
Abstract
We examined nurses’ perceptions of the ethical climate of their workplace and the relationships among the perceptions, medical error experience and intent to leave through a cross-sectional survey of 1826 nurses in 33 Korean public hospitals. Ethical climate was measured using the Hospital Ethical Climate Survey. Although the sampled nurses perceived their workplace ethical climate positively, 19% reported making at least one medical error during the previous year, and 25% intended to leave their jobs in the near future. Controlling for individual and organizational characteristics, we found that nurses with a more positive perception of the ‘patient’ dimension of ethical climate were less likely to have made medical errors. Nurses with a more positive perception of the ‘patient’, ‘manager’, ‘hospital’ and ‘physician’ dimensions of ethical climate were less likely to leave their current job. Enhancing workplace ethical climate could reduce medical errors and improve nurses’ retention in public hospitals.
Introduction
With rapid advancements in therapeutic technologies and pharmacological interventions in healthcare, the number of moral and ethical issues experienced by healthcare professionals is escalating in uncertain, complex clinical situations, along with limitations in the amount of healthcare resources. 1 Workplace ethical climate – employees’ perceptions of an organization’s conditions and practices that affect the way various problems with ethical implications are handled 2,3 – has received increased attention as an important contextual factor for ethical decision-making and practices.
Ethical climate affects moral distress, job satisfaction and turnover in nurses. 4 –8 Ethical climate is considered a significant antecedent of unethical intention and behaviour such as unsafe care. 9 In addition, nurses’ experience of medical errors results in intent to leave their profession. 10 However, to the best of our knowledge, no study has identified an explicit association among ethical climate, medical error experience and turnover of nurses in hospitals.
Against this background, the purpose of the present study was two-fold: (a) to examine nurses’ perception of the ethical climate in their workplace and (b) to explore relationships among nurses’ perceptions of ethical climate, their medical error experience and their intent to leave. Specifically, we investigated the relationship between ethical climate and medical errors as well as how ethical climate and medical errors affect intent to leave. This study provides an insight on which aspects of ethical climate need to be enhanced for ethical decision-making and practices. The findings will provide a better understanding of ways to improve patient safety and nurses’ retention in hospitals.
Background
Ethical climate
Workplace ethical climate represents the organization’s policies, procedures and practices on ethical issues, and it influences employees’ attitudes and behaviour and serves as a reference for employee behaviour. 2,3 Ethical climate is defined as individuals’ perception of how ethical issues in their work environment are handled. 11 This construct has multiple dimensions. For instance, Cullen and Victor 12 suggested nine types of theoretical ethical climates with two dimensions of ethical theory and locus of analysis. Olson, 11 with focus on ethical climate in hospitals, suggested five ethical climate dimensions related to colleagues, patients, managers, hospital and physicians. For the purpose of this study, we adopted Olson’s conceptualization of hospital ethical climate.
Ethical climate is closely related to moral distress. Moral distress – the experience of serious moral compromises in practice according to one’s accepted professional values and standards 13 – is shaped not only by the characteristics of individuals but also by the organizational and structural contexts within which the individuals are working. 13 Furthermore, moral distress negatively affects nurse and patient outcomes, including making nurses leave their profession or provide unsafe, low-quality care. 4,14 –17 Several studies have found that the morally distressing situations that nurses face were most often linked to organizational factors, including inadequate staffing and hierarchical structures. 15,17,18 Recently, the importance of structural and organizational factors that shape the experience of nurses’ moral distress in the workplace has been emphasized, 13,17,19 and thus, researchers have highlighted organizational factors, including ethical climate, in order to prevent and reduce moral distress and its negative consequences. Nurses’ perception of ethical climate is inversely related to moral distress. 4,7,8,16
Individual and organizational characteristics affect ethical climate. 3,20,21 For instance, nurses’ perception of ethical climate varied by their age, hospital type and care units where they work. 20 In addition, researchers have suggested that department-level and hospital characteristics such as ownership, teaching status and geographical regions influence ethical climate. 3,21 However, the majority of previous studies did not take organizational variables into consideration when investigating ethical climate. 5,6,21 Thus, we included these individual and organizational variables in our exploration of ethical climate across various healthcare organizations in order to compare our work with previous findings.
