
Abstract
In relation to the phenomenon of moral distress, this article presents two original perspectives. First, the literature to date reflects a focus on moral distress in an occupational context. In this article, however, the impact of moral distress on siblings is explored. Moral distress is considered in a particular context, stem cell donation, but there are clear insights and implications for wider practice, particularly in life-threatening contexts and situations where live donation enhances the potential for survival. Second, the article represents some progress in relation to creating conceptual clarity. It is suggested that in addition to external and internal moral constraints a further classification of constraint emerges, and that this is useful in teasing out the distinction between moral stress and moral distress. The insights drawn from exploring the experiences of these siblings should enhance the ability to pre-empt and ameliorate potential distress and, ultimately, reduce harm.
Introduction and background
Moral distress (MD) is an intense, potentially debilitating experience and the use of the term has been explored in relation to nursing and other health-care professionals including the following: physicians, 1 medical students, 2 psychologists, 3 physical therapists 4 and pharmacists. 5 There is little evidence of the concept of MD being employed outside the health-care setting, although similar yet unrelated concepts such as emotional or psychological distress and suffering are widely and commonly employed. 6 Most significantly, the current literature focuses almost exclusively on the development and impact of MD in health-care professionals.
Inspiration for this article, however, has been generated by the experience of siblings whose brother required stem cell transplantation and insights gained from this case have generated a shift in focus from exploring the phenomenon of MD in the professional context to the experiences of the client group. The need for health-care professionals to pre-empt and manage MD is important in a wide range of clinical contexts, particularly in situations where survival is dependent upon live donation. These circumstances have the potential to generate profound distress in siblings and the wider family.
Haematopoietic stem cell donation and moral distress
As a result of cytotoxic chemotherapy used in the treatment of haematological malignancies, blood cells are destroyed and the bone marrow stem cell pool, activated by this loss, replenishes the blood cells, thus promoting haematological reconstitution. Any genetic fault within the stem cells, however, is not corrected and haematological malignancy is characterised by a pattern of remission and relapse. 7 In contrast, stem cell transplantation is a potentially curative therapy. 8 Donor cells have the capacity to repopulate the bone marrow, and have the ability to detect and reject residual disease. It is this combination of effects that can improve survival outcome in the long term. 9 Stem cell transplantation necessarily involves live donation and the demand can only be satisfied if potential donors, usually siblings, agree. Donation can literally be a matter of life and death.
All potential sibling stem cell donors (PSSCDs) are invited to discuss issues surrounding donation and they are given an opportunity to decide on a course of action. Some siblings choose not to provide a sample for tissue type testing. Others may have health problems which exclude them from donating. The initial request for tissue typing, therefore, triggers a chain of events where factors combine to create the potential for moral stress (MS) and MD. For many PSSCDs the contact from the transplant coordinator is an ‘out of the blue’ request that can turn life ‘upside down’. The probability of finding tissue compatibility in an extended family or an unrelated person, in comparison to siblings, is considerably less, especially where the patient is of mixed ethnicity. 10 The moral pressure on a family, therefore, can be intense.
All siblings are invited to discuss the issues surrounding stem cell donation with a transplant coordinator and an opportunity to give a blood sample for the tissue type test is then provided. The result is made available 1–3 weeks later, with each sibling receiving only their own result. If more than one sibling is found to have a compatible tissue type, additional selection criteria are then considered. These include current health, medical history, gender, age, blood group, virology screen and willingness to cooperate. Invariably, discussions encompass the principles, practicalities and risks surrounding stem cell donation and transplantation. Donor risk relates mainly to the use of anaesthesia and/or the administration of drug therapy depending on the method adopted. 11 Stem cell pool depletion following donation is minimal and has few known short- or long-term effects. 12 Issues that are important to one sibling may be of little significance to another, so at the conclusion of a directed family group discussion each sibling is interviewed individually and invited to make a decision, in confidence, regarding their participation in the search for a suitable donor. The responses and choices made by PSSCDs can be unexpected and surprising, and these are not necessarily related to the risks involved.
