
Abstract
Background:
In previous research on ethics case reflection (ECR) sessions about specific cases, healthcare professionals in childhood cancer care were clarifying their perspectives on the ethical issue to resolve their main concern of consolidating care. When perspectives were clarified, consequences in the team included ‘increased understanding’, ‘group strengthening’ and ‘decision grounding’. Additional analysis of the data was needed on conditions that could contribute to the quality of ECR sessions.
Objective:
The aim of this study was to explore conditions for clarifying perspectives during ECR sessions.
Research design:
Data were collected from observations and interviews and the results emerged from an inductive analysis using grounded theory.
Participants and research context:
Six observations during ECR sessions and 10 interviews were performed with healthcare professionals working in childhood cancer care and advanced paediatric homecare.
Ethical considerations:
The study was approved by a regional ethical review board. Participants were informed about their voluntary involvement and that they could withdraw their participation without explaining why.
Findings:
Two categories emerged: organizational enablers and barriers and team-related enablers and barriers. Organizational enablers and barriers included the following sub-categories: the timing of the ECR session, the structure during the ECR session and the climate during the ECR session. Sub-categories to team-related enablers and barriers were identified as space for inter-professional perspectives, varying levels of ethical skills and space for the patient’s and the family’s perspectives.
Discussion:
Space for inter-professional perspectives included the dominance of a particular perspective that can result from hierarchical positions. The medical perspective is relevant for understanding the child’s situation but should not dominate the ethical reflection.
Conclusion:
Conditions for ECR sessions have been explored and the new knowledge can be used when training facilitators as well as for those who organize/implement ECR sessions. Awareness of space for different perspectives, including the possible medical advantage over the nursing perspective, could reduce the somewhat unilateral attention and contribute to an inter-professionally shared reflection.
Keywords
Introduction
Caring for children with cancer is associated with frequent experiences of ethical issues that are often related to goals of care, end-of-life care, decision-making, truth-telling and inter-personal conflicts. 1 –3
In recent research it was found that, as a means of dealing with ethical issues, healthcare professionals who cared for children with cancer expressed a need for inter-professional reflection sessions. 1 To help professionals deal with their ethical issues, various ethics support actions have been developed. 4 One action for ethics support that has recently received considerable attention is moral case deliberation (MCD). 5 –7 In this study, we use the related term, ethics case reflection (ECR) sessions. 8 ECR sessions are meetings where reflection on an ethical issue in a specific case is achieved by ethical argumentation so as to gain quicker access to moral insight. 8,9 Participants in these meetings vary, but can include the inter-professional team. 8 In ECR sessions, healthcare professionals learn to reflect upon their ethical values and arguments in relation to the ethical issue. The ECR sessions are guided by a trained facilitator, who commonly uses a conversation method but does not give advice. 9 Implementing ECR sessions in healthcare teams can provide an opportunity for professionals to share and deