
Abstract
The aim of this study was to explore and reflect upon mental health nursing and first-episode psychosis. Seven multidisciplinary focus group interviews were conducted, and data analysis was influenced by a grounded theory approach. The core category was found to be a process named ‘working behind the scenes’. It is presented along with three subcategories: ‘keeping the patient in mind’, ‘invisible care’ and ‘invisible network contact’. Findings are illuminated with the ethical principles of respect for autonomy and paternalism. Nursing care is dynamic, and clinical work moves along continuums between autonomy and paternalism and between ethical reflective and non-reflective practice. ‘Working behind the scenes’ is considered to be in a paternalistic area, containing an ethical reflection. Treating and caring for individuals experiencing first-episode psychosis demands an ethical awareness and great vigilance by nurses. The study is a contribution to reflection upon everyday nursing practice, and the conclusion concerns the importance of making invisible work visible.
Introduction
Mental health nurses constitute the majority of the work force in mental health care and can therefore make an important contribution to treatment and care of mental health patients. Several international guidelines describe best practices in treatment and care of individuals experiencing first-episode psychosis (FEP). 1 –5 However, these guidelines do not distinguish between how different professionals should contribute. Consequently, this provides little information about the role of the mental health nurse regarding treatment and care of individuals experiencing FEP.
FEP refers to the first time a person experiences a psychotic episode, and it often occurs in late adolescence. 6 The characteristic symptoms are delusions, hallucinations, disordered thoughts and behaviour. Individuals experiencing FEP are at risk of reduced social and occupational function and, therefore, constitute a vulnerable group. 1,7 There is considerable research on the importance of early identification and treatment in FEP. 8 –11 Patients may require care and treatment involving several aspects, such as family support, psychoeducation, illness management, psychotherapy, vocational rehabilitation and pharmacological treatment. 1,7,12 Early intervention is essential regarding the psychological impact on patients and their families, 9 and several studies indicate that early intervention of psychosis predicts a better outcome. 8,10,11,13
Internationally, there has been a transition from hospital-based to community-based care of mental health disorders. 12 The Norwegian national guidelines promote community-based mental health services. 14,15 Community Mental Health Centres (CMHC) have a core role in treatment and care in their geographic sector, and they are a pathway to specialized hospital care. 16 Local adaption is emphasized within frames of political and health guidelines. 16
Previous studies show that mental health nurses are involved in many aspects of treatment and care of individuals experiencing FEP. 1,7,17 Van Dusseldorp et al. 1 identified five domains defining the contribution of nurses: development of therapeutic relation, relapse prevention, enhancement of social function, stimulation of medication adherence and support of family members. They also emphasize the importance of research providing evidence-based insight into the role of mental health nurses, and that nurses should reflect upon their own daily practice. 1 Little research is found from the CMHC context in Norway concerning early intervention of psychosis, and therefore, the aim of this study is to explore and reflect upon mental health nurses’ clinical practice regarding care and treatment of individuals experiencing FEP in a CMHC.
Methods
Qualitative research methods were selected to explore the nurses’ clinical practice in CMHC, treating and caring for individuals experiencing FEP. This study is part of a larger research project exploring other aspects of CMHC, so data collections were done with several aspects. The data were collected using focus group interviews, 18 and the analysis is influenced by a grounded theory (GT) approach. 19 –21
Participants/context
The study took part in a rural area of Norway. All CMHC (n = 7) within a county were invited to participate. The leaders of the centres were contacted by telephone for information about the study and asked to suggest participants for focus group interviews. They were asked for six to eight participants who were directly involved in the treatment of young individuals (16–35 years old) experiencing FEP, and variations in health professionals and gender. An information letter circular was sent to the leader, who distributed it to the participants. Two of the participating CMHC had a specialized early intervention team. The others had generalist services.