Relationship between ethical climate and medical error experience
With the current emphasis on patient safety, the reduction of medical errors has been a major challenge that healthcare professionals face. A substantial proportion of inpatients have experienced medical errors in hospitals. 22,23 A medical error refers to an adverse event or near miss that threatens patient safety. A qualitative study showed that the occurrence of medication errors was linked to ethical issues such as the management of patient harm and respect for persons involved in the error. 24 Morally distressing situations have resulted in poor-quality and unsafe patient care. 15,17 Workplace ethical climate is considered a significant antecedent of unethical behaviour such as unsafe care. 9 Thus, ethical climate in the workplace may be linked to the occurrence of medical errors due to unsafe behaviours, such as the commission of incorrect acts or omission of acts in the delivery of healthcare. However, there is lack of empirical studies on the relationship between ethical climate and the occurrence of medical errors.
In addition, previous studies in nursing have shown that the occurrence of medical errors, including medication errors, are associated with nurses’ age, gender, years of nursing experience, clinical departments, type of facility, geographical location of the hospitals where nurses work and so on. 25 –28 Therefore, the relationship between perceived ethical climate and medical error experience after controlling for these variables needs to be explored.
Relationship of ethical climate and medical error experience with nurses’ intent to leave
Retention of qualified nurses is important for high-quality nursing care and patient safety. As nurse shortage has received increased attention globally, strategies for retaining nursing staff are urgently required. 29 Intent to leave is considered a proxy indicator to predict nurses’ actual turnover. Several studies have shown that ethical climate influences retaining nurses in competitive healthcare settings. Hart 5 found that hospital ethical climate was most important in explaining nurses’ positional and professional turnover intention. Ulrich et al. 6 reported a negative relationship between ethical climate and turnover intention. However, in order to support nurses’ retention, it is critical to investigate which dimensions of hospital ethical climate have greater influence on turnover intention among nurses.
In addition, medical error experience is considered a factor affecting nurses’ intent to leave. However, there are inconsistencies in current findings regarding the relationship between experience of medical errors and intent to leave in nurses. 10 Several studies have found that nurses involved in medical errors experienced emotional distress such as anxiety and guilt; such experiences resulted in intent to leave. 30,31 However, a qualitative study found that experience of medical errors in most nurses did not result in their intent to leave. 32
Furthermore, in one study, a substantial proportion of nurses surveyed reported that they and other nurses had made clinical errors and experienced untoward clinical incidents, and they felt moral distress as a result. 18 In other studies, 15%–45% of the nurses in the samples reported having left or considered leaving a position due to moral distress. 4,14,16 Similarly, qualitative studies have found that unsafe, poor-quality care that occurred in morally distressing situations, including medical errors, contributed to nurses’ leaving their profession. 15,17 Thus, the need for empirical research on the relationship between medical error experience and nurses’ intent to leave, along with ethical climate, is justified.
Therefore, we investigated the relationship of nurses’ perception of ethical climate and medical error experience with their intent to leave. In this investigation, we controlled for individual and work environment characteristics that have been known to be associated with these studied variables, such as nurse age, gender, educational level, years of nursing experience, workplace, employment type, workload and hospital type. 33 –35
Methods
Design
A cross-sectional survey design was employed. This study was conducted as part of a large research project on the patient safety and work environment in hospitals. Findings of related studies on individual and work environment characteristics and error occurrences and work-related injuries have been published elsewhere. 27,36
Study settings and participants
The target population was nurses in 33 out of 40 regional public hospitals (RPHs) in South Korea, which refer to public hospitals at the county or city levels. They have played major roles in ensuring accessibility to comprehensive healthcare, including emergency care, rehabilitation, long-term care, hospice and infectious disease care, especially for vulnerable populations in each administrative geographical area. 27,37 The nurses worked in three 8-hour shifts. At the time of the study, there were 2358 eligible nurses, all of whom we surveyed. This sample size was considered sufficient to achieve stability in the parameter estimates according to the recommendation that the number of cases for each predictor in a logistic regression model ranges from 10 to 20. 38
Variables and instruments
Nurses’ perception of ethical climate was measured using the Hospital Ethical Climate Survey (HECS) developed by Olson. 11 Permission for use of the questionnaire was obtained from the original developer. The HECS consists of 26 items and has five subscales of perceptions regarding the relationships with peers (4 items), patients (4 items), managers (6 items), the hospital (6 items) and physicians (6 items). 11 The scale was translated into Korean by the first author (J-I.H.), and the translated version was subsequently validated by an English professor in a university academic centre. In this review, we focused on translating the exact meaning through comparison between the English and Korean versions of the HECS. The translated scale’s content validity and relevance in Korean hospital settings, along with the fluency of the translation, were reviewed by a bilingual nursing professor and two researchers in the Center for Public Healthcare (CPH), National Medical Center under the Ministry of Health and Welfare. Next, the items were pretested for clarity and readability by two head nurses, two registered nurses and a researcher in the CPH. No adaptations with regard to a Korean context were judged to be necessary. The items were rated on a 5-point Likert scale (1 = ‘strongly disagree’, 5 = ‘strongly agree’). A higher score indicated a more positive perception of ethical climate. The overall HECS had high internal consistency reliability (Cronbach’s alpha = .95). The Cronbach’s alpha coefficients for the five subscales were .89, .75, .95, .82, and .92, respectively.
