
Abstract
Background:
Suicidality is a life-and-death struggle in deep loneliness and psychological pain. There is a lack of knowledge about what could help the suicidal patients’ struggle for continued life. The aim of this study was to develop a deeper understanding of suicidal patients in the aftermath of suicidal attempts. The research question was ‘What resources in the person himself or herself and his or her surroundings are crucial in a suicidal crisis to maintaining the will to live and hope for life’?
Methodology:
The study has a hermeneutic approach and an explorative design. Data were collected using semi-structured interviews with 10 participants: men and women 21–52 years of age. The context was two emergency psychiatric units and one crisis resolution team.
Ethical considerations:
The participants signed an informed consent before the interviews were conducted.
Findings:
This article presents three themes: (a) becoming aware of the desire to live, (b) an experience of connectedness and (c) someone who cares.
Discussion:
The suicidal person’s awareness of wishes, dreams, hopes and will, but also of their feelings in the aftermath of the suicide attempt, seemed to play a crucial role in a suicidal crisis. Experiences of connectedness remind the person of the responsibility in his or her own life and in the lives of others and seemed to strengthen the urge to go on. Private and professional relationships seem to be crucial in stimulating the desire and hope to go on living.
Conclusion:
Becoming aware of the desire to live, being connected to others and experiencing someone who cares is necessary for life. Both private and professional networks seemed to be important resources that could remind the suicidal person of his or her own dignity as part of being human.
Keywords
Introduction
The development of suicidal ideation can be understood as an interpersonal and intrapsychological process. 1 An unbearable psychological pain is well documented as suicide’s most important stressor 2 and perceived hopelessness as a central emotion and risk factor in suicidality. 2,3 According to Joiner, 4 suicide occurs when the desire to die is linked with the capacity to carry it out. The sense that one does not belong, the perception of burdensomeness and fearlessness in the face of death are all factors that exacerbate suicidality. 4,5
On a worldwide basis, about one million people die each year from suicide. In 2012, a total of 515 Norwegians took their own lives. 6 The occurrence of suicide attempts resulting in hospital admission is estimated to be at least 10 times higher than suicides resulting in death. Research in the field of suicidology is to a lesser extent based on patients’ experiences and perceptions. Based on a search in various electronic data bases, 16 studies published in the period 2000–2014 were selected and scrutinized in terms of relevance for this study. Most of the hits resulted from search words such as attempted suicide, patients’ experiences and suicide prevention.
Being suicidal is described as a struggle, particularly before the suicide attempt itself. 7,8 In this struggle, which is characterized by deep loneliness, 9 the establishment of connections with other people is perceived to be important for the will to continue to live. Experienced turning points in life exacerbated suicidality for some, but helped others to choose life. 8 To have suicide as a potential way out, an ‘open door’ can be perceived as a consoling thought. 9 In a randomized study, 10 15% of 217 participants with serious depression reported consolation as a clinical variable related to suicidal ideation. Suicidality can be perceived as being in want of control. 11
Shame is also an important phenomenon related to attempted suicide. 9,12 –16 Experiencing that one’s attempted suicide is taken seriously and being shown respect and friendliness alleviated feelings of shame and helped patients to cope with the suffering and to accept professional help. 13 Being given time, being listened to without prejudice and experiencing mutual trust all appeared to be very significant for the patient’s perception of being confirmed as a person. 17,18 Being seen and confirmed stimulated hope. 19 Suicidal persons experienced the contact they had with psychiatric health services as helpful and the social network as supportive, to the extent that they spoke with friends or family about their feelings. 15,20 Suicidal persons experienced responsibility for persons close to them. 21,22 Three ‘key factors’ important for care and for the design of psychiatric health treatment emerged in an interview study in which 36 formerly suicidal young men participated: better assessment, expanded future-oriented follow-up and focus on strengthening young men’s ability to meet challenges in terms of the future. 23
Based on the literature review, few studies appear to have a direct focus on factors that are perceived to reinforce hope and the will to live in suicidal crisis situations. The purpose of this study is to develop a deeper understanding of the experiences of persons who were in contact with psychiatric healthcare as a result of a suicide attempt. The research question was ‘What resources in the person himself or herself and his or her surroundings are crucial in a suicidal crisis to maintaining the will to live and hope for life’?
Theoretical perspective
The study proceeds from a multi-dimensional view of humans. 24 –26 To be human involves a continual struggle between being and not being. It entails a freedom but at the same time a responsibility related to the individual’s life context and life world. To be a whole person involves a quest for community, interpersonal connectedness, mutual love, belief and hope and meaning. In Eriksson’s theory of health and suffering, human experience is part of being a whole person, unique and valuable. According to Eriksson, 26,27 dignity is existing for the other. Suffering is part of being human. Eriksson 26,28 describes suffering on the basis of three dimensions: life suffering, suffering from disease and suffering in the absence of care. Eriksson’s theory goes into depth concerning ontological suppositions about the human being, health and suffering and is therefore deemed to be a relevant frame of interpretation in this study. According to Shneidman, 2,29 the term pscychache encompasses phenomena such as despair, loneliness, shame and anxiety and is regarded as a key in understanding the suicidal person’s suffering. A holistic, existential approach 27,30 with a view to alleviating and preventing suffering is a central element of pre-knowledge in this study.
Methodology
Gadamer’s 31 hermeneutics has been a general guiding star in this study. A hermeneutic approach in the encounter with people and texts requires a conscious awareness of one’s own prejudices and pre-understanding. Hermeneutics is characterized by sensitivity and openness to what emerges so that the text opens for new questions. 31,32 In Gadamer’s 31 reasoning, prejudices are understood as positive conditions for attaining a new understanding. In this study, the first author’s (M.V.) pre-understanding through experience with suicidal patients within psychiatric healthcare is assessed as having positively influenced the study. This applies to the planning of the study, data collection through research interviews and the process of analysis and interpretation of data in the search for a deeper understanding of what can reinforce the personal struggle towards life in a suicidal crisis.
Participants
The participants in the study were selected, informed and invited to participate by psychology specialists at two emergency psychiatric units and one crisis resolution team. There were four inclusion criteria: (a) serious suicidality – after a suicide attempt, the interview was to take place 2 weeks after the attempt, at the earliest; (b) non-psychotic; (c) able to verbalize experiences; and (d) access to a therapist at least 2 weeks after the interview was conducted. The sample consisted of six men aged 25–52 years and four women aged 21–45 years. One of the interviewees was married, four had children and six had broken couple or partnership relationships as part of their background. Of the ten, seven lived in their own home, one in a flat with municipal supervision and two lived with parents – one of the latter temporarily, after an attempted suicide.
The ten interviewees had different life histories and varying degrees of experience with psychiatric health services. For two younger interviewees, the suicide attempt was the direct cause of their first encounter with this branch of the health service. Suicide was attempted, in all cases, by ingested overdoses of medication. Four of the interviewees spoke of larger or smaller amounts of alcohol taken prior to or at the same time as medication was taken. One of the ten was prevented from carrying out the suicide attempt through involuntary commitment to psychiatric hospital. For five of the interviewees, the suicide attempt was detected by other people. Three of the interviewees interrupted the suicide attempt by calling a family member, a friend or the casualty clinic. One male patient had taken narcotic substances combined with strong painkiller tablets four times in the course of 4 weeks and contacted his family doctor after the fourth suicide attempt. Two of the female patients had attempted suicide several times some years prior.
Data collection
Semi-structured interviews inspired by Kvale and Brinkmann 33 were conducted. The interview guide contained questions such as follows: In your opinion, what is it that held you back and caused you to continue struggling for life? What are your thoughts on the treatment and follow-up you got during the suicide crisis? What are your thoughts about your own contribution towards changing your life to go in the direction you want? The interviews began with the following question: Can you say something about what caused you to get in contact with the healthcare system? The question opened for an account of the current situation and triggered associations and descriptions of situations and earlier periods of life which provided important information. The research interviews can be regarded as narratives. 34 Information was elaborated on in a dialogue, with follow-up questions and confirming comments from the researcher. The interviews lasted 90–110 min and were tape-recorded. The interviews were conducted in the interviewee’s home, on the psychiatric ward or at the researcher’s office, according to the interviewee’s preference.
Analysis and interpretation
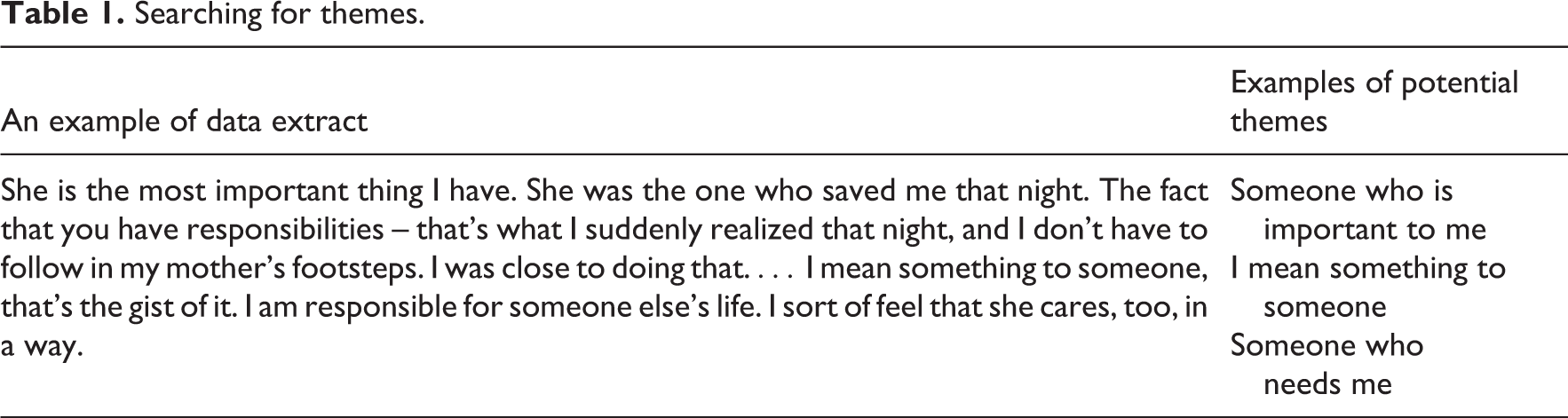
Through repeated listening followed by transcription of the interviews, tentative themes were identified and noted. Following this, the texts were reviewed with openness with a view to identifying the interviewee’s self-understanding. 33 The interviews were then reviewed to glean information that could identify the resources being described. Relevant parts of the text from each interview were copied into a new document. During the review of this text, potential themes were marked, such as ‘I actually want to live’, ‘Someone who is important for me’, ‘Someone who needs me’, ‘I would not want to cause others to suffer’, ‘Responsibility for one’s own life’, ‘It was friends who got involved’, ‘Someone to call’, ‘To share makes it easier to live’ and so on. Table 1 shows how potential themes emerged from selected statements.
Searching for themes.
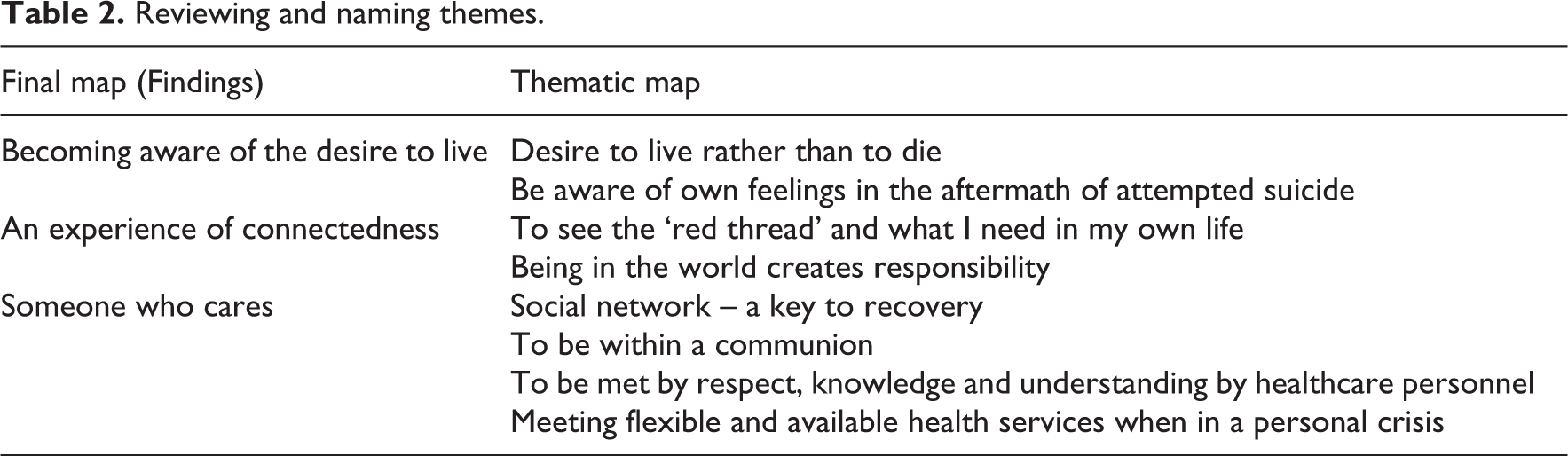
The process is explained by Braun and Clarke’s 35 description of the phases of a thematic analysis. Through a new review in this study, eight themes emerged as key elements, as demonstrated in the study’s ‘thematic map’ in Table 2. The phase includes checking whether the themes are supported in the data. Finally, themes were defined, examined in context and given names, called ‘the final map’. 35 This review consolidated eight themes into three themes which are the findings in this study (cf. ‘Final map’ in Table 2). Braun and Clarke 35 describe ‘Producing the report’ as the last phase. Discussion of this study’s findings is based on earlier research and in light of the Finnish theorist K. Eriksson 24,26 –28 as the overarching theoretical reference.
Reviewing and naming themes.
Ethics
The study was approved by the Regional Committee for Medical and Health Research Ethics, Southern Health Region, Norway, and by the Data Protection Official for Research of the Norwegian Social Science Data Services. Three treatment institutions were queried and gave written consent to permit interviews to be conducted. In a meeting between the first author (M.V.) and potential participants, the written information pertaining to confidentiality, the right to withdraw from the study and how the interviewee’s information would be used were communicated to the participants orally, and written consent was signed. The first author also spoke with the interviewees after they had read the transcripts of the interviews. Several of the meetings before and after the interview provided additional information, but it is applied only to acquire a deeper understanding of the information provided in the interview itself.
