
Abstract
Background:
An ongoing challenge for clinical ethics consultation is learning how colleagues in other healthcare professions understand, make use of, and evaluate clinical ethics consultation services.
Aim:
In pursuing such knowledge as part of clinical ethics consultation service quality assessment, clinical ethics consultation services can learn important information about the issues and concerns that prompt colleagues to request ethics consultation. Such knowledge allows for greater outreach, education, and responsiveness by clinical ethics consultation services to the concerns of clinician colleagues.
Design:
This quality assessment project explores consultation requests and follow-up questionnaire responses voluntarily submitted from nurses who requested clinical ethics consultation. We present qualitative data analyzed using content analysis and constant comparison methods to identify key concerns that prompted requests as well as common themes among nurse requestors’ evaluations of what was most important in clinical ethics consultations.
Participants and context:
A total of 41 nurses requesting clinical ethics consultation and 15 who returned the follow-up questionnaire.
Ethical considerations:
Our Office of Research Compliance and Quality Improvement determined that our project was not considered human subjects research and so did not require institutional review board approval or exemption. However, efforts were made to avoid any sense of coercion and all data were de-identified prior to analysis.
Findings:
Our analysis revealed six main categories of issues that prompted nurses’ requests for ethics consultation, as well as unifying themes around nurses’ experiences, advocacy, and family support while caring for patients in the intersections of patients, families, and physicians.
Discussion:
The insights gained from analyzing nurses’ requests for and responses to clinical ethics consultation may serve as a resource for clinical ethics consultation services seeking to identify, respond to, and educate regarding issues of importance to nurse colleagues and may be a resource for nursing administrators and leadership seeking to identify and address common ethical issues nurses face.
Conclusion:
Ongoing work on clinical ethics consultation service quality improvement and engagement with our nursing colleagues about their concerns prompting—and their evaluations of—clinical ethics consultation are necessary.
Keywords
Introduction
Clinical ethics consultation is a relatively new phenomenon—the first formal mention of it occurred in the legal context of the Quinlan case in 1976 1 —and so it should not be surprising that there continue to be many different kinds of debates swirling around it; dominant among these are issues addressing the training and qualifications of those who perform ethics consultation, 2 –4 different methods and practices for performing ethics consultation, 5 –7 and appropriate means for evaluating ethics consultation. 8 –10 All are crucial issues and worthy of attention. But these are not the only crucial issues to which those who provide clinical ethics consultation services (CECSs) need pay attention. Indeed, however, these may be ultimately settled; there are also a host of more local considerations that also demand attention. Examples include how do the nurses, physicians, social workers, and so on with whom the ethics service will interact actually themselves interrelate in the institution, that is, what are the formal and informal power gradients both on the immediate clinical level and administratively; under whose aegis does the CECS fall—and how is that institutional entity’s authority, accountability, financial constraints, and so forth institutionally understood; what kind of clinical access and latitude do those who perform ethics consultation have, for example, can they freely access and leave notes in patients’ medical records; to whom is the ethics service held accountable—and in what manner of accountability (e.g. monthly or annual formal reports, retrospective mortality and morbidity-like clinical presentations)? Each institution, in other words, presents its unique context in light of which the ethics consultation service is provided and hence must be responsive.
Bridging these two different levels of issues is yet a third category of considerations pertinent to clinical ethics practitioners; this is most prominently seen in concerns associated with evaluating clinical ethics consultation in which not only might there be general professional criteria utilized (such general criteria are some of the concerns being addressed, for instance, by the American Society of Bioethics and Humanities (ASBH) Quality Attestation effort 11 ) but also institutional-specific criteria. Per the latter kind, these may be established external to the ethics consultation service, for example, by hospital administration, or they may arise from within the ethics service itself, for example, as part of an effort to provide accountability to various stakeholders within the institution. We are particularly interested in the latter. To be accountable in this manner includes having accounts from those others with whom ethics consultants interact. What we present here is, therefore, part of an internally generated, accountability-oriented effort associated with our interest in learning from the healthcare professionals with whom we regularly interact as part of our CECS. In particular, we are exploring what one group of stakeholders—our colleagues in nursing—shared with us about their reasons for requesting ethics consultation, and what they found most important in engaging with the CECS. We present the following as both as an example and as an encouragement that more efforts to learn from nurses, in their own voices, how they understand the activities of their clinical colleagues engaged in clinical ethics consultation.
The CECS at Cedars-Sinai Medical Center
Cedars-Sinai Medical Center (CSMC) is a 900-plus bed tertiary care facility that is both a community hospital and a major academic medical center which employs over 400 resident and fellow physicians and has a stand-alone PhD and MS programs in translational biomedical sciences. The medical staff comprise roughly 1800 community and 400 faculty physicians while the nursing staff is also over 2000; the total employed staff of CSMC is nearly 14,000. For over a decade, CSMC has had a robust MD–RN collaborative network for every patient care unit in addition to an extensive nursing unit practice counsel structure, and since 2007, a formal Unit Ethics Champion structure of nurse volunteers interested in helping raise awareness of ethics-related issues associated with the day-to-day bedside nursing. i
It is within this context, and with strong institutional backing and support from the Medical Center’s Administration and Board of Directors, that the CSMC CECS is fully staffed and run by the faculty of Cedars-Sinai’s Center for Healthcare Ethics (CHE). Due to this arrangement, and given that the CECS is organized around a guiding recognition that moral experiences are always rooted in contexts of interpersonal interactions, the CHE faculty, whose time and effort is 100% dedicated to CHE activities, provide ethics consultation in an “individual but tethered” style whereby CHE faculty individually engage with the key participants associated with a given ethics consultation, but that individual remains in communication and consultation with the other CHE faculty members throughout the process. As for the core objectives of the CECS, these are explicitly articulated in the formal institutional policy governing the CECS: to discuss relevant facets of a situation with the involved participants so as to promote good communication and understanding; to assist participants in identifying ethical values and goals at stake in decisions, situations, and/or disagreements; to enable clear understanding among those involved participants of each person’s basic moral framework; and to help resolve problems, conflicts, or dilemmas. Moreover, anyone directly involved in the care of a patient—including the patient, the patient’s family, nurses, physicians, social workers, chaplains, and others—may request ethics consultation without requiring permission from anyone; the warrant for requesting involvement of the CECS is, simply stated, because one has an ethics question, concern, issue, and so forth. Over the past 5 years, the CECS has received an average of 220 requests for ethics consultation per year, with about 45% coming from physicians, 25% from social workers, 20% from nurses, 5% from other staff, and about 5% from patients and families.
Design and methods
The CECS quality assessment effort process overview
Within this context, between 1 July and 31 December in both 2011 and 2013, the CECS engaged in a quality assessment (QA) effort examining the activities of the CECS in which the primary aim was to learn how other clinicians make use of, describe, and evaluate the Service.
ii
During the first study period (2011), we had a total of 106 consecutive consultations requested, and during the second study period (2013), the total was 115 consecutive consultations requested. The primary data for use in this QA effort were drawn from a variety of sources including two data gathering documents: Case opening form: This form, which serves as the core permanent internal documentation for every ethics consultation performed at CSMC, contains a variety of data, including data collected at the time a request for clinical ethics consultation is received, for example, the name, role, and contact information for the requestor, the verbatim reason for the request, basic patient demographic and location information, and the names, roles, and contact information for key participants in the patient’s care. CECS Questionnaire: This form, which was designed specifically for our quality review effort and developed in light of published surveys from others who were similarly interested in understanding nurses’ and physicians’ perspectives regarding the ethical issues they encountered in their clinical context,
12
–15
was sent at the conclusion of each consultation to staff identified as “key participants” by the ethics consultant. The Questionnaire includes quantitative questions (e.g. check boxes for identifying helpful activities in which the CECS might have engaged a Likert scale for rating overall effectiveness) as well as open-ended questions asking respondents to describe why the CECS was involved and what they thought was the most important aspect of CECS involvement ( Figure 1).
CECS Questionnaire.
During the months in which we asked our colleagues to help us with our review, each consultation was assigned a review number (distinct from the case log number used in our regular documentation) when a request for consultation was received, and this review number marked all documentation associated with that consultation. While the CECS Case Opening forms were completed by CECS faculty or the Center’s office staff in real time during the course of providing ethics consultation, the one-page Questionnaires were sent to up to six “key participants” involved in the consultation only after the patient around whom ethics consultation revolved was discharged or died. In an accompanying cover letter that outlined the CECS QA aim, that completion of the Questionnaire was voluntary, and that we would review responses as de-identified data, these “key participants” were asked to complete and return the Questionnaire within 1 week (return envelopes were provided). If no reply was received within 10 days, a second letter and Questionnaire were sent. Our Center’s management assistant had complete responsibility for this entire phase of our QA effort, that is, she assigned the review numbers, sent out Questionnaires and cover letters, kept track of returns, sent out reminders, and then entered all information for each consultation (from the Case Opening and Questionnaires) into an Excel database, organized by review number. We had no role in any of this effort and had no access to returned Questionnaires or data until after the close of each study period, that is, January 2012 and January 2014, respectively. In this way, we created a clear separation between our clinical work with our colleagues and the QA effort, not to create any form of pressure for completing Questionnaire or answering in certain ways.
For our first round of analysis, we looked at the reasons our colleagues initially requested ethics consultation (Reasons) and then for those requestors who returned our CECS Questionnaire, the comparison between their Reasons for request (RFRs) and their retrospective responses to the questions of why clinical ethics consultation had been requested (Why) and what they believed to be the most important aspect of the CECS involvement (MIA).
Some verbatims include more, some less, detail. Accordingly, as an initial step of determining what we might learn, we, along with a staff assistant hired solely for the effort of analyzing the data on the Case Opening sheets and Questionnaires, reviewed each of the three sets of verbatims (Reasons, Why, and MIA), beginning with the Reasons. The process of review entailed several steps using content analysis and constant comparison methods to ensure reliability. 16 –20
Specifically, first, working independently, each reviewer read each Reasons verbatim and then wrote a summary in order to identify what, specifically, served as the core content for each. We then collectively compared our summaries for agreement, and then independently coded the summaries and, again, compared for inter-reader reliability. At this point, we began looking for themes and patterns emergent from the language used in the original verbatims. We again compared for inter-reader reliability and then independently re-coded with an eye for broader, general categories among the identified themes, and then once again compared for reliability. The process was then repeated for the other two sets of verbatims.
Finally, we independently compared the broad, general categories for the three verbatims for each ethics consultation and rated them as the Same, Similar, Diverging, or Different. We then again compared for reliability, after which our staff assistant reviewed these ratings and identified wherever there was discrepancy—for instance, if we rated one pairing of categories one way but differently for a different pairing. We then collectively discussed the several identified discrepancies, re-reviewing the general themes and summaries associated with the relevant verbatims and then re-rated to ensure consistency across all ratings. In this way, we were able to compare the frequencies of when Reasons versus Why, Why versus MIA, and MIA versus Reasons were the same, similar, diverging, or different in content.
What we are reporting here is based on those data coming from our colleagues in nursing.
QA participants
Nursing requests: how many call, who calls, and from which units?
As mentioned above, our nursing colleagues have accounted for roughly 20% of the requests for ethics consultation at our institution over the past 5 years, and this pattern held true for both 6-month periods during which we asked for feedback from our colleagues: 21 of the 106 requests during the 2011 period (19.8%) and 21 of the 115 requests during the 2013 period (18.3%) came from nurses (Figure 2). Nurses who requested ethics consultation were working in a variety of nursing roles: as bedside nurses, charge nurses, nurse case managers, nurse practitioners, and in other nursing roles (Figure 3). In addition, these nurses were located in a variety of clinical locations: in 2011, 55% of the requests came from nurses working in an intensive care unit (ICU), 40% come from nurses working in a non-ICU in-patient unit, and 5% from the outpatient setting. This distribution is similar to the overall distribution for all requests for ethics consultation by all requestors over the past 10 years. That being said, during the 2013 period, 67% of nursing requests came from an ICU as compared to 54% for requests by all requestors during all of 2013.
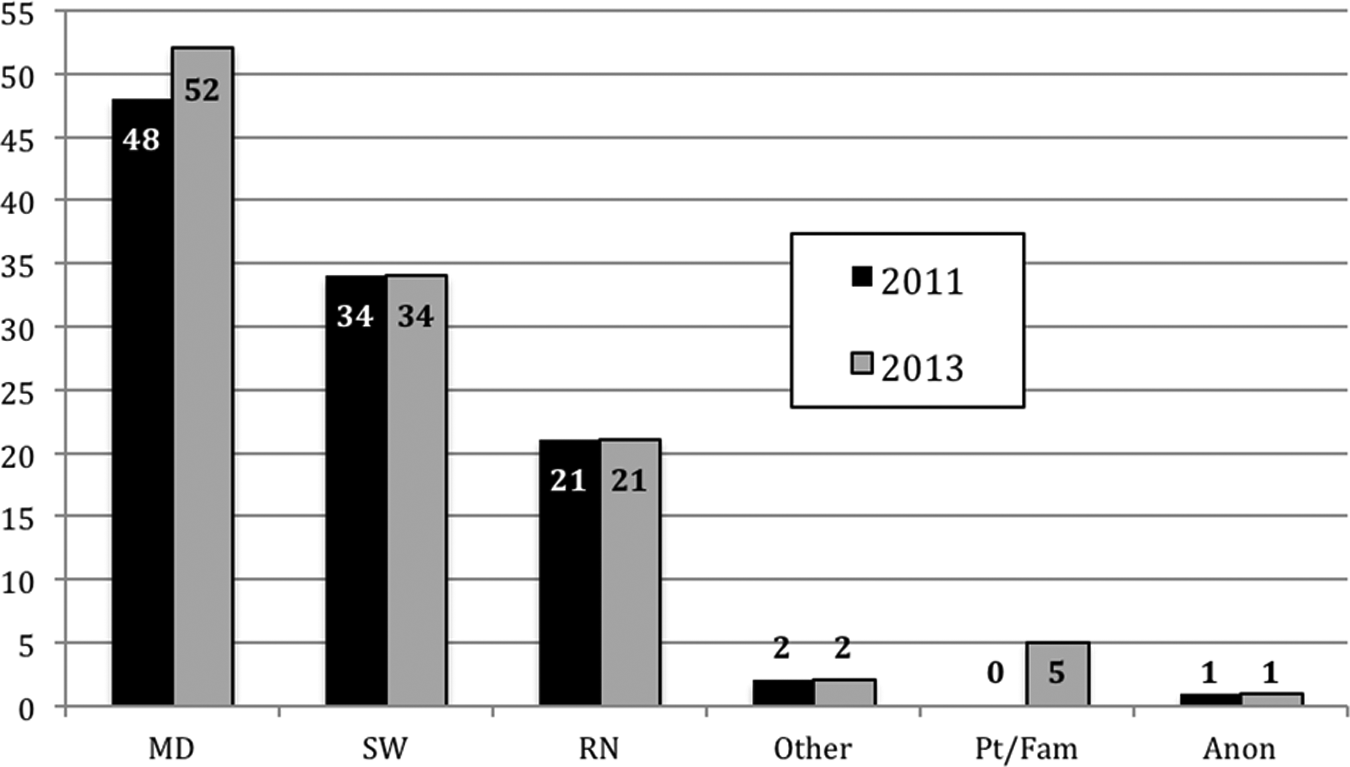
All requestors of ethics consultation during 2011 and 2013 study periods.
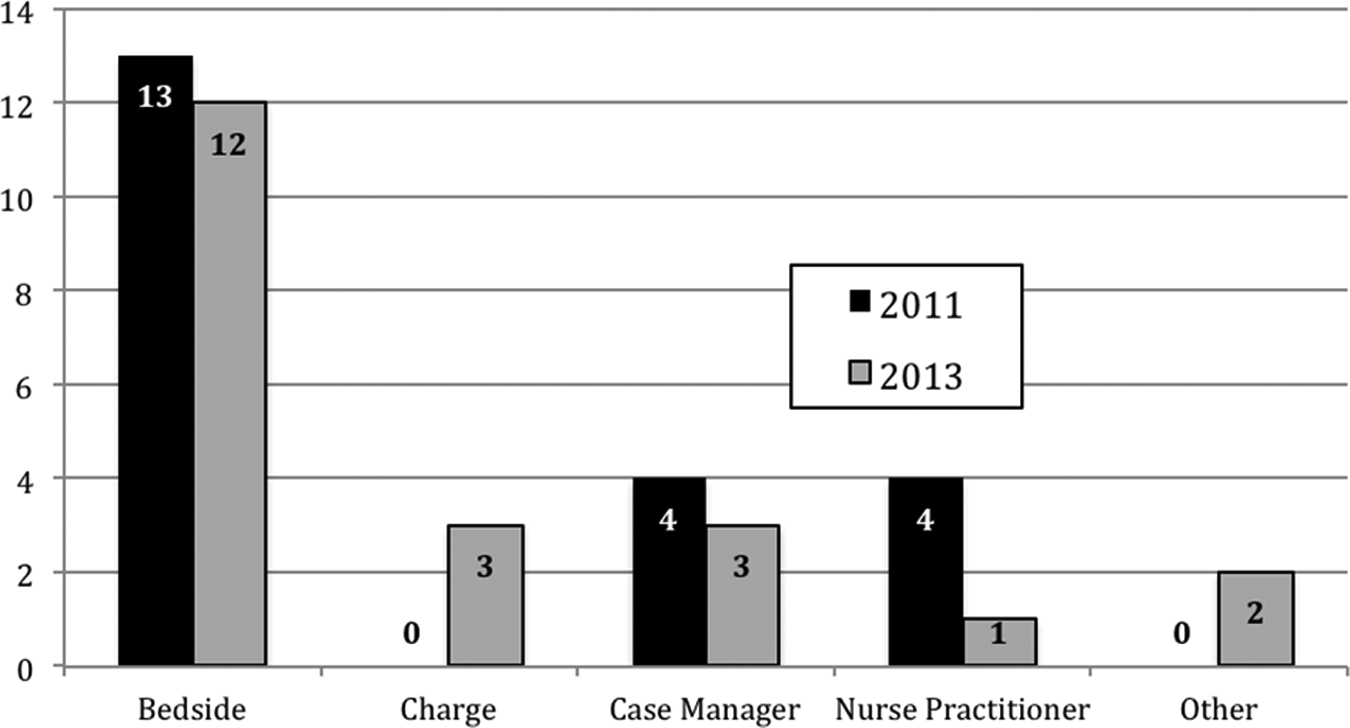
Nursing roles of nurse requestors.
Findings
Nursing requests: the RFRs
As also previously mentioned, at the time of request for ethics consultation, the reason for the request is documented verbatim on a unique Case Opening form completed for each clinical ethics consultation.
Initial review revealed that requests fell into several broad topic-oriented categories: Plan of Care, End of Life, Goals–Values–Preferences Questions, Nurse–Physician Issues, Honoring Patient Preferences, Futility, and several that were unique and hence categorized as “Other” ( Figure 4). The following sections briefly describe each category and give examples, iii in light of which we then explore the observations and questions that emerge from nurses’ requests for clinical ethics consultation.
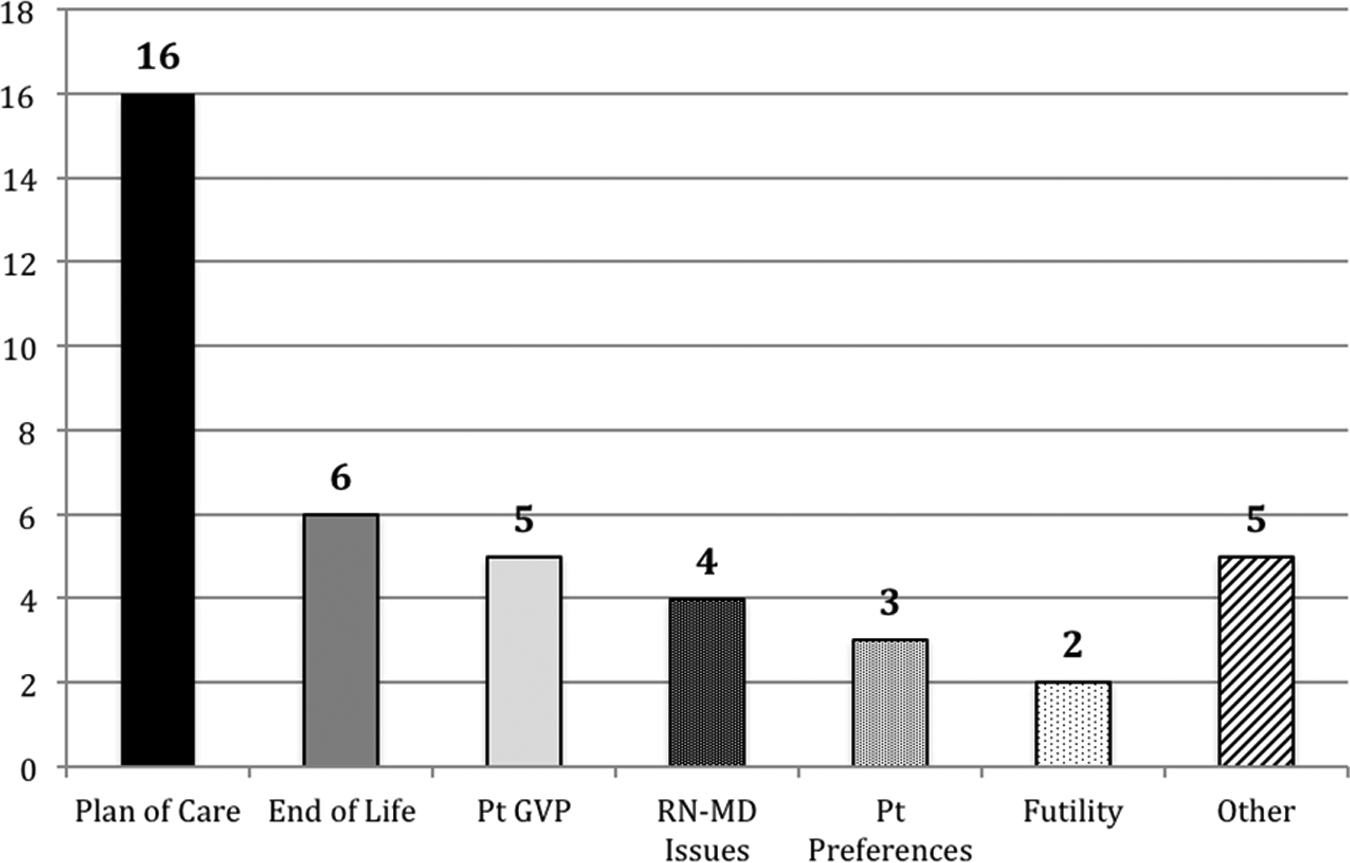
Topic-oriented categories of nurses’ reasons for requesting ethics consultation.
Nursing requests regarding plan of care
Requests regarding plan of care most often focused on either clarifying the plan of care or helping establish an appropriate plan of care (10 of 16 requests). The requests regarding clarification arose in situations where there was reference to a plan of care or some kind of understanding that a plan of care had been established, but that plan had perhaps not been clearly communicated or was possibly inconsistent or difficult to follow. Examples of such verbatims include Nurses have questions regarding patient’s plan of care (2013-66) and Nurses confused about plans/goals given patient on Dying Patient Protocol iv yet receiving blood and antibiotics. Requesting help with communication (2011-42).
Requests regarding help in establishing an appropriate plan of care, however, often emerged because there was no evidence of a plan or there were practical concerns about establishing a plan: Patient in active rejection after kidney transplant (purchased kidney overseas). Bi-polar, lacks decision-making capacity, refusing meds/tx and very agitated (violent?). Wants to leave AMA. Wife/DPOA told RN she fears going home with patient (2011-26) or RN Case Manager requesting Ethics consultant participate in family meeting scheduled for noon on MM/DD/YY—meeting is to discuss POC—including proposed amputation of pt’s leg—w/pt’s spouse (2013-8). Furthermore, most of the requests about clarifying or establishing plan of care were centered around family issues (6 of 10), such as the two preceding examples as well as this one: RN Case Manager asked for Ethics Consultation because “This is an ethics issue. We need to have a meeting regarding the patient’s refusal to go to SNF [skilled nursing facility] and his family’s refusal to care for him after discharge.” (2011-51)
The remainder of the requests regarding plan of care (6 of 16) stemmed from nurses’ disagreement with, and even distress regarding, physicians’ plans of care. For example, as one Case Opening form verbatim reads: Team wants to start 1st time dialysis on 96 yr old patient with metastatic concern—wife wants “everything done.” Nurse Case Manger feels this plan of care is inappropriate (2011-93). Or another stated the following: Pt voiced to her MD that she wanted “Physician assisted suicide.” Palliative care was ordered. Pt’s oncologist upon discovering P.C. was ordered, cancelled the order stating it was inappropriate. RNs are distressed by this action (2013-12). Half of the nursing concerns regarding physician plan of care were specifically couched in terms of distress, a significant issue well documented in the nursing literature for several decades.
Nursing requests regarding end of life
In our review periods, nursing requests included a second category—end-of-life concerns—that, in each case, centered around family. While one request was specifically about family disagreement with the patient’s end-of-life care, five of the six requests were about family not accepting a patient’s end of life. For example, Patient’s family refusing Palliative Care and not wanting patient to know about her prognosis. RN is distressed due to patient being in pain, not being placed on comfort care (as recommended) and not being allowed information about her condition (2013-23) or Patient declared brain dead—husband is insisting to transfer patient to Other Hospital (he was given false hope last night by a friend that told him Other Hospital can “Save her with a miracle”) (2013-56). While family concerns emerged in other categories as well, we found it striking that all the requests regarding end-of-life care were about family issues and, more specifically, about family difficulties accepting a patient’s potential, approaching, or medically established death.
Nursing requests regarding need for discussion of patient goals, values, and preferences
A third group of requests for clinical ethics consultation came from nurses concerned about patients’ goals, values and preferences, or what we call “GVP” in our institution, and thus the desire for explicit GVP discussions. During the 2011 and 2013 review periods, we received five requests to facilitate GVP discussions or to help clarify the patient’s GVP, although there were different flavors within the broad category. For example, the reason one nurse requested ethics consultation was because Patient is failing to thrive, has stated “he wants things turned off, except for the biventricular assist device.” RN would like ethics assistance in facilitating communication with patient, his family and care team regarding his goals and plan of care. (2011-12)
Nursing requests regarding nurse–physician issues
Another area of specific concerns from nursing requests centered on nurse–physician relationships, particularly physicians not communicating with family (4 of 41 requests). Although most nurse requests were specific to issues regarding physicians’ communication—for example, Concerns than primary MD is not appropriately communicating with the patient regarding goals of care. Code status needs to be addressed (2013-70)—other requests incorporated both communication and behavioral concerns: Dying patient—patient’s family (including DPOA
v
) requested that the patient be on Palliative Care—attending does not want this and convinced the family to put patient on Dying Patient Protocol. At 8am today, the family told the attending they do indeed want Palliative Care—but attending has not taken action and is not responding to the care team’s requests regarding this. RN stated that the attending is behaving “very inappropriately—rude with the family and making them feel stupid.” (2011-37)
Nursing requests regarding honoring patient preferences
As another example of nurses’ concerns at the intersection of patient, family, and physician, several requests during the course of our assessment asked for help because the nurse felt that either a patient’s family or patient’s physician was disregarding the patient’s preferences. For example, one bedside nurse requested ethics consultation because the Patient has stated to medical team that she does not want to continue treatments and would like comfort care. Patient’s son is fighting this and is pressuring for code status to be changed to full and is demanding aggressive treatment. (2013-48)
Nursing requests regarding futility
The smallest number of requests we received from nurses for our CECS were those addressing the issue of futility, a fact which in and of itself is striking given the common popular perception that this is a topic of great clinical concern and the prompt for much ethics consultation. Although we have noted, above, many requests regarding end-of-life care or nursing disagreements with the plan of care, none of these explicitly used the language of “futility.” That being said, we did have two requests that, while also not using the term “futile,” did seem more specific to an intervention or plan of care being seen as “futile” (which we define operationally as being ineffective in reaching an intended goal or outcome): Patient’s family wants PEG placement for this patient that is failing (2011-30), and Patient believed to be at EOL from grave cardio/respiratory pathology. Brother requesting continued support til estranged 19 y.o. daughter who lives back east can be notified and visit (2013-15). Neither request mentioned conflict, but instead each described a troubling circumstance where the plan or intervention did not seem to make sense, and hence was seen as futile.
Nursing requests regarding “Other”
The final group of requests is a group of “misfits”—five consultation requests that did not quite fit into any one of the other categories. Some seemed to be questions about institutional practice or policies; for example, one nurse expressed concern for a potentially unrepresented patient—Pt reportedly has no family to consent for PEG (2011-50)—whereas a nurse practitioner seemed to be seeking institutional support on behalf of the team—MDs have raised possibility of extremely high risk (and reportedly never been done before) procedure for very frail elderly patient and before proceeding want input from Ethics (meet with patient and family) re: is it appropriate (2011-100). Other concerns centered around surrogate concerns or particular aspects of patient care, for example, Patient’s MD son (not on our staff) interfering with nurses caring for his father yesterday, before being transferred from floor to ICU (2013-55). Each was distinct or unusual enough, however, to where it did not quite fit in the broader categories previously outlined.
Although working with small numbers of requests from nurses (20 in 2011, 21 in 2013), the distribution of general categories—and the themes that emerged across categories—provides interesting points for reflection about the kinds of concerns nurses see as warranting a request for clinical ethics consultation, which sets the stage for exploring what nurses found to be most important about the CECS.
Nurses’ experiences, advocacy, and family support
Looking at the data from one direction, we discovered some striking commonalities running throughout the different categories of RFRs. All the nurses requesting clinical ethics consultation were seeking help, in some form or another, for responding to some concern as described in the general categories above. But there is also the commonalities found when these categories are connected. Specifically, we suggest there are three main categories of connection. One major commonality is that requests appear to emerge from nurses’ experiences of being care providers. Another is that requests emerge from what could be described as nurses’ role as patient advocates. And finally, a smaller grouping of requests emerge from nurses’ efforts to support patients’ families (Figure 5).
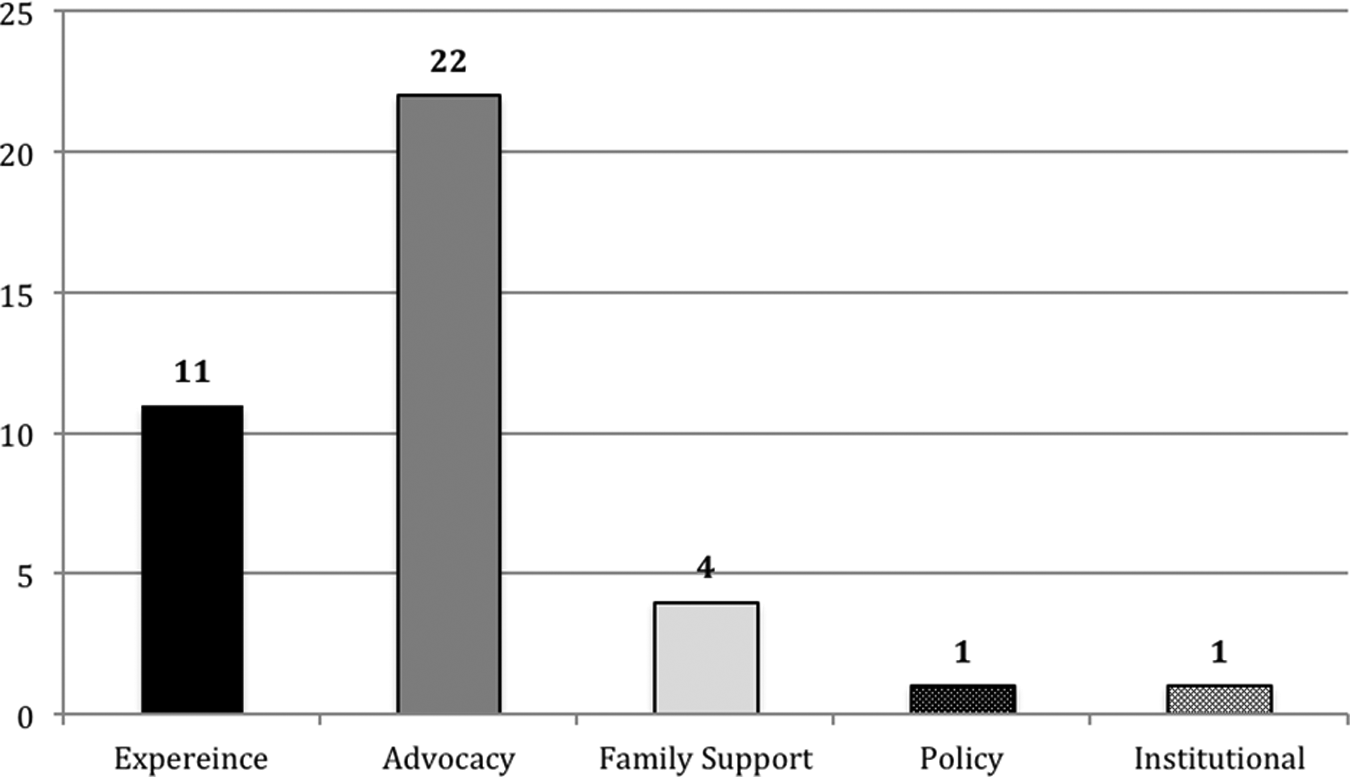
Common themes in nurses’ reasons for requesting ethics consultation.
The requests regarding nurses’ experiences often arose in morally challenging experiences or experiences of distress, with 11 of the 41 requests (a full 25% of the requests from nursing) emerging from concerns around challenging family dynamics, difficulty clarifying or establishing plan of care, and distress over nurse–physician interactions. The recognition of, voicing of, and even explicit use of the terminology of “nurses’ distress” or “moral distress”—and the fact that such experiences make up 25% of nurses’ requests for clinical ethics consultation—are not surprising, especially, as mentioned, given the rich literature on these topics over the past 30 years.
Nor is it surprising that even more nurses’ requests for ethics consultation emerged from another prominent theme in the literature: nurses’ role and responsibilities as patient advocate. Of the 41 requests from nurses we received during the two review periods, 22 were rooted in nurses’ advocacy for patients. This theme or trend is visible in the requests categorized as concerns about futility, clarifying patient goals–values–preferences, code status, family interfering with care, establishing or clarifying the plan of care, and even explicit disagreement with plan of care. Across these different types of requests, the underlying, or overarching, theme was that nurses’ requests demonstrated their having deep concern for the kind of care their patients were receiving, or, more simply, what was good for their patients.
The final cross-category theme was one of requesting ethics consultation in an effort to provide family support; this constituted 10% of all requests from nurses. Although such requests may have been rooted in a subtle recognition that supporting a patient’s family is part of supporting and advocating for a patient, they emerged and were explicitly voiced as family focused, in distinction from nurses’ concerns and advocacy for their patients. The requests regarding support for patients’ families differ from the other two themes of patient advocacy and nursing support, but all three seem rooted, at the very least, in the intimate interactions that make up the daily work of nurses—whether as bedside nurse, charge nurse, nurse case manager, or nurse practitioner.
Stuck in the middle with you
A second set of themes we noticed cutting through and across the general categories of RFRs is the relationships underlying the nurses’ requests for ethics consultation, namely, their interactions with patients’ families and with patients’ physicians. Of the 41 requests for ethics consultation, 16 requests or 40% included concerns about family issues. Looking more closely at this grouping, the six requests regarding end-of-life concerns grew from worries about family not accepting that the patient was at the end of his or her life—EOL concerns, care providers seeking an advocate for pt that is failing to thrive. Pt’s son will not accept that his mother is dying and has become disruptive in the MICU (2011-7)—or the presence of patient and family disagreement about end of life care—Case Manager has concerns that the family is insisting on care the patient wouldn’t want—“they took off Dying Patient Protocol!, that family needs a talking to about goals and big picture” (2013 -1).
Also within the concerns about family issues, another six requests focused on plan of care, including clarifying plan of care, facilitating family understanding of plan of care—Nursing concerned that patient’s nephew does not understand POC
vi
(2013-54)—and helping to establish an appropriate plan of care secondary to family issues: Nurse Practitioner requested clinical ethics consultation to help clarify patient goals and plan of care, including code status, for this heart failure patient with multiple co-morbidities. A major concern for NP (and possibly other team members) is that the patient’s daughter has not been present and may not be making decisions in her mother’s best interest. Attempting to arrange a family meeting. (2011-83)
The other theme in the pair comes from nursing interactions with physicians—including the interactions explicitly labeled as distressing for nurses. Of the 41 requests for ethics consultation, 12 requests (almost 30%) expressed distress from or dispute with physicians’ plan of care, physician disregarding patient preferences, or concern about physician behavior. Requests about physician orders and communication—RNs are concerned about patient’s comfort—no orders for pain meds and they are having difficulties communicating with MDs. In addition, wife is having difficulties with end of life issues (2013-50)—illustrate that despite much work in recent decades, and even explicit systemic efforts at our institution (e.g. MD–RN Collaborative meetings, Unit Practice Councils), there appears to be a long way to go in terms of nurse–physician interactions.
All told, 70% of the requests from nurses emerged from their focus and responsibilities at the intimate intersection of all those caring for the patient: the patient himself or herself, the patient’s family or other surrogates, and the various physician and physician teams. And as even further corroboration, 9 of the 16 requests about family issues and 9 of the 12 requests about nurse–physician issues (total 44% of all requests) came from the bedside nurses—those whose are positioned squarely in the middle of all those involved in patient care.
Nursing requests: what did they value?
In addition to looking at the reasons nurses requested clinical ethics consultation, we were also interested in learning what nurses valued in the CECS. To do so, we looked at the group of nurses who requested clinical ethics consultation who also completed and returned our QA Questionnaire. Of the 41 nurses who requested ethics consultation, 15 returned the Questionnaire, or 37% of requestors. For this project, we looked specifically at two parts of the questionnaire: the fill-in-the-blank questions of “Why was the CECS involved?” and “What was the most important aspect of the Clinical Ethics Consultation?” (hereafter WHY and MIA, respectively). Of the 15 nurses who returned questionnaires, 14 provided some response for the WHY question. Most (two-thirds of the respondents) recollected their initial RFR fairly accurately—only three gave a different response to WHY than their RFR, and one left the question blank, versus 10 whose WHY matched their RFR. In this group of nurses, we saw more correlation among the WHY versus the RFR than we did looking at the responses of requestors in general.
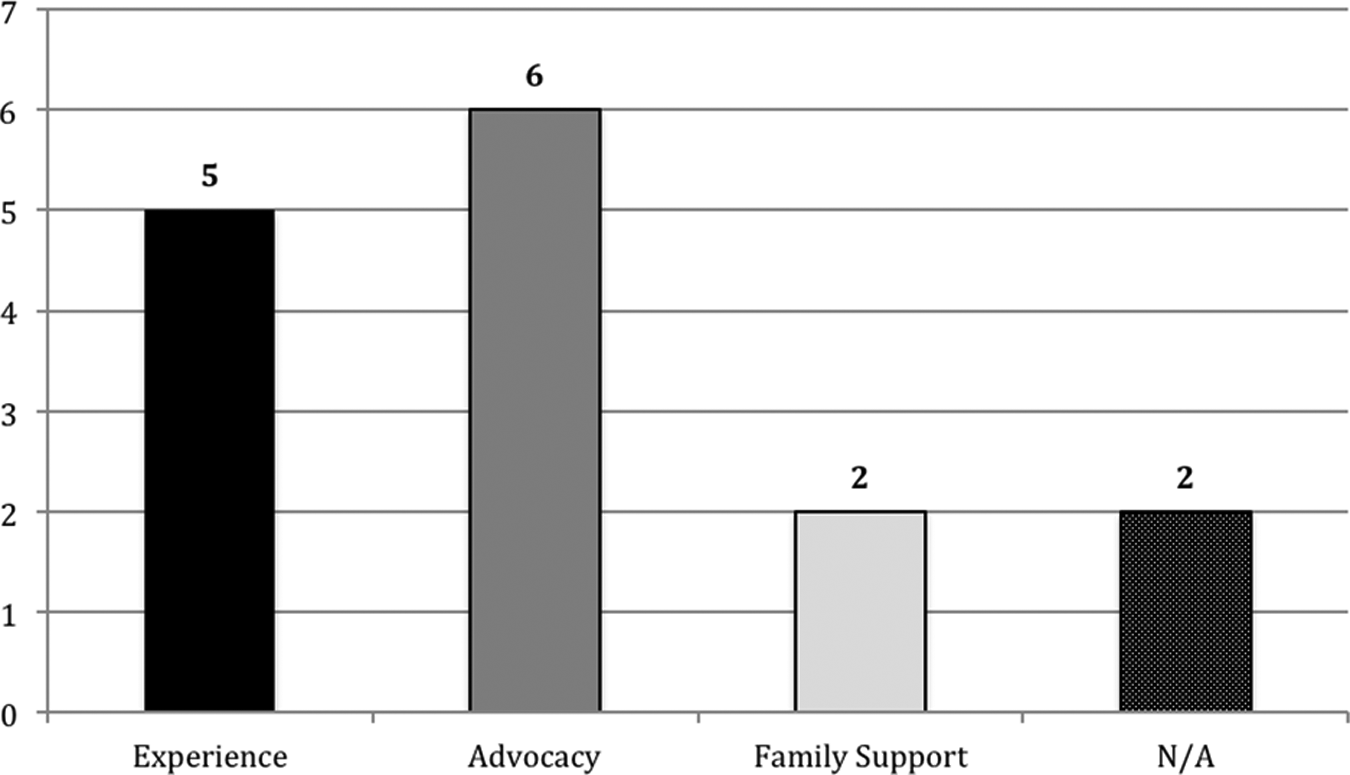
As with the initial RFRs, we noticed broad themes within the responding nurses’ descriptions of MIA of the ethics consultation, although the numbers were more evenly spread. Whereas concerns about experience only made up 25% of the requests from all nurses, 5 of 13 nurse respondents who provided an MIA (38%) focused on support for nurses’ experience (i.e. for support of providers with a very difficult volatile family, 2011-83). Nurses described an MIA with an underlying theme of patient advocacy in 46% of the responses, slightly less than the 54% of advocacy concerns from all nurses requesting clinical ethics consultation. Finally, there was a slightly higher percentage of family support among the nurses who responded and provided an MIA than among overall requests (15.3% vs 10%, respectively), although the numbers for both are small (Figure 6).
Common themes in nurses’ reasons for requesting ethics consultation for nurses who returned a QA Questionnaire.
As to the second group of themes we saw among nurses’ reasons for requesting clinical ethics consultation (the 40% emerging from family issues and 30% from distress with physician plan, communication, or behavior), we saw a similar prevalence among the nurses’ descriptions of the most important aspect of the consultation. Of the 13 who responded, 5 requests mentioned providing support for family issues, 3 mentioned support regarding physician issues or for providers, and 2 mentioned support for both staff and family, showing a total of 77% of nurses who felt that the most important aspect of clinical ethics consultation involved support regarding interpersonal relationships and interactions among patient, family, nurses, and physicians.
Is this really what matters to nurses?
These observations on what nurses who requested ethics consultation and what those who returned the Questionnaire described as the most important aspect of ethics consultation are fascinating, but what was more striking, perhaps, was how closely aligned those initial requests and retrospective evaluations were. We have already noted that the retrospective WHY matched closely to the initial RFR in two-thirds of the consultations we tracked, but we also discovered, and were intrigued by the fact that the 15 nurses who both requested clinical ethics consultation and returned the Questionnaire described the MIA in a way that matched the initial RFR and the WHY for two-thirds of the consultation. For the MIA response, 10 nurses wrote a retrospective description that was equivalent to the RFR, 2 were different, and 3 were left blank: a high correlation, even for the relatively small numbers we have.
Furthermore, looking at the data to see whether the comparisons of RFR, WHY, and MIA were the same across each consultation, we found that 7 of the 15 matched across all three descriptions (RFR vs WHY, WHY vs MIA, and MIA vs RFR), while one was different across all three comparisons. Four had variations where two of the three were the same (e.g. for consultation 2011-51: RFR was “to help establish plan of care 2° to family” issues which is different than the recollected WHY “to make decisions on EOL issues” although the RFR more closely matches the MIA of “facilitate EOL plan of care”), or two of the three that were different. Three consultations could not be compared across all three categories because of one or two blank fields. Again, for the nurses for whom we have both the initial reason for the request and both responses from their retrospective Questionnaire, two-thirds show agreement as to the impetus for clinical ethics consultation and what was seen as valuable in those consultations.
What is perhaps the most striking is the types of situations for which nurses who both made requests and returned their Questionnaire, and how closely their WHY and MIAs matched in those circumstances. Specifically, those who retrospectively recollected that the CECS had been involved for end-of-life concerns, goals–values–preferences issues, and concerns about patient preferences all felt the most important aspect of CECS involvement addressed those concerns (Figure 7). Two respondents felt the most important aspect of CECS involvement met their concerns about plan of care, but two others also felt the most important aspect was establishing or clarifying plan of care even though their reason WHY clinical ethics was involved was different (RN–MD issues or futility, perhaps). The close correlation from nurses’ retrospective responses seems to indicate, at the very least, that a fairly high percentage of those requesting clinical ethics consultation were satisfied with the service provided, and, when understood alongside the similarly close correlations among the initial RFRs, the reason why CECS was involved and the most important aspect of that involvement, it provides a solid internal validation of the results. Charting all three data sets together, the one noticeable change between RFRs and retrospective WHY is where the initial request for assistance with plan of care gets reclassified as either an end-of-life concern or a concern about goals–values–preferences, or may be the blank WHY response (Figure 8). Again, the commonalities are striking, and part of what we find so interesting for our nurses and our CECS.
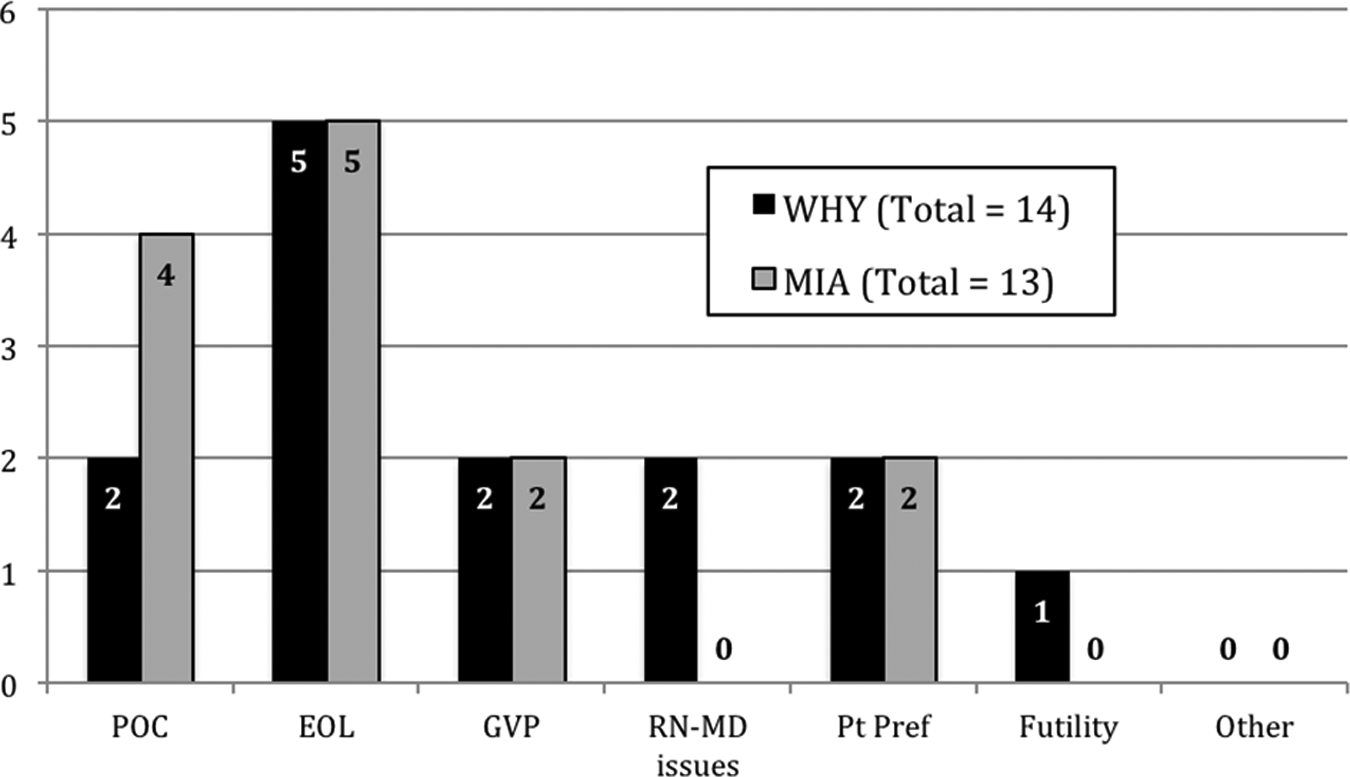
Nurses who returned a QA Questionnaire recollected responses regarding why the CECS was involved versus what they reported as the most important aspect of the clinical ethics consultation.