Nurses’ error experience was measured using one item to indicate whether they had experienced any medical errors in the last year (1 = yes, 0 = no). Intent to leave was measured by a single item – ‘Would you like to leave your current job in the near future?’ – with a simple response of yes or no.
In addition, we collected data on nurses’ characteristics such as age, gender, marital status, educational level, year of experience as a nurse, employment type, job position and departments where they work. As organizational characteristics, we collected data on variables such as nurse staffing levels, hospital type, ownership, bed size, teaching status and location. Nurse staffing levels were formally determined by the ratio of the number of patient beds per nurse. This is classified into seven levels: from 1 (less than 2.5 patient beds per nurse; the highest level) to 7 (6.0 or more patient beds per nurse; the lowest level). The study hospitals had Level 4 (3.5 to less than 4.0 patient beds per nurse), Level 5 (4.0 to less than 4.5 patient beds per nurse), Level 6 (4.5 to less than 6.0 patient beds per nurse) or Level 7 (6.0 or more patient beds per nurse).
Data collection and procedures
We prepared questionnaires according to the number of staff obtained from the RPH Profile. 37 We sent the questionnaires with return envelopes to the public healthcare planning department at each study hospital. Through intra-hospital communication channels, we invited nurses to participate in the survey. Staff in the public healthcare planning department distributed the questionnaire with return envelopes to nurses via representatives at unit or department levels. These questionnaires were distributed to nurses who agreed to participate in the study. The staff in the public healthcare planning department then collected the sealed questionnaires from the nurses after completion, again through representatives at the unit or department levels, and mailed them to the research team. A reminder notice was given to nurses in order to collect the completed surveys, approximately 2 weeks after the distribution of the questionnaires. Nurses were asked to indicate the level of agreement on each item.
The return of completed questionnaires was considered as consent to participate in the study. Participation was on a voluntary basis, and the confidentiality of responses was guaranteed. Data on the hospitals’ characteristics were collected from the RPH Profile. 37
Ethical considerations
Formal research approval was obtained from the CPH and each study hospital. Questionnaires, with a cover letter explaining the study purpose and data confidentiality and encouraging nurses’ voluntary participation, were mailed to the hospitals that agreed to participate in the study. The anonymity of participants was guaranteed.
Data analysis
Data were analysed using SAS version 9.2. Internal consistency reliability of the HECS was measured using Cronbach’s alpha coefficients. General characteristics of participants, perceived ethical climate, medical error experience and intent to leave were summarized using descriptive statistics. Univariate analyses to identify any differences in the nurses’ error experience and intent to leave according to individual and organizational characteristics were performed using chi-square tests. Student’s t-tests were used to examine differences in ethical climate scores between two groups of nurses: (a) those with medical errors and those without an error and (b) those with and without intent to leave. Finally, in order to determine the relationship of perceived ethical climate with nurses’ medical error experience and the relationship of perceived ethical climate and medical error experience with nurses’ intent to leave, multiple logistic regression analyses were used. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. The threshold for statistical significance was set at .05, and all significance tests were two-tailed.
Results
Of 2358 nurses in 33 RPHs, 2116 nurses returned the questionnaire. However, only the 1826 questionnaires with complete responses (valid response rate = 77.4%) were used for analysis.
General characteristics of participants and ethical climate
The general characteristics of the participating nurses are shown in Table 1. Most (n = 1447; 79%) worked at general hospitals, 53% (n = 963) worked at intern training hospitals and 86% (n = 1575) were employed at regional medical centres. A total of 43% (n = 785) were employed at hospitals with 150–299 beds, and 70% (n = 1282) worked at hospitals in smaller cities. Of the participating nurses, 64% (n = 1167) worked at Level 6 hospitals and 49% (n = 902) in general care units. Most (99.5%) were female with a mean age of 31.1 (standard deviation (SD) = 7.0) years. They had an average of 8.4 (SD = 6.7) years of nursing experience. This red-lined sentence is moved after the yellow–marked sentence, along with the change of the order of the description. (Table 1).
General characteristics of participants and perceived ethical climate.
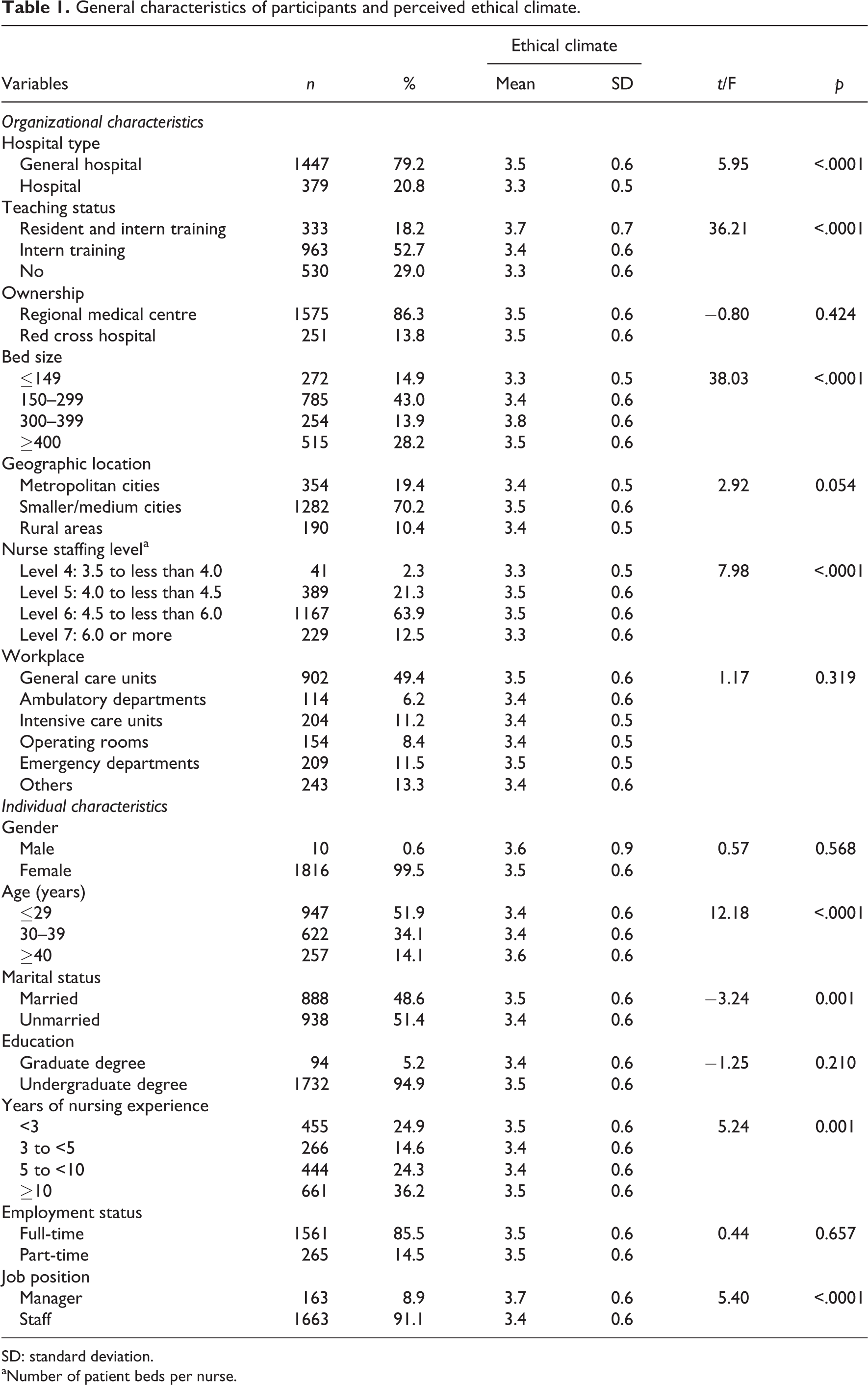
SD: standard deviation.
aNumber of patient beds per nurse.
The mean score on the HECS was 3.5 (SD = 0.6) on a 5-point Likert scale. The mean scores for the five subscales of the HECS, namely, peers, patients, managers, hospital and physicians were 3.7 (SD = 0.7), 3.6 (SD = 0.6), 3.8 (SD = 0.8), 3.3 (SD = 0.6) and 3.0 (SD = 0.8), respectively. Student’s t-tests showed significant differences in the overall scores on the HECS according to nurses’ age, marital status, years of nursing experience and job position, along with the hospital type, teaching status, bed size and nurse staffing level of the hospital where nurses work.
