
Abstract
Background:
Several authors have focused on the aesthetics of nursing care from diverse perspectives; however, there are few studies about the sublime and the beautiful in nursing.
Aim:
To identify beautiful and sublime moments in the context of the aesthetics of nursing care.
Methods:
A theoretical reflection has been contemplated about sublime and beautiful values in the context of the aesthetics of nursing care from the cultural history perspective. For that purpose, a revision of this issue has been completed. The terms ‘beautiful’ and ‘sublime’ have been analysed to identify the characteristics of both in the context of nursing care.
Ethical consideration:
We have followed all ethical requirements regarding the sources, conducting research and authorship. There is no conflict of interest in this paper.
Results:
With aesthetic knowledge, the nurse expresses the artistic nature of nursing care by appreciating the act of caring for individuals. The sublime is a complex phenomenon, since apparently contrary feelings are interwoven. Nursing care is an art with an anthropological object-subject on which the ‘artist’ applies their prior knowledge and skills. Feelings and emotions that develop during the clinical nursing practice – especially at times sublime and beautiful, aesthetic – constitute experiences which are professionally significant.
Introduction
Women’s history and gender studies have generally paid little attention to the role of feelings, values and beliefs in the process of occupational socialisation in general and in nursing care in particular. In this article, nursing care is defined on the basis of the most traditional and widespread notion of nursing as the most ancient art and the most modern science, and the term encompasses both pre-professional and professional nursing. Aesthetics as knowledge stemming from the nursing praxis (performing care on the anthropological object-subject in a particular situation) 1 constitutes the study of the feelings that emerge from the dialectic process: prior knowledge-application/interpretation during the act of care in the nurse/patient interaction.
The subject of aesthetics has long been the monopoly of disciplines such as philosophy, psychology and art. However, feelings are considered essential elements of analysis in the field of nursing. Aesthetics has been considered important since classical antiquity, and the philosophers of ancient Greece addressed this issue by identifying the form or idea of the good as the supreme value. From the perspective of poetry, drama and history, aesthetics has been interpreted as a logic of sensation. The Platonic principle that ‘good is beautiful’ has been reinterpreted by other authors, who have linked ethics to aesthetics in the context of nursing care. 2,3
By Plato’s understanding, beauty was a previous, innate and permanent idea: it encompassed values that we tend to call aesthetics, as well as moral and cognoscitive values. This concept of beauty differed very slightly from the concept of good, moral and ethics. By following this Platonic understanding of beauty as a prelude to aesthetics, its connection to ethics is noticed as a discipline which studies moral, virtue, duty and so on. It is in this sense that Durán de Villalobos considers the ability of keeping the moral conduct of the citizens’ practice as an essential aspect to be able to create an aesthetic act. In essence, ethics analyses the idea of beauty according to Platonic thoughts, due to the fact that it analyses the evil, good, correctness and so on, making use of the morally established criteria.
The interaction between a nurse and a patient implies a process of decision-making about what is appropriate and good for the patient’s care. It also implies a relation between the nurse, who applies care in a professional and scientific way, as well as in an artistic way, regarding the raw material of her work, which is the human being: exchange of looks, words and, ultimately, feelings that form a context where aesthetics must take up its appropriate place. That is to say that nurses must be aware of the importance of their object/subject and dignify it in accordance with their sole and unique regulation of the individual. In that sense, Heidegger suggests dignifying the object that the artist performs by adding his artistic point of view. Such point of view contrasts with another one (non-verbal communication) that together with the word (verbal communication) and the technique in practice forms a work of art that does not lack beauty and in which the sense of good is perceived.
In fact, history has shown that nursing care has long been the responsibility of people attuned to the supreme values, such as motherhood and religiosity, 3 which have aesthetically determined the form and function of the social structures involved in care. Every value refers to human necessities or aspirations and to the most essential and fundamental values that in all rational hierarchy have the supreme rank: truth, good and beauty. These are the values involved in self-fulfillment and refer to finding a meaning to life, transcending in a creative work, fighting to reach a goal, such as truth, beauty, kindness or enquiring about the meaning of nursing, its plain truth. For some authors, it constitutes a form of poetry (a way of expressing a deep feeling connected to the supreme value). 4
The self-fulfillment of a nurse as a professional entails considering the patient as a unique person that is subject of care and knowledge from a scientific and artistic perspective that allow to glimpse the beauty in caring (how good and beautiful caring is). The direct relation between value and aesthetics lies in the consideration of value as a subjective resonance of feelings as well as aesthetics as a field that, basically, involves the depths of feelings and the way we perceive them. In this context, deep feelings (very intense ones) constitute subjective resonances of supreme values. 5 This study was based on the following objective: to identify beautiful and sublime moments of nursing care in the context of nursing aesthetics.
This objective arises due to the fact that the most sublime and beautiful moments of nursing are impossible to identify without clarifying aesthetics as a source of knowledge as it is focused on, among other fields, the study of feelings. Nursing is about applying care by experiential processes in the course of which, apart from the act of caring itself, nurses and patients interact by means of looks, words and feelings and, depending on the content, intensity and depth, they will be beautiful or sublime. 5
Background
Cultural historians, who mainly have their roots in social history, study both the feelings and values of a society and the mechanisms of cultural transmission and pressure. By means of the cultural history, feelings and values are studied. They standardise the nursing and caring activity in different cultures throughout time. 5 An influential group of cultural historians emerged from the Birmingham School who engaged in the study of literature and the mass media and their impact on the ways people think and feel through fomenting the standardisation of mass aesthetics. 6 In this sense, cultural history allows the study and analysis of feelings and values that appear during care processes throughout time. Cultural history also tackles the study of aesthetic feelings in the organisation and motivation of care and contributes to the identification of beautiful or sublime moments of nursing based on the content, intensity and depth of feelings that arise from the act of caring. 5
Carper, 7 in a classic study on the patterns of nursing knowledge, classified these into four levels: empirical knowing, ethical knowing, personal knowing and aesthetic knowing. This classification of the patterns of nursing knowledge has been adhered to by many researchers 8 applying different perspectives but respecting the essence of the classification and principles established by Carper. Some years later, an article was published presenting a critical analysis of Carper’s work and adding a new pattern: socio-political knowing, which, in line with Heidegger’s concept of ‘being-there’ developed in ‘Being and Time’, implies taking the historical, geographical, ideological and sociocultural context into account in the ways of structuring knowledge. 9 Chinn and Kramer 10 provide an integrated point of view of the theory and development of knowledge in which they include the Emancipatory Knowing.
Other researchers have conducted dialectical studies and analyses of nursing as an art with rational dimensions. 11 Wainwright 12 criticises Carper on the basis of the difficulties of clearly discerning between art, on one hand, and aesthetics on the other hand. Contreras 13 says that the aesthetics and art of nursing can be objectified by the evidence through communication and intersubjectivity.
The word ‘art’ mainly means the act of production and aesthetics, the act of perceptions and feelings arising from it. As far as nursing is concerned, while caring constitutes production, perceptions and feelings arise in the course of interaction between the nurse and patient, implying such perception. Wing 14 believes that aesthetics can be a point of convergence between folk healers and nurse theorist. Mitchell and Cody 15 reflect on the scientific and artistic nature of nursing. Busquets 16 vincula el cuidado de enfermería a la estética y a la ética y Teixeira 17 analiza los componentes éticos y estéticos de los cuidados.
Edwards 18 describes the difference between fine art and other arts, positioning nursing as an art, but not a fine art. Similarly, several authors have focused on the aesthetics of nursing care from diverse perspectives: from ethics and philosophy, examining the need for nursing to develop and implement professional spaces and strategies for the subjective expression of feelings 2,16 from the perspective of the scenarios where nursing care is delivered, differentiating the aesthetics of hospitals, religious buildings and homes. 19,20 Some authors have investigated about aesthetic and cultural interests of patients 21,22 and from the perspective of poetry, socio-poetics and prose written as a means to express and preserve the aesthetic knowledge produced in the intensity of nurse–patient interaction processes. 23 Other authors think poetry is a source of knowledge for nursing, 24 and Watson 4 between her ideas praised the possibility that poetry is a way of knowledge to truth. Some authors believe narratives generated in the execution of care as a source of moral consciousness and knowledge aesthetic 25,26 by revealing the human condition, 27 and the beautiful and the sublime in diseases and their treatments. 28
Method
Data sources
In this study, a theoretical reflection has been contemplated about sublime and beautiful values in the context of aesthetics of nursing from the cultural history perspective. For that purpose, a revision of this issue has been completed. The criteria of selection of articles and monographs have been pieces of work based on feelings of beauty and the sublime, aesthetics and nursing, beauty and the sublime in nursing, feelings and aesthetics of care and cultural history of nursing.
The fundamental theoretical framework, cultural history and aesthetics, which originated in the Birmingham School, is characterised by the study of society’s feelings and values and their role as mechanisms of cultural transmission and pressure. The relationship between history and aesthetics forms the core of human feelings; aesthetics is integrated into the temporal quality of nursing care, to which it endows form and style, establishing the trends that distinguish nursing care over time in different cultures. To clarify the theoretical basis of this study, it is necessary to provide a definition of cultural history which is both comprehensive and accurate and which encompasses the essence of the statements used to express the characteristics of need, culture, nursing care, anthropology, aesthetics and history. The cultural history of nursing care may be defined as a speciality within the discipline of history which aims to study human beings in the context of their culture over time, examining all the behaviours, ideas, feelings, symbols and meanings that occur in a given social, economic, family and occupational context and which are involved in the process of meeting the health needs of a human group. 5 The cultural history of nursing care constitutes an appropriate tool for studying the aesthetics of nursing care in relation to cultural and axiological factors. Etymologically, the word aesthetics derives from the Greek words aisthetikê, meaning ‘sensation, perception’ and aisthesis, meaning ‘feeling, sensibility’. In his ‘Critique of Judgment’, Kant affirmed that aesthetics can be defined as the science that studies and investigates the systematic origin of pure feeling and its expression, art. To the same extent, in ‘Observations on the Feeling of the Beautiful and Sublime’ published in the 18th century, Kant refers to feelings that can be identified within aesthetics: the beautiful and sublime. According to Kant, 29 the sublime touches, while beauty fascinates. The feeling of the sublime is more intense and powerful than the feeling of beauty.
Chinn and Watson 30 put forward a definition of the art of nursing that is in keeping with the theoretical perspective adopted in this study: ‘The art of nursing is the art fact of the experience in the moment. It is the direct apprehension of a situation, the intuitive and embodied knowing that arises from the practice of nursing’. Following this perspective that accepts the artistic nature of nursing care, it is essential to widen the concept of aesthetics beyond the fine arts and to consider that knowledge patterns cannot be interpreted as unrelated aspects.
The literature search was conducted using key words which reflected in objectives (aesthetics, beautiful and nursing, sublime and nursing, sublime and illness, beautiful and illness, nursing care, nursing and aesthetics, aesthetics and illness, cultural history of nursing care, feelings and nursing care, functional structures and nursing care, art and nursing care, patterns of knowledge and aesthetics) in secondary or derived sources selected to facilitate the search as regards the previously established criteria (Cuiden, Cinahl, Medline, Bireme), from which the primary sources were identified and selected. Throughout cultural history, aesthetic feelings are identified in a first phase in the organisation and motivation of citizens and, in a second phase, beautiful and sublime moments in nursing are analysed based on their content, intensity and depth of feelings involved in the act of caring. 5
Categorisation and data analysis were carried out following the principles of the nursing aesthetics and the cultural history of nursing. The terms ‘beautiful’ and ‘sublime’ have been analysed to identify the characteristics of both in the context of nursing care. The categories ‘art’, ‘aesthetics’, ‘sublime’ and ‘beautiful’ put forward by different authors1,3,5,7,12,27,29,30,32 were analysed. The concept analysis was conducted using guidance given by Walker and Avant. 33 Data source included 39 articles and monographs covering the period 1980–2013 from a variety of disciplines, including nursing, medicine, sociology and philosophy.
Results
Aesthetics as knowledge stemming from the art of nursing care
We agree with Carper 7 as regards understanding nursing care as an art. The nurse must interpret prior theoretical knowledge in a unique context: patient, surroundings, ward, temperature, odours, touch, sight (colours, non-verbal language) and so on. It is a process of dialectic interaction in which perceptive capacities (the senses) have a bearing on the interpretation and execution of the nursing act. As pointed out by Edwards, 3 although the nursing act does not fall under the fine arts, it does involve the interpretation of prior knowledge in a particular context: the interpretation of a beautiful symphony involves genius and creativity in the field of fine arts. It involves performing a previous musical piece on a particular stage, with a different audience, different spatial characteristics and so on. The nurse must interpret how to apply their care to the patient with so many variables that the act of caring becomes a process fulfilled by both prior knowledge and the perceptive sensations that take place during the execution of said care. The above involves the application of knowledge in practice and comprises a professional and also personal nursing experience. It is a dialectic process in which the thesis is the prior knowledge, the antithesis is the reality in which the practice has to be applied and the synthesis is where the theoretical, practical and aesthetic knowledge converge.
The nurse has prior theoretical knowledge, and when interacting with the patient, this knowledge is reinterpreted through the feelings that emerge via their perceptive capacities. Consequently, in line with Van der Zalm and Bergum, 34 aesthetic knowledge in nursing care occurs as the result of perception on an expressive, creative and empathetic level regarding a particular situation in the nursing experience. With aesthetic knowledge, the nurse expresses the artistic nature of nursing care by appreciating the act of caring for individuals.
The relation between aesthetics and ethics has been supported by authors who advocate the convergence of aesthetic feelings such as beauty, good, truth and so on with ethical principles and values. According to Durán de Villalobos, the difficulty of specifying the art of nursing is mainly related to the fact that it lies in an ontological level; it is expressed by means of nurse’s being and knowing. It may also be possible to get to know aesthetic aspects, but it is impossible to isolate them from scientific and ethical components and from the therapeutic use. 32
After thinking about the relation between art and nursing, other authors come to the conclusion of considering aesthetics as a point of convergence between folk healers, and nurse theorists, Wing and Carper, suggest an alternative regarding the lack of recognition of the importance of art in nursing which is that in the past, the definition of the term ‘art’ has been limited in an excessive and inappropriate manner. 7 In some way, it answers to Edwards who rejects the use of art in the sense of an activity qualified as nursing considering it inappropriate, and interprets the term ‘art’ in a restrictive way by limiting it to the ‘fine arts’ 3,12 By drawing inspiration from the Greek concept of ‘technique’ and the construction of art as an experience of Dewey that perceived art as a consequence of the act of work production (the act of caring), and aesthetics as the perception of feelings that such work provokes, Carper considers that the concept of ‘fine arts’ must be broadened so qualified activities, such as nursing, could be included in it. 12
One of the strategies to keep considering nursing as an art and settle the point of choosing between a minor art and ‘fine art’ for which Carper was widely criticised consisted in highlighting the anthropological object-subject of nursing science (individual, human being) and verifying the complexity, singularity and its nature as a sender and receiver of feelings (source of nursing aesthetics) also in the context of care. 5
In conclusion, nursing is art because it encompasses knowledge, technique, intuition and sensitivity, 5,40 and the discussion on its adscription to one act or another (regardless of how profitable these discussions are) should be settled before the magnificence, singularity and uniqueness of the person (anthropological object-subject) receiving (artistic work-product) care, due to the fact that nursing is the only art that implies the application of techniques, intuition and sensitivity within such a special and privileged field as is the human being.
The aesthetic point of view contributes to the awareness of the importance of the object-subject of nursing as a science and art and makes it easier to dignify it according to the unique and sole statute of the individual. 36 A nurse’s care is necessarily applied in a process of interaction between people in which feelings arisen from the act of caring are contrasted: an exchange of looks (non-verbal communication) that, if combined together with words (verbal communication) and the performed technique, manages to constitute a work of art which does not lack beauty and in which the sense of good is perceived. 16,17
Beautiful and the sublime in nursing
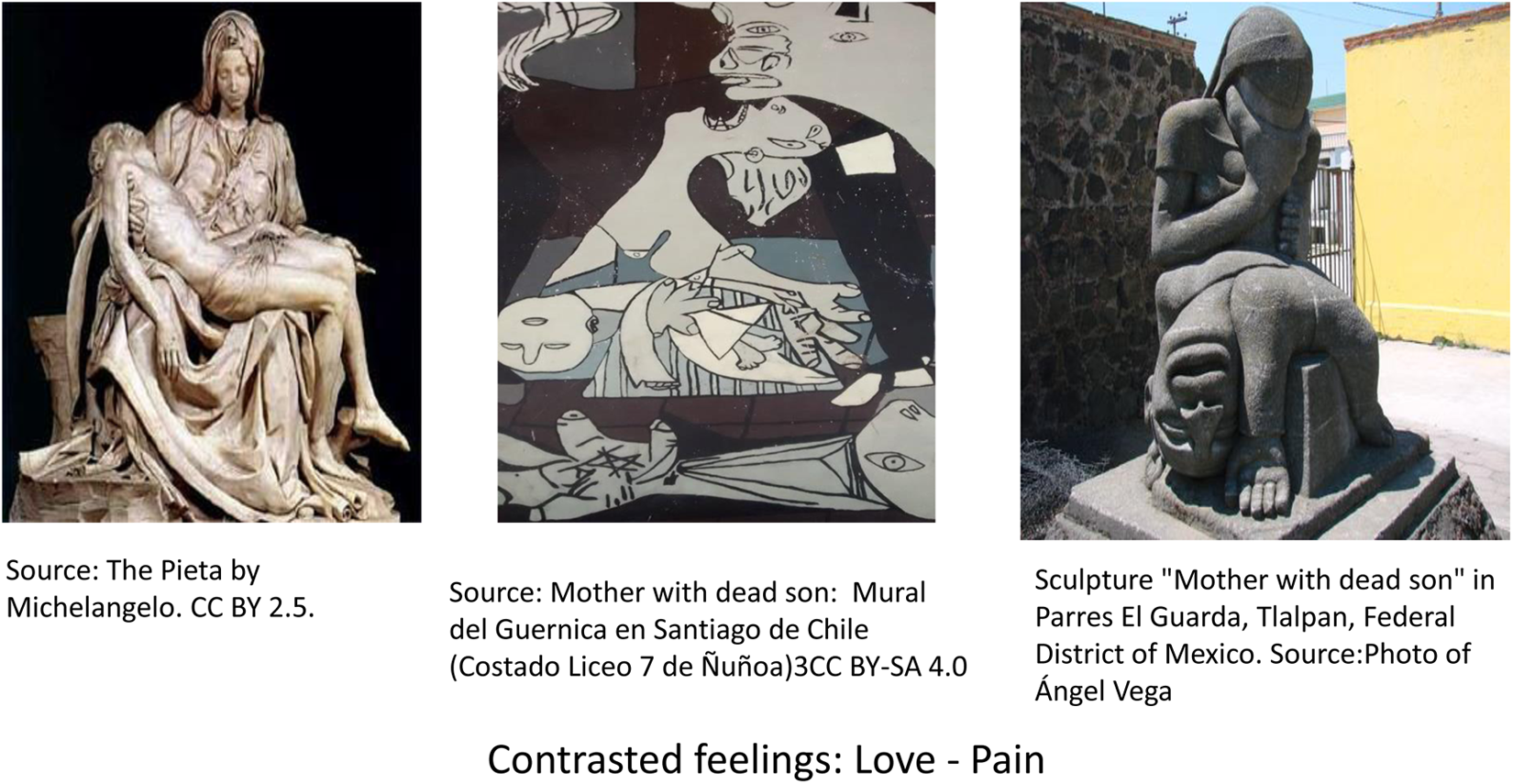
Beautiful moments in nursing are identified by means of simple contents that imply the canonical fulfilment of basic care and inspire feelings and values of low intensity and depth, because they are involved in the process of satisfying the needs of daily life: food, excretion, clothes, hygiene and so on. On the other hand, sublime moments take place in complex contents in which highly intense feelings are associated, provided by the significance and depth of beliefs and values which are characterised by a singular moment in the context of nursing care: the birth of a child which is a special and unique moment and to which joy, tender and pain are associated; love and pain associated with the loss of a loved one, care prior to the death of patient who is saying goodbye to their family and so on. 5
For Kant, 29 who believed that we all have a cultural idea of what is beautiful or sublime, beauty is that which is perceived as something pleasant: a flower, tree, woman or man. The Platonic principle that ‘good is beautiful’ has been reinterpreted by Busquets 16 and Teixeira, 17 who linked ethics to aesthetics in the context of healthcare. It should therefore be possible to use the ethics of nursing care taking into account the theory of the platonic ethics in which good is beautiful, to identify beautiful moments in the context of nursing. The image of a mother breastfeeding her child and the interaction between them subjectively constitutes a beautiful image (ethical dimension of the aesthetics of nursing care). From an aesthetic point of view, it is associated with feelings such as maternity, mutual dependence, tender, pity and love. In order to show the close connection between caring and feelings of a mother’s love, we analyse Fromm’s theories 35 that state that love is a feeling, as well as an art, and has four main elements in common with other forms of love, but it has its highest form in a mother’s love: care, responsibility, respect and knowledge.
The link between breastfeeding and nursing is shown in the process of historic and social construction of caring by means of satisfaction of a basic and essential need, food. In a historic and etymological way, this has served to refer to nursing (nutrix, nutrire) which has evolved throughout different aesthetic phases: maternal, religious and professional stages. 5
All the beautiful and sublime moments occur during the nurse–patient interaction. The beautiful moments that generally occur in everyday life reflect the effects of a well-performed nursing art/act and give rise to ‘beautiful’ feelings as a result. This undoubtedly involves a judgement about the nursing act, a judgement about correct performance that forms part of a continuous process of seeking ‘excellence’ in which reflection on practice and experience are essential. ‘The nurse as artist can bring out the inherent beauty common and integral in our care (…) we can recognize the beauty that is already present (…) is caring praxis’ (p. 209).
25
In this practical context of care recipient–caregiver interaction, aesthetics constitute a source of meanings. Aesthetics, as well as looking for meanings for the nursing practice (art of nursing), has a teleological (universal) element that investigates how to optimise the nursing act (seeking excellence), thereby pointing to the existence of an aesthetic judgement.
25
An ethical analysis of nursing care inevitably involves a study of the values and beliefs that promote one kind or another of nursing practice. The principle ‘good is beautiful’ has been reinterpreted by other authors, who have linked ethics to aesthetics in the context of nursing care.
1,2,16,17
All of the moments that occur in the care recipient–caregiver interaction which give rise on the part of the caregiver to feelings of great satisfaction derived from the thought that he or she is performing their work well, and which coincide with the cultural currency of the beliefs and values present in their culture (domestic, professional, religious, etc.), could be described as beautiful moments in the context of care: teaching a new mother to breastfeed, tucking a baby up in his or her cot, helping to feed an older people and so on. There are ethical implications of the aesthetic and the sublime in nursing: If illness accounts are a recovery of the sick persons,s sense of identity having an ethical as well as an aesthetic dimension to them, then the ‘handles’ that provide for the articulation of the sublime will sometimes be fortuitous fragments, no always major events, in the mundane world these are likely to concern the effects of clinical diagnosis of serious disease of medical treatment (…).
28
As a particular form of symbolism, the aesthetic project involves a vital engagement with features of suffering, and is through this engagement that the sublime aspects of illness experience penetrate the sensuous and material world of disease and its treatment.
Origin of the aesthetics of the sublime.
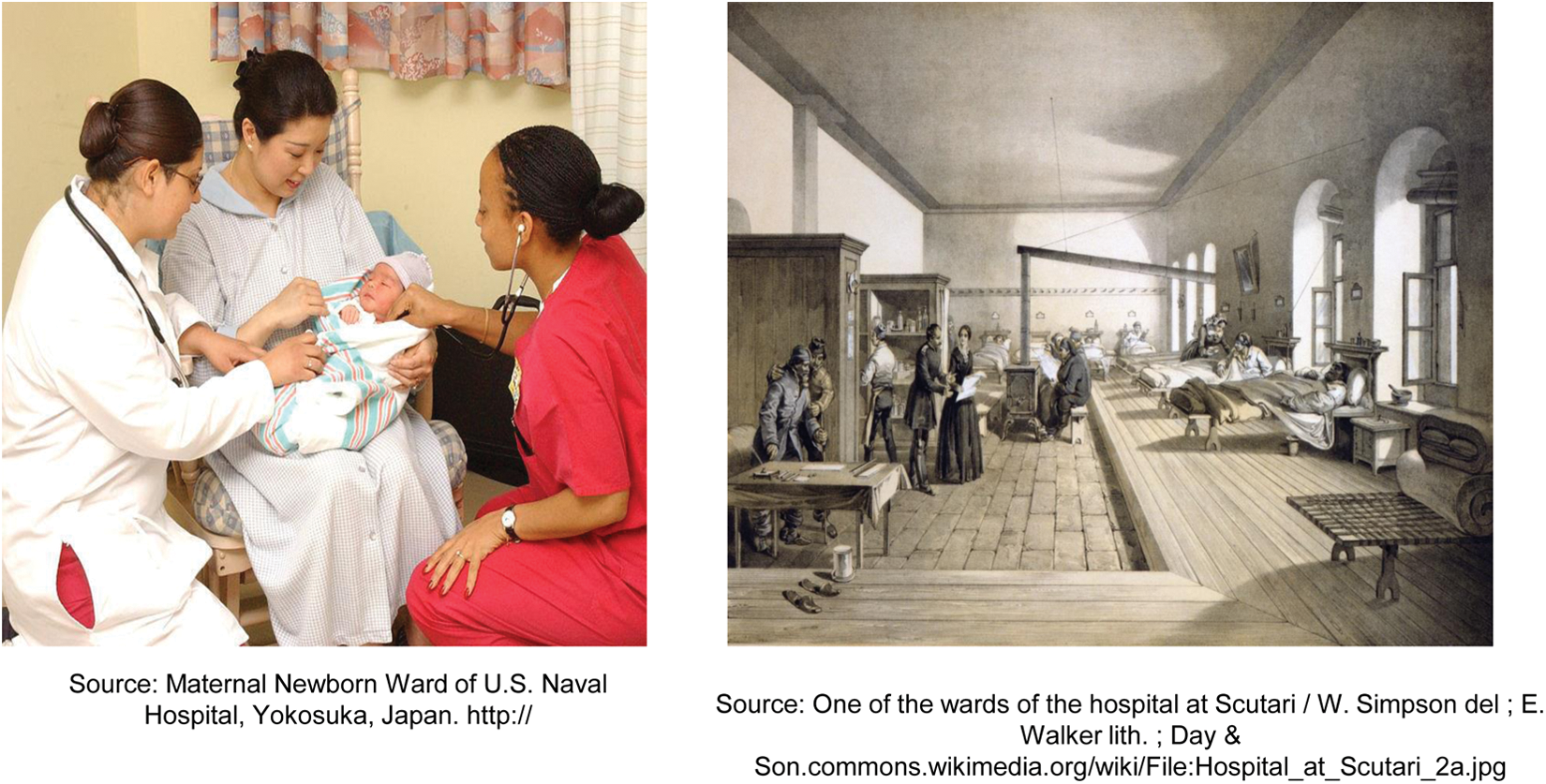
The origins of modern nursing are grounded in aesthetically sublime moments such as the Crimean War, where feelings of tragedy and the pain of the soldiers were interwoven with the beauty and intensity of care provided by Nightingale and her nurses. Sublime moments constitute important episodes in nursing, but nowadays they are not part of the daily life of nursing.
The everyday and the beautiful are encapsulated in the image of the nurse helping the mother to place the child for feeding. The beautiful moments that generally occur in everyday life reflect the effects of a well-performed nursing art/act (Figure 2). The origins of modern nursing are grounded in aesthetically sublime moments such as the War (Crimea, Sarajevo, Vietnam, etc.). 5
Aesthetically beautiful and aesthetically sublime moments in nursing.
Subjective and objective dimension of the beautiful and the sublime in nursing care
As mentioned above, for Plato, doing good was something which produced pleasant sensations and could even lead to feeling a certain level of happiness, while for Kant, something which is pleasing to the senses possesses a component of beauty (although this is not always the case). According to Kant, 29 both the beautiful and the sublime are constructed subjectively, and consequently, objective care constitutes a purely abstract dimension. The practice of nursing care as seen from a humanistic perspective, which has reclaimed the holism of pre-professional care following the cold objectivity imposed by the neo-positivism characteristic of neo-positivist professionals, enables a return to the subjective component of care and therefore opens the door to an analysis of the beautiful and the sublime in nursing care.
Thus, despite its subjectivity, something is defined as beautiful according to a canon of beauty that is socially constructed by the values, beliefs and feelings that constitute the mechanisms of cultural pressure. Since the evolution of the idea of the beautiful and the sublime is linked to the temporal validity of these values and the mechanisms of cultural pressure, aesthetic changes in values and feelings involve a dialectical constructivist–deconstructionist process that evolves over time. 36
Both sublime and beautiful moments are subjective, since they occur during a nurse’s personal and professional experience in an interaction process with a patient in a particular situation in which perceptive capacities, instinct, knowledge, empathy, previous experience and creativity come together. 26
The aesthetic objective dimension in nursing of beautiful and sublime moments, according to Plato, has its origin in the knowledge prior to the aesthetic experience as a formal and preliminary idea by means of which a consecutive judgement or diagnosis is construed and issued within a specific act of nursing. 30 Plato declares that the formal idea of beauty (or any other idea) is prior and objective and contributes to clarifying concrete and subjective evidences of beauty in daily life. By means of communication and intersubjectivity, the product of perception is reduced to the essential aspects (the feeling), due to the fact that by comparing different perceptions and feelings of the same phenomenon, aesthetic objectivity and evidence can be achieved. 13
The personal element and the experience cannot be separated from aesthetic knowledge in the art of nursing. 7
The art of nursing exists because it brings together the following characteristics: An artist (nurse) who has prior knowledge and skills and can potentially use them at a given moment. An anthropological ‘object-subject’ (body/soul) that exceeds any other material in complexity, sensitivity and individuality (even the fine arts): the human being. An interpretation of prior knowledge in practice via the nurse–patient interaction that is applied to the ‘object-subject’ and that gives rise to the work: the artistic care.
Hierarchical organisation of values as a mechanism of cultural pressure, its relationship to the aesthetic standards of nursing care
From the shadows – at least as far as traditional history is concerned – values, beliefs, feelings and symbols have influenced how nursing care is organised. Cultural history has studied the cultural pressure that values and feelings have exerted in the form of social organisation and the progress of fulfilling the needs of human groups, in which professional care (domestic and religious) and professionals have been deemed to be decisive to survive. The universal nature of values stems from an ideology which is in itself indiscernible if these values are not embodied in individuals who express them as a quality or attribute of their being.
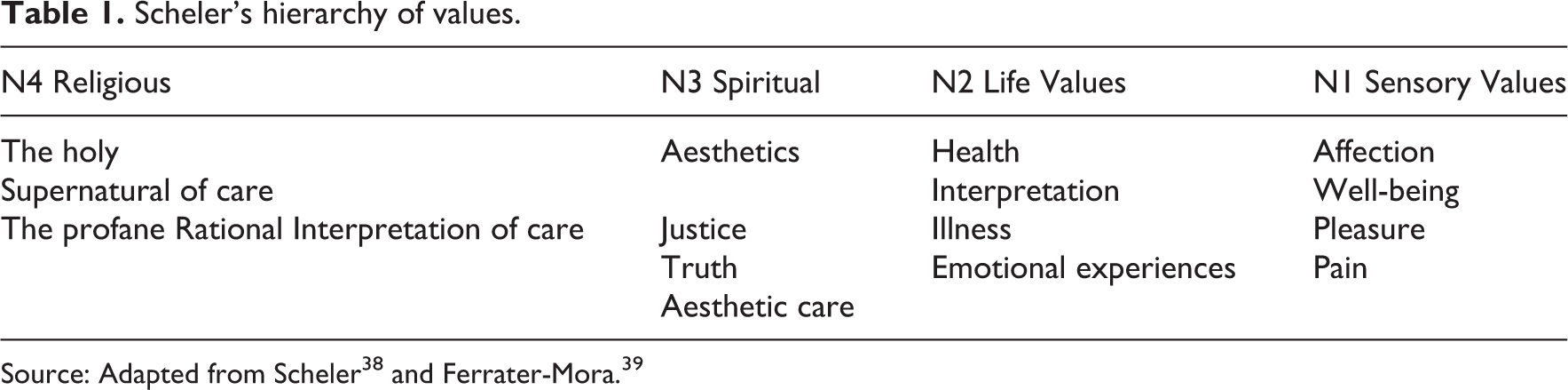
Harry Pross 37 has stated that the coercion necessary for people to carry out their socially assigned roles is produced by the artificial superimposition of values vertically and that this process is closely related to human communication and technology processes, and above all, to the feelings they involve (Mass Media). Scheler 38 (Table 1) categorised the concepts of health and disease as life values that generate feelings or ‘subjective resonances’ embodied in aesthetically meaningful symbols that have represented and transmitted a particular aesthetic of nursing care in a given society. These values and their associated feelings (subjective resonances) and symbols, which influence the configuration of the aesthetics of nursing care, have been subject to cultural variations over time which constitute an important part of the subject of study in cultural history. One consequence of the historical cultural variations in nursing care is the change in values and feelings from motherhood to professionalism and expertise. The transformation of an aesthetic of nursing care based on pre-professional values and maternal feelings occurred through a process of deconstruction prompted by feminist thought 8 and critical thinking during the last third of the 19th century and the first half of the 20th century. This new aesthetic of professional nursing care gradually consolidated around the values and feelings prompted by rational technological thought, science and professionalism.
Scheler’s hierarchy of values.
Discussion
A consideration of the socio-political pattern of knowledge would help to contextualise the interpretation of the role of aesthetics in the evolution and organisation of nursing care; 9 however, such contextualisation would require studies focused on more specific cultural contexts in order to overcome the potential ethnocentrism of this study, the more generic and essentialist nature of which can only provide an overview of the phenomenon. As Durán de Villalobos noted, 32 many authors have assigned an essentially technical nature to the pattern of aesthetic knowledge; however, in this study, the aesthetics of care has been interpreted as an integrative pattern of knowledge about the sensory dimensions of the world of feelings, whereas rationalist dimensions have been more closely linked to the technical context. According to Durán de Villalobos, the majority of the professional nurses circumscribe the aesthetic or art of nursing care to the technical dimension, although authors such as Chinn and Kramer 10 have advocated a conciliatory integration of emotional or sensory and rational or technical dimensions.
However, from a consideration of the universality of humanity’s core feelings (motherhood, piety, altruism, professionalism, etc.), other authors have shown that the essence of nursing care does not lie in know-how but in the feelings that motivate such activity. 5 Paradoxically, motherhood, altruism, charity, piety and other feelings have influenced both the development and the delay of the incorporation of nursing care into a professional framework. This reveals the dialectical nature of aesthetics, since depending on the historical moment, its role has been interpreted as either an impetus or a barrier to care.
Wainwright 12 criticises Carper on the basis of the difficulties in clearly discerning between art, on one hand, and aesthetics, on the other hand. Whereas for Carper nursing care is art in the practice of nursing, Wainwright has many doubts in this respect. In this same regard, Edwards 3 states that the art of fine arts is not the art of nursing. Carper insists on the artistic nature of nursing practice and on the fact that it is a source of aesthetic knowledge that is essential for a good/beautiful nursing practice. Chinn and Watson 30 highlight the artistic nature of nursing, linking it to experience, prior knowledge and application in practice during the interaction with the patient. In this sense, Tucakovic, 1 Siles-González and Solano-Ruiz 5 support the idea that aesthetics comes from the practice of nursing; in other words, it comes from the art of nursing as an act that is anthropological (human beings as an object-subject of care), but it comes from an art that not consists in practical skills; yet we should also include it in this ‘know-how’ of how feelings involved are managed and decisions and judgements made. Nursing is art because it integrates knowledge, technique, intuition and sensitivity. 5,40 The question of its adscription to the ‘fine arts’ or to another type of art should be settled before the magnificence, singularity and uniqueness of the individual (anthropological object-subject) and the privileged raw material in which nursing applies its care.
An impetus in the sense that in a pre-industrial and even industrial society where there are no alternative social structures to assume the care-giving role of the family (the Church – care provided by members of religious orders; the State – care provided by professional nurses), the feeling of motherhood has constituted the core that has maintained the group’s cohesion through the structure of kinship and emotional ties. Motherhood inspires feelings through which the entire parental system is organised and on the basis of which the fundamental social structure of coexistence and socialisation is constructed: the family, strongly linked to care, and the sexual division of labour and its essential role in satisfying everyday human needs such as food, hygiene, sleep, rest, safety, love and learning and so on. A barrier in the sense that the aesthetic feeling of motherhood and religion constitutes an obstacle for the professionalisation of nursing care and the birth of nursing as an academic discipline.
Limitations and practical applications in nursing
Open discussion about artistic or technological nature of nursing is one of the main limitations of this study due to the complexity of the topic that analyses the existence of different perspectives, rational thoughts and constructions by different authors. The sublime and beautiful, as a feeling, expression and interpretation, is a complex phenomenon, since apparently interwoven contrary feelings are making it difficult to analyse in a professional context.
Values and their associated feelings (subjective resonances), which influence the configuration of the aesthetics of nursing care, have been subject to cultural variations. The beautiful and sublime moments in nursing care have ethical implications which need to be studied in future research. This cultural complexity is influenced by several factors hindering its analysis: feelings, values, gender, religion, technology, art and so on.
Regarding the application in current nursing practice, this study helps to reveal the artistic and aesthetic potential of clinical practice as a tool to optimise the quality and humanisation of nursing care in so far that the anthropological object-subject, on which nursing focuses all its attention, empowers the holistic vision of care.
Conclusion
Cultural history of nursing, that can be traced back to social history, allows the study of feelings, beliefs and values and mechanisms of cultural transmission that have influenced the way of organising and construing care in different cultures and historical periods (beliefs, values, feelings). However, this cultural and historical approach also includes problems such as the complexity that entails its global approach of the facts. The cultural history constitutes an apposite tool for the study and analysis of the feelings involved in nursing care and their subjective resonances (beliefs, values), in other words, the aesthetics of nursing care. Cultural history tackles the study of aesthetic feelings in the organisation and motivation of care and contributes to identifying beautiful or sublime moments of nursing depending on the content, intensity and depth of the feelings involved in the act of caring.
The values and beliefs that promote one kind or another of nursing practice (art of nursing) involve an ethical analysis of nursing care. The principle ‘good is beautiful’ has been reinterpreted by other authors, who have linked ethics to aesthetics in the context of nursing care. The theoretical and practical relationship between art of nursing and aesthetics of nursing constitutes a dialectical dynamic, since the subjective dimension particular to nursing care fuels the objective and universal dimension.
A holistic nursing approach is only possible if the aesthetic aspects of nursing care are taken into account, since it is only thus that a strictly technical vision of the discipline of nursing can be surmounted. Feelings of motherhood, altruism, charity and piety have underpinned and motivated the care-giving function throughout much of the history of pre-professional nursing. The link between feelings and values arises from society’s hierarchical organisation of the same and serves as a mechanism of cultural pressure which socialises society’s members to share a common aesthetic of nursing care.
Aesthetic factors are essential in the construction of the history of nursing. Social structures such as the family, religious groups and corporate associations have fomented both pre-professional values and feelings (maternity, altruism, piety, charity) and professional ones (professionalism, technologism, humanism in nursing care) and have constituted the fundamental sources for the meanings which have been used to organise, underpin and enhance the motives and aesthetics of nursing care in different historical periods.
Aesthetic standards have influenced the organisation of pre-professional and professional nursing care throughout history by means of the drafting of social standards, as a consequence of the social intersubjectivity of aesthetics, which have defined different types of nursing.
The feelings involved in the evolution from considering nursing care to the patient like a mother’s care for her child, to feelings arising from the achievement of excellent nursing care/beauty, reflect the importance of aesthetics in the social and emotional construction of nursing. The sublime nursing moments were the subject of history long before women and nursing had a historic voice.
The concepts of care and nursing constitute values that generate feelings or ‘subjective resonances’ embodied in symbols which represent and transmit them to a dynamic society subject to historical and cultural variations. In conjunction with the structures which socialise feelings of maternity, piety, altruism, empiricism, technologism, professionalism, scientism and humanism, aesthetic values and feelings have underpinned and motivated pre-professional and professional nursing care. They have determined the characteristics of sublime and beautiful moments in the context of nursing care, clarifying their nature and their influence on nursing care.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.