Data collection
GT allows for different methods of data collection. This is because different groups and problems need different ways of collecting information, and the researcher needs to be flexible. 20 Focus groups were chosen because it is a useful method to collect data from more participants in a time-saving and cost-effective way. 22 The method has been useful to obtain participants’ practice and opinions, by discussing with each other and exploring their collective memory. 23 It was intended that participants should reflect upon their own daily practice. The interviews were planned and conducted as described by Krueger and Casey. 18 All seven focus groups were conducted at the mental health centres from October 2010 to March 2011 and lasted for 90–120 min. There were two to seven participants in each group. A moderator, who ensured that all participants felt included and got the chance to share their opinions, led the interviews. The interviews were focused with a question guide, and adjustments were made before each interview based upon the ongoing analysis according to GT and the focus group method. 18,20 An assistant moderator took notes during each interview, summarized and asked complementary questions at the end. During the focus group interviews, we asked participants what they think was the nurses’ role, and recorded the discussions by both nurses and other professionals. The data from this multidisciplinary group might differ from a group with just nurses, but authors believe the other professionals gave supplementary data.
Analysis
A GT approach was used for data analysis. GT was developed by Glaser and Strauss, 20 but this study is mainly inspired by Glaser’s approach. 19 –21 GT is a useful research method when there is little prior information about a topic. Glaser describes the goal of GT as ‘to generate a theory that accounts for pattern of behaviour which is relevant and problematic for those involved’ (p. 93). 19 The method was considered useful to explore nurses’ clinical work and how they experienced and coped with their challenges.
Each interview was transcribed verbatim. Transcripts were coded line by line (open coding) searching for words describing the nurses’ clinical work, role and challenges. Memos were written after each interview and during the analysis process, focusing on relationships between codes, phrases and categories (constant comparison). The codes were sorted into categories, and a core category was found. The codes related to the core category were sorted out (selective sampling) and sorted into three subcategories. NVivo software was used as a tool to arrange data and document the analysis process (Table 1). 24
Phases in the analyses.
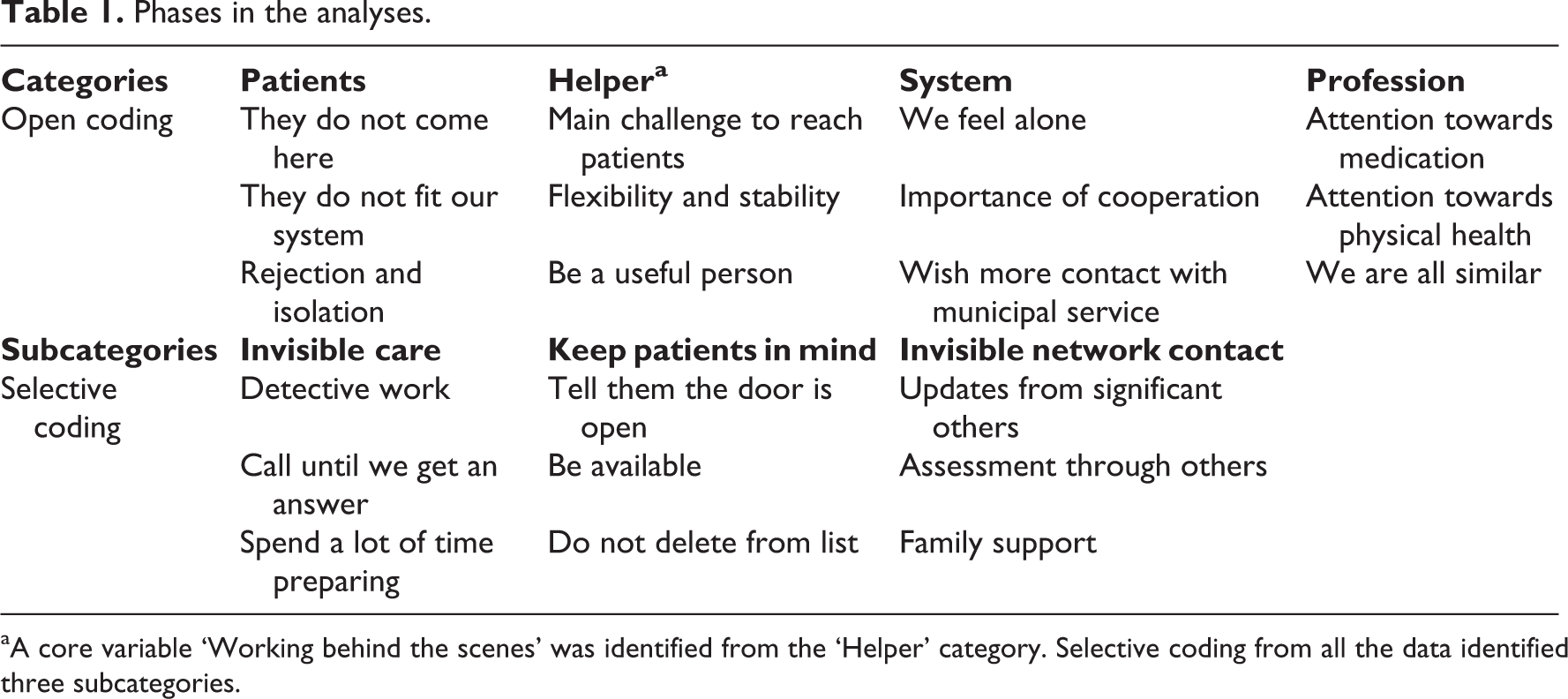
aA core variable ‘Working behind the scenes’ was identified from the ‘Helper’ category. Selective coding from all the data identified three subcategories.
Ethics
The study is approved by the Regional Committee for Medical Research Ethics (REKNORD 2009/1426). All participants gave informed consents. All data have been treated anonymously.
Results
Our findings are presented in one overarching theme (core category), which we named ‘working behind the scenes’ along with three subcategories: ‘keeping the patient in mind’, ‘invisible care’ and ‘invisible network contact’.
How participants defined their task concerning individuals with FEP varied. Some CMHC focused on clinical assessment and considered support and recovery as tasks for the municipal services. Other centres offered both clinical assessment and recovery. The degree of involvement from the hospital varied. All centres were organized in a multidisciplinary manner, and beside medication and attention towards physical health, there was little awareness of the nurse’s role versus other health-care and social-care professionals. Descriptions of practice also confirmed that professional background does not affect patients’ treatment and care. Therefore, the findings in this study will describe clinical work by both nurses and other health-care and social-care professionals.
‘Working behind the scenes’
The CMHC nurses experienced a diversity of challenges regarding helping young individuals experiencing FEP. They shared a common feeling of responsibility and a willingness to be flexible. Nurses described the patients as hard to engage and reluctant to undergo treatment. This was explained both by the patients’ symptoms, such as social withdrawal, apathy and emotional distress, and the fact that nurses were hindered from visiting the patients in their home because of long distances and demands for effectiveness. The nurses’ main challenge was not being able to reach the patient, both physically and mentally. To cope with this challenge, we identified a process named ‘working behind the scenes’. This indicates how the nurses spend time working around the patient, without the patient’s knowledge, participation or engagement. In the words of one of the participants, We do a lot of things, but no one knows – to put it that way. We kind of work behind the scenes to get in touch.
‘Keeping the patient in mind’
The nurses kept the young individuals in their mind, and in the health-care system. Usually patients drop out of the patient list if they do not show up for three appointments, but these patients were informally exempted from this procedure. Even though the nurses did not physically meet a patient, they did spend a lot of time worrying, discussing the patients’ health and wondering how to reach them and do assessments. An ethical dilemma concerning how persistent they could be towards patients was also mentioned. Participants were divided concerning whether patients actually said no to meeting with them or whether they agreed to meet, but did not manage to show up: And we say the door is open and we know the person. Give us a hint, we are ready, and we try again. How assertive is it allowed not to be? When does it become a sin of omission? The reason why we lose these patients is hiding behind ethics. We don’t want to be persistent. It is unethical not to be assertive ...
‘Invisble care’
Although not always explicitly expressed, the nurses seemed to emphasize the importance of building a safety net for each individual. This was meant to ensure that the patient could continue school or work, have financial security and receive practical support in daily life. Activities such as going on a drive or visiting a café were useful to build a trusting relationship. Although such activities are visible and noted in the patient’s journal, there is still a lot of invisible work around these activities. Several days before the planned meeting, the nurses sometimes started to prepare the patient and themselves. Sometimes, they had made an agreement that the patient would receive an e-mail or text message a certain time before the encounter. If the patient did not show up, the nurses often called several times to get in touch, consulted colleagues or municipal services or rented a car to seek the patient at home, if they were worried.
The nurses were always looking for creative ways to reach the patient. Text messages and e-mails were widely used. The participants agreed that the CMHC does not fit the FEP patients, but they still tried to make the service more suitable for the particular individual and more relevant to his or her individual needs. Most of this work stayed invisible because it was not noted in the patient’s journal, and no one saw it. We spend a huge amount of time trying to reach the patient. It’s so hard with these patients, they don’t show up. It requires a lot of preparations to make them accept treatment. Yes, I think we spend a lot of time calling, we spend a lot of time sending text messages. We spend a lot of time being available, we spend a lot of time inviting to.
‘Invisible network contact’
Supervision and teaching were assigned tasks for the nurses at the CMHC. They had regular meetings with municipal health employees and families to enhance their competence and help them endure their challenges with a certain patient. However, a part of the practitioners’ networking remained neither scheduled nor within the patient’s consciousness. If patients did not show up for an encounter or lacked words to describe their situations, the practitioners could feel they did not get enough information to assess the patient’s health. This was important because the nurses were often responsible for treatment and were the only contact in specialized mental health care. The nurses often contacted the patient’s network for supplementary information. Information about symptoms, medication compliance and activities of daily living (ADL) functions was considered important. Likewise, the network contacted them if they were worried or needed some advice, and they were offered support, information and reassurance. Nurses tried to think of creative ways to cooperate with the network, to make services more available to them and to facilitate helpers near the patient.
Owing to the long distances or patients’ health, nurses from CMHC sometimes had a more withdrawn and coordinating role. They ‘worked through others’ or had ‘indirect’ contact with patients. This could be asking municipal services to initiate interventions or asking the families to observe certain symptoms or functions. They reported back to CMHC clinicians who made assessments. … we don’t give up, we don’t. We don’t close the case, we keep contact with the patient’s network to make them feel they are a part of something. Forming relationships takes time, the young ones fall out. We need to be more active and work with network around them, that kind of activity.
Discussion
The core category ‘working behind the scenes’ summarizes a process describing some of the nurses’ work at a rural CMHC. In this article, the phrase ‘working behind the scenes’ indicates that something is hidden, invisible or unregistered. The purpose of the study was to explore the clinical work and reflection of mental health nurses in treatment of FEP. The ongoing analysis and study findings raised some ethical questions, and ethical theory of autonomy and paternalism was chosen to illuminate the core category.
Ethics of autonomy and paternalism
The principle of respect for autonomy recognizes individual choice and freedom of the will, 25 and in modern health care, it is considered to be important. 26 Beauchamp and Childress 25 define three conditions for an act to be autonomous: the acts are (a) intentional, (b) with understanding and (c) without controlling influences that determine their action. In health care, the principle of respect for autonomy primarily recognizes the right to decide about one’s own treatment, and in particular, to refuse treatment. 27
Paternalism is considered contradictory to the values of autonomy. Beauchamp and Childress 25 define paternalism as ‘the intentional overriding of one person’s known preferences or actions by another person, where the person who overrides justifies the action by the goal of benefitting or avoiding harm to the person whose preferences or actions are overridden’ (p. 178). Paternalism is the sharp end of professional beneficence 28 and should only be considered when patients lack capacity and when treatment is in the patient’s best interest. 29 In psychiatric practice, there has always been a tension between restraint and freedom. Practice easily slips into paternalism, even though there may be good intentions. 30
‘Working behind the scenes’
The participant’s main challenge was not being able to reach the patient, both physically and mentally. To cope with this, we identified a process named ‘working behind the scenes’. This indicates that the nurses spend time working around the patient, without the patient’s knowledge, participation or engagement. The mental health nurses’ clinical practice moves along an autonomy–paternalism continuum. ‘Working behind the scenes’ is considered as an area towards paternalism, justified by ethical reflection based on the principle of beneficence and the nurses’ responsibility for the patient’s health (guidelines). What characterizes this area is that care is ‘determined by others’, or in other words, patients do not participate in decisions concerning their own treatment (Figure 1).
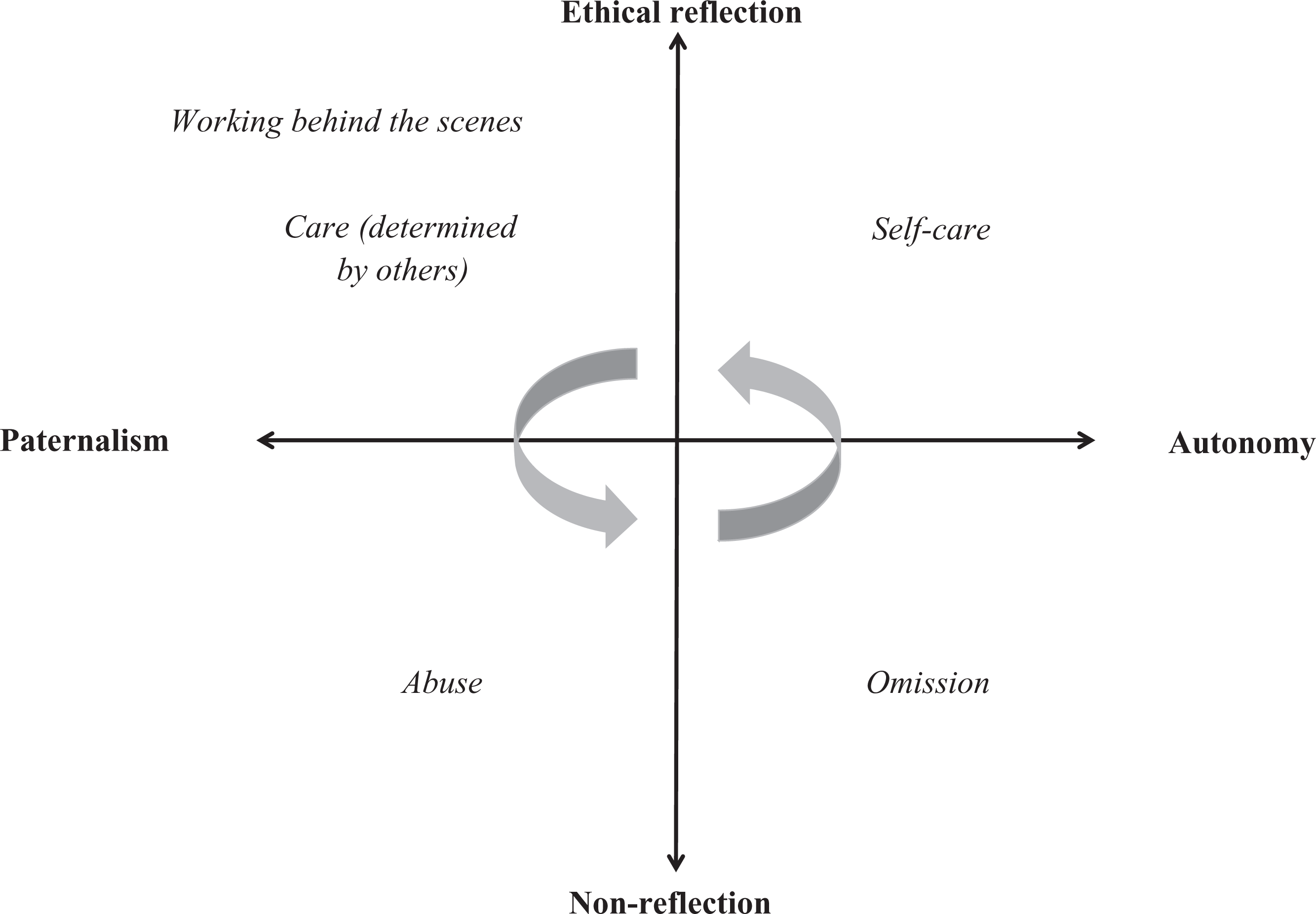
‘Working behind the scenes’, an ethical view of mental health nursing.
‘Keeping the patient in mind’
An ethical dilemma concerning how persistent the participants could be towards patients was mentioned in the interviews. The nurses kept the young individuals in their mind, and in the health-care system. Usually patients drop out of the patient list if they do not show up for three appointments, but these patients were informally exempted from this procedure. Even though the nurses did not physically meet a patient, they spent a lot of time worrying, discussing the patients’ health and wondering how to reach them. Psychotic symptoms might lead to avoidance, anxiousness and isolation, which make it difficult for nurses to assess whether patients refuse treatment or do not manage because of psychotic symptoms and distress. This makes everyday practice challenging because nurses do not want to be persuasive nor to be accused of omission. They ‘keep the patients in mind’ and do assessments concerning the patient’s health. What makes it more complicated is the fact that interventions are often justified as preventions for deterioration risk on a long-term view and future compulsory treatment, but not on present mental health. Sjostrand and Helgesson 27 find defending the patient’s future autonomy interest at the cost of present authentic interest, unacceptably paternalistic.
‘Invisible care’
A lot of the mental health nurses’ work is invisible. The nurses were always looking for creative ways to reach the patient. Text messages and e-mails were widely used. The participants agreed that the CMCH does not fit the FEP patients, but they still tried to make the service more suitable for the particular individual and more relevant to his or her individual needs. Most of this work stayed invisible because it was not noted in the patient’s journal and no one saw it. Invisible care is an example of nurses’ action justified by beneficence. Shattell et al. 31 also found ‘invisible caring’ as a description of thoughtful actions provided by nurses in their care. No one, not even the patients themselves, notices what nurses actually do for them. Invisible care is easy to consider as nice and friendly, but should also be based on ethical awareness. What is done in the best intention might be perceived as a violation of trust.
‘Invisible network contact’
A part of the practitioners’ networking was neither scheduled nor within patients’ consciousness. The nurse often contacted the patient’s network for supplementary information. Information about symptoms, medication compliance and ADL function was considered important. Likewise, the network contacted them if they were worried or needed some advice, and they were offered support, information and reassurance. Nurses tried to think of creative ways to cooperate with the network, to make service more available to them and to facilitate helpers near the patient. Individuals experiencing FEP are often withdrawn and hard to engage in treatment. 32 If the nurses do not have an opportunity to assess the patient’s mental health and interact if necessary, there could be a risk of relapse, untreated psychosis and even a risk of suicide or violence towards others. 33 The nurses feel responsibility for each individual and strive to get an overview of their situation. If the patient avoids treatment, it feels as if it is crucial for nurses to be persuasive or stay in touch with the patient’s network. ‘Working behind the scenes’ when working indirectly or through others might be in the grey zone of a concept named by Lutzèn 34 as subtle coercion where clinicians, through others, are judging patients’ competency.
An ethical view of mental health nursing
Acute psychosis may impair a person’s reality testing, distort his or her comprehension of the world, and therefore, lead to an impaired ability to make rational treatment choices. This complicates the principle of respect for autonomy. It is still important to be aware that most people with psychotic disorders recover from the acute episodes, and although they may still experience delusions or hallucinations, the symptoms have less intensity and the person may have their reality-testing capacity intact. A patient with a psychotic disorder may understand that auditory hallucinations differ from external phenomena and will be fully competent to decide for himself or herself whether or not to accept treatment. 27
If paternalistic actions are done without ethical reflection, there is a risk of abusing patients. Deception, manipulation or non-disclosure of information and coercion are examples of actions that might be abusive, if they are not ethically reflected and justified. Likewise, if patient autonomy is fully set into action without any ethical reflection, there will be a risk of omission. Nurses would not be aware of a patient’s vulnerability and loss of self-care skills.
Mental health nursing containing ethical reflection and awareness of patient autonomy will lead to an improved degree of self-care. Orem’s 35 theory of self-care refers to human behaviour that is self-directed and self-permitted. Self-care is a practical endeavour and needs to be deliberately engaged in by patients. 36 It requires knowledge and skills, and nurses promote these skills with ‘motivating self-care’ together with their professional competence and the patient’s lived experiences. 36 Research emphasizes the importance of focusing on young patients’ own goals, not what practitioners think is in their best interest. 37
Beauchamp and Childress 25 define ‘whether respect for autonomy of patients should have priority over professional beneficence directed at those patients’ (p. 176) as a central problem in biomedical ethics. Nurses hold professional obligations and are bound by policies, norms and organizational directives, which might conflict with individual obligations. 38,39 Psychotic symptoms, emotional distress and impaired cognition make individuals vulnerable and might disrupt reality-testing and decision-making capacity, 40 which complicates nurses’ commitment to the right to autonomy of a person experiencing psychosis. Obligations for individuals’ and society’s safety might also lead to paternalism, forcing patients to accept treatment.
Nurses’ striving for security might be perceived as a pessimistic attitude towards the views of individuals and their will to recovery. 37 Tait et al. 41 recommend services to aim to develop practical living skills and avoid dependence in young people, which might be a contradiction to ‘working behind the scenes’. Representing an individual and enabling the person to express what he or she wants is considered better than working behind the scenes in their best interest, which is considered an autonomous attitude; nurses should only speak on behalf of someone if requested. 39 The patients’ engagement in treatment in mental health centres is fundamental to reduce the impact of FEP on the individuals and their families, and to facilitate recovery. 41 When nurses ‘work behind the scenes’, there might be a risk of focusing on what they think is in the patient’s best interests, instead of the patient’s own personal goals. 41
Study limitations
The main theme in the focus group was FEP, but clinicians participating in the focus group also worked with young people with similar problems, not necessarily diagnosed with FEP, but sometimes with multiple psychotic episodes. It could be hard to distinguish between them in a focus group. Yet the current situation will not differ much.
We believe that greater emphasis on what patients value in FEP and their recovery would have strengthened the discussion. Another study involving patients and their relatives is now being planned.
Conclusion and implications
The intention of this study was to explore mental health nurses’ clinical work in a rural area CMHC, treating and caring for individuals experiencing FEP. The study shows that the nurses’ clinical practice is comprehensive. Treating and caring for individuals experiencing FEP demands an ethical awareness and great vigilance by nurses.
Nursing care is dynamic, and clinical work moves along continuums between autonomy and paternalism, and between ethically reflective and non-reflective practice. In this article, ‘working behind the scenes’ is considered as being in a paternalistic area containing an ethical reflection.
This study leads to a further question of how mental health nurses engage with patients in what should be a genuine, collaborative relationship. It highlights the distance between nurses and patients experiencing FEP, and the separation in the nursing relationship. This study is a contribution to reflection upon everyday nursing practice. However, more ethical reflection, insight into evidence-based nursing interventions and a higher consciousness of the nurse’s role are needed.
Listening to each individual, instead of telling him or her the truth, is essential when building a partnership. It is important that nurses offer help requested by the patient, not impose what they think is in the patient’s best interest. We need to become more aware of invisible work, and it is necessary to make invisible work visible.
Footnotes
Acknowledgements
We would like to gratefully acknowledge the research participants for their generous contributions.
Funding
This study is partly funded by a research grant from the Northern Norway Regional Health Authority and Nordland Hospital Trust (grant number PFP974-10).
Conflict of interest
The authors declare that there is no conflict of interest.