Nurses’ medical error experience and intent to leave
Of the 1826 nurses who comprised the final sample of this study, 19% (n = 351) reported having made at least one error in the previous year. Chi-square tests revealed significant differences in nurses’ experience of medical errors according to their age, marital status and years of nursing experience, along with the hospital type, bed size and geographical location of the hospital where the nurses work. There were significant differences in the overall and subscale scores for HECS between nurses who had made medical errors and those who did not (Table 2).
Nurses’ medical error experience and intent to leave by general characteristics.
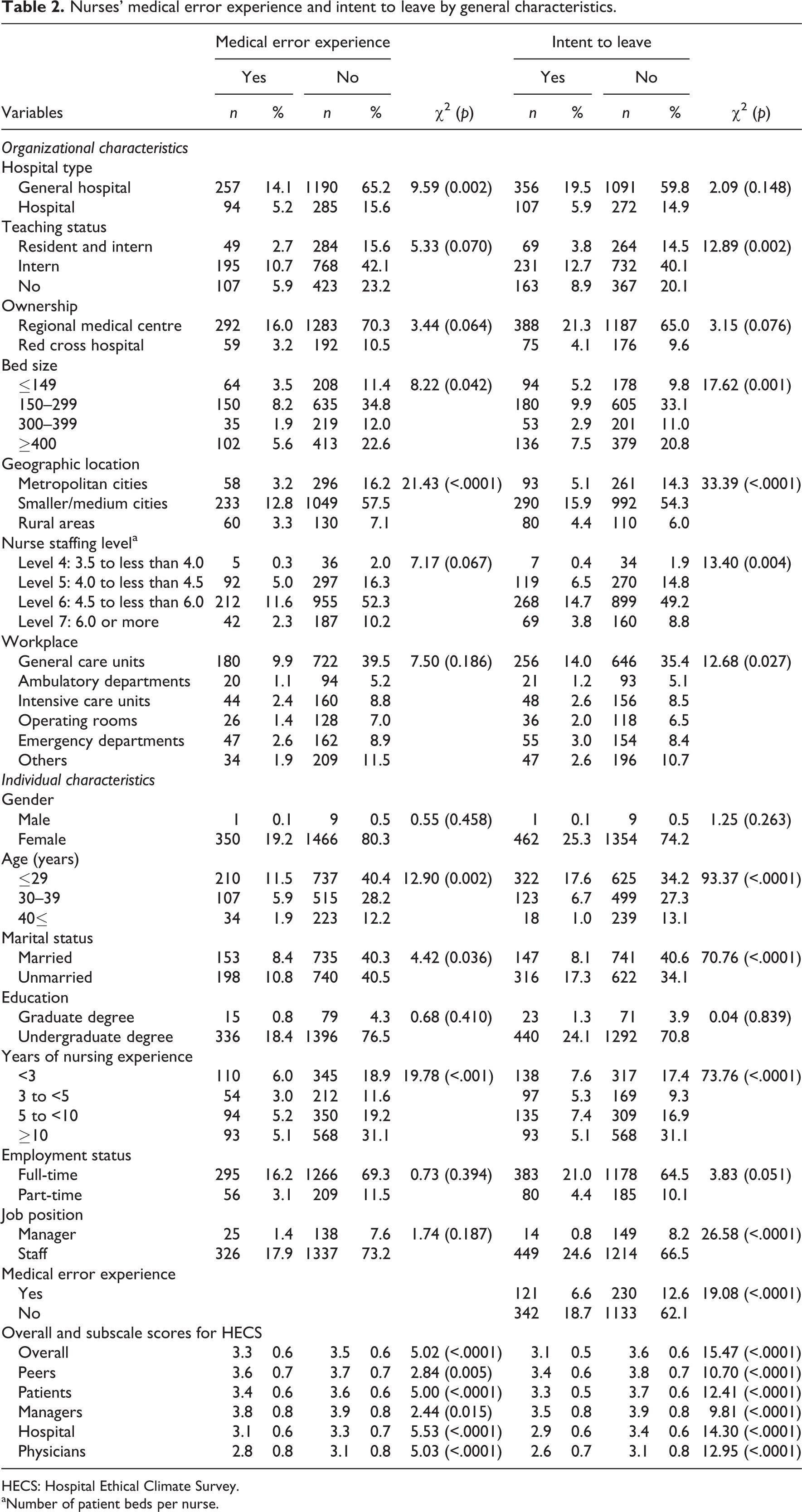
HECS: Hospital Ethical Climate Survey.
aNumber of patient beds per nurse.
In all, 25% (n = 463) reported intent to leave their current job in near the future. Chi-square tests revealed significant differences in nurses’ intent to leave according to their age, marital status, years of nursing experience, job position and medical error experience, along with teaching status, bed size, geographical location, nurse staffing level and workplace of the hospital where the nurses work. The overall and subscale scores for the HECS differed significantly between nurses with and without intent to leave (Table 2).