Blessing or burden?
Being the ‘chosen one’ can prove to be an immense moral challenge when, for various reasons, an individual cannot or will not donate. Being considered as the ‘saviour sibling’ may appear to others as a blessing, but depending on the circumstances, it may be more aptly described as a ‘burden in disguise’. Clearly in clinical situations like this, the focus of attention is the patient. The stark reality is that this person is unlikely to survive without stem cell transplantation, so it is understandable that the potential donors are seen as ‘treatment’ sources. The focus is on cure and achieving the best possible outcome for the patient, and as a result of this the needs of potential donors can be overlooked at a time when they ought to be cushioned from harm. The patient waits and hopes for a successful transplant, and some PSSCDs wait and hope that they will be selected, and others that they will not be a match and that they will be ‘let off the hook’.
All these considerations point to the potential for MD described by Jameton 13 as ‘painful feelings and/or psychological disequilibrium that occurs in situations in which the ethically right course of action is known but cannot be acted upon’. There is a gap in the literature in relation to how this phenomenon can emerge within the context of patients and siblings, and there is also a need to consider how we can do good (if possible anticipate problems to prevent/reduce MD) and avoid harm (not contribute to MD).
MD is triggered by any event or set of circumstances where the individual knows what the morally compelling thing is, he wants to comply but cannot do so because of constraints. These constraints can be internal, emanating from within the person, or external involving factors such as codes, laws and policies.13,14 McCarthy and Deady 14 make the link between that which we classify as internal constraints and Aristotle’s notion of akrasia, also known as weakness of the will, or moral incontinence (MI). An agent with MI knows what the phronimos (paradigm person) would do in order to behave well, but cannot overcome his weakness and fails to do good (Aristotle Nicomachean Ethics (NE) 1146a30-b15). 15 This is worth exploring further in an attempt to understand the moral motivation, decisions and subsequent well-being of the characters involved. Although constraints are generally considered to fall into two categories, external constraints and internal constraints, 13 as a consequence of this exploration it is suggested that there is a third class of constraint, one that straddles the internal classification (MI) and external classification – it is not exclusively internal or external, but it is a ‘combined constraint’. This class of constraint is comprehensive in nature, marrying external and internal constraints and it is suggested that the distinction can throw new light on the nature of this phenomenon in the context of effective care of clients and their families. This distinction has emerged through exploring the phenomenon of MD as experienced by siblings when faced with the prospect of being a stem cell donor. It is a distinction that will also be useful in considering MD from a wider professional or occupational perspective.
Moral distress: what it is and what it is not
An individual may experience MS but emerge from the experience having resolved the problem in such a way that he suffers no sense of moral wrongdoing or lasting damaging effects. Stress of any type that exceeds the individual’s capacity to cope results in distress, 16 and in the case discussed below it became clear that those who felt that they were failing to live up to their perceived moral responsibilities progressed to MD. Moral certainty is a clear knowledge and understanding of what the morally correct course of action should be. It is moral certainty that creates the perception of wrongdoing when an individual acts in a manner contrary to their moral values and this leads to MD. 17
MD is also to be distinguished from emotional distress (ED) and the difference lies in the cause, the nature of the event or circumstances that generate the distress. ED is experienced by patients with leukaemia and their siblings, and this is to be expected in such circumstances. MD, on the other hand, is generated by the agent’s perception of their moral response to the situation, in this case, the response to a request to donate stem cells.
MD is experienced by those who want to do what they consider to be the right thing (donate) but are constrained from doing so and the concept of MD encapsulates a wide range of human responses to real or perceived moral wrongdoing. A person may experience MD in one particular situation but not in another similar one, and the same situation may cause MD in one person but not in another.3,18 Psychologically, MD is associated with strong negative feelings, including unhappiness, anger, resentment, frustration, guilt, sorrow, shame, helplessness, anguish, despair and anxiety.18–21 Nurses experiencing MD also report a loss of self-worth, decreased coping abilities and sleeplessness. 19 Physiologically, individuals experience anxiety and stress-related symptoms such as sweating, shaking, headaches, gastrointestinal distress and crying. 3 Professionally, nurses may feel guilty and blame themselves for not living up to their professional ideals. 17 If the response to MD is not addressed, self-worth is jeopardised with the potential to adversely affect both professional and personal relationships.22,23 It seems reasonable to extrapolate from these findings and claim that such symptoms are also felt by relatives and clients. The triggers may be different but the manifestations appear to be similar. MD, therefore, is distinct from ED and MS. Although it can be triggered by many situations, the common denominator in the development of MD is perceived as moral wrongdoing due to MI and the nature of the constraints involved.
Moral distress and states of character
Internal constraints
Aristotle’s NE 15 offers a valuable source of insight in relation to moral responses and behaviour in applied ethics. MI is central to Aristotle’s approach to understanding moral motivation. An individual with MI is one who attempts to make himself act properly but fails. In the case presented below, PSSCDs want to behave well, but cannot do so because of some weakness in their own natures (internal constraints). The agent with MI chooses the good but does not act on it because of constraints internal to himself (Figure 1(a)) and sometimes because of a combination of internal (MI) and external constraints (Figure 1(b)).
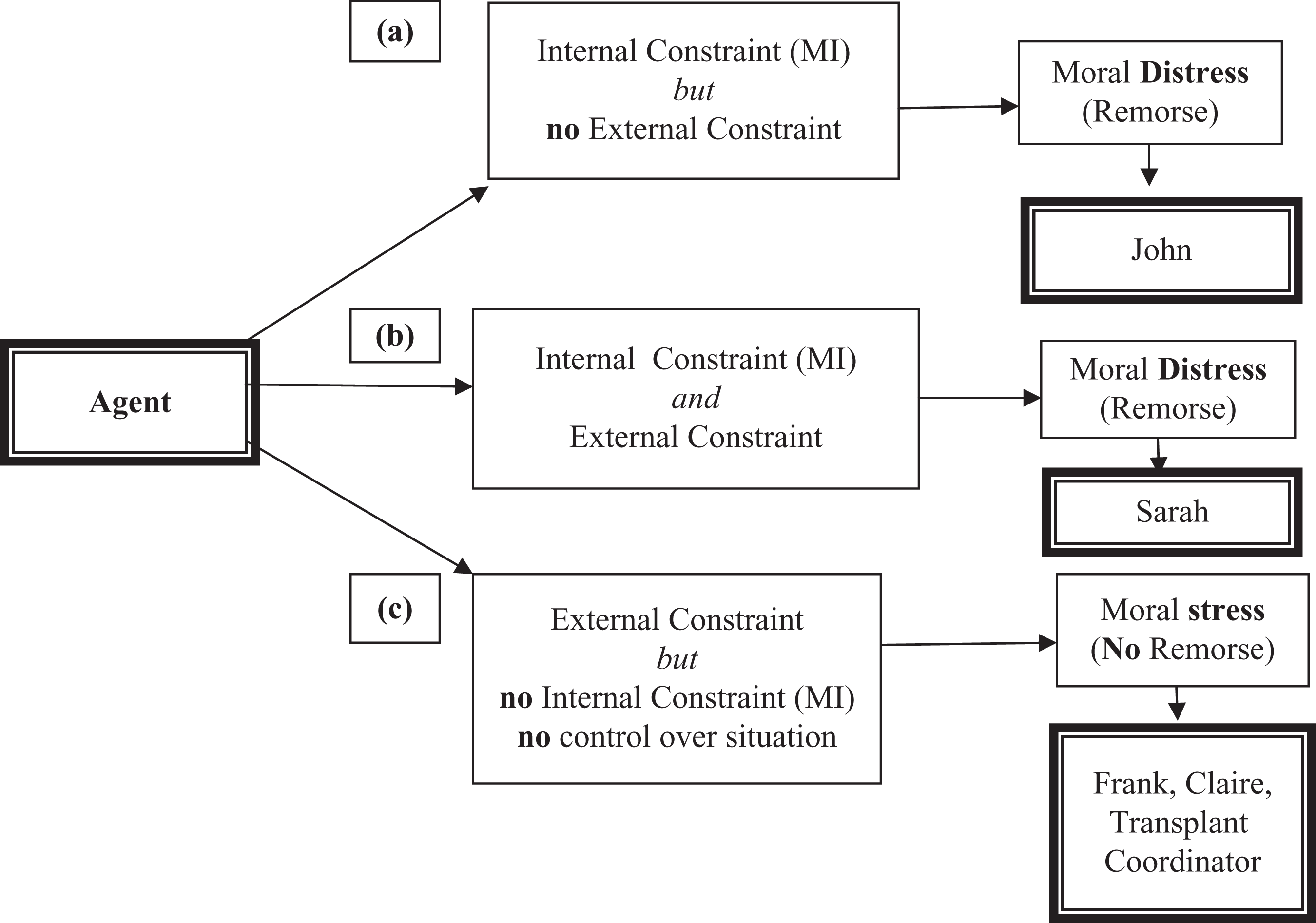
Constraints, moral distress and moral stress.
According to Aristotle there are four states of character, full virtue (arete – excellence of character), continence (enkrateia – strength of will), incontinence (akrasia – weakness of will, MI) and vice (kakia – viciousness, badness and callousness).15,24 A morally incontinent person wants to do good, tries to make himself do good and fails: he is not able to overcome his weaknesses and fears.
