides women the opportunity to ask questions, be sign posted to other services, safe guarding, infection detection etc. CervicalCheck has been more than just a “HPV test”’. Others articulated concerns that HPV self-sampling would not allow the opportunity to perform a clinical assessment of the cervix which was seen as an important aspect of the clinician-collected HPV exam. One respondent highlighted that benign cervical pathology, such as polyps and Nabothian cysts, would not be detected. Another respondent succinctly stated ‘Self sampling means nobody visualises the cervix’.
Theme 4: Mistrust in the accuracy of self-sampled HPV tests
A minority of respondents who opposed the introduction of HPV self-sampling questioned the accuracy of self-sampled HPV tests. Some respondents conveyed unease about participants being able to perform a test correctly, potentially leading to inaccurate and false negative results. Indeed, one respondent concluded ‘I'm worried about accuracy of results. We’ve had hours of training to take a sample and they will have none … I wouldn’t trust all my patients to do this test’. Others expressed concerns that participants themselves would be sceptical of results from self-sampled HPV tests, with one respondent saying their patients would ‘not have faith in their ability to screen’ themselves and another remarking that ‘many patients would prefer the traditional smear system as they would be dubious about the accuracy of a self taking sample’.
Perceived advantages and disadvantages for sample takers
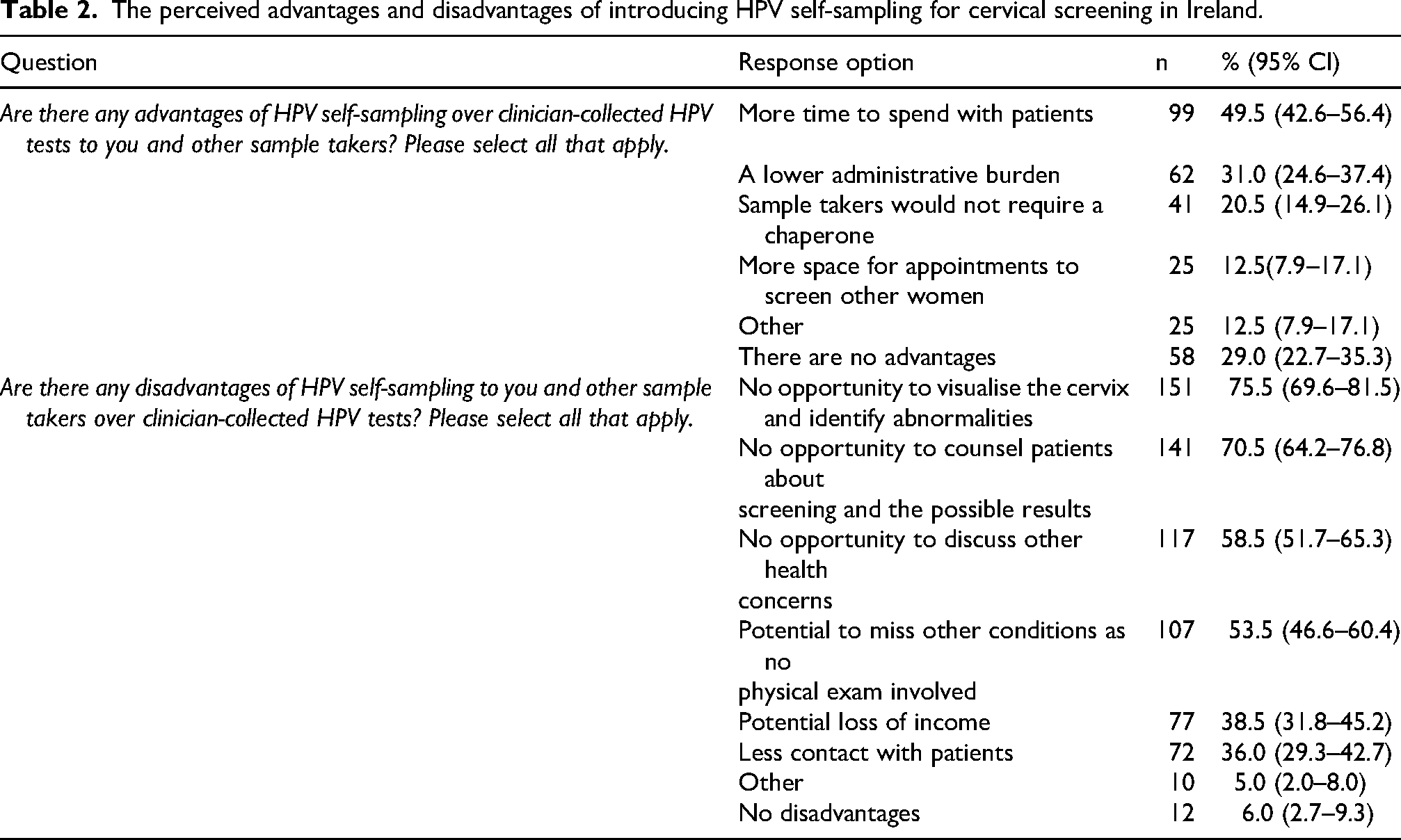
With respect to the perceived advantages for sample takers of introducing HPV self-sampling, respondents thought it would allow them more time with patients attending their services for non-screening reasons (49.5%, 42.6–56.4%; n = 99) and would result in a lower administrative burden (31%, 24.6–37.4%; n = 62) (Table 2). As for perceived disadvantages, respondents thought not having the opportunity to visualise the cervix (75.5%, 69.6–81.5%; n = 151), counsel participants about cervical screening (70.5%, 64.2–76.8%; n = 141) or discuss other health concerns (58.5%, 51.7–65.3%; n = 117), and potentially missing other conditions due to a lack of physical examination (53.5%, 46.6–60.4%; n = 107) were key concerns.