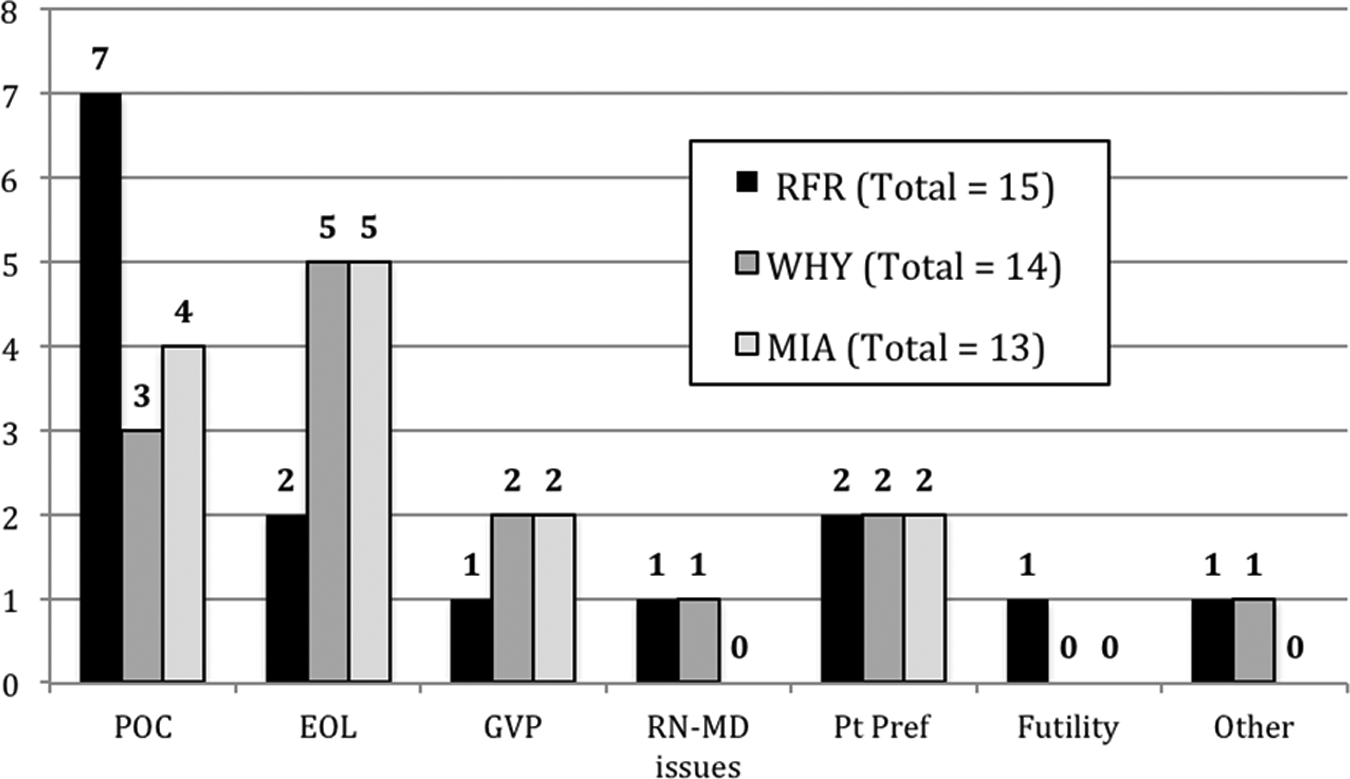
Nurses who returned a QA Questionnaire verbatim reasons for requesting ethics consultation as documented at time of request versus recollected responses regarding why the CECS was involved versus what they reported as the most important aspect of the clinical ethics consultation.
Discussion
Observations and ongoing questions
As might be expected, we discovered that nurses requested clinical ethics consultation for a variety of reasons, from across the institution, and from a variety of nursing roles. What we found most interesting was the high percentage of nursing requests that focused directly on advocacy for their patients and how many of those who returned the Questionnaire indicated that they felt supported in their patient advocacy. As a way of taking the temperature of our institution, it is reassuring to know that the CECS appears to be addressing nurses’ concerns. It is also a reminder to us that ongoing education and outreach to nurses regarding CECS availability and processes can increase awareness and recognition of the support available.
On the other hand, while not an insignificant percentage of nurses requested clinical ethics consultation for concerns about their experiences, fewer nurse respondents indicated feeling supported in their challenging experiences. This raises questions for those of us providing clinical ethics consultation: Are the nurses who request consultation for support with challenging or distressing experiences actually finding those concerns addressed by the CECS? If not, how can we better address such needs and concerns? Or, could it be that the nurses’ concerns are being addressed, but that the experiential components and support provided are more difficult to report on, and hence, the Questionnaire is not an adequate vehicle for respondents? Since any answer to these questions is conjecture at this point, we instead have chosen to focus on the challenge we face in needing to pay more attention to, and more fully embrace and support, the experiential elements of nursing practice. This also emphasizes the need to create and maintain space in which nurses can articulate their challenging experiences—in the moment and after the fact. As such, we see this as a prompt for us to reevaluate our CECS feedback mechanism to allow, support, and encourage nurses’ feedback regarding CECS responses to their challenging moral experiences, so we can learn more about whether we are failing to address them or simply failing to capture how we are addressing them.
Conclusion
As noted at the beginning of this article, the field of clinical ethics is still relatively young, and there are still many outstanding concerns with which the field is grappling, including and especially appropriate means for evaluating clinical ethics consultation. What we have attempted to demonstrate is what can be learned when searching for an account of clinical ethics practice from the perspective of those clinicians with whom ethics consultants work in the midst of performing ethics consultation. Thus, what we have presented above is meant to serve as an example, and hence the beginning (as opposed to the conclusion) of the work at hand. And as such, we hope it is an encouragement of others to similarly turn to their clinical colleagues and see what might be discovered.
To that end, this project, which is also the beginning of our ongoing work with our nursing colleagues, is but the first round of examination of nurses’ requests for, and evaluations of, our CECS. Given the highlights of both the commonalities and the nuanced diversity among the situations and concerns that prompt nurses’ requests, this exploration also serves as a reminder that identifying, reflecting on, and hopefully learning from nurses’ reasons for requesting clinical ethics consultation may also provide new insights into nursing practices—and in so doing, perhaps suggest new avenues or opportunities for ethics education, engagement, and support.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.