Findings
Three main themes emerged as important for maintaining the will to live and hope in a suicide crisis. The first two themes are primarily understood as pertaining to the person’s inner resources. The third theme pertains to the relationship with the surroundings, even though the patient’s inner self and his or her surroundings cannot be seen in isolation. The themes are presented as summaries and selected utterances from the interviewees.
Becoming aware of the desire to live
The interviewees described the suicide attempt as motivated out of a desire to die, with one exception when the ingestion of an overdose was described as a desperate act in order to get professional help. The utterance I actually want to live was commonly repeated in the interviews, including when the interviewee's life situation remained unchanged after the suicide attempt. At the same time, the interviewees cited anger and disappointment over not having succeeded at taking their lives or over ‘chickening out’ and not completing the suicide. One man described a feeling of calmness, happiness and comfort when he felt that the tablets and alcohol had begun to work, because then you know that it’s over, that now you are finished. When he awoke and realized that he had failed to end his life, he said in the interview, ‘then I was bloody furious’. At the time of the interview, however, he was relieved that he had survived.
The attempted suicide was described by most of the interviewees as an unreal and frightening event. As one put it, if you have done something a first time, it is easier to do it again the next time. The incident created a fear of repeating it, as another interviewee described, I don’t want, don’t wish to repeat it, but I can’t promise on my honour that I won’t do it again: if I were to promise that, I would be lying. What scares me is this ‘courage thing’ when you try to carry out a suicide; that’s what frightens me. I am satisfied that I am alive, but I’m not exactly doing a wave over it either. I am still rather indifferent. It’s true, I am. But I couldn’t think of trying to die today, while at the same time it is not actually frightening either – it isn’t. The one side of me wanted it (the overdose) to succeed, and the other side wanted it to fail. So in all the panic, when I felt that my lungs and everything were constricting, there was a part of me that wanted to grab hold of life and pull myself up again. Actually I think it was then that I decided I wanted to live.