The perceived advantages and disadvantages of introducing HPV self-sampling for cervical screening in Ireland.
Views on the delivery of HPV self-sampling
Most respondents (72.5%, n = 145) thought HPV self-sampling should be performed at home (Table 3). Almost half (49.5%, 42.6–56.4%; n = 99) thought HPV self-sampling kits should be sent directly from CervicalCheck to participants to perform HPV self-sampling at home. A smaller proportion thought HPV self-sampling should be performed at home, but with involvement from participants’ GPs, either through a virtual appointment explaining how to use the self-sampling device (16.5%, 11.4–21.6%; n = 33), or by asking participants to collect HPV self-sampling kits from their local GP (6.5%, 3.1–9.9%; n = 13). The reasons given for a preference for performing HPV self-sampling at home included more convenience and privacy for participants, as well as participant preference for this. Among respondents who thought HPV self-sampling should occur in a GP practice, the primary reasons given for this choice were that it could provide sample takers with the opportunity to give instructions on self-sampling and counsel participants, and it could give sample takers more confidence that the self-sampled test would be performed correctly.
Respondents’ views on the delivery of HPV self-sampling for cervical screening in Ireland.
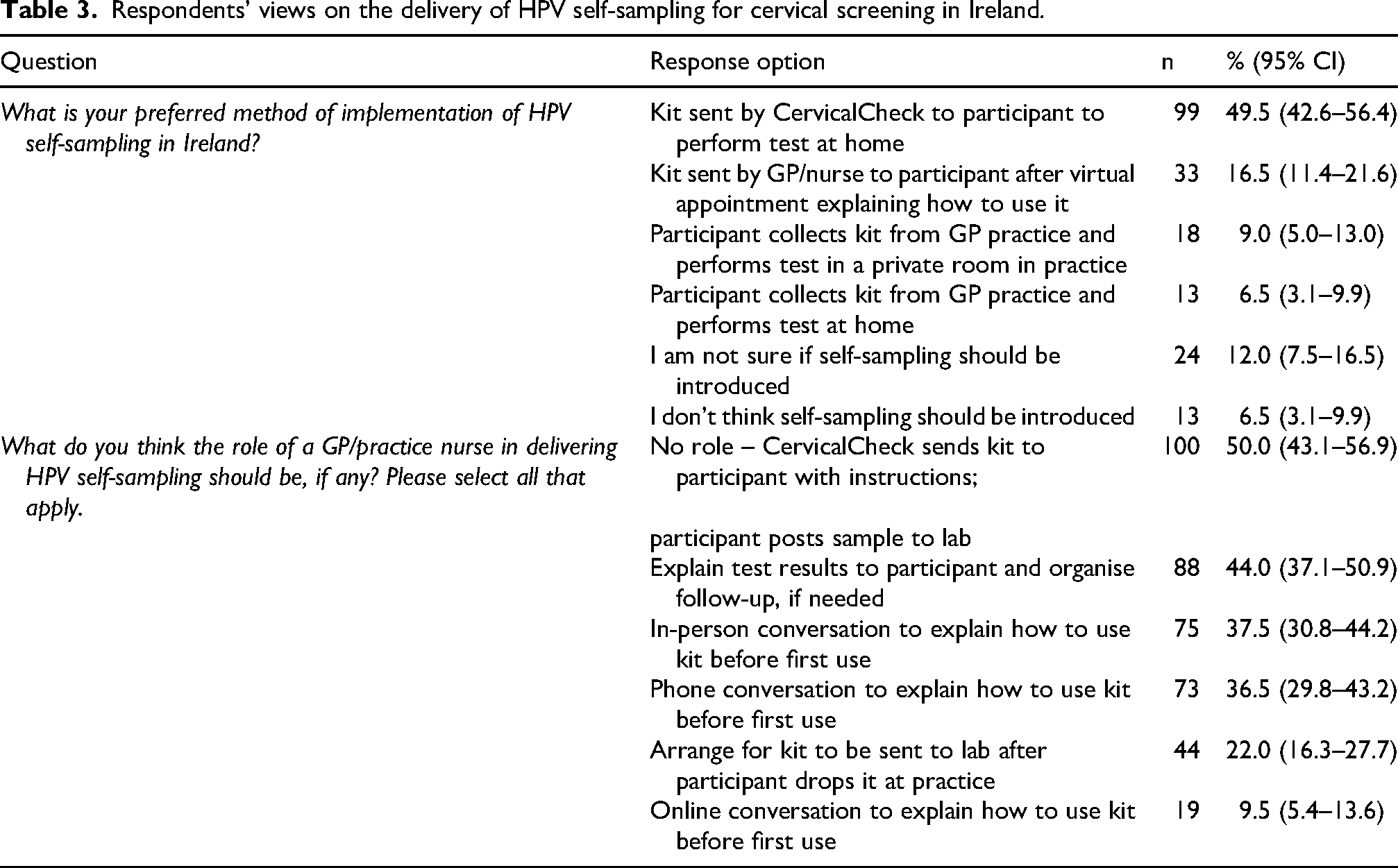
Half of all respondents (50%, 43.1–56.9%; n = 100) thought sample takers should play no role in delivering a HPV self-sampling programme. Half of respondents thought sample takers should be involved in the process, be it through explaining to participants how to use self-sampling devices in person (37.5%, 30.8–44.2%; n = 75), over the phone (36.5%, 29.8–43.2%; n = 73) or online (9.5%, 5.4–13.6%; n = 19), or explaining test results to participants and organising follow-up, if required (44%, 37.1–50.9%; n = 88).
Analysis of responses according to professional role
No clear differences in views were observed by professional role. While doctors and nurses held slightly different opinions on HPV self-sampling, most differences were not statistically significant (Supplemental Table 1). A smaller proportion of nurses and midwives than doctors thought HPV self-sampling should be introduced (65.8% vs. 76.0%, p = 0.57), more nurses and midwives thought HPV self-sampling should take place in participants’ homes (73.1% vs. 68%, p = 0.1), while fewer nurses and midwives thought sample takers should not be involved in delivering a HPV self-sampling programme (49.1% vs. 56%, p = 0.52).
Discussion
