
Abstract
Introduction:
To meet and take care of people with dementia implicate professional and moral challenges for caregivers. Using force happens daily. However, staff also encounter challenges with the management in the units. Managing the caretaking function is also significant in how caretakers experience working in dementia care.
Purpose:
The purpose of this study is to explore the caregiver’s experiences with ethical challenges in dementia care settings and the significance of professional leadership in this context.
Method:
The design is qualitative, and data appear through narrative interviews. A total of 23 caretakers participated in the study. The transcribed interviews were subjected to a phenomenological-hermeneutical interpretation.
Ethical considerations:
The respondents signed an informed consent for participation prior to the interviews. They were assured anonymity and confidentiality in the publication of the data. Ricoeur’s method for interpretation ensures anonymity as the researcher relates to the data as one collective text. The study is part of a larger research project in ethics, in its entirety approved in line with the Helsinki Convention.
Results:
The findings show that the caretakers experienced inadequacy. Some of them described a negative work atmosphere where they experienced that their leaders did not take them seriously. Because of this, informal negative sub-groups functioned as an exclusive debriefing arena. Some of the informants described the opposite experience where the leaders actively supported them.
Discussion:
The analyses of the findings are discussed in light of the concepts of trust and mistrust in leadership.
Conclusion:
There is a correlation between the leadership and the caregivers’ experience of being in difficult situations.
Introduction
To be a professional caretaker means to work with vulnerable people who have limited abilities to take care of themselves. People suffering from dementia are particularly vulnerable since their disease influences their ability to make judgments, including their ability to make well-considered decisions. To meet and take care of these patients challenge the caretaker, professionally and morally. 1 However, it is not just the encounter with patients that creates challenges. Managing the caregiving function also influences how caregivers experience their work in dementia care. 2 Several studies show that caregivers, in caring for older people, daily experience ethical challenges that create demanding tasks in their everyday work. 3 –5
In a study by Jakobsen and Sørlie, the caregivers daily experienced encountering difficult ethical situations related to the use of force. The caregivers experienced that it was painful and stressing to take moral responsibility for these situations. Several studies confirm this. 6,7 Moral challenges in healthcare are often unpredictable. This reinforces the caregivers’ experience of frustration in their work. 3,7 –9 Work frustration is always the result of requirements that are linked to work itself. They may also be defined as requirements from the management and organization. 8 –10 Caregivers are also expected to master the challenges they encounter in dementia care. 4 These requirements are, however, not unequivocal. The caregivers often have to choose between loyalty to the patient, to themselves, or to the management. 11,12 Jakobsen 1 confirms this in her study. She found that caregivers felt they had to go against the work culture and the management in order to deliver good care. Experiencing conflicting values daily not only creates frustrations. It also effects the work culture negatively. 6,8,13 –15 This is in line with Pauly et al.’s study. 16 They found that the role of the leader had a significant influence on the ethical climate and created moral distress in the workplace. They uncovered multiple factors that influenced perceptions of the ethical climate and the development of moral distress, among others, the role of the leader. 16 The complex nature of the work environment with increased stress creates challenges for leaders in healthcare organizations. 17
The purpose of the study
The purpose of this study is to explore the caregivers’ experiences with being in ethically difficult situations in nursing homes and the significance of professional leadership in this context.
Method
The study builds on a qualitative design where data appear through narrative interviews. Lindseth and Norberg’s 18 phenomenological-hermeneutical method for research on life experiences is chosen as the method of interpretation. This method is previously used in several studies describing ethics and care practice. 1 –3,19 –22
Participants
The informants’ working experience in dementia care ranged from 1 to 25 years. Although their education varied and they had different functions in the nursing home, they all had direct contact with patients in their daily work.
The informants’ positions.
The narrative interview
The data consist of 23 transcribed interviews, lasting from 20 to 40 min, recorded and transcribed verbatim. Told and interpreted narratives from peoples’ experiences are, according to Polkinghorne 23 and Lindseth and Nordberg, 18 particularly suitable in accounting for life experiences, including experiences from work with people. Work in nursing homes is about work with people where challenges and actions can be difficult to formulate precisely. Narratives include more than answers to questions. They are when told, made explicit and available for the surroundings where they may be interpreted in a broader context. 24 The caregivers’ experiences are valuable sources in illuminating ethical challenges in healthcare for older people and, in this context, the significance of professional leadership.
The interviews are individual, where just one open question is formulated which in its open form invites to narrate:
25
Tell me about your experiences with being in ethically difficult situations in the nursing home.
The advantage of one simple question is the few leads given by the interviewer and greater room for the informant to focus on personal experiences. The interview situation gives the researcher the possibility to take part in the experience of others by listening to their narratives and subsequently to analyze and interpret the narratives in light of relevant theories. In this way, the study may contribute to developing a greater understanding of the issue of discussion. 22,26
Ethical considerations
The respondents signed an informed consent for participation prior to the interviews on the basis of both verbal and written information. They were assured anonymity and confidentiality about adaption and presentation of the data and publication. Ricoeur’s 26 method for interpretation ensures anonymity as the researcher relates to the data as one collective text. The study is part of a larger research project in ethics, in its entirety approved in line with the Helsinki Convention.
Data analysis
In phenomenology, the central question concerns the meaning of lived experience of the phenomenon, whereas hermeneutics deals with the texts’ meaning or sense and its reference. The phenomenological-hermeneutical method of analysis was, therefore, considered appropriate to investigate the healthcare providers’ experience with ethically difficult situations in their work. 22 In the analysis, the researchers relate to the data material as one text.
The single question invites the informants to express themselves openly through their narratives. Hence, it is up to them to define the situations that are ethically difficult.
The phenomenological-hermeneutical method
26
has three steps: The text is initially openly read and naively repeated in order to catch meanings. It is important to understand the flow in text from what it says to what it implicitly talks about. The naive understanding creates the foundation for the next phase. In the structural analysis, the text is divided into units based on sentences or sections, reflecting the substance that appears to the researcher through the first readings. In this phase, the text’s units of meanings are sorted in line with the purpose of the research for what appears to be a sub-theme and what gradually is considered the main theme. An overview over the interpreted sub-themes and themes will here constitute the findings in the study itself. The last phase, where comprehensive understanding is the question, is a critical interpretation aiming at a comprehensive understanding of the text’s meaning.
22
In the discussion, main phenomena will, relevant for the purpose of this study, be considered in light of own experiences and relevant theory in order to derive new understanding and insight.
Findings
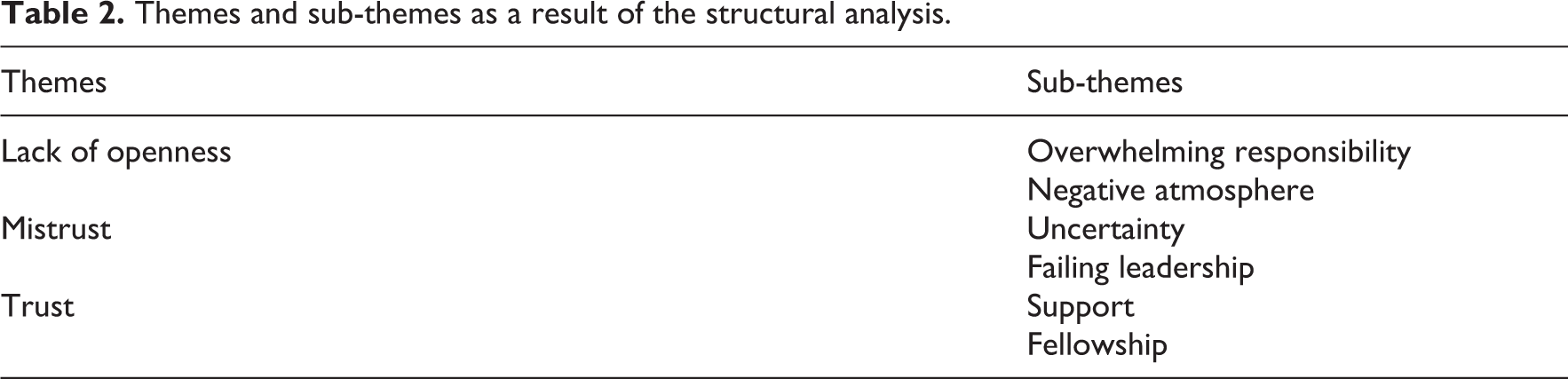
The findings are thematized in sub-themes and themes as shown in Table 2. The themes constitute the headings in the presentation of the findings.
Themes and sub-themes as a result of the structural analysis.
Lack of openness
Overwhelming responsibility
The informants wished that they could speak more openly with their colleagues and leaders. Statements like “I dare not speak up. I speak up, but nobody listens. I see that mistakes are made, but dare not speak up” were frequent in the data. Lack of understanding among colleagues and leaders was the most important reason for their powerlessness. Several of the informants expressed that this affected their health. Not being able to give good enough care affected their conscience: “The patients’ dignity is threatened by lack of competence and lack of personnel on duty. Many are tired.” The informants express concern for the patients, but also for themselves. Stories were told about mistrusting colleagues. They also told stories concerning their frustrations about having to bear the responsibility alone: “I couldn’t take it anymore; I got a long term sick leave.” The informants tell that their frustrations were not taken seriously: Frustrations are not to be talked about. I hit the wall and became powerless and unmotivated. When and how shall I bring things up? I have to be brave and speak up again and again. I wish we had a more open and less defensive work climate. But this really depends on the leaders attitude and her ability to follow-up on what we have agreed on.
Negative atmosphere
Some informants said “I,” whereas others said “we.” Where the care culture appears closed, the narratives focus on “I.” This includes descriptions of very stressed units: “There is a negative mood amongst the personnel. They are tired. The unit has a high frequency of sick leaves.” The caretakers express resignation and exhaustion, due to the lack of resources, competence, and leadership: “We take out our frustration in the duty room, in particular when the leader is absent. It is worse for the unskilled and the summer substitutes. They are not able to discuss their frustrations.” The permanent employees have created their own arena for problem solving. However, it is exclusive and not for everyone: Little by little a divided culture has evolved where some staff members don’t greet each other. Colleagues also talk a lot about each other behind their backs. This creates tension in the work culture. We bring it up, but the atmosphere is not good. Because of this, I prefer to work alone as much possible.
Mistrust
Uncertainty
Several informants tell us that the leaders are vague and unclear about their standards for nursing care. This creates uncertainty among the staff members because they are unsure of what the leaders expect from them. The leaders rarely initiate conversations about their standards of nursing care and the ethical challenges and priorities they have to struggle with.
The staff therefore experience that it is extremely difficult to voice their concerns about ethical dilemmas in the unit: “I often experience that unskilled employees address patients without respect. Unacceptable behaviour is more difficult to correct than practical nursing skills. I don’t know how to get through to the leader about these problems.”
The caregivers experience that the leaders give them too much responsibility. They frequently have to deal with overwhelming situations on their own. Many caregivers experience that they are forced to deliver “conveyor belt care” due to lack of time and resources. They experience that the leaders do not take their concerns seriously when they try to talk with them about their frustrations. Hence, they lose faith in their leaders: It is extremely frustrating not to be listened to. One of our patients is very restless and shouts all the time. The noise really affects other patients and personnel. We have tried to talk with our leader about this. But she just answers that we have to learn to live with the commotion.
Failing leadership
The informants state that poor leadership creates disillusionment in the staff: “It is all about the leaders ability to enable staff cope with the units’ ethical challenges. People become exhausted and frustrated when the leaders stick their heads in the sand.” As an example, the leader’s inability to provide enough skilled nurses on every shift creates resignation: In the evenings in particular, it seems like the leaders “take in” anybody just to have enough staff on the shift. Few skilled nurses diminish the quality of care. Relatives complain that the staff doesn’t understand them. This is reported to the leader. But they don’t do anything about it. It seems like they only care about having enough staff on the shifts, and don’t care about their level of competency.
Trust
The informants also talk about good leadership contributing to a better handling of difficult ethical situations. Here, leaders are described as good role models in the unit.
Support
The leader sets the standard of care in the units: “She often sets the agenda and makes room for discussion. She clarifies expectations and oversees that work is done in accordance with the ethical values.” How the leader does this is described concretely. Knowledge is important: The primary nurse is present in the dr.visitto speak directly about “their” patients. The leader takes part in situations to discuss and confirm choices so that she understands the problems better. This is important for us in order to build competence.
Fellowship
Nurses who trust their leaders often use “we” instead of “I” when they talk about managing challenging situations: We often start our duty discussing ethical problems. The unit’s head nurse asks the personnel to describe difficult situations so we can reach a consensus. We share our experiences and nobody is a winner or a looser. We have all experienced difficult situations. We have a very open work environment, and appreciate discussing difficult situations in the group. We can all learn from good as well as bad experiences.
Discussion
The findings show the caregivers’ experience inadequacy. They all experience ethically difficult situations daily. They describe negative work atmosphere, where people do not greet each other. They also experience that their leaders do not take them serious. There are tendencies to sub-cultures in the wards. However, the criteria for being accepted are not explicitly defined. However, we have narratives about care cultures characterized by a shared whole, where people share experiences and knowledge. In these cultures, the leader is highlighted as a central role model who takes the staff’s challenges seriously.
What makes these units so different? There seems to be a correlation between the staff lack of recognition, poor work climate, and negative sub-cultures. 13,27 There also seems to be a correlation between good leadership and open, supportive care cultures.
The caregivers tell about daily ethically difficult situations related to use of mild force. They are frustrated and risk becoming burnt-out due to these circumstances. Use of force in nursing homes is well documented. 6,7 Several studies document that being in difficult situations makes the staff susceptible to burn out, 3,12 in particular where time is scarce in relation to the tasks, and they have to make difficult priorities. 6 –9,12
The caregivers’ choice of action depends to a great extent on their competence, social and professional support by leader, and operating conditions. 9,10,17,27 –29 The findings in this study support this. Let us look at the unit nurses’ role and significance based on these findings. The unit nurse’s position is the formal leader position closest to care providing. This role is challenging in nursing homes for several reasons. The caregiving is extensive. The frames are limited and the caregivers have a varied competence to meet the patients’ need. 17,29
Nurses, physiotherapists, and other skilled health workers normally safeguard formal competence. The particular challenge is, however, linked to the large number of unskilled employees. This group is to a larger extent more dependent on routines and rules in their work than those with formal skills. They are therefore more dependent on the professional of the care culture in the unit. This appears to be particularly challenging related to care for people with dementia. The difficult situations related to dementia care require competence beyond rules and regulations. Care culture and leadership through guidance and discussions must therefore mirror correct standard. 2,10,30
Leadership is about developing a work culture, where care is given in line with the patients’ and their families’ individual needs. 31 It goes without saying that a leader must trust that the staff members deliver care in line with legislation, professional principles, and the institution’s set of values.
Trust is a central idea in the findings. There are many definitions and reflections on the concept trust. This indicates that the concept is difficult to define. 30,32 With Løgstrup, 33 trust is an expression of life and thus vital between individuals. Under normal circumstances, human beings meet each other with natural trust. 34 Trust is threatened and turns into mistrust under abnormal circumstances. What is to be considered normal and abnormal circumstances is learned through our life cycles. People develop sensitivity to trust—mistrust in relations. Løgstrup 33 claims that trust between people is basic and therefore comes before mistrust. Grimen 30 applies the term trust giver in his texts about trust. A trust giver leaves something to the other, usually in good faith. What does this imply? Good faith may be understood as trusting the one who is given authorities to be able to make reflected choices of action. Trust in good faith can be misused. The trust giver, hence, takes a chance making himself or herself vulnerable. 30 According to Luhmann, 35 showing trust is a gamble.
In this study, the term is actualized on several levels. The leader can be understood as a trust giver delegating responsibility and decision power to the caregivers. The leader takes a chance by handing over responsibility, trusting and expecting that this will be handled in the best possible way. 9 When informants experience that their leaders do not see or hear them, the condition of trust is challenged. How? Let us answer with the following question: Can a leader misuse his or her role as trust giver? In organizations where people’s lives and health are in question, leadership is about mobilization of common commitments through interpersonal interaction. 9 In this statement, the leader, the trust giver, is given an active role through the terms “mobilizing” and “interaction.” Therefore, the leaders as trust givers bear the responsibility, even when they delegate it, and trust that the caregivers will safeguard it. Hence, it is not just the trust recipients who have power to choose how the given trust should be managed. Trust givers also have the power to choose how to follow up their part of the responsibility. 32 According to some of the nurses in this study, it is reasonable to assume that misused trust becomes a disclaimer. 27,30
When the care providers claim that they are not heard or seen despite extensive challenges in their work, it is reasonable to call the leader’s attitudes indifferent where trust at a certain point turns into mistrust. According to Grimen, 8,32 it is possible to understand this thinking as a leader’s chosen position, conscious or unconscious. They can defend their choices through the delegated responsibility. It is, therefore, reasonable to characterize this choice as a kind of power display. Leaders can choose their position and action toward care providers as care providers can do toward patients. The result of the leaders’ choices may be perceived as mistrust. This may trigger other reactions in the work culture. As in this context, leaders, trust givers, assign responsibility to the individual caregiver. The caregivers on the other hand experience difficult situations in the unit and demand a distinct leader as advisor, coach, and role model. They need to be seen and heard in their everyday challenges. 9,17,27,29 It is possible to call this institutionalized mistrust. In this case, the leadership leaves an extensive moral and professional responsibility to the caregivers without dealing with the challenges that go with this responsibility and which qualifications the staff possesses to safeguard this trust. The leaders so to speak hand over their responsibility, despite the consequences this may cause for those given such trust and for the patients receiving the care this trust is about. 9,27,35 To give trust in care work is not about leaving total responsibility to the one receiving trust. It is also about actively relating to this trust by, for instance, asking whether the person in question is worthy of this trust. 9 Caregivers’ frustrations and feelings of not being heard when they speak up indicates that the leaders do not relate actively to the trust given. The caregivers say that it is important that leaders set the standards, act as role models, and take frustrations seriously. When this is absent, it is possible to understand the caregivers’ perception of the leader as indifferent and neglectful, a leader not trusted to resolve issues. Consistent mistrust has a greater psychological cost than trust. Mistrust demands a much greater vigilance than trust. 30 The caregivers become exhausted since nothing helps. Is there possibly a connection between an established negative sub-culture in a unit and lack of trust in the leader?