Relationships of ethical climate with medical error experience, and relationship of ethical climate and error experience with intent to leave: multivariate analyses
After controlling for individual and organizational characteristics based on prior research findings, logistic regression analysis was performed for medical error experience as a dependent variable in order to explore the relationship between ethical climate and experience of making medical errors (−2 log L = 1692.0, chi-square = 95.4, p < .0001). Only the ‘patient’ dimension of the HECS was significantly associated with the occurrence of medical errors. Nurses who had a more positive perception of ethical climate related to patients were less likely to have made medical errors (OR = 0.68, 95% CI = 0.51–0.92) (Table 3).
Logistic regression results for nurses’ medical error experience and intent to leave.
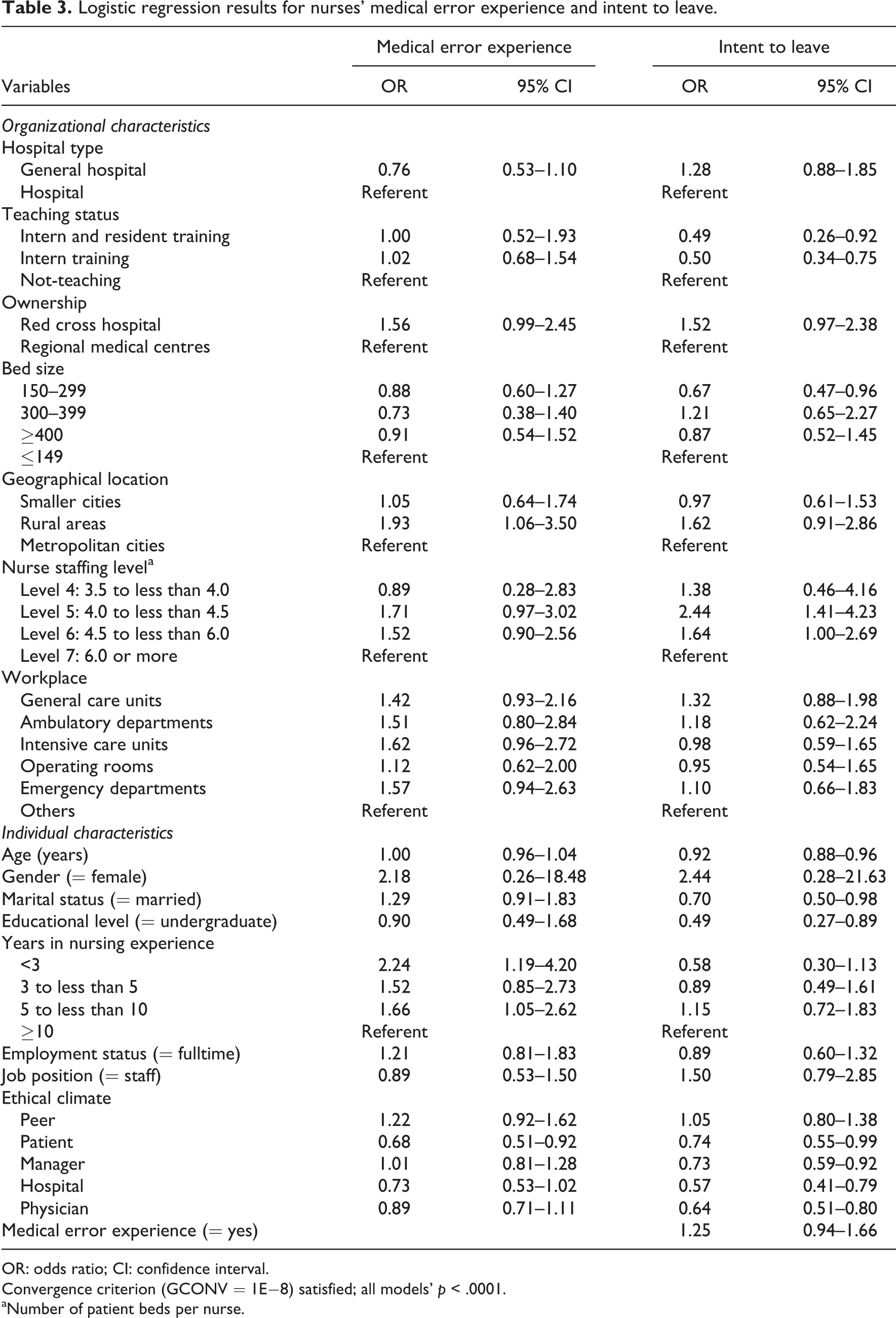
OR: odds ratio; CI: confidence interval.
Convergence criterion (GCONV = 1E−8) satisfied; all models’ p < .0001.
aNumber of patient beds per nurse.
Logistic regression analysis with intent to leave as a dependent variable was performed after adjusting for individual and organizational characteristics in order to examine the relationship of ethical climate and error experience with intent to leave (−2 log L = 1698.7, chi-square = 369.1, p < .0001). The ‘patient’, ‘manager’, ‘hospital’ and ‘physician’ dimensions of the HECS were significantly associated with nurses’ intent to leave. Specifically, nurses who had a more positive perception of ethical climate related to patients were less likely to leave their current job (OR = 0.74, 95% CI = 0.55–0.99). Those who had a more positive perception of ethical climate related to managers were less likely to leave their current job (OR = 0.73, 95% CI = 0.59–0.92). Nurses with a more positive perception of ethical climate related to hospital were less likely to leave their current job (OR = 0.57, 95% CI = 0.41–0.79). Those who had a more positive perception of ethical climate related to physicians were less likely to leave their current job (OR = 0.64, 95% CI = 0.51–0.80). Nurses’ error experience was not significantly associated with their intent to leave (Table 3).
Discussion
Ethical climate is one of the constitutional elements of ethical decision-making. An ethical work environment provides a context for professional nursing care. To the best of our knowledge, this is the first study to investigate the relationships among nurses’ perception of ethical climate, medical error experience and intent to leave in public hospitals. The findings indicate that nurses’ perception of ethical climate differed by individual and organizational characteristics. Ethical climate was significantly related to nurses’ medical error experience and intent to leave, and such relationships varied by dimensions of ethical climate.
Regarding ethical climate in Korean public hospitals, nurses had positive perceptions regarding the ethical climate of their work setting. This finding was similar to results from previous studies. 6 –8 However, the total mean score on the HECS was slightly lower than that of previous studies. 6,7 In particular, the score for the ‘physician’ dimension of ethical climate was lowest. This indicates the necessity for improved collaboration between nurses and physicians. Patient care in hospitals is provided by a team in which nurses and physicians are major players. Therefore, the ethical climate for promoting mutual support and respect between nurses and physicians and shared decision-making in patient care should be enhanced.
The nurses’ perceptions of ethical climate differed by various individual and organizational variables. Nurses aged 40 years or older and who were married, were managers and had accumulated less than 3 years or 10 years or more of nursing experience had more positive perceptions of ethical climate. Notably, these results were different from a previous finding that nurses aged 18–22 years perceived ethical climate more positively than those aged 23 years or more. 20 Additionally, in this study, the nurses in general hospitals and teaching hospitals for training interns and residents had a more positive perception of their workplace ethical climate than the others. Nurses in hospitals with 300–399 beds and with nurse staffing Levels 5 and 6 perceived ethical climate more positively than nurses in other settings. This finding provides evidence that organizational characteristics are the antecedents of ethical climate. 3 However, nurses’ perception of ethical climate did not significantly differ with respect to the care units where nurses worked, unlike in a previous study. 20 This inconsistency might be related to differences between the studied hospitals. The workplace ethical climate reflects organizational policies, procedures and practices. 2,3 Korean RPHs are small or medium-sized hospitals, and all the public hospitals in the present study had computerized hospital information systems, including provider order entry systems. Accordingly, their policies, procedures and practices could be shared efficiently and effectively across the work units, which might have resulted in improved interdepartmental communication. Thus, only hospital-level characteristics such as hospital type, nurse staffing level, teaching status and bed size were influential factors affecting nurses’ perception of their workplace ethical climate in this study.
Regarding the relationship between ethical climate and the occurrence of medical errors, nurses with a more positive perception of the ‘patient’ dimension of ethical climate reported having committed fewer medical errors. This finding supports the suggestion that ethical climate is an antecedent of unethical behaviour such as unsafe care. 8 In addition, this result can be interpreted within the contexts of previous research findings, which indicated that a positive ethical climate contributes to less frequent occurrences of morally distressing situations, 4,7,8,16 thereby reducing the occurrence of unsafe, low-quality care. 15,17 This finding provides evidence that an ethical climate, with emphasis on patient-centred care evinced by, for example, respect for patients’ expectations and shared decision-making for and with patients, is important to ensure patient safety. Hospital ethical climate can be enhanced by increasing patients’ awareness of the care they are provided, by respecting patients’ wishes and by encouraging nurses to seek access to and utilize relevant information for patient care. 11 These efforts will contribute to reducing the occurrence of medical errors in nursing practice.