In this cross-sectional survey that aimed to assess sample takers’ views on HPV self-sampling, two thirds of respondents supported its introduction primarily due to its potential to increase screening uptake and provide screening participants with a less painful and less daunting screening experience. The minority of respondents who opposed the introduction of HPV self-sampling expressed concerns that it could represent a reduction in important clinical encounters with women and people with a cervix during which they could counsel them about screening, physically examine them, visualise the cervix, discuss other related health concerns and signpost them to other services. Some were also concerned that self-sampled HPV tests may be less accurate than clinician-collected tests. Almost half of respondents identified the main benefit to sample takers of introducing HPV self-sampling as having more time to spend with other non-screening patients attending their services. While there was agreement among respondents on where HPV self-sampling should take place – with the majority believing it should be performed in participants’ homes – respondents were evenly divided on whether they should be involved in the delivery of HPV self-sampling. Finally, there were differences in the responses of doctors compared with nurses and midwives, with doctors showing stronger support for introducing HPV self-sampling, and nurses and midwives showing a greater preference for self-sampling to take place in participants’ homes, but none reached statistical significance.
A number of studies have explored the views of healthcare professionals involved in delivering cervical screening on HPV self-sampling and the findings of this survey are largely consistent with them. Studies have found HPV self-sampling to be largely acceptable to healthcare professionals due to its potential to increase screening uptake.19,20 Studies have also identified inadequate counselling of participants on screening, 9 lack of opportunities to discuss their health concerns or physically examine them, 21 and fears around the quality of the sample taken through self-collection22–24 as significant concerns in relation to HPV self-sampling, which closely matches the findings from our survey. While many studies have assessed the views of healthcare professionals on HPV self-sampling, few have also assessed their views on how such a programme should be delivered. 25 This study, therefore, offers unique insights that could be instrumental in implementing any future HPV self-sampling policy in Ireland or a similar context.