In order to understand how a person may develop MD as a consequence of his decision, we need to consider the processes involved in a decision to act, rather than to look at the act itself, and Aristotle considered choice to be a better test of character than actions (NE 1111b5 – 1112a17).15,24 An individual with MI (akrasia) who tries to act well but fails does not attract such strong disapproval as the cruel or callous person (kakia): ‘he is only half wicked’ (Aristotle NE 1152a1-20). 15
Thus it is evident that incontinence is not a vice (except perhaps in a qualified sense) because it is contrary to the agent’s choice, whereas vice is in accordance with choice. (Aristotle NE 1145a6-10) 15
Within the context of the PSSCD, therefore, a sibling may choose to donate but fail to do so, and the important thing is that he chooses to help and is inclined to donate. He may be kind and well meaning, but weak. On the other hand, the bad, callous person (kakia) would refuse to donate and experience no guilt, remorse or other symptoms of MD as outlined above.18–21
Aristotle, therefore, differentiates between the person who wants to do the good thing (donate) but cannot bring himself to do it, and the individual who simply does not care or is motivated by spite or cruelty. This is the key to understanding both internal and external constraints leading to MD, and more importantly, to indicating a way in which the practitioner can help the client to understand and be more tolerant of his own perceived moral weakness. Kant did not acknowledge this grey area, but the neo Aristotelian approach is more sensitive to individual characters and contexts such as these. 25 The difficulty is that the person who wants to donate but is constrained by MI (or MI combined with external constraints) fears that he will be perceived as an uncaring, wicked person, and he needs help to understand that, from a moral perspective, there is a difference between his moral status and that of the callous person. Insight into character states gained from exploring the approaches of Aristotle represents a valuable contribution to our understanding of MD in general, and in this case, in a client and family group.
External constraints
In relation to practice, external constraints encompass institutional or organisational factors that direct or influence a nurse’s course of action regardless of whether that action is in line with his or her moral values. 26 Within the context of PSSCD external constraints might translate to family commitments (childcare needs and elderly parents), work constraints, geographical/travel limitations and family dynamics.
Constraints, control: stress and distress
A significant point and one that helps distinguish between MS and MD is that some external constraints are within our control and some are not. For example, from a professional perspective we may not have the moral courage to act contrary to a law or policy in the interests of doing good, but morally we are still in control and choose to act in a certain way. Failing to demonstrate moral courage in situations where external constraints take the form of laws or codes can cause guilt and remorse 27 and a practitioner who fails to follow his moral instincts is subject to a combination of external and internal constraints (MI) (Figure 1(b)).
In contrast, when the external constraint is beyond the agent’s control and there is no internal constraint (MI), there is an absence of guilt or other characteristic symptoms of MD as outlined above.18–21 The agent (practitioner, relative or client) may still feel a sense of moral dismay and frustration at being prevented from doing the ‘right thing’ and this can lead to symptoms of MS rather than progressing to MD (Figure 1(c)).
On the basis of these observations it seems more likely that MD develops when there is an element of control and the agent, in this case the PSSCD, feels guilt and remorse arising from the internal constraint of MI (Figure 1(a)) or when there is a combination of external and internal constraints (MI) (Figure 1(b)).
A case in practice
The majority of potential donors linked to the recipient by a familial relationship rapidly agree to be tested for compatibility and willingly proceed to donate on request.8,28 Data collected from newspaper and magazine reports suggest that individuals who choose to deviate from the values held within a family, or those who disregard familial obligation or duty, are liable to attract significant pressure to conform.29–31
The following scenario illustrates how this can happen
Ben has acute lymphoblastic leukaemia and is likely to benefit from stem cell transplantation. His siblings, Claire, Sarah, Frank and John, are contacted and asked to come for testing/screening. John lives abroad and has had little contact over the past 20 years, but is contacted through a friend, to arrange a family discussion. John links up via Internet. Frank, John and Claire agree to be tested and Sarah opts out. Postal screening is arranged for John.
Outcome
Frank and John are identified through tissue typing as potential donors and Claire is excluded. Frank is keen to donate and, since John lives abroad, this seems to be the best way forward. Unfortunately, shortly after this is agreed, Frank has a myocardial infarction and he is excluded as a donor due to unstable angina. John is healthy and he is, therefore, the most suitable potential donor, ‘the chosen one’.
Impact on family
Claire
Claire has no control over the situation and expresses no sense of moral wrongdoing or remorse. She wants to donate and initially feels frustrated and stressed but becomes resigned to the situation.
John
The transplant coordinator receives a confidential email correspondence from John who explains that he really cannot donate stem cells. He cites a variety of reasons – he does not like flying, the medical commitment worries him and the pressure of being the focus of his brother’s survival concerns him. He agreed to be tested but had hoped that he would not be a match, or that there would be others who lived closer and would step up to donate. He also hoped that if he was chosen, he would feel differently, and that his brother’s need would help him to generate the courage to ‘rise to the challenge’, as he put it. Frank’s illness and subsequent inability to donate has put John under the spotlight. When it first emerged that Frank wanted to donate, John was relieved – although he wants to help, he cannot bring himself to do so. He is too ashamed to tell his wife and children that Frank cannot donate, and they assume that all is well. John cuts off any form of communication with his siblings. In subsequent telephone conversations with the transplant coordinator it becomes clear that John is experiencing immense distress, guilt, shame and isolation and that these symptoms become worse as time elapses. In John’s case, then, being ‘the chosen one’ is a burden that has a major impact on his life, his sense of self-worth and his family relationships. John is experiencing symptoms of MD as identified above.18–21 John’s constraint is internal (MI). He tries to take control of his feelings, but they overwhelm him. He knows what he ought to do but is not able to overcome what he perceives to be a moral weakness. On the surface, John seems selfish and callous. There is no physical reason, no illness, phobias or other external constraints such as pressure from family (as in Sarah’s case). He is experiencing MD due to internal moral constraints (MI) (Figure 1(a)).
