
Abstract
The aim of the present study was to describe how registered nurses in nursing homes ensure legal security, good and safe nursing care and uphold the dignity of nursing home residents with severe dementia without violating residents’ integrity. Semi-structured interviews were conducted with 10 charge nurses in a county in central Sweden. The transcribed interviews were examined using manifest and latent content analyses. The manifest analysis identified actual local routines involving coercive treatment and registered nurses’ descriptions of complications and alternative measures. The latent analysis resulted in three themes describing nursing strategies: one with coercive treatment, one with coercive treatment under specific circumstances and one to prevent coercive treatment. Interpretations of legal terms regarding coercive treatment and inadequate gerontological nursing training and understaffing seem to preserve the use of coercive treatment.
Introduction
There has long been a debate on how the legal security of people with reduced decision-making capacity can be ensured in dementia care. 1 All humans have constitutionally protected rights and freedom, 2,3 including the right to make their own decisions, unless there is a law restricting these rights. In everyday dementia care, there are severe ethical dilemmas, in that legitimate demands for good and safe nursing conflict with national and international legislations. 2 –4 In their everyday work, registered nurses (RNs) must balance between legislation and safe gerontological nursing, where preserving the dignity and integrity of older people with dementia is the aim of professional nursing. 5,6 Understanding when established constraints are to be perceived as an enforced physical violation or detention, and reflecting over existing norms and attitudes in care of older people, requires legal knowledge, competent staff, committed leadership and multi-professional teamwork. 1,7 –11
Historical background
Swedish studies 1,5 have revealed how coercive treatment regulations in municipal dementia care were used incorrectly. Physical restraints were used to a greater extent than permitted by legislation, and the decision to use such restraints had been made by professional healthcare staff other than physicians. More than one in four with dementia in Swedish nursing homes was restricted in their freedom of movement. 12 Preventing older people from falling is a high priority in nursing homes for dementia care, and one preventive measure has been physical restraint. However, a recent Swedish study aimed at reducing the use of physical restraint in nursing homes for dementia care showed no increased incidence of falls despite reduction of restraint practices. 13 Various types of coercive measures, such as mechanical and non-mechanical restraint, compulsion to take part in nursing and medical treatments or activities of daily life (ADLs), seem to be common practice in institutional care in most Western countries. 7,14 –19 Coercive measures have been associated with severe adverse effects. 12,14,17,18 Despite coercive measures’ harmful effect on quality of life, use of them is probably primarily based on lack of education and unawareness of alternative measures. 9,10,13,15,20
To enhance the legal security of persons with dementia in Sweden and to ensure the legitimacy of legislation, especially in situations involving physical violation and detention, a governmental commission was appointed. 1 New legislation, allowing coercive treatment in the care of older people with dementia, was proposed. But various Swedish public authorities and organizations 21,22 expressed their doubts as to whether this new legislation would reduce such treatment and increase their legal security. In 2010, the Swedish National Board of Health and Welfare declared invalid the regulation of coercive treatment for nursing home residents with dementia and for people on institutional somatic wards. 23 The Swedish Dementia Centre, 24 commissioned to further investigate the need for specific legislation, declared that adequate staffing, facilities and knowledge must be the top-priority principles in any future legislation. There is little current research on how the ethical dilemmas of coercive treatment in municipal dementia care are practically dealt with by RNs following abolition of the legislation on coercive treatment. There is thus a need for deeper knowledge of how RNs behave to enhance legal constitutional legislation 2,3 and to provide high-quality care for nursing home residents with dementia.
Study aim
The aim was to describe how RNs in nursing homes ensure legal security, good and safe nursing care and uphold the dignity of residents with severe dementia without violating residents’ integrity, after the National Board of Health and Welfare’s legislation on coercive treatment was abolished.
Method
Design
The study was qualitative and descriptive in design. 25
Definition of coercive treatment
Nursing and medical examinations or treatments, medications and social care interventions cannot be implemented through coercion or deception. 2,3,11 In the international literature, coercive treatment is defined in different ways. The definition used here is in accordance with the European Convention on Human Rights and Freedoms as well as with the Swedish Constitution. 2,3 All humans are protected against deprivation of liberty and disregard for privacy by public authorities unless there is a law restricting these rights. Swedish protection against detention 3 includes any physical violations or restraints that make it impossible to move freely, including mechanical restraints (e.g. a belt, bed rail and tray table) and non-mechanical restraints (e.g. locked doors, removal of mobility aid equipment, putting a table in front of a chair or leaning a wheelchair backwards to prevent freedom of movement). Electronic surveillance of various kinds without consent is regarded as a significant breach of privacy by a public authority. 2,3,11 In the following text, terms such as restraint and constraint will be used synonymously.
Settings and participants
The study location was a county in central Sweden. The participants were 10 Registered Nurses (RNs) working in 10 different nursing homes in a city and surrounding rural areas. Participants’ background characteristics are presented in Table 1.
Participants background data (n = 10).
SD: standard deviation.
Interviews
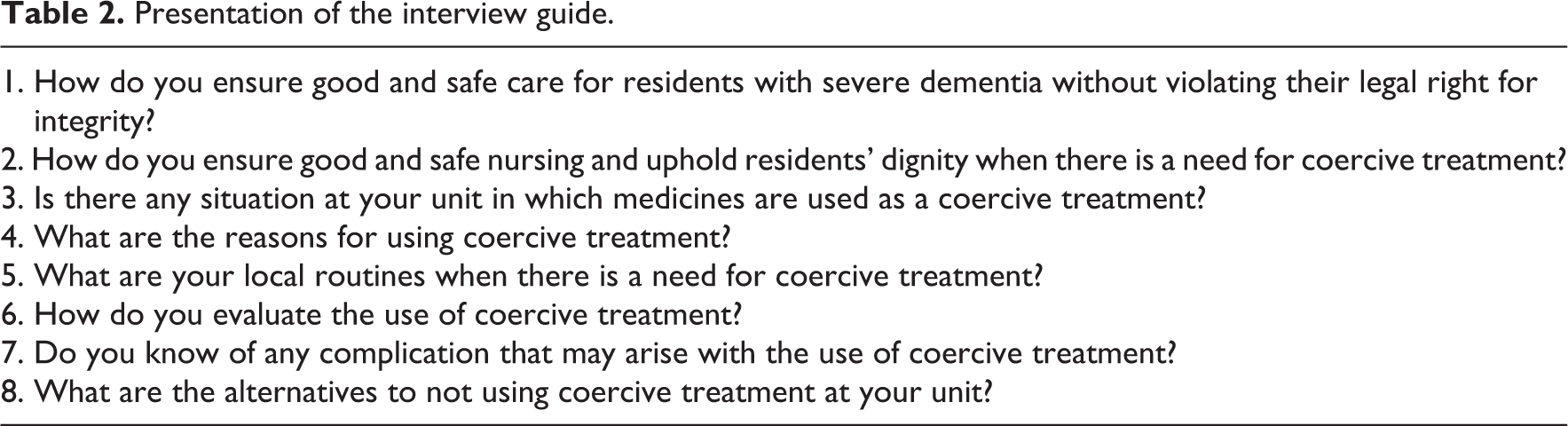
The interview method was chosen for data collection because it was judged to be simple, reliable and most suitable for this kind of study. The qualitative interviews were performed using an informal interview technique: a conversation focusing on the informant. Spontaneous follow-up questions were posed during the interviews. The interview guide is presented in Table 2. The semi-structured interviews were conducted by the first author (E.L.) in a separate room at participants’ respective workplaces during working hours. The interviews lasted between 30 and 60 min; they were audio-recorded and transcribed verbatim.
Presentation of the interview guide.
Data analysis
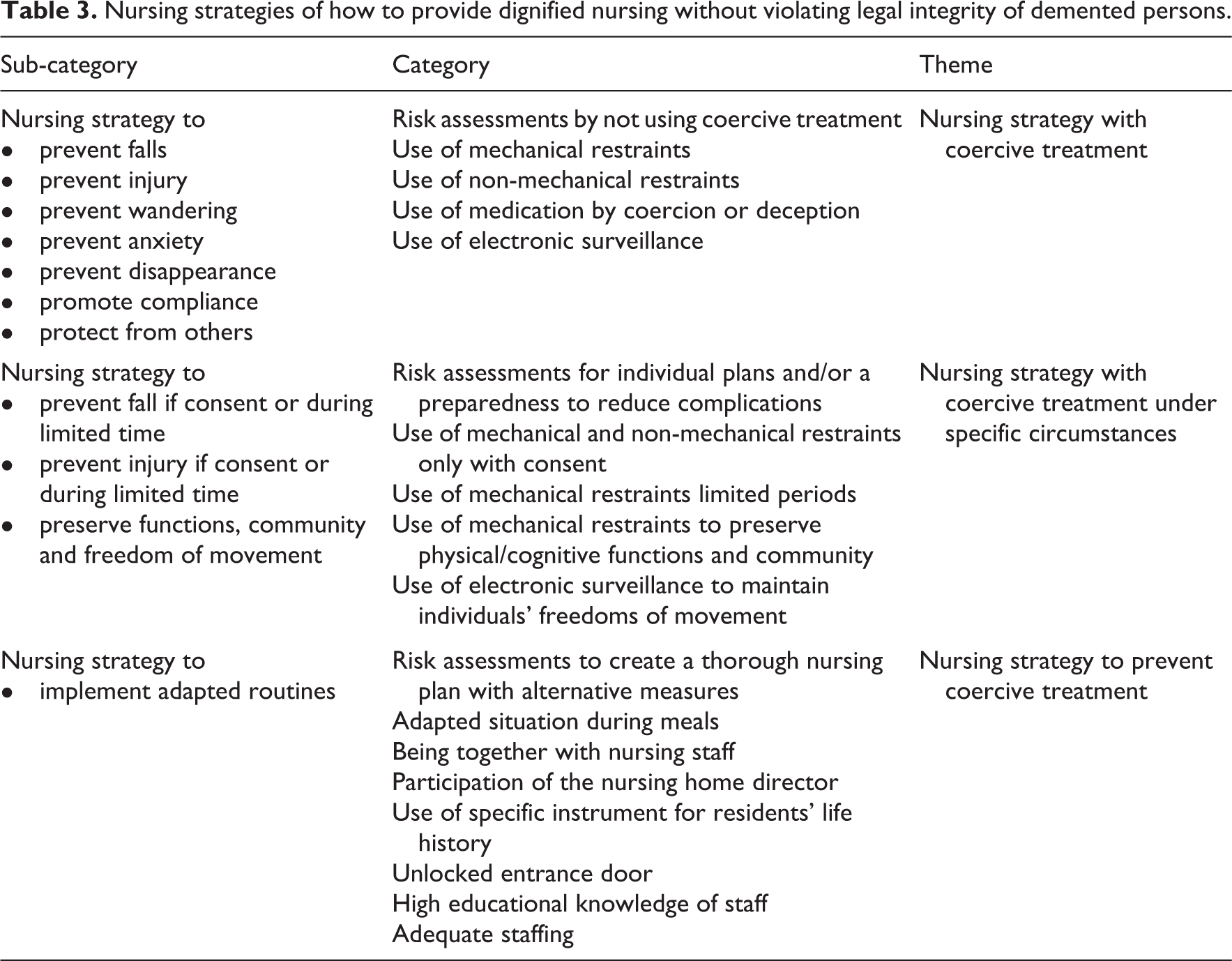
Both manifest and latent inductive content analysis were used. 25 The analysis began with reading the interview text several times to obtain an overall sense of the content. While reading the transcripts, similarities and differences in the text were observed. This phase was concrete and involved identifying the properties clearly evident in the text. The text content was divided into meaning units relevant to the aim of the study. These units were condensed on a descriptive level, keeping close to the text. In the next step, the units were combined into codes, where the descriptions were labelled on a more abstract level for the first time. After coding, the interview text was divided into two different units of analysis. Descriptions applying to questions 5–8 were grouped in categories describing the RNs’ descriptions of local routines, complications and alternative measures on a manifest level. Descriptions applying to questions 1–4 were further analysed using a latent inductive approach. The codes were combined into categories describing the nursing