
Abstract
Background:
The Taiwan Nursing Accreditation Council has proposed eight core professional nursing qualities including ethical literacy. Consequently, nursing ethics education is a required course for student nurses. These courses are intended to improve the ethical literacy. Moral sensitivity is the cornerstone of ethical literacy, and learning moral sensitivity is the initial step towards developing ethical literacy.
Objectives:
To explore the effect of nursing ethics educational interventions based on multiple teaching strategies on student nurses moral sensitivity. Based on the visual, auditory and kinaesthetic model, three strategies were developed for determining the programme components and corresponding learning styles.
Research design:
This was a quasi-experimental study.
Participants:
A total of 234 junior-college student nurses participated in this study. All participants were aged 18–19 years.
Ethical considerations:
The study protocol was approved by the institutional review boards of Kaohsiung Veterans General Hospital. Only the participants who signed an informed consent form took part in the study. The participants were permitted to withdraw from the study at any point if they wished to do so without affecting their academic score.
Results:
The scores of Modified Moral Sensitivity Questionnaire for Student Nurses were significantly improved after the intervention of integrating multiple teaching strategies (p = .042). Significant relationships were observed between the satisfaction scores of two teaching strategies and moral sensitivity. The results indicated that using multiple teaching strategies is effective for promoting nursing ethics learning.
Conclusion:
This strategy was consistent with the student nurses’ preferred learning style and was used to correct their erroneous ethical conceptions, assisting in developing their ethical knowledge.
Keywords
Introduction
The Taiwan Nursing Accreditation Council has proposed eight core professional nursing qualities including ethical literacy. Consequently, nursing ethics education is a required course for student nurses (SNs) in Taiwan. These courses are intended to improve the ethical literacy. Moral sensitivity is the cornerstone of ethical literacy, and learning moral sensitivity is the initial step towards developing ethical literacy. When SNs possess moral sensitivity, they can empathise with their patients’ needs, promote their patients’ rights and interests, and endorse their patients. 1 Morally sensitive people are aware of their roles and corresponding responsibilities in moral or ethical situations; 2 thus, they maximise benefits for their patients and enhance service quality. 3,4 Hence, nursing ethics education should be aimed at developing moral sensitivity among SNs.
Numminen et al. 5 contended that nursing ethics education provides SNs with the opportunity to recognise professional ethical problems, practise ethical decision making, establish amiability/virtue/attitude/values, and learn to apply ethical rules in changing work environments. Teaching strategies for nursing ethics education include lectures, group discussions, case studies, 6 and dialogue as well as problem-based learning, which was first applied to nursing education in 2003. 7
Teaching effectiveness is greatly enhanced when teachers develop teaching strategies on the basis of various student learning styles. The visual, auditory and kinaesthetic (VAK) model is a commonly used teaching model. This model is based on the concept that individuals’ instructional mode preferences differ. 8 This model involves three fundamental types of learning style, namely, VAK learning. Visual learners have visual skills and are accustomed to learning through sight; auditory learners tend to acquire knowledge by listening, and they learn most effectively through verbal speech, discussions and listening to others; and kinaesthetic learners tend to acquire knowledge through bodily actions, such as touching and doing. According to the VAK model, most students have a preferred learning style or mixed learning styles, 9 and the VAK model can enable course designers to adjust course teaching methods to student learning styles 10 in order to assist students in acquiring knowledge and skills.
This study integrated three teaching strategies (reading Nightingale’s Diary, 11 analysing the personal experiences shared by kidney transplant patients and one practising clinical ethical decision making according to the Four-Topic Approach 12 ) for an intervention to develop SNs’ moral sensitivity.
Objectives
The two research questions are outlined as follows: Does SNs’ moral sensitivity change after nursing ethics educational interventions that are based on multiple teaching strategies? How do nursing ethics educational stress level change after nursing ethics educational interventions that are based on multiple teaching strategies?
Methods
Study design and participants
This was a quasi-experimental study. A pre-test involving the Modified Moral Sensitivity Questionnaire for Student Nurses (MMSQ-SN) and the stress of learning nursing ethics (SNE) was administered to SNs in a nursing ethics course during week 1, and intervention was performed using multiple teaching strategies for 12 weeks, including (1) reading Nightingale’s Diary, (2) analysing the life experiences shared by kidney transplant patients and (3) practising ethical decision making. A post-test involving the MMSQ-SN, the SNE and the satisfaction of multiple teaching strategies (SMTS) was administered during week 17.
The participants in this study were 250 year-3 SNs of a 5-year junior college programme who were enrolled in a college nursing ethics course. Participants were excluded if they had requested more than 6 h of leave from the nursing ethics course or had emotional or mental problems including depression. Before participating in the study, they were briefed, after which they consented to their inclusion in the study.
Programme design
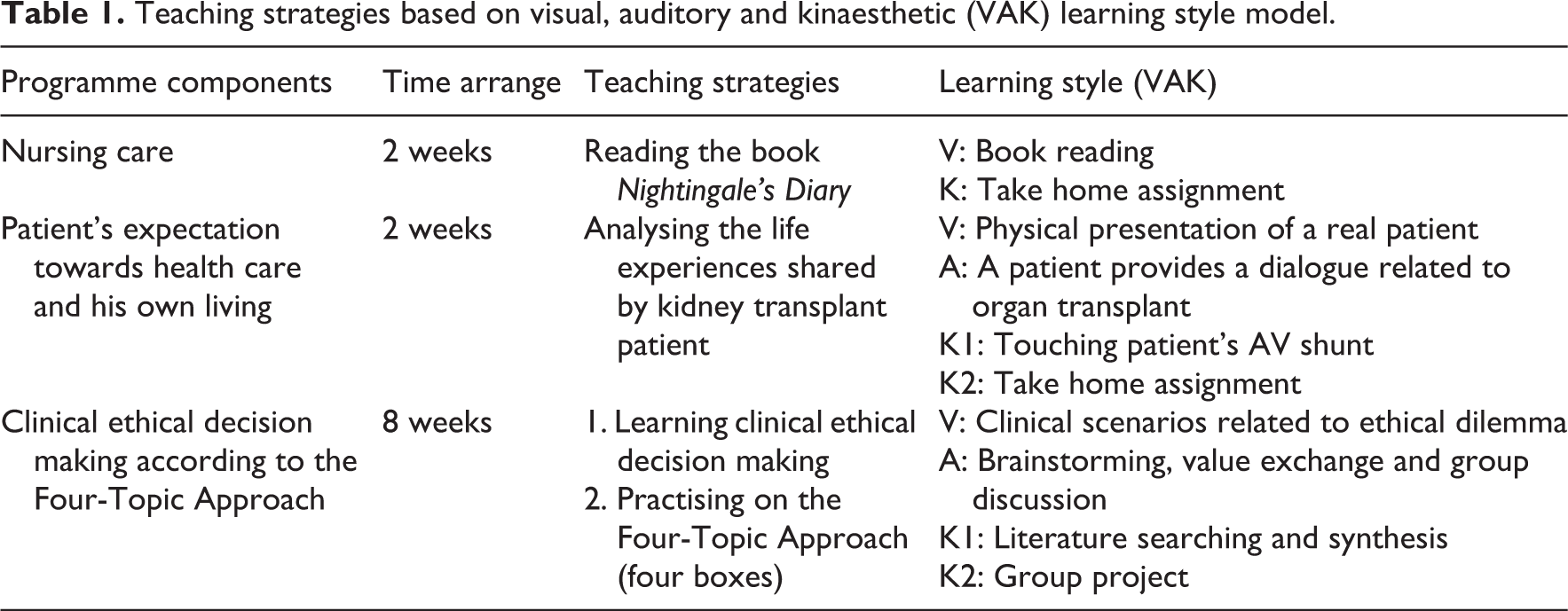
The research design is described in Table 1. The VAK model was used to teach nursing ethics. Three strategies were developed for determining the programme components and corresponding learning styles. The first teaching strategy focussed on the value of nursing care; the course topics were ‘reading Nightingale’s Diary and completing home assignments’. The visual learning style involved reading a book, and the kinaesthetic learning style entailed completing writing assignments. The second teaching strategy emphasised ‘Patients’ healthcare and life expectations’, and the course topic was kidney transplant patients’ sharing of personal experiences. The visual learning style involved the physical presentation of an actual patient, whereas the auditory learning style entailed a patient engaging in dialogue related to an organ transplant. Moreover, the kinaesthetic learning style involved SNs’ touching a patient’s arteriovenous shunt and completing an assignment. The third teaching strategy focussed on ‘ethical decision making’; the participants engaged in clinical ethical decision-making learning and practice according to the Four-Topic Approach. 12 The visual learning style entailed reading descriptions of clinical scenarios involving ethical dilemmas; the auditory learning style involved brainstorming, exchanging values and group discussion; and the kinaesthetic learning style involved researching and synthesising the literature, exchanging values and group discussion.
Teaching strategies based on visual, auditory and kinaesthetic (VAK) learning style model.
Teaching strategy implementation
This section explains the three teaching strategies. The first strategy was to encourage the SNs to read Nightingale’s Diary. This strategy involved the visual and kinaesthetic learning styles. The SNs read Nightingale’s Diary, understood the model of the nursing profession and proposed numerous nursing concepts that merited exploration and learned for 2 weeks. Florence Nightingale believed in nurse training that focuses on developing a nurse’s character, senses, mind and spirit. 11 The SNs learned about Nightingale’s proactive care for people, her passion and her active involvement in life. Nightingale’s Diary states the following: (1) SNs must be willing to learn and have stable personalities, (2) interpersonal interaction is based on morality and spirituality and (3) nurses reflect on nursing and are ethical. After reading Nightingale’s Diary, the SNs gained a strong sense of responsibility. 13
Under the second strategy, the educator invited a dialysis and kidney transplant patient to share his life experiences and his mission to promote the love of life with the SNs. The SNs discussed the ethics of clinical organ transplantation, increasing their ability to analyse situations involving ethical values. The second teaching strategy entailed VAK learning styles. By conversing with a patient, the SNs understood the ethical dilemma confronting this patient and the temptation to engage in organ trading. The course continued for 2 weeks. SNs can internalise knowledge when they learn to focus on the life experiences and listen to the kidney transplant stories of the case, dialogue with the case and the completion of home assignments.
Numminen and Leino-Kilpi 14 found that practising ethical decision making was crucial in teaching nursing ethics. Therefore, the third teaching strategy in this study entailed practising the Four-Topic Approach to ethical decision making, and it included VAK learning styles. Moral sensitivity plays a major role in nurses’ ethical decision making. Ethics education involving SNs’ discussing their experiences with ethical issues in clinical practice was effective for developing moral reasoning skills in SNs because this type of education enables SNs to engage in more ethical refelction. 6 Moral sensitivity is a personal attribute and a crucial factor in decision making regarding patient care. 15 Ethics education involving SNs’ experiencing ethical issues in clinical practice was effective for developing moral reasoning skills in SNs because SNs are provided with the opportunity to reflect on their previous experiences during ethics instruction, 16 and SNs can practise ethical decision making if necessary. Ethical decision making is the process of recognising ethical issues, exercising moral reasoning and assessing key values. 17,18 However, how can the ethical decision-making capabilities of nurses be improved? SNs are relatively lacking in opportunities for judgement and training on nursing ethics. 19 When SNs enter the workforce to complete internships or serve as new nurses, they possess an additional defence, which functions like a vaccination. A nurse that has diligently practised ethical decision making has stronger moral judgement capabilities than a nurse who has never practised ethical decision making does. 20 A nurse who has practised ethical decision making more effectively understands the responsibilities and roles played by a nurse when entering the workforce. In this study, the Four-Topic Approach was used as the ethical decision-making model for the interventions. Under this model, SNs use four topics to identify and analyse ethical problems regarding patients. 12 Such analyses support ethical decision making. The four topics are medical and nursing indications, patient references, quality of life and contextual features.
The third teaching strategy entailed the Four-Topic Approach, which was used for 8 weeks. During week 1, the teacher introduced the approach to the SNs and explained the case study. During week 2, the SNs practised decision making based on this approach (Figure 1).
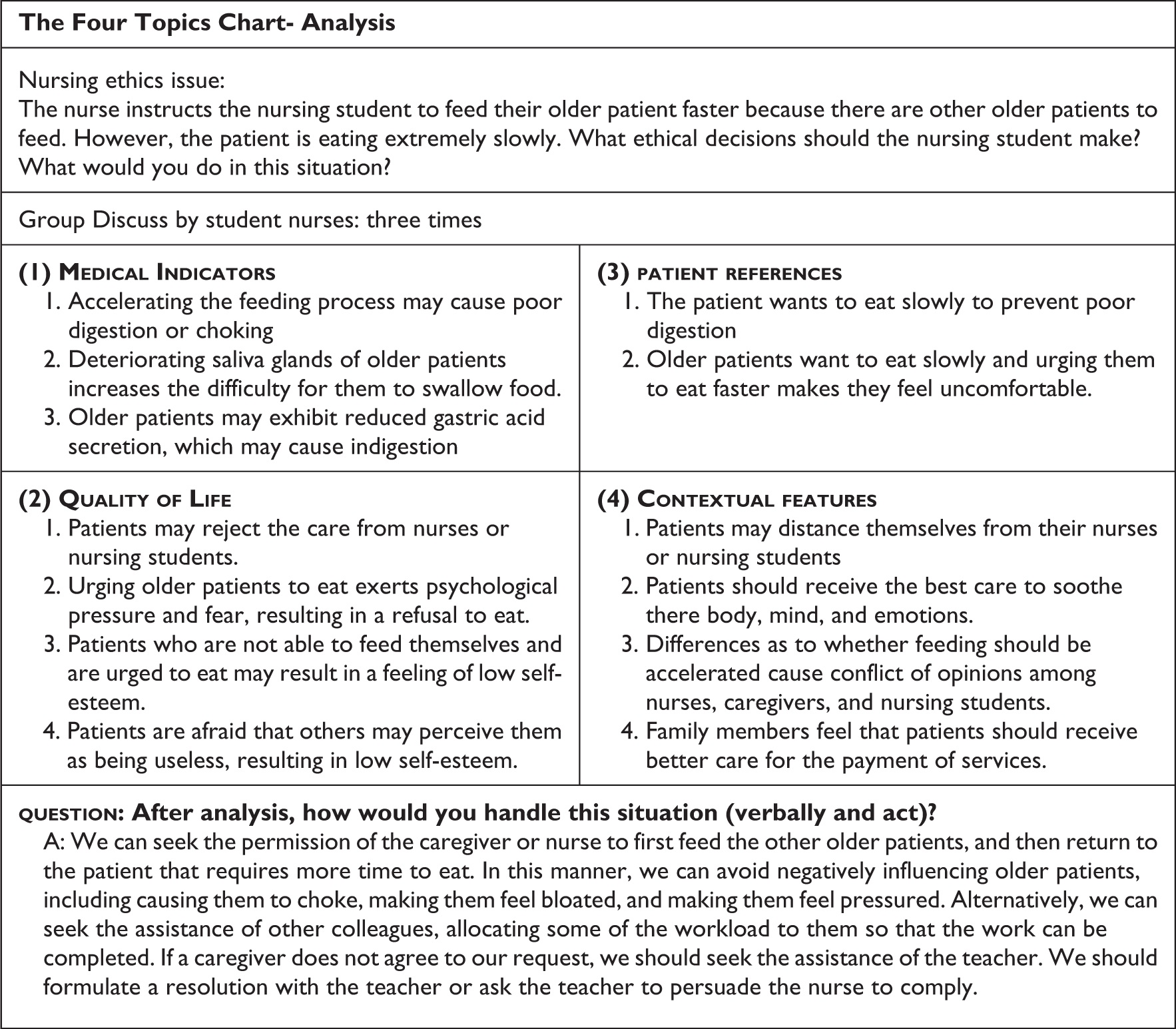
Practising the Four-Topic Chart Approach to ethical decision making.
The class was divided into eight groups, all of which discussed the same ethical issue. Each group was instructed to write its decisions on the blackboard, introduce their decision making to the classmates and explain the reasons for their decision. The groups then engaged in discussion. During week 3, the ethical issue for the final report was discussed. SNs were instructed to identify literary resources, engage in group discussion, and employ the Four-Topic Approach to complete their closing report. This strategy was used for approximately 8 weeks.
The effectiveness of teaching interventions may be influenced by the ethical teachings of other courses or the occurrence of ethical problems in clinical practice. Therefore, in this study, an intervention period was selected during which the SNs were not required to participate in an internship. In addition, this study confirmed that, among the 34 credits (612 h) per semester required for graduation, only 1.6% (10 h) of the credits required ethical coursework.
Instruments
MMSQ-SN, 21 Comrie’s authorised by Lützén for adaptation to SNs, was used in this study. This moral sensitivity scale was employed with the authorisation of Comrie and Lützén. The MMSQ-SN includes six categories: expressing benevolence (EB), structuring moral meaning (MM), interpersonal orientation (IO), experiencing conflict (EC), modifying autonomy (MA) and professional knowledge (PKN), with scores from 1 (strongly disagree) to 7 (strongly agree). The scale includes 30 items, and SNs’ agreement with the statements in the items is measured using a 7-point Likert scale with anchors ranging from 1 (strongly disagree) to 7 (strongly agree). Comrie’s scale had a reliability level (Cronbach’s alpha) of .63, 5 but the scale in this study achieved a reliability level (Cronbach’s alpha) of .852.
SNE
The scale for the SNE was developed by reviewing the literature on personality traits, interpersonal relationships, work stress and learning stress, and statistics on the frequency of SN stress were obtained using the 5-point Likert scale anchored by 1 (never), 2 (occasionally), 3 (half the time), 4 (often) and 5 (always). The score of each question was summed to determine the frequency of the SNE. The reliability of the SNE (Cronbach’s alpha) was .922.
SMTS
The satisfaction with the teaching strategies (reading Nightingale’s Diary, analysing the sharing of patients’ life experiences and practising ethical decision making) was measured on a 5-point Likert scale to determine the level of agreement (1: ‘strongly disagree’; 2: ‘slightly disagree’; 3: ‘neutral’, 4: ‘slightly agree’ and 5: ‘strongly agree’). The reliability (Cronbach’s alpha) of the SMTS was .952.
Ethical considerations
The study protocol was approved by the institutional review boards of Kaohsiung Veterans General Hospital (130510-2). Two researchers explained the purpose and importance of the study to participants. Only the participants who signed an informed consent form took part in the study. All participants were older than 18 years. However, if they were younger than 20 years, their parents or guardians received a letter with study information and their written consent were appreciated. The participants were permitted to withdraw from the study at any point if they wished to do so without affecting their academic score. The participants took about 20 min to fill out the questionnaire. Participants who completed the questionnaire received a small gift for their participation.
Statistical analyses
Descriptive statistics were provided for research participant demographics, including frequency and percentages. A Pearson’s product-moment correlation test was conducted for determining the participants’ correlation was based on the scores of the MMSQ-SN, SNE pre-test and post-test, and SMTS. A paired t test was conducted to determine any changes in the pre-test and post-test scores of the MMSQ-SN or the SNE after the nursing ethics education intervention.
Results
Participant demographic data
A total of 234 SNs participated in this study; 227 (97%) were females and 7 (2.9%) were males, 92 (39.3%) were firstborn children, 110 (46.8%) held no religious views, 204 (87.9%) lived in urban areas, 109 (46.6%) education of the key person impact to student nurses’ ethical values was college and 79 (33.6%) occupation of persons influencing student professional ethics are professional work. In this study, no significant difference was observed between demographic variables (e.g. gender, birth order, religion and living area) according to the MMSQ-SN (p < .05). Only various occupations of the major ethically influential agents generated a significant difference (p < .05) for the MMSQ-SN results, with semi-professional occupations being associated with the highest MMSQ-SN scores (Table 2).
Comparison with participants’ demographic data on MMSQ-SN (n = 234).
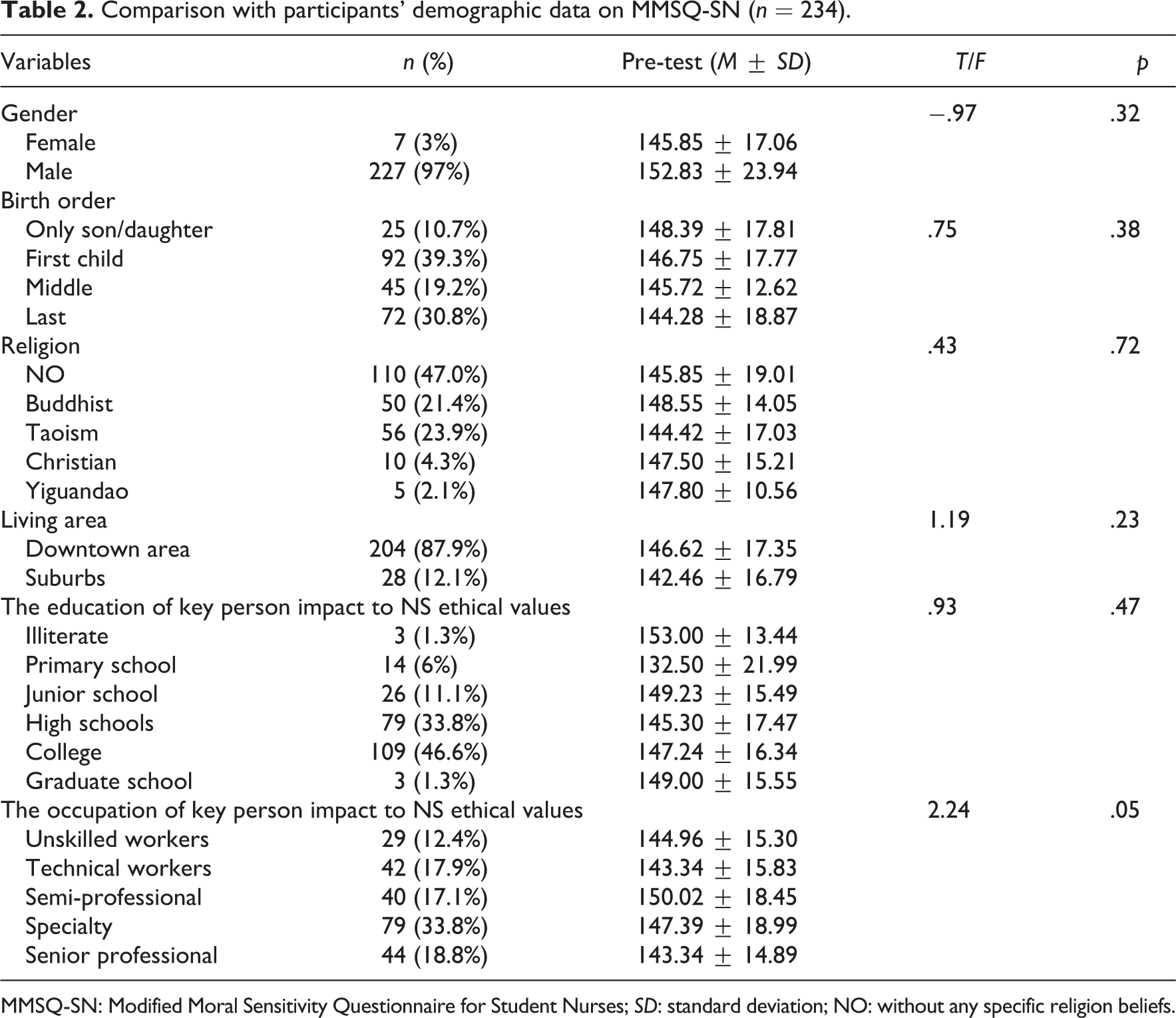
MMSQ-SN: Modified Moral Sensitivity Questionnaire for Student Nurses; SD: standard deviation; NO: without any specific religion beliefs.
Changes in student moral sensitivity
The results demonstrated the following. (1) Reading Nightingale’s Diary did not significantly correlate with MMSQ-SN scores (p < .05). (2) Analysing the personal experiences shared by kidney transplant patients significantly correlated with MMSQ-SN post-test scores (r = .177, p < .01), and practising ethical decision making significantly and positively correlated with MMSQ-SN post-test scores (r = .138, p < .05; Table 3). Therefore, after the implementation of the multiple teaching strategies, the post-test MMSQ-SN scores of the SNs significantly exceeded their pre-test scores (p = .042; Table 4). Comparing the pre-test and post-test results revealed that the MMSQ-SN EB, MM and MA category scores increased significantly, whereas no significant differences were observed in the remaining categories (Table 4).
The correlation of MMSQ-SN, SNE and SMTS in student nurses (n = 234).
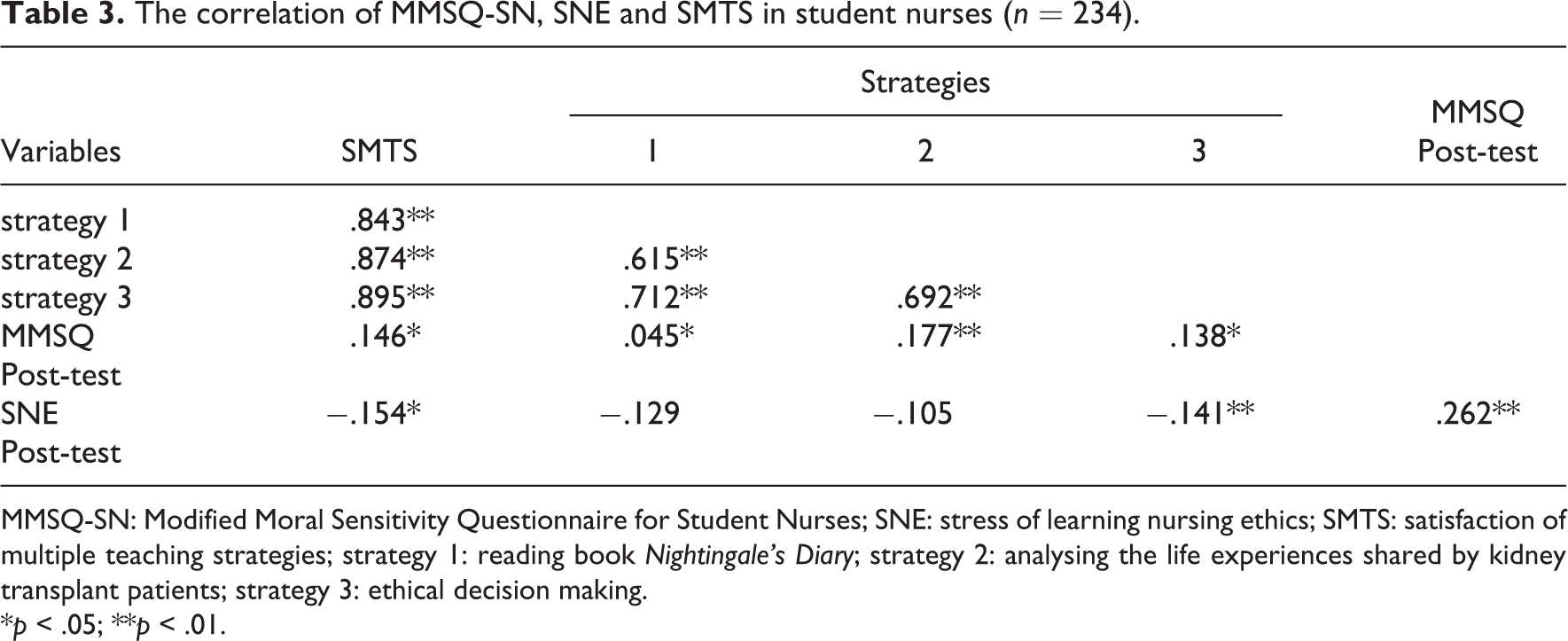
MMSQ-SN: Modified Moral Sensitivity Questionnaire for Student Nurses; SNE: stress of learning nursing ethics; SMTS: satisfaction of multiple teaching strategies; strategy 1: reading book Nightingale's Diary; strategy 2: analysing the life experiences shared by kidney transplant patients; strategy 3: ethical decision making.
*p < .05; **p < .01.
Comparison pre-test with post-test on MMSQ-SN and SNE (n = 234).
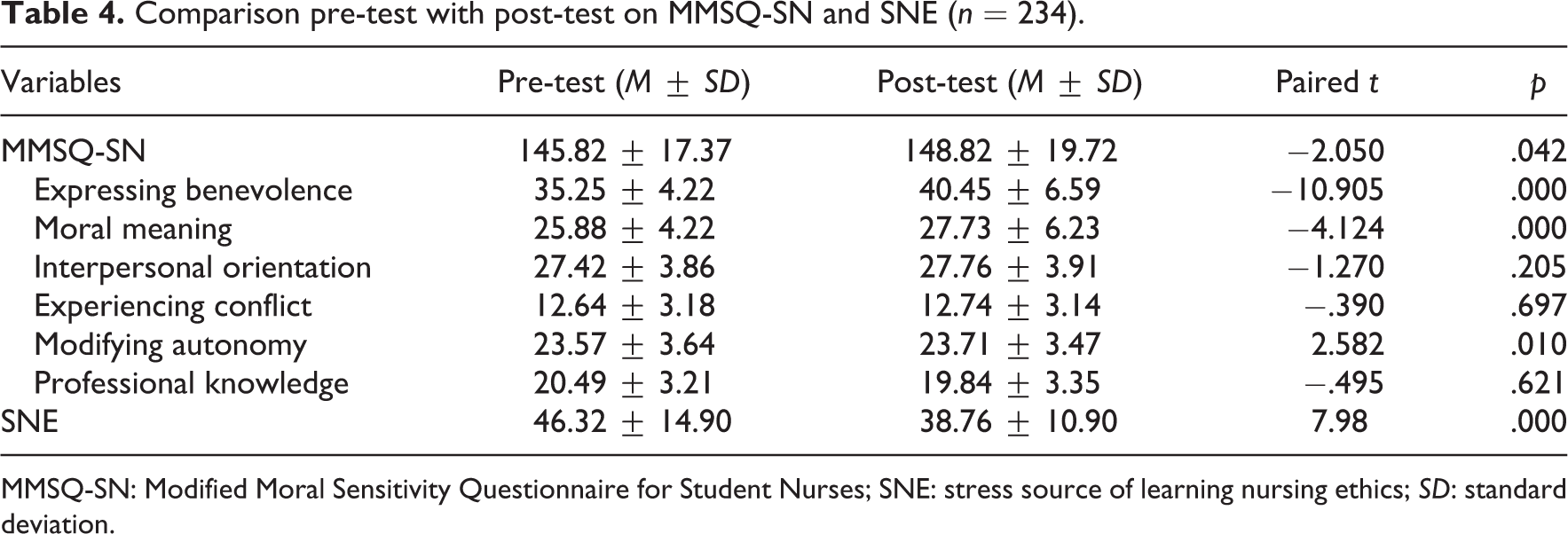
MMSQ-SN: Modified Moral Sensitivity Questionnaire for Student Nurses; SNE: stress source of learning nursing ethics; SD: standard deviation.
Comparison pre-test with post-test on item score of MMSQ-SN (n = 234).
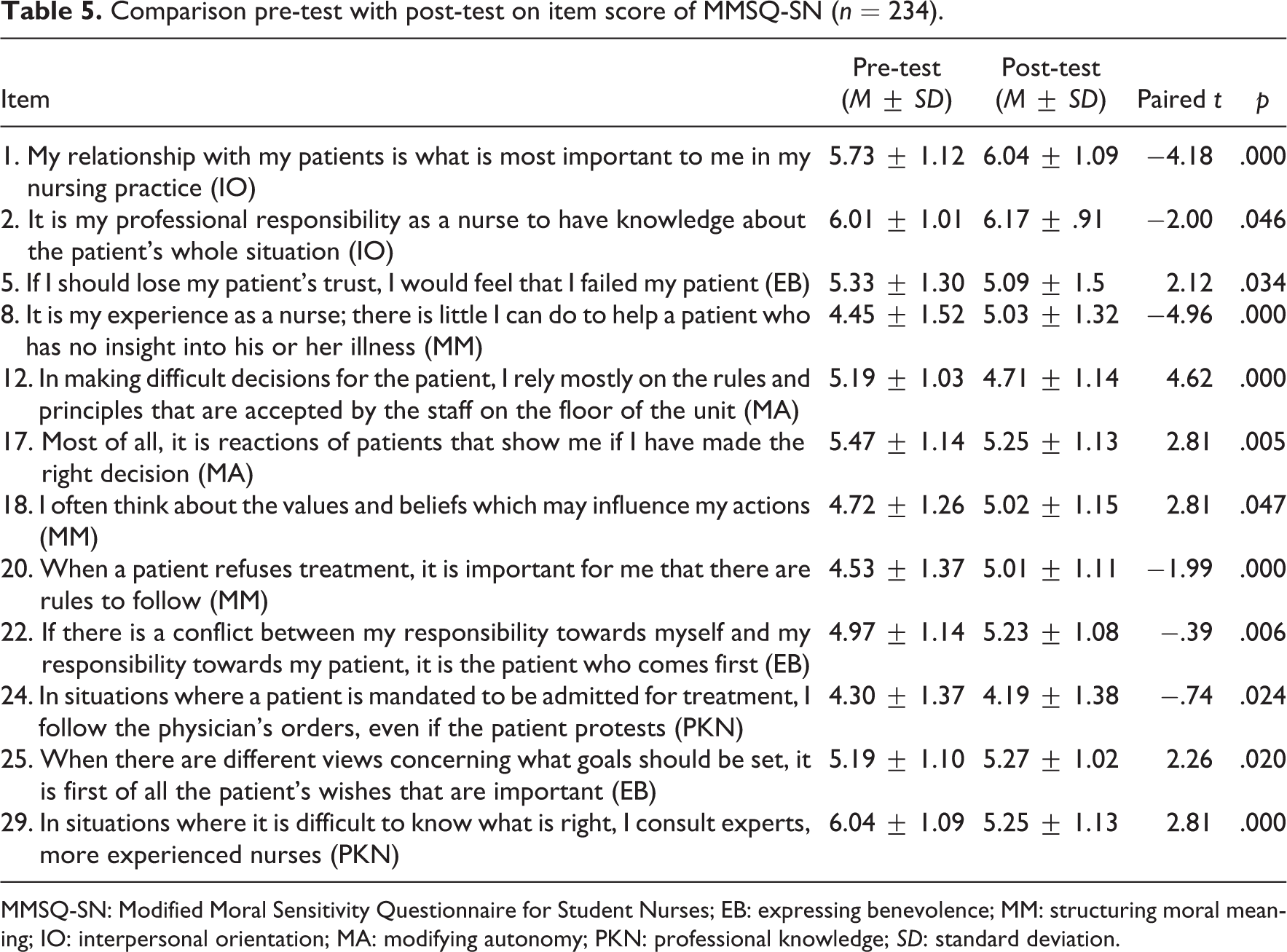
MMSQ-SN: Modified Moral Sensitivity Questionnaire for Student Nurses; EB: expressing benevolence; MM: structuring moral meaning; IO: interpersonal orientation; MA: modifying autonomy; PKN: professional knowledge; SD: standard deviation.
A comparison of the pre-test and post-test scores of each item in the MMSQ-SN indicated that the post-test scores of eight items significantly exceeded the pre-test scores. These eight items were contained in the following categories: IO (two items), MM (three items), EB (two items), and MA (one item). However, four items had post-test scores that were significantly lower than their pre-test scores. These four items were contained in the following categories: MA (one item), PKN (two items), and EB (one item). Items with significantly higher post-test scores in the MMSQ-SN corresponded to the perspectives with significantly higher post-test scores in the MMSQ-SN categories (Table 5).
In week 1, for all SNs, Item 7 (‘I believe that “effective” nursing care includes respecting the patient’s self-choice’.) received the highest MMSQ-SN score, reflecting that the SNs respected patient autonomy; in week 17, Item 2 (‘It is my professional responsibility as a nurse to possess knowledge of a patient’s entire situation’.) received the highest MMSQ-SN score, signifying that the SNs emphasised nursing professionals’ duty to entirely understand patients. The lowest ranked item among SNs was Item 29. (‘I am occasionally motivated to threaten the patient with an injection by force if he or she does not voluntarily agree to use the medicine that is prescribed’.) Thus, the SNs perceived that threatening or coercing patients into obedience is unethical.
Changes in the stress of learning nursing ethics among SNs
No significant difference was observed among demographic variables (e.g., gender, birth order, religion and living area) according to the SNE (p < .05). The results demonstrated the following: (1) the agreement scores of reading Nightingale’s Diary were not significantly correlated with the SNE post-test scores (p > .05), (2) the agreement scores of analysing the personal experiences shared by kidney transplant patients significantly correlated with SNE scores (p > .05) and (3) the agreement scores of ethical decision-making strategies significantly and negatively correlated with the SNE post-test scores (r = −.141, p < .01). Only ethical decision-making strategies significantly reduced SNE scores. Hence, the SNE post-test score (38.76 ± 10.90) decreased significantly compared with the SNE pre-test score (46.32 ± 14.90; paired t = 7.98, p = .000; Table 3). This showed that SNs’ SNE decreased significantly after 16 weeks. The top five reasons for the SNE in week 1 were as follows: (1) tight assignment deadlines, (2) assessment anxiety, (3) excessive workload during year 3, (4) anxiety regarding performance and not fulfilling the course objectives and (5) lack of time-management knowledge. The top five sources of the SNE in week 17 were as follows: (1) assessment anxiety, (2) tight assignment deadlines, (3) anxiety regarding performance and not fulfilling the course objectives, (4) excessive workload during year 3 and (5) lack of time-management knowledge. These five items were SNs’ stress sources throughout the semester.
SNs’ agreement with the multiple teaching strategies
The SNs’ agreement with the multiple teaching strategies was evaluated. The results revealed that ‘analysing the life experiences shared by kidney transplant patients’ received the highest score (M ± SD = 4.26 ± .76), ‘practising ethical decision making’ ranked second (M ± SD = 3.84 ± .68) and ‘reading Nightingale’s Diary’ received the lowest score. The SNs appreciated the strategy analysing the life experiences shared by kidney transplant patient.
Various teaching strategies resulted in different degrees of learning effectiveness. Learning ethical decision making improved the SNs’ moral awareness and reduced their SNE. By contrast, the teaching strategy under which sharing a patient’s personal experiences of kidney transplant could only foster the SNs’ moral awareness, whereas the strategy under which the SNs read Nightingale’s Diary neither improved their moral awareness nor alleviated their SNE. However, a positive and significant correlation was observed among the three teaching strategies (Table 3).
Relationships among the MMSQ-SN, SNE and SMTS
The results of exploring the relationships among the MMSQ-SN, SNE and SMTS demonstrated that the pre-test MMSQ-SN scores significantly correlated with the post-test MMSQ-SN scores (r = .434, p < .01) as well as significantly and positively correlated with the post-test SMTS scores (r = .146, p < .05). SNs with higher MMSQ-SN scores in week 1 tended to have higher post-test MMSQ-SN and SNE scores. In addition, the MMSQ-SN post-test scores correlated with the SNE post-test scores (r = .262, p < .01). In week 17, those with higher SNE scores tended to have higher MMSQ-SN scores, and those with a higher level of agreement with the SMTS also had higher MMSQ-SN scores, but those with higher SNE scores tended to have a lower level of agreement with the SMTS (Table 3).
Discussion
According to the research findings, the strategy involving reading Nightingale’s Diary and that entailing SN analysis of the life experiences shared by kidney transplant patients had lecture times of 30 min and 2 h, respectively. SNs exhibited increased interaction with the case subjects during the intervention, and they raised more questions and received more opportunities to role-play. Thus, the SNs employing this teaching strategy engaged in VAK learning, and using this strategy improved SN moral awareness. The results further show that, for nursing ethics education, two to three case subjects can be invited to share their experiences and converse with the SNs in the future. The reading strategy required the SNs to learn independently. However, whether the SNs could have been self-demanding or required supervision is questionable. The SNs practised decision making for 8 weeks between weeks 11 and 18. The SNs employed their after-school time to research relevant literature, engage in group discussions or discussions with the teacher and complete their final report using the Four-Topic Approach. Therefore, the SNs engaged in VAK learning. This strategy encompassed three learning styles, facilitating SNs in learning nursing ethics. The SNs could foster their moral awareness and alleviate the SNE. Therefore, the feasibility of continuing to apply the practicing ethical decision making teaching strategy was confirmed.
A period during which the SNs attended only three ethics education courses (10 h) out of 14 courses (612 h; 1.6%) was selected as the intervention period in order to avoid potential interference factors. However, such factors could not be completely avoided, constituting a limitation of this study. Future researchers can endeavour to elucidate whether enrolment in other ethics education courses interferes with SNs’ moral awareness. Nursing ethics was taught for two periods per week, with additional time provided for out-of-class reading, assignments and group discussions. Because of the teaching intervention, the SNs were required to study nursing ethics for an additional 50–60 min/week. During the intervention period, the SNs did not attend a clinical practicum. Future researchers can attempt to determine whether differences exist between the moral awareness of interning SNs and in-school SNs. Moreover, evaluating the learning patterns of SNs can enhance the development of teaching strategies. In this study, the teaching strategies were designed on the basis of learning objectives. Future researchers can endeavour to integrate learning styles and objectives to develop teaching strategies.
The total moral sensitivity scores of the SNs were improved through the use of multiple teaching strategies in ethics education. The results of analysing the MMSQ-SN categories demonstrate that the SN scores in the EB and MM categories were significantly higher than those of the other categories. However, the SN scores in the IO, EC and PKN categories did not differ significantly. After the intervention, which involved multiple teaching strategies, the SNs displayed significant improvement in the following moral sensitivity categories: EB, MM and MA. These categories include content that approximates the perspectives of Kantian deontology: (1) being universalisable, (2) autonomy and (3) the principle of ends. 21 Regarding the IO category, improving the nurse–patient relationships in a short period for SNs aged 18–19 years with 3 weeks of internship experience is not easy. The results of this study are consistent with those of Comrie’s study, 22 which revealed that experienced SNs believe that establishing nurse–patient relationships is not easy. 19 These relationships may be affected by other factors, such as a patient’s medical condition, personality and SN initiative. This corresponds with Gastmans’ findings that nurse–patient relationships result from their interpersonal networks, and the quality of interpersonal relationships is usually not determined by individuals. 23 In this study, PKN was the only category in which the SNs received lower post-test than pre-test scores. PKN does not refer to ethical knowledge here. Therefore, people with PKN are not necessarily morally superior to those who lack PKN. This is illustrated by the fact that intelligent people commit crime; they use knowledge as a criminal tool. As Gastmans stated, competent patient care comprises not only general PKN but also insight into what constitutes effective nursing. 17 The PKN category is an area of moral sensitivity that requires reconsideration. In this study, the SNs strongly disagreed with Item 29: ‘I am occasionally motivated to threaten the patient with an injection by force if he or she does not voluntarily agree to use the medicine that is prescribed’. This result concurs with Comrie’s findings. 21 Whether reverse scoring should be applied to this item or the result of this item should be deleted, as it was in Comrie’s study, has yet to be determined. Although this item was included in the survey, its score can be removed when the MMSQ-SN total score is computed.
After multiple teaching strategies were used to instruct the SNs in nursing ethics, the SNs’ SNE scores significantly decreased. The top five stressors from weeks 1 to 17 were as follows: (1) assessment anxiety, (2) tight assignment deadlines, (3) anxiety regarding performance and not fulfilling the course objectives, (4) excessive workload during year 3 and (5) lack of time-management knowledge. This reveals that the SNs were required to increase their knowledge of time management and that the assignment workload exceeded their capacity. Consequently, their academic performance may have been influenced if the quality of their assignments was adversely affected because of their inability to manage the workload. The SNs’ SNE scores were positively related to moral sensitivity but negatively related to their agreement with the multiple teaching strategies. This shows that SN had more stress to promote the development of SN moral sensitivity, but results in a lower level of agreement with the multiple teaching strategies. Future studies may aim to develop appropriate stress-relief practices for SNs experiencing the SNE, and the various moral sensitivity categories may be developed using different teaching strategies.
Conclusion
The results of this study revealed that the intervention of multiple teaching strategies in nursing ethics education enhanced SN moral sensitivity. These results can be applied to the training of clinical nursing interns and nursing professionals in the future. In this study, the SNs’ favourite teaching strategy was the patient’s sharing of organ transplant experiences with them because the SNs could raise questions and discuss with the patient during class. This strategy was consistent with the SNs’ preferred learning style and was used to correct their erroneous ethical conceptions, assisting in developing their ethical knowledge. Moreover, the teaching strategy under which the SNs practised clinical ethical decision making assisted them in considering the problems of patients in clinical situations and enabled them to practise resolving moral dilemmas. By employing the Four-Topic Approach, SNs can develop a broader perspective. Both analysing the life experiences shared by kidney transplant patients and entailing the practise of clinical ethical decision making require SNs to engage in VAK learning, thus improving learning effectiveness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.