Sarah
Sarah has three children and her husband is unhappy about her becoming a donor. He is going for promotion, the children have important school years ahead of them and he does not want disruption to family life. Sarah feels trapped. She wants to donate but has not got the emotional strength or moral courage to overcome the external constraint. She perceives this as moral weakness and is ashamed of her powerlessness and inability to take control of her own life. This is similar to the situation in the workplace where a nurse knows what she ought to do, but has not got the moral courage to challenge policies and procedures, or, for example, a bullying situation. There is some choice and some potential for taking control over the situation. The salient point is that if the external pressure did not exist, Sarah would agree to be tested and donate. Sarah’s weakness (as she perceives it) lies in challenging the external constraint, while John’s lies in not having the courage to become a donor. Sarah is experiencing MD due to a combination of external and internal constraints (MI) (Figure 1(b)).
Frank
Meanwhile, Frank has tried to persuade the transplant team to let him donate. Like Claire, he feels stressed at the thought that he cannot help his brother despite the fact that it is beyond his control. There is no tension between his moral position and his resolve to donate. The medical veto has taken the decision out of his hands. The external constraint takes the form of an overriding clinical judgement. Frank is experiencing symptoms of MS due to an external constraint over which he has no control. The source of his stress is his moral obligation which he cannot fulfil, but there is no guilt or other symptoms identified as being congruent with MD (Figure 1(c)).
Transplant coordinator
The transplant coordinator experiences MS. She is constrained by external factors over which she has no control. She feels frustrated by her inability to facilitate Ben’s transplant, but she also has to respect John’s choice. Her stress is understandable and she empathises with both Ben who has a bleak prognosis and John who is suffering and has become isolated from his family. She feels no guilt, no remorse and she has no choice in the matter. She has no control over the situation and does not demonstrate any of the symptoms of MD as outlined above.18–21 There is no sense of moral wrongdoing and the source of her stress is the moral quagmire in which she finds herself (Figure 1(c)).
Primum non nocere (first do no harm)
In clinical situations such as this, there is always a need to find a balance between doing good and doing no harm. It must be acknowledged that focusing on the needs of Ben and not being sensitive to the position of the potential donor may contribute to the development of MD and family disharmony at a time when siblings need to support each other and the recipient. It is not, however, easy to be an advocate for both the PSSCD (having respect for autonomy and choice) and the patient, and this contributes to the development of MS in practitioners.
In this case it is clear that harm, in the form of MD, has been done. John and Sarah’s lives have suddenly been ‘turned upside down’, but if live donors are to be found people must be approached. The objective, therefore, is to assist those who cannot donate due to internal constraints (MI), or a combination of internal and external constraints, to understand the source of their distress and to be more tolerant of their own perceived weaknesses. Most importantly, they should not conflate MI (akrasia) with being callous and mean spirited (kakia). Facilitating an understanding of the nature of the constraints can help professionals to support clients dealing with distress and, ultimately, to minimise the destructive force that this situation can have on siblings and wider family groups.
Engaging with people in emotional turmoil relating to diagnosis and prognosis calls for sensitivity and empathy. While the emotions settle and the ED subsides with the healing of time and professional help, MD carries with it the potential to arise every time the potential donor thinks of the sick (or deceased) sibling. Episodes of MD are known to cause a cumulative and enduring negative effect in terms of self-worth and life satisfaction. 32 The consequences of this experience for John and Sarah may linger over time and may be manifest in continued guilt, shame and regret.33,34
Blood is thicker than water
Advertising and recruitment campaigns by the National Health Service Organ Donor Register 35 are used to heighten public awareness of the growing need for organ donors and more specifically to appeal to the public’s sense of social or cultural responsibility and moral duty. Within the context of sibling donation, the perception of expectation, familial responsibility, a sense of duty and obligation can be considerable. 36
The film ‘My Beautiful Son’ 37 depicts an estranged mother and son who wrestle with the difficulties that the sudden need for a stem cell transplant brings. The media portrayals challenge the viewer to consider what they would do in a similar situation, what value they would place on the moral virtue of benevolence and generosity and the notion that family always come first. The expression ‘blood is thicker than water’ captures the assumption that family relationships are more meaningful and stronger than other nonfamilial bonds. Powerful images such as those by Raban 38 and journalistic articles reporting on parent-to-child 39 or sibling-to-sibling donation 40 are increasingly common in the media and these attest to the emotive power of familial connections.