interventions used by the RNs in order to ensure good and safe nursing. The categories were divided into subcategories describing the reason behind the interventions. The sub-categories are not exclusive to one category only. Emerging from the latent analysis were three themes describing how the RNs ensure high-quality nursing without violating dementia care residents’ legal rights following the abolition of legislation on coercive treatment.
Ethical considerations
The formal approval of an ethics committee was not required according to the national directives. 26 However, the recommendations for research ethics in Sweden were followed. The nursing home directors and RNs received written oral information about the study, stating that participation was voluntary and that their responses would be treated confidentially. 27 Informed consent was obtained from all participants.
Findings
Three different nursing strategy themes emerged from the analysis. The themes concerned how to ensure high-quality nursing without violating dementia care residents’ legal rights following the abolition of legislation on coercive treatment (Table 3). Two nursing strategy themes involved coercive treatment. Specific guidelines for dealing with situations involving coercive treatment existed, but to a varying degree: some RNs reported a complete lack of written directives. The findings also include information on actual local routines (Table 4), RNs’ reports of related complications (Table 5) and six categories of alternatives to using coercive treatment (Table 6).
Nursing strategies of how to provide dignified nursing without violating legal integrity of demented persons.
Categories describing which staff perform risk assessments and decision-making and routines of evaluation.
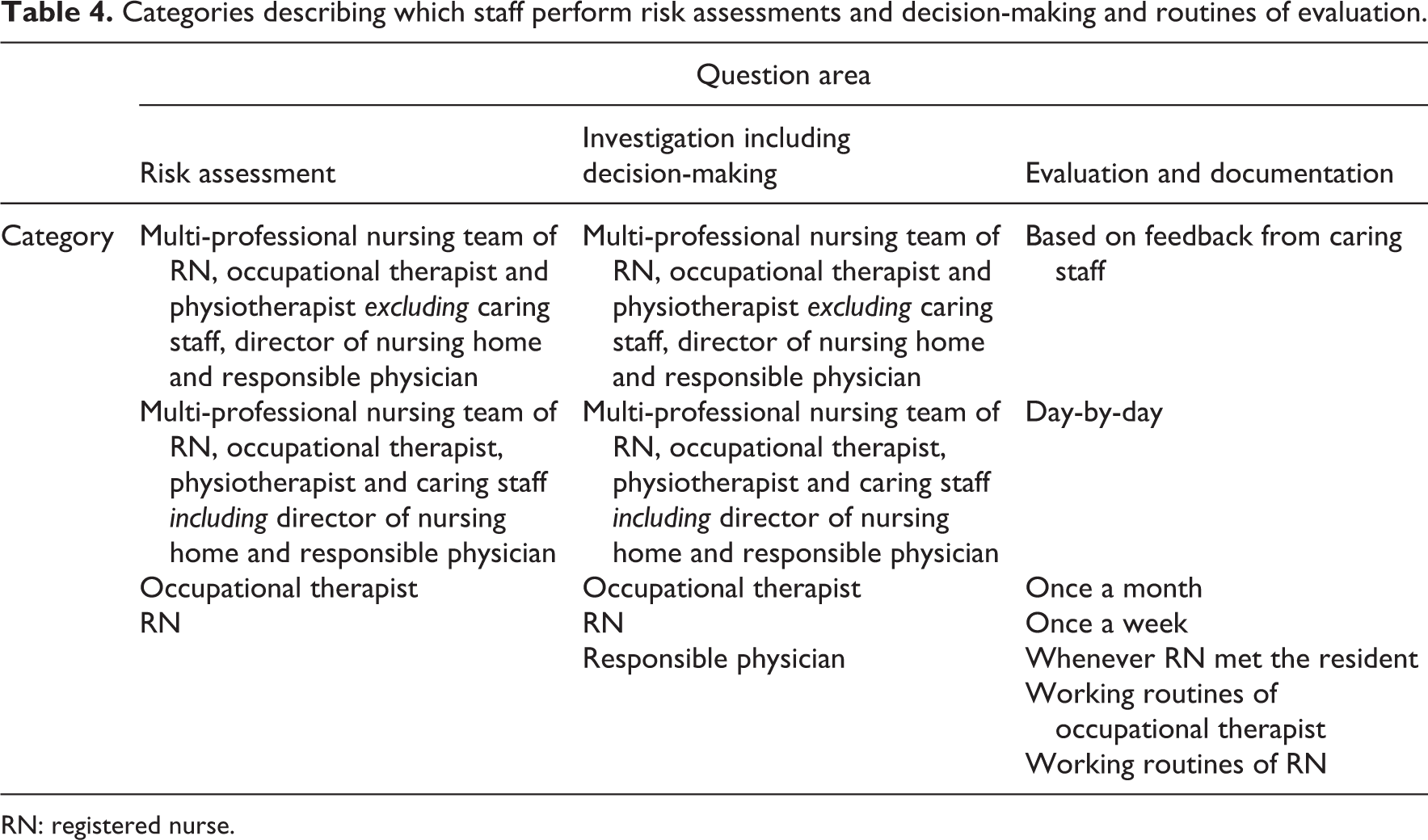
RN: registered nurse.