Regarding the relationship of nurses’ perception of ethical climate and medical error experience with their intent to leave, the four dimensions of ethical climate were significantly associated with nurses’ intent to leave. This was similar to the findings of previous studies showing the inverse relationship between ethical climate and intent to leave. 5,6 We performed additional analysis of the relationship between ethical climate and intent to leave, after excluding medical error experience from the logistic regression model. The same result was obtained, indicating that the four dimensions of ethical climate were significantly related to intent to leave, all in the same direction. This finding indicates that ethical climate pertaining to patients, managers, hospital and physicians should be promoted to improve nurses’ retention in hospitals. Therefore, the work environment should enable nurses to meet patients’ needs by using relevant information, receive support from their managers and hospital and actively participate in shared decision-making for patient care with physicians. However, nurses’ medical error experience was not a significant factor influencing their intent to leave. This finding was similar to that of a qualitative study, wherein most nurses did not consider leaving the profession because of their medical errors. 32 However, it contradicts other reports that nurses had intent to leave after experience of medical errors. 30,31 One possible explanation for this inconsistency is that in the present sample of nurses, their medical errors might have resulted in no patient harm or very minor adverse events. Such events are less likely to affect nurses’ intent to leave. Another explanation could be that the nurses in the present study might have handled mistakes in a constructive and healthy manner as meaningful learning experiences. 32
Overall, the present study found that a positive ethical climate prevailed in public hospitals. However, this study indicated that the ethical climate dimension related to physicians needs to be improved. As such, a collaborative approach between nurses and physicians – characterized by trust and shared decision-making in the treatment decision for patient care – needs to be encouraged. In addition, ethical climate was a significant factor associated with nurses’ error experience and their intent to leave. The ‘patient’ dimension of ethical climate was a common factor influencing both error experience and intent to leave. Therefore, strengthening hospital ethical climate will contribute to improved patient safety and retention of nurses. In particular, hospital executives and nurse managers need to encourage nurses to use relevant information for patient care and make ethical decisions with and for their patients. Such efforts should include meeting the needs of patients, receiving and giving support and information with the workgroup and working as a team with a standard for behaviour. 39
Study limitations
This study has several limitations. First, it was conducted in only 33 public hospitals, even though it included 83% of all RPHs in Korea. Therefore, the generalization of the findings is limited. Second, we measured experience of medical errors by using a questionnaire. Thus, recall bias is possible. Third, the issue of common method biases exists because one questionnaire included several related construct measures. 40
Conclusion
This study examined nurses’ perceptions of the ethical climate in Korean public hospitals. Nurses perceived their workplace ethical climate as positive. The score on the ethical climate dimension related to physicians was lowest. Nurses’ perception of ethical climate varied by hospital characteristics such as hospital type, teaching status, nurse staffing level and bed size, as well as individual characteristics. In addition, among the five ethical climate dimensions, only the ‘patient’ dimension was significantly associated with nurses’ medical error experience, and the four dimensions of ‘patient’, ‘manager’, ‘hospital’ and ‘physician’ were significantly associated with nurses’ intent to leave. Nurses with a higher score for these dimensions were less likely to have made medical errors and leave their current job. These findings indicate that hospital executives and nurse managers should be involved in enhancing ethical climate to improve patient safety and nurse retention in hospitals. Actions for promoting a positive ethical climate can include providing continuing education on nursing ethics, along with increasing nurses’ accessibility to ethics resources and information; promoting ethics rounding in multidisciplinary teams; introducing a committee or system for reviewing hospital or nursing policy related to ethical issues and the crucial contexts for ethical decision-making and practice and performing regular assessments of ethical climate and moral distress.
Future research in different care settings is recommended to expand existing knowledge of and theories on relationships among the issues of ethical climate, the occurrence of medical errors and nurse retention. As such, the relationships between ethical climate and medical errors, including the types and frequency of medical errors, degree of patient harm and preventability of medical errors, need to be further explored for a better understanding of this relationship. Moreover, we did not include the extent and degree of moral distress in the current research, but we suggest that future studies investigate the associations between ethical climate, moral distress and patient and nurse outcomes such as unsafe care and intent to leave, which would allow for the development of better theoretical models on these relationships. The findings of this study could serve as a basis for future studies. In addition, we suggest future studies on interventions to promote hospital ethical climate.
Footnotes
Acknowledgements
The authors would like to thank Dr EJ Hwang for assistance on data collection.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Korea Research Foundation Grant funded by the Korean Government (KRF-2007-313- E0058).