Appeals by families searching for an estranged sibling appear with regularity in the popular press. 30 The ‘chosen one’, ‘a perfect match’, ‘a saviour sibling’ are phrases used in a sibling donor context41,42 and those who have donated have expressed the intensity of the special nature of donation: ‘My heart told me to do it’; ‘I felt called to do this’ 43 and ‘this is the purpose for which I was born’. 44 Donation is described as a ‘defining moment’ by one sibling, 43 while the consequences of failing to donate are described as a ‘life-sentence’ by another. 44 John and Sarah experience guilt and shame as a result of their perceived moral wrongdoing and such guilt is reported as particularly problematic when the potential recipient does not survive. 45 When a potential donor withdraws, family, friends and even work colleagues can display a lack of sympathy and failure to understand or respect the decision. It is, therefore, difficult for a sibling to refuse and it is clear that the emotional connection between siblings should not be understated. 28 Not all family members will be unsupportive of course; they may appreciate the motivation behind a sibling’s decision and/or recognise the constraints on moral action but this acknowledgment may do little to alleviate a sibling’s feelings of guilt. 46
The breakdown in family relationships is perhaps the most damaging consequence of MD. Family members who fail to understand or support a sibling in MD may impose sanctions in terms of communication and affiliation. 47 Circumstances requiring the search for a sibling stem cell donor are already likely to be stressful for a family group; the decisions and conduct of siblings experiencing MD can further add to that anxiety. It can be difficult for people such as John (Figure 1(a)) and Sarah (Figure 1(b)) to avoid moral judgement and to protect their interests, autonomy and privacy. The reproach of family members is a powerful force and relationships can become compromised as a result. This was obvious from the response of both John and Sarah, who excluded themselves from the family group because they felt such shame and guilt.
Conclusions and implications for practice
McCarthy and Deady 14 suggested that further conceptual clarity is needed in relation to MD and it is suggested here that there is also a need for empirical ethics and investigations in relation to the impact of MD in a wide range of clinical contexts, particularly in situations where patients and relatives struggle with surviving life-threatening conditions. The article raises concerns in relation to stem cell donation and suggests that understanding triggers of MD and moral constraints may enhance communication and avoid long-term damage. Research, innovation and progress in the treatment of life-threatening conditions will continue to generate moral challenges for professionals. We need, however, to recognise that patients and relatives also have hard choices to face and that these can have a serious impact on their lives. This is particularly true of live donation and the need for donor compliance.
This article offers some contribution to our understanding of the nature of MD by suggesting that there is a third, a ‘combined’, class of moral constraint (Figure 1(b)). This is demonstrated by the person who exhibits weakness in their resolve to act despite feeling morally compelled to do so (MI). This person fails to challenge and overcome external constraints (Figure 1(b)). This class of constraint has emerged during exploration of this particular case, but it is significant to both professional and clinical contexts because it distinguishes between straightforward weakness of will (Figure 1(a)) and one who demonstrates weakness of will in relation to challenging external constraints. It also helps draw a line between those who have no control over external constraints (Figure 1(c)) and those who have some measure of control (Figure 1(b)).
A health-care professional who is aware of the sources of MD and the potential for its development in all areas of practice can cultivate strategies that aim to maintain the moral integrity of clients, siblings and the wider family group, thus avoiding harm.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interests.