In the study, frustrations are handled in exclusive and informal sub-cultures. Not everybody in the units is included, for instance, extra staff and students are excluded. When frustrations about lacking leadership take a lot of attention, the informants talk about the group as a place for “survival” and is the reason why they continue to work there. At the same time, there are other caregivers in this culture who define such a sub-culture as very unfortunate for the work environment, and they consider leaving. Sub-cultures can be negative as well as positive for the work culture. They are positive because they create a sense of belonging and identity. They are negative when they create exclusivity resulting in a split culture. 13,27 In this study, it is possible to see the sub-cultures as a way of dealing with perceived poor leadership. It may lead to survival for some, whereas others use the term “bad atmosphere,” poor cooperation, as is the case where some colleagues do not greet each other. What is remarkable in the study is that where distrust was high in the units, they are the ones characterized by poor atmosphere and creation of sub-cultures. This is in line with Fukuyama 13 who shows the correlation between mutual trust among employees and leaders and the degree of job satisfaction. Other studies support this. 9,16,17,27,29 The concept of trust is close to the concept of respect. 36 There seems to be a lack of respect for the moral challenges and the intensity of moral distress in the working environment. This lack of respect is experienced between the leader and the caregivers, as well as between the caregivers. There seems to be a correlation between the leaders’ lack of respect and the caregivers’ experiences of moral distress and mistrust. This is in line with Pauly et al. 16 who found a correlation between moral stress intensity and perceptions of ethical climate, where leadership was found to be significantly correlated to moral distress.
The data material also shows another side of trust and work culture. Some caretakers experience to be seen and heard. A good leader, as seen by the caregivers, is thus one who acknowledges their difficult ethical situations and contributes through collective reflections in order to extend the room for action and form the basis of decisions in similar situations. 1,9,27 The good leadership demands acknowledgement and respect for the challenges the care work creates. The leader uses the positive power in the leader position. It is about normative power and persuasion. 16,17,27,29,37 By being a role model, mastering the profession, expectations, assessments, and choices of action become apparent for the staff. The leader is visible in the unit and confirms and challenges without threatening the trust given. With this approach, challenges appear as a collective responsibility, not individual. The challenges are ours, not mine. The cultural unity thus becomes a united concern where the individual care provider experiences to belong, and where it is easier to relate to the difficult ethical situations than when the leader appears to be indifferent. These results are supported by the studies of Wong and Laschinger 29 and Busch, 36 which show that the more managers are seen as authentic, by emphasizing transparency, balanced processing, self-awareness, and high ethical standards, the more nurses perceive they have access to workplace empowerment structures, are satisfied with their work, and report higher performance.
Summary
In dementia care where ethically difficult situations are experienced on a daily basis, it seems particularly necessary to have a leader who creates trust by delegating responsibility and actively follow up the responsibility given. The caregivers’ narratives bear witness to two different work cultures where the leader’s role turns out differently. Where trust between caregivers and leader is great, the culture seems to be able to meet the ethically difficult situations. You find disharmonious cultures where the relationship between leaders and care providers is characterized by distrust. Disharmonious cultures are characterized by stress and disillusioned caregivers, where ethically difficult situations are heightened and individualized.
Methodological considerations
This study has a qualitative design, and it is not appropriate to discuss concepts of validity, reliability, and generalizability in their traditional senses. The phenomenological-hermeneutical interpretation is about lived experiences and will inextricably be linked to the interpreter’s interpretation. The informants have been posed one open question. The results have been gleaned through the interpretation of the transcribed narratives. They can be used to illustrate the meaning of lived experience and influence people in how they perceive their lives, in this case around trust and leadership in nursing homes. Thus, it is possible to say that this is not about documenting the truth but rather to present experiences the way the informants tell them based on their understanding and how the interpreter perceives it, based on his or her understanding. Accuracy in interpretation is, therefore, important in deriving knowledge from the material. Loyalty to the narratives is essential in the reflections. Further studies are recommended around trust, leadership, and healthcare.
Footnotes
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.