If HPV self-sampling is to be rolled out in Ireland, this survey suggests there may be broad acceptability of it among sample takers. This acceptability would facilitate the implementation of a HPV self-sampling programme and make it more likely that sample takers would promote its use among screening participants. 26 Evidently, the disadvantages of HPV self-sampling identified in this survey should be mitigated wherever possible before its implementation. For example, providing an online or telephone consultation with participants before they perform HPV self-sampling could give sample takers an opportunity to counsel them on the benefits, risks and limitations of cervical screening and discuss general health concerns, while mitigating the risk that participants would perform the test incorrectly. 27 Additionally, awareness campaigns and education of sample takers and the public in HPV self-sampling may help to increase their trust in it and increase the likelihood that participants testing positive on a HPV self-collected test would attend a follow-up appointment with a healthcare professional. 28 The inability to visualise the cervix or physically examine participants who are performing their own HPV tests, however, cannot be addressed without compromising on some of the potential benefits, namely convenience, privacy and comfort, afforded to participants by HPV self-sampling. 29 Finally, if HPV self-sampling is introduced in Ireland, it will be crucial that the way in which it is delivered leads to increased uptake of cervical screening, whether that is through an opt-in, opt-out, or outreach strategy. 30 It is imperative that the initiative does not threaten the already high screening coverage of approximately 75%. 31
The limitations of this study included its low response rate, which was likely due to the narrow window during which the survey was open. Our study sample had an overrepresentation of nurses and midwives – 88% of respondents compared to the 61% of all registered sample takers. While our study only recruited a small number of doctors in Ireland and our sample was not perfectly representative of all sample takers, the risk of selection bias was likely low to moderate. As HPV self-sampling was only starting to be considered for introduction in Ireland at the time of survey completion, it is unlikely that many sample takers had strong attitudes towards it, and thus the survey was unlikely to have attracted respondents more likely to be in favour of HPV self-sampling. Indeed, only 10% of respondents said they had ever been asked about HPV self-sampling by patients and 28% reported not even being aware of the concept of HPV self-sampling (data not shown), highlighting the limited knowledge of respondents in this regard. Finally, the subgroup analysis comparing responses by professional was underpowered and thus unable to identify significant differences between the views of doctors and nurses. Further research to elucidate the views of doctors on HPV self-sampling may be warranted.
Conclusion
This survey shows that while there may be enthusiasm for the introduction of HPV self-sampling in Ireland, there are important issues that would need to be considered and, wherever possible, addressed before its introduction. Future research could explore further the views of doctors on HPV self-sampling, the exact role healthcare professionals might have in the HPV self-sampling pathway and how they could best support participants, particularly those who have never been screened, to make an informed choice about using HPV self-sampling.
Supplemental Material
sj-docx-1-msc-10.1177_09691413261466046 - Supplemental material for A cross-sectional survey of sample takers’ views on HPV self-sampling for cervical screening in Ireland
Supplemental material, sj-docx-1-msc-10.1177_09691413261466046 for A cross-sectional survey of sample takers’ views on HPV self-sampling for cervical screening in Ireland by Philippa White, Salma Al-Kalbani, Sarah Fitzgibbon, Rachael Comer, Mairéad O'Connor, Patricia Fitzpatrick, Nóirín E. Russell, Therese Mooney, Caroline Mason Mohan, Sinéad Woods, Alice Le Bonniec, Estelle McLaughlin, Gráinne Gleeson and Laura Heavey in Journal of Medical Screening
Footnotes
Author note
Acknowledgements
The authors would like to thank all CervicalCheck sample takers who participated in this study.
ORCID iDs
Ethical considerations
Ethics approval for the survey was granted by the Royal College of Physicians of Ireland's (RCPI) Research Ethics Committee in June 2023 (RCPI RECSAF 189) and conformed to the principles embodied in the Declaration of Helsinki.
Consent to participate
Prior to survey participation respondents were provided with information outlining the purpose of the survey and the role of the NSS in conducting it. They were made aware that the survey was anonymous, of their right to not participate and their right to withdraw from the survey at any point. They had to provide their written consent to participate.
Author contributions
LH, PW, SF and RC conceptualised the study. PW conducted a literature review to inform the content of the survey instrument. PW, LH, SF and RC devised the survey instrument. PW, SRK and LH analysed the survey data. PW, SW, CMM, MO’C, PF, NR, ALeB, EMcL and TM drafted the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability
The data used and analysed in the study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.