Categories describing complications related to coercive treatment.
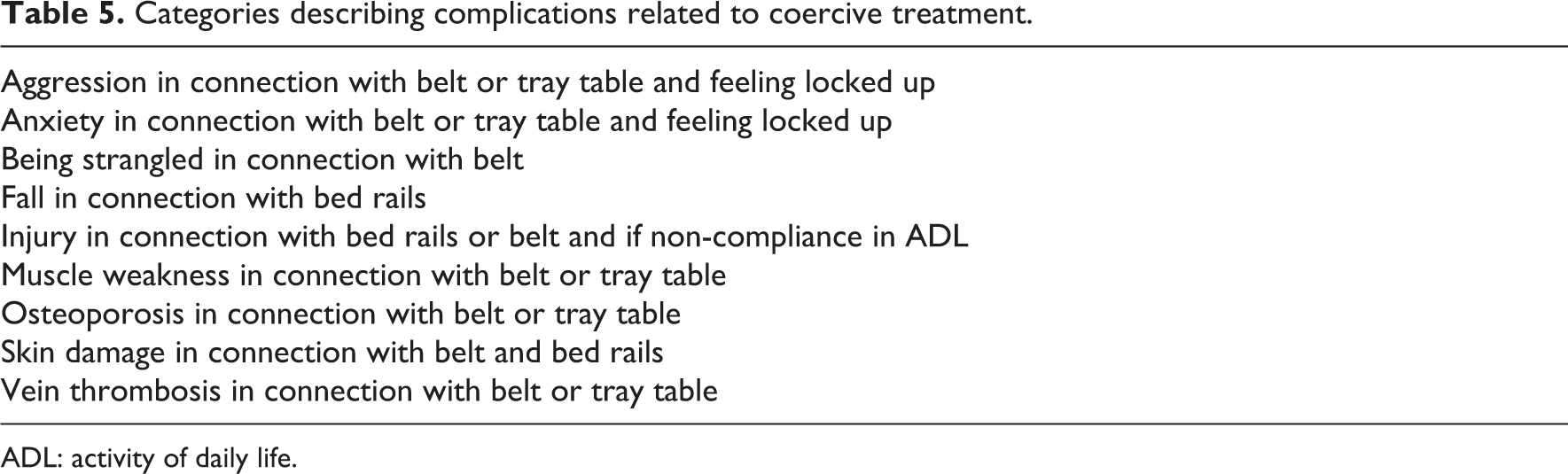
ADL: activity of daily life.
Categories and sub-categories describing alternative treatment.
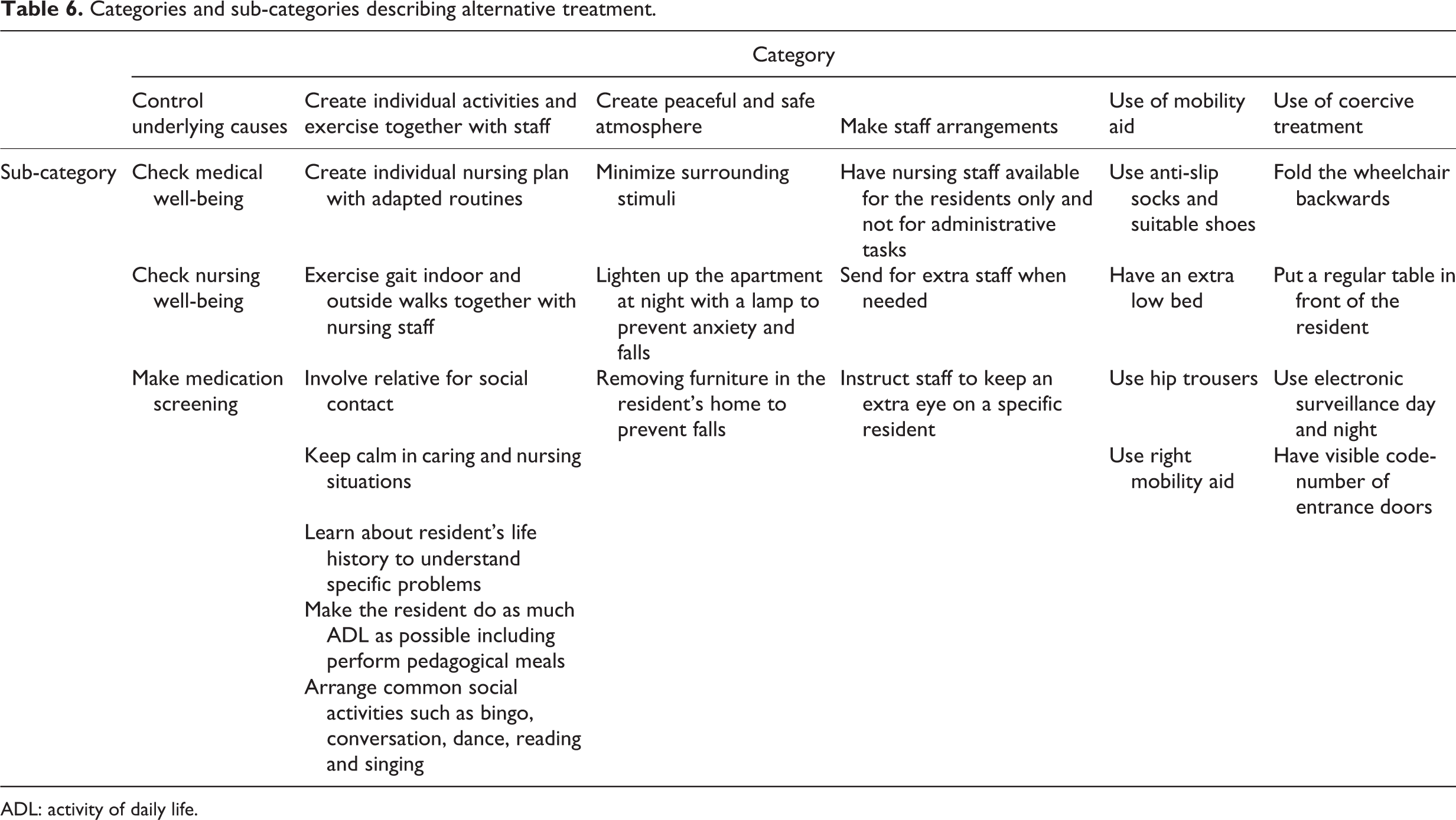
ADL: activity of daily life.
Nursing strategy with coercive treatment
If it’s about physical restraints, for example, belts, that’s what we’re allowed to use. Then we try to convince the resident to use it. When it’s about bed rails it’s even more difficult. We try to take their opinions into account … Then we have electronic surveillance, which you can’t use … but you can’t sit with them in their apartment, it’s for rapid transmission … And then the doors, we’re not allowed to lock them, but we would need one extra staff member for each resident otherwise ...
This strategy was seen as acting with good intention. The RNs could not see how these measures limited the residents’ freedom. The need for appropriate staffing, premises, facilities, knowledge and informed consent to avoid coercive treatment was not mentioned. There was also variation in their knowledge of what kinds of coercive treatment were seen as illegal and under what circumstances. Some RNs described how physical and chemical restraints could no longer be used in dementia care. They reported that belts, bed rails and electronic surveillance were no longer legal and said residents could not be forced to take their medication. However, when there was a potential risk of harm, they never mentioned obtaining consent from residents for the use of coercive treatment. The RNs also described trying to compromise or to persuade residents to use the proposed measures. Residents who long had physical restraints and had not verbally rejected the treatment were considered to have given their consent. When coercive measures were used, the RNs mentioned information provision to and collaboration with family members. However, when there was a risk of harm, family members’ opinions were not considered in the decision-making. The respective five categories of actual nursing strategies are described in the following.
Risk assessment by not using coercive treatment
At any risk of fall or harm, RNs described how risk assessment and subsequent investigation were achieved to verify the risk by not using coercive measures.
Use of mechanical restraints
The RNs saw belts, tray tables and bed rails as a necessity for senior safety. Residents who could not stand alone, and who were moved with lifting aids, used a belt to minimize the risk of falling. Those who had fallen previously, and who might get out of bed, were always prescribed bed rails. The RNs described how belts and bed rails, voluntarily initiated by the resident, gave the person a sense of calm. The use of restraints in wheelchairs allowed staff to leave residents unattended. The action was considered a safety matter, as the prescription was made by the family doctor and according to nursing home routines, although staff should supervise every 15–30 min. The RNs also described that residents were strapped in their wheelchair owing to understaffing. But during meals, they could sit in a chair without restraint, as at that time, there were sufficient staff on duty. According to some RNs, the consequences of falls and injury were much worse than the consequences of physical restraint.
Use of non-mechanical restraints
The RNs felt that doors with code-locks were indispensable for preventing injury. Code-locks provided assurance to staff and family members that nothing dangerous could happen. When residents felt trapped inside, the staff tried to distract them so they would forget they wanted to go out. To minimize constant wandering and falling and to create a peaceful atmosphere, the wards were divided by sliding doors. For residents with a friend on the other side, these doors were covered with a less transparent plastic film to minimize their anxiety and urge to see each other.
Use of medication by coercion or deception
The RNs described how legal social interventions had to be carried out with physical force if the resident resisted help with personal hygiene for a period of time. This was done even if the resident felt violated. To lighten the burden, the RNs tried to alleviate such feelings with sedatives. When residents refused to take prescribed medication, the RNs tried different methods of tricking them into swallowing the tablets. This could involve hiding tablets in food or putting dissolving tablets in the corner of the resident’s mouth. The RNs described they would never use violence and force, but by deceiving residents instead, safe nursing practices could be maintained. They also mentioned that residents with a tendency to wander at night were administered sedative drugs due to understaffing, without being told why.
Use of electronic surveillance
Electronic surveillance was used as a routine to protect other residents when individuals with severe dementia wandered around at night. The RNs talked about how electronic surveillance prevented falls and injury, as the detector signal was an indicator for staff to immediately run to the needy resident.
Nursing strategy with coercive treatment under specific circumstances
We have only one resident sitting in a wheelchair with a belt. She hasn’t been able to walk for several years, is spastic, kicks with her legs and slips out of her seat. And she can’t answer questions. We’ve told her she needs it so she won’t slide down onto the floor … She’s always with staff in our common rooms, but to be sure she doesn’t fall out of the chair, she has this belt. She feels safe with it, hasn’t tried to pull or tear it away and she doesn’t seem to be irritated. If she were, we would take it away immediately.
The RNs were aware of the non-legitimate status of coercive treatment, but still felt they had to use such measures in specific situations. They were also aware of the legal need for informed consent and conscious of some of the severe complications of these measures. Some described how specific nursing plans were made to minimize any risk of complications. The residents’ preferences and needs were the source of information when coercive treatment was proposed. When there was no possibility to get the resident’s consent or when he/she refused the use of any constraints, a meeting with family members (and if possible, with the resident) was always held. Information was always given on the assessed risk of not using constraints and on the nursing home’s working routines when staff could not be present at all times. In cases of risk of falling or injury or to maintain physical/cognitive functions, social community and promote freedom of movement, the RNs took time to explain to the resident why these limited measures meant safety. When the resident’s family member wanted physical restraint to be used, information on the family member’s wishes was given to the resident in the hope that he/she would understand why such a measure was needed. According to some RNs, family members did not have a legitimate role as legal representative, which meant that family could not dictate the use of coercive measures if staff were of another opinion. The respective five categories of actual nursing strategies are described in the following.
Risk assessment for individual plans and/or preparedness to reduce complications
The RNs described how, in cases of risk for harm, or when a new resident arrived, these assessments and investigations were used to create individual nursing plans to promote physical and cognitive functions, social community and freedom of movement with the use of coercive treatment. They talked about nursing plans to avoid complications when constraints were used. The RNs’ descriptions of complications related to coercive treatment are presented in Table 5. The RNs reported that risk assessment was done even if the resident herself or himself had insisted on using constraints.
Use of mechanical and non-mechanical restraints only with consent
Information on each individual’s needs and desires, personality and previous life experience was essential to RNs’ design of nursing. This was particularly true of daily nursing care and when coercive treatment was used, as the outcome of constraint had to be constantly re-evaluated. The RNs described how attention to the resident’s body signals and characteristics revealed how well he or she accepted the nursing care and allowed RNs to adapt to the individual’s preferences. According to several participants, it was obvious that one should ask residents’ permission about proposed nursing actions. In situations where physical restraint had been prescribed by a hospital doctor, the staff respected residents’ presumed reluctance to be restrained and their unwillingness to engage in ADL; the staff waited for residents to express their trust. Instead, staff assistance was given day and night.
Use of mechanical restraints for limited periods
At one nursing home, using physical restraint for residents in poor physical condition after severe injury due to previous falls was only allowed for a limited time, combined with a nursing plan to reduce residents’ feeling of being locked in the wheelchair.
Use of mechanical restraints to preserve physical/cognitive functions and community
RNs described how, to maintain physical and cognitive functions and preserve self-esteem, residents could be held in place with a tray table in their wheelchair during meals. Afterwards, this constraint was always removed. Use of a belt in the wheelchair allowed residents to participate in the social community despite severe physical disabilities.
Usage of electronic surveillance to maintain individuals’ freedom of movement
Electronic surveillance was described as a way to preserve residents’ freedom of movement and to enable nursing staff to rapidly assist in the event of a fall. Without surveillance, there was risk that residents would be left lying on the floor for longer periods, undetected by staff. One respondent described how the use of monitoring, such as global positioning system (GPS), helped to satisfy residents’ need to go out whenever they wished. With GPS, a necklace with identification, a telephone number and address and appropriate personnel assistance, the risk of residents disappearing was clearly diminished.
Nursing strategy to prevent coercive treatment
It’s very much about my role as a nurse. How I explain, how I support and show nursing staff how to behave towards residents showing anxious or aggressive behaviour, without giving sedative drugs. Because it’s all about how we approach residents with dementia. I do think we have a very important role as a nurse to support our staff and show them how to use individually adapted strategies.
Strategies described by these RNs to prevent constraints were preventive measures, such as obtaining information on residents’ life history, needs and preferences. This was an essential prerequisite for adapting appropriate strategies in dementia care nursing. Awareness of current legislation on human rights and freedom, together with the requirement for safe gerontological nursing, was somehow clear. They spoke of preventive strategies to avoid wandering, falling, anxiety and aggression and to fulfil residents’ wishes without using constraint. One RN spoke of the major challenge of drawing the right conclusions based on responsiveness, understanding of behaviour and mapping the problem, as well as of finding alternative measures. The respective eight categories of actual nursing strategies are described in the following.
Risk assessments to create a thorough nursing plan with alternative measures
Assessments and investigations were used not only to map risks and habitual daily routines, but also to create acute and long-term preventive nursing plans. This obligatory process had caused RNs to think about whether limitations really were necessary.
Adapted situation during meals
Pedagogical meals to assure the integrity of residents were emphasized, as good nutritional status was thought to reduce anxiety and thereby indirectly reduce wandering behaviour. Telephones were switched off during meals, and relatives were asked to come either before or after meals. Suitable language and topics of conversation during these meals were also thought to promote residents’ self-esteem.
Being together with nursing staff
To reduce the feeling of being locked up, nursing staff spent time with the residents. The RNs mentioned activities like walking, conversations and drinking coffee or looking at residents’ photo albums to reduce their anxiety. Activities in which all residents were gathered were not thought to promote their integrity or to be optimal nursing care. To prevent anxiety, activities should be planned individually and based on the residents’ own preferences.
Participation of the nursing home director
According to the RNs, the nursing home director played an important role in preventing violation of residents’ integrity. When the director was visible among staff at the ward, participated in daily work during lunchtime and promoted nursing care without constraints, all staff were encouraged to think and act like the director.
Use of specific instrument for residents’ life history
To avoid coercive treatment, RNs mentioned using narratives from residents’ life history. The instrument was seen as a tool for all nursing staff to establish an understanding of how to treat residents in a professional manner.
Unlocked entrance door
One respondent described that, to comply with legislation, the entrance door notified staff when someone tried to exit the unlocked door. The RNs described that the new legislation made it impossible to switch a broken code-lock on the entrance door. However, new routines for surveillance had been implemented. Every time the entrance door opened, a signal rang whereon staff immediately proceeded to the door to ensure that no residents were about to leave the ward.
High educational knowledge of staff
Staff’s knowledge of dementia care was described as solid. On the whole, staff knew how to respond and to distract anxious residents; they did not need to use force in caring situations. The RNs described that administration of sedative drugs to residents was rare, as they knew the pharmacological side effects. One RN emphasized the importance of being a good role model for other staff at the nursing home.
Adequate staffing
It was emphasized that sufficient numbers of physically available staff were needed to adapt nursing care to residents’ preferences and to avoid coercive treatment. Staffing was described as good, and staff surrounded the residents day and night. According to the RNs, single night staff had, for the most part, a good overview of the residents. There was no restriction on bringing in more night staff, as several residents wandered around at night. Because they were aware of the consequences of coercive treatment, evaluations were carried out to assure adequate staff assistance in situations entailing risk of harm to residents.
Local routines of coercive treatment
Guidelines on how to handle situations involving coercive treatment were uncertain, and there was variation in ideas about how practices of assessment, investigation, evaluation and documentation should be performed. Some referred to the Swedish National Board of Health and Welfare’s guidelines and/or local routines, but for the most part, there were no written directives at all. Table 4 shows which staff categories carried out risk assessments, decision-making and routine evaluations. Family members’ participation was described as important to keep well informed, although RNs also talked about residents’ family members’ position as non-legitimate. Nurses’ legal interpretation of this non-legitimate role meant that only staff could decide to use coercive measures, not family members alone.
Complications and alternative measures
RNs’ descriptions of complications related to coercive treatment are presented in Table 5. Most RNs had not experienced any of the complications mentioned. Six categories of alternative measures to limit the use of coercive treatment were extracted from the interviews, see Table 6.
Discussion
The findings reveal three themes describing different nursing strategies for ensuring legal security and high-quality nursing for older people with severe dementia, following abolition of Swedish legislation on coercive treatment. The choice of strategy could depend on the RNs’ knowledge of legislation, gerontological nursing and what constitutes adequate staffing to ensure human rights and freedom, topics dealt with in earlier studies. 5,9,10,13,16 However, all participating RNs based their actions on ethical considerations. Some RNs defended their actions, saying that coercive treatment was the right strategy and based on residents’ best interest. Previous international studies have revealed similar results. 5,28,29
There was a major difference between the two nursing strategies that included coercive treatment. This difference could be related to educational skills and/or adequate staffing. The RNs in both themes reported how preventing falls and injury was of utmost importance to maintain high-quality nursing. But RNs’ interpretations of legal rights varied between the categories. Within the theme ‘nursing strategy with coercive treatment’, the RNs reported that various types of constraints were prohibited, but did not feel these actions violated residents’ human rights and freedom. These RNs’ interpretations of informed consent also supported their obligation to prevent falls or harm using constraints, especially when residents could not express themselves verbally. This nursing strategy was also used when residents would not comply with hygiene routines. In such situations, their autonomy was overruled, despite the fact that there was no danger to life or health. As previous studies have shown, 4,7,12,15,16,19,28 RNs using coercive measures had convinced themselves that residents’ problematic behaviour was due to lack of insight, and therefore, constraints were seen as appropriate. It seems as though legal rights were understood as actions to prevent falls or harm, and not as actions to support autonomy and non-coercive dementia care. Similar results on nurse aids and licensed nurses were presented in an earlier study. 5 In the theme ‘nursing strategy with coercive treatment under specific circumstances’, RNs seemed to interpret legal rights as meaning informed consent prior to the use of coercive measures.