For some, the awareness of their own impulsiveness became a threat to life and an important discovery: before, I went straight from thought to action, I sort of didn’t have any period of reflection. Others described periods of low self-esteem and lacking confidence, a tendency to isolate themselves, increasing periods of depression and suicidality prior to attempting suicide. Becoming aware of their own behaviour patterns, getting in touch with their feelings and their will or lack of will to live were all described as important in becoming aware of their own desires and needs in life.
An experience of connectedness
A large portion of the interviewee’s thoughts concerned responsibility as an element for creating meaning in their own life and for showing responsibility in a relationship. The attempted suicide was not described as motivated by a need for revenge or a desire to hurt others. I don’t want anyone else to suffer, do I? as one put it. The utterance below illustrates the struggle between the wish to escape one’s own suffering and the fear of causing suffering that would complicate the lives of others. The interviewee wrote a letter to her adult children and two other next of kin, while she sat with a handful of tablets and debated shall I, or not?
There was something that held me back. I had taken a solemn oath and promised my sons that I wouldn’t do anything like this again after the attempt two and a half years ago, so of course that sticks with me, it does.
One of the interviewees had lived with prolonged suicidality since his teenage years and had been admitted many times to the psychiatric health ward. He came to the conclusion that the attempted suicide, which he interrupted himself, had given him a sense of security – he was now capable of carrying out a successful suicide. Earlier on in life, with only one remaining parent, who was also ill, suicidality had been very strong in his mind: But I just could not do it to dad: it was simply not possible, it was not an alternative at the time. Another man described the dilemma between ending his own life, in which he had trouble finding any meaning, and the consequences his suicide would have on the lives of others: My wish to die isn’t about causing problems for others … There is a limit to what you should put other people through. At the same time, I can’t keep myself alive because the family is supposed to be alright; I am the one who is supposed to feel that I have meaning in my life. I am not really demanding in life, but things have to, sort of, work. You mustn’t take your own life because then your family is going to take it very hard and they will blame themselves because you took your life. And it helped me to hear that, because I care a lot about my family; I love them very much and I don’t want them to suffer.
The thought that I mean something to someone appeared to be important in the struggle between the urge to live or to die. Two single interviewees thought that responsibility for children would have further complicated the decision to commit suicide. Five of the interviewees were parents. They struggled with trying to understand why they had tried to end their lives and harboured a feeling of guilt. One of the interviewees had lost his mother to an overdose during his childhood. He described how his thoughts about his daughter’s needs ‘awakened’ him from a near comatose state, after he had taken large quantities of medication and alcohol, and made him seek help: She is the most important thing I have. She was the one who saved me that night. The fact that you have responsibilities – that’s what I suddenly realized that night, and I don’t have to follow in my mother’s footsteps. I was close to doing that. But things turned out all right in the end, so she still has a father … I mean something to someone, that’s the gist of it. I am responsible for someone else’s life. I sort of feel that she cares, too, in a way. I have never been particularly good at learning how to set limits for other people, so I will have to practice. Because it creates a kind of sorrow when you go along with things just because you don’t have the courage to say no. Now and then everyone does this, of course, but if you have to do it constantly you feel sort of violated. So instead of saying no, I just severed relationships with those people, within my circle of acquaintances.
Someone who cares
The perception that someone cares about me was described by many interviewees as very important, including those who talked about the lack of involvement of others in their own lives. Some described families who became deeply involved after the suicide attempt; others had few close family members, and still others neglected to involve family because they did not expect to receive support from them. Nevertheless, all interviewees described various forms of support associated with individual family members. Friends were involved in varying degrees. Some interviewees attributed a significant role to close friends during the suicide crisis.
The interviewees described family relations, to various degrees, as being both a part of the painful experience and a helping hand during the crisis. Interviewees gave elaborate accounts of how parents, siblings, adult children and grandparents became involved after the attempted suicide. Several described how their sisters became involved by moving in with the interviewee, motivating the interviewee to seek psychological help or involving themselves in other ways.
The interviewees described conflicting feelings towards persons close to the victim, such as the account of one woman whose parent tried to convince her that she was suffering from a serious mental illness and that she should be involuntarily committed to a psychiatric ward. At the same time, the interviewee described how she sought and obtained important support from the very same parent during phases when suicidality was perceived as an immediate threat. The parents’ own problems and lack of contact between parents following a divorce were also cited as factors that affected contact between the parents and the interviewee. A young man talked about a father who had psychiatric problems and whom he seldom saw, but said, My father provides support as best he can. He knows that he has done a number of things that he couldn’t help doing and which have harmed people close to him. He says he thinks about me all the time now. Mum worries so much. And that can be a little stressful. She gets involved all the time, goes on about things I would rather not discuss, and she almost demands status reports from me – I am not so interested in giving those. So I am a little ambivalent towards her … On the other hand it’s all right that they are informed about the situation, but then they get stressed by it, and I don’t like to be a burden on them. On the other hand, it gives me a sense of security, in a way. I have a friend who knows everything; I lean on him very much. He is not so good at speaking about problems, either. The rest of my friends just know that I have had problems. But friends give me a social network, contact with them, that is very important. The key to being able to continue in life is to maintain contact. Of course if you have to make phone calls all the time, you get tired of it. And the times my friend want to meet me are never convenient. A network is not something you get for free. So now I owe people two telephone calls. That’s how I try to think.
The interviewees talked about meetings with professionals who had made a difference and who had helped them in various ways. They emphasized the importance of being met by professionals who listened, showed respect, gave them the feeling of being equally valuable persons, got involved, possessed professional knowledge and signalled hope and the belief that we will be able to tackle this together. In addition, examples of guidance and tips needed to cope with daily life and situations that continually taxed one’s feelings of worth and self-confidence were deemed important. Getting help to establish a type of structure in daily life was seen as important, particularly during the first few days after an attempted suicide.
The interviewees provided examples of good dialogues they had had with professionals, and it was exactly this kind of dialogue that they would have preferred to have more often. Sharing makes the day a little lighter, said one of the young interviewees who had difficulty expressing thoughts and feelings in words: Even though everything is chaos, there is someone who knows about me … But I have to feel that they will safeguard what I say, not use it against me, but use it to help me. So there are fewer layers of protection; the layers are thinner, it is easier to bear … I called him: he was fantastic when I had that depression last year. And so I told him over the phone that …, well, now I just tried to take my own life. ‘Would you like to come in and talk about it?’ he replied. So I got an appointment right away, and while I sat there, he wrote an application to the emergency ward and called them, and then all I had to do was go directly to the emergency ward. In terms of family, it has made things much easier … it is an important part, because if you feel that you are losing your family in a situation like this; … they have stood by me the entire time.
Discussion
Suicidality can be understood within what Eriksson 26,28 describes as life suffering, entailing threatened existence, total loneliness and a situation that is perceived as hopeless. The theme becoming aware of the desire to live is interpreted as a struggle in which hope is strengthened at the same time as longing to escape something unbearable 2 is present. This illustrates the phenomenon of ambivalence. 1 The suicide attempt emerged as what Williams 36 describes as ‘a cry of pain’, more than as ‘a cry for help’ – the frequently used metaphor to denote an attempt to take one’s own life. The accounts given by the interviewees seem to reflect a personal vulnerability, but also a capacity to withstand major and long-lasting burdens in life. A basic wish to continue living, to believe in change and the hope of finding meaning, seems to be an important driving force to hold out in suffering and pain for a while longer. In ‘the suicidal drama’, Shneidman 29 lists primary psychological needs as being counteraction, inviolacy, shame-avoidance, succour, order and understanding. Frustrated needs stimulate painful loneliness. Becoming aware of the universal human needs can be a step along the way to being seen and met by other people.
Fearlessness in the face of death is claimed to increase the risk that a suicide attempt may be successful 4,5,37,38 and seemed to be present in two of the male interviewees in this study. The fear of repeating a suicide attempt was still the prevalent shared experience, a phenomenon that does not appear to be sufficiently illuminated in other research. The experience of losing perspective in life, and of becoming aware of one’s own courage to carry out a suicidal act, was frightening to the interviewees. One of them spoke of a feeling of panic in connection with the overdose and of how the desire to choose life gradually emerged. Experiences like these can be understood as turning points, in that the experiences appeared to increase awareness of the danger signals and of acts to prevent the development of suicidal thoughts when they were detected. Turning points are also acknowledged in other studies 7,19 as promoting the recovery process in cases of suicidality. The experiential knowledge of suicidal patients is important in clinical work, but also in terms of building up suicide prevention programmes. 11 Identification and reinforcement of turning points through dialogue about the attempted suicide involves taking the patient’s experiences seriously. One aim must be increased involvement and cooperation in the treatment process 39 as this can reinforce the suicidal patient’s perception that his or her dignity is confirmed.
The theme an experience of connectedness is interpreted as the interviewee’s perceived responsibility from having gained a life. Being human involves having the right and freedom to shape one’s own life. 24,25 At the same time, the person is influenced to make choices and influence others by the decisions taken. Being aware of connectedness to others can be interpreted in the present study as a turning point that strengthened the decision to cling to life. One of the interviewees described a moment during a dramatic phase of the attempted suicide when he became aware of the fact that he was about to abandon his own child in the same way that he himself had been abandoned as a child. To put off the carrying out of a suicide plan or to discontinue the attempt itself is understood as a moral act. Reflections about worries and fears of inflicting suffering on others through one’s suicide were keys in the data material, echoing concurring data reported in other studies. 21,22 The person’s moral set of values can be understood as inner resources that can strengthen the wish and will to continue living, a hypothesis that appears to lack investigation.
Increased awareness about one’s needs and values can preserve one’s dignity and make it easier to seek help. Seeking help in a crisis may be made difficult because of the shame associated with being unable to manage one’s own life, as was mentioned by several of the interviewees. Moralizing attitudes and statements can be experienced as reinforcement of the feeling of shame as well as suicidality. Therefore, statements such as the one referred to by an interviewee, that You mustn’t take your own life because then your family is going to take it very hard, should be avoided. Suicidal persons long for closeness but have difficulty opening up for dialogue. 40 They want health personnel to actively delve into the topic of the suicide. 18 To express existential themes in words may have a preventive value. 19 People need to be met in order to satisfy primary needs of affiliation, dignity, understanding and caring. 29 Meeting the patient with understanding and caring can release words that open for dialogue. Dialogue and cooperation can contribute towards making the suicidal person aware of reasons for living. 39 Through dialogue and dreams, wishes, opportunities and the need for support, clearer insight can be acquired as to what and who can support the will and hope to live. Hope, understood as relational, 41 entails that by being in the world, hope can be stimulated, but also reduced. The fact that interpersonal relationships have a decisive significance in reinforcing hope in suicidal patients appears to be solidly supported by research. 42
Every person has an upper tolerance limit for suffering. The ‘suicidal drama’ 29 is characterized by deep loneliness. 18,43 Having a social network that reacts and intervenes appears to be crucial in a suicide crisis. In the theme someone who cares, the suicidal patient’s environment is interpreted as being a crucial resource. In particular, the involvement of family and friends and their support in a suicidal crisis are of key importance in the struggle to survive, including in cases where relations were characterized by contradictory feelings. The significance of one’s social network in suicidal crisis does not appear to be focused on to any great extent in research. The interviewees who told someone in their environment about their suicidal thoughts and about a suicide attempt were mainly met with understanding and caring; this is in line with the findings of others. 15,20 A social attitude characterized by understanding suicidal thoughts as a normal reaction to unbearable psychological pain 2 will perhaps be able to encourage suicidal people to tell about their own pain in life and thereby feel that they are confirmed. Perceived moralizing or trivializing, however, may reduce the courage to share pain. To talk about suicidal tendencies can be perceived as relinquishing control because it can trigger strong worries and controlling behaviour on the part of other people in the patient’s environment. Lakeman and FitzGerald 7 are of the opinion that nurses should help suicidal persons to acquire greater affiliation with their natural network, a recommendation that is supported by findings in this study. To be seen and confirmed in social relations can reduce pain and stimulate hope. 19 The opposite, that is, not being seen, according to Eriksson 26 is to be considered as dead. People’s basic needs for caring and fellowship need to be met. Being confirmed as unique and valuable in the sense of being for other people 27 is interpreted as having had decisive significance in the interviewees’ decision to strive to cling to life.
Courage and will belong together 28 and are crucial for the kind of dialogue that can break down taboos on the subject of suicide. Sharing with others can make the dark thoughts easier to bear, as one interviewee put it. Patients require an invitation to dialogue; they need the helper to be moved by their suffering, to show commitment and to take initiative. 18,43 In their struggle to regain hope and the will to live, many will need easily accessible help and follow-up from professionals for a long time after a suicide attempt. In this study, the support of professionals was emphasized as important help. Some of the interviewees, for example, talked about family doctors who had known them over a period of time and who set aside time for them and confirmed them. A good relationship invites fellowship, but at the same time separateness. 43 To be seen, given time and confidence and to be listened to without judgement, but with openness and acceptance, are all described by suicidal persons as helpful. 4,17,18 Through significant others, the perception of self-dignity can be reinforced. Suicidal persons, along with their social network, will frequently need to meet professionals with the ability to listen, with a tolerance for pain that is related by the patient, and who are able to see possibilities and communicate the belief and hope that life can be changed to follow a desired direction.
Methodological considerations
We sought to ensure validity through continual dialogue between the first author (M.V.) and the second author (D.N.), and in dialogue about the findings with other professionals. The researchers’ questions and the interviewees’ information were transcribed verbatim. The interviewees checked the information by reading the transcript of the interview. Included in the validation process was a review by the second author of all texts, along with participation in the analysis and interpretation process. During the writing process, the findings were continually checked up against the data.
Mutual trust and contact in the interview situation will be very important for the data obtained. 44 A strong emphasis on mutual trust is assessed as having been important for the richness of the data content. To allow oneself to be personally affected by the data, which in this study was a matter of life and death, while having sufficient distance in the interpretation process, can be related to what Wiklund et al. 34 call an ‘art’ in the hermeneutic approach.
Limitations
The findings in this study are judged to be valid and reliable based on the methodological and theoretical perspectives through which they are derived. Bengtson 45 describes the dialectical relationship in hermeneutics: by its nature, we have limited access to phenomena. The limitation is the driving force that makes phenomena fully conceivable by building bridges over historical, social and linguistic obstacles. Other researchers would possibly find other phenomena or nuances in the themes that emerge in this study.
Every account brings in new elements; nevertheless, the data material after 10 interviews was assessed as being nuanced and rich in content. All accounts are based on a Western cultural understanding. An inclusion criterion that would have ensured participation by persons of different cultural backgrounds might have provided more nuances in the data, for example, pertaining to religious factors that may be life-maintenance resources.
Conclusion and implications
To be aware of one’s desire to live, of dreams and hopes appear to strengthen the suicidal patient’s struggle for life rather than for death. The fear of repeating a suicide attempt appears to have a protective function. At the same time, an experience of connectedness is an awareness of responsibility in life and emerges as a value having a strong preventive power. The suicide attempt can be a turning point at which juncture it can be assessed whether the struggle to live is worth continuing. The social network of family and friends is experienced as a significant resource. To encounter health personnel who stimulate hope, who are accessible and who adapt help to the needs of the individual are all perceived as crucial to strengthening the desire to live.
Empirical findings in this study support the ethical responsibility of health personnel working with patients in suicidal crises. Professionals must both invite patients to talk about suicidality and at the same time keep focus on the patient’s reasons for living. This study demonstrates that it may be very important to give experiences of connectedness space in the dialogue. The study also appears to demonstrate that the suicidal person’s network should be given greater attention than it is given currently. Services that are available and flexible must be further developed so that the threshold for asking for help is seen as reasonably manageable for both persons in suicidal crises and for the persons closest to them. At the same time, health personnel continuously need to talk about and discuss their own attitudes and values in encountering persons who have attempted suicide.
The need to assist the next of kin and persons close to the patient so as to enable them to support the suicidal person while also taking care of themselves, particularly when suicidality is prolonged over a period of time, may be an area for further research.
Footnotes
Acknowledgements
The authors want to thank the participants for sharing their experiences.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.