Just as a previous Swedish study may imply, 12 the RNs in the present study described how sedative drugs were used to decrease anxiety and wandering. They seemed to be unaware of patient-centred approaches to caring for older people. 30 –33 Moreover, there seems to be some uncertainty among RNs as to when such actions are to be seen as an enforced physical violation. 11 The RNs using coercive treatment explained that constraints were used in the cases of understaffing. However, previous international studies have shown conflicting results. In one study, staff level did not reduce the use of coercive treatment, 4 and in another, understaffing was a significant factor in promoting such treatment. 16
In the theme ‘nursing strategy with coercive treatment under specific circumstances’, the RNs prioritized the residents’ autonomy, but not non-coercive nursing care. Coercive measures were not only used to prevent harm, but they were also used to promote freedom of movement and residents’ self-esteem. When constraints were used to protect residents from harm, this was done only during limited periods and with the intention to diminish some known complications. However, the RNs did not describe all the severe complications associated with coercive treatment, 12,14,17,18 which may explain why they failed to evaluate all evidential complications regularly and to promote non-coercive nursing for residents with dementia. Nor were they aware of recent Swedish intervention study results showing that reduction in restraint use did not lead to increased incidence of falls. 13 The RNs using the strategy with coercive treatment did not pay attention to complications, which may indicate their unawareness.
The RNs represented in the theme ‘nursing strategy to prevent coercive treatment’ seemed to be aware of the complexity of situations involving constraint. They showed an understanding of the person-centred approach described in the guidelines on dementia care. 31,32 They spoke not only of educational skills and adequate staffing as important factors in preventing coercive treatment, as previously described by others, 9,16,34 but also of developing new working routines with unlocked doors and new technology. There was an awareness of the importance of gerontological nurses being part of daily care to promote non-coercive nursing care. 34 Acquiring information on residents’ nursing needs and personal preferences was an essential prerequisite for RNs who used preventive strategies to avoid violation of residents’ autonomy. In cases of understaffing, these RNs made use of the interventions described within the theme ‘nursing strategy with coercive treatment under specific circumstances’.
Overall, there was a variation in how situations involving coercive treatment were dealt with. Even at nursing homes where RNs used coercive treatment under specific circumstances, written local routines were non-existent. The extent to which different categories of nursing home staff were involved in assessment, investigation (including decision-making), evaluation and documentation varied. Among the RNs using both a preventive strategy and coercive treatment under specific circumstances, there were written guidelines with common routines for the multi-professional team. Their evaluations were made daily or once a week, depending on their working routines. Previous international studies have shown that joint working practices within a multi-professional team promote resident autonomy, high-quality nursing and medical care, as well as comply with preferences of residents with dementia. 9,16,34 Multi-professional teams could also encourage understanding of human rights and freedom, as such an approach would generate discussions among the whole team. 9,28,34 Despite their ability to describe alternative measures, the RNs still practice good and safe nursing with coercive treatment. Perhaps the lack of training in gerontological nursing, as revealed in the present study, may be one of the reasons for the preservation of coercive treatment. The RNs in the study did not see alternative measures as a way to promote resident safety and enhance legal rights.
The present study showed that it is difficult for RNs to balance resources, and that there is a need for individualized, high-quality, safe nursing. It also indicates that RNs in nursing homes may not have sufficient knowledge of legislation and ethical issues. Perhaps engaging in more ethical discussions in nursing homes could improve their knowledge. Having general discussions in the society about the ethical dilemmas associated with dementia care could improve awareness of the problems and facilitate understanding of the need for appropriate, educated staff as well as for adequate resources if we are to offer high-quality dementia care.
Use of a qualitative design was advantageous, as such an approach allowed the RNs to expand on the topics and to direct the conversation. During the interviews, most of the RNs answered the questions in detail, and they were very interested in sharing their experiences. A questionnaire could never give the same picture or deep description of their views as is provided by this kind of study. Investigating whether the present RNs’ experiences and opinions can be generalized requires a large sample and the use of quantitative methods. The present results could serve as a point of departure in designing a questionnaire about this topic.
When evaluating qualitative data, the concept of trustworthiness is important. Our intention was to use purposive sampling to ensure variation in the RNs’ ages and experiences. However, in practice, we were forced to use RNs who were willing to participate in the study, that is a convenience sample. The sample was drawn from different nursing homes and consisted of RNs of different ages and with varying experience, which can be considered a strength. 35 In the analysis process, the first author’s former practical experience of ethical dilemmas in dementia care and theoretical knowledge of the cultural phenomenon of coercive treatment enhanced the study’s credibility. However, the pre-understandings may be a disadvantage regarding interpretation of the findings. To demonstrate credibility, the analysis procedure was described in detail, and the article includes a thick description of the research context. Conformability was strengthened by providing a detailed description of the analysis process and illustrative quotations, and the findings can be viewed as trustworthy. 36 To strengthen dependability, analysis of the interview text was carried out by the first author and then validated by the other authors. Considering transferability, the results of this study may be applicable to other RNs, as they are in accordance with the previous knowledge of the cultural phenomenon of coercive treatment within nursing homes for people with dementia. 9,15 –17,19
Conclusion
Despite the de-legalization of coercive treatment in Sweden, the RNs still used constraint as a way to ensure good and safe nursing. The RNs’ interpretations of legal terms, important to understanding when coercive treatment is to be perceived as constraint, the lack of gerontological nursing in dementia care and inadequate staffing seem to preserve the use of coercive measures. Further research on person-centred care for people with dementia and on existing alternative approaches is needed to implement appropriate nursing strategies in the care of older people in nursing home residents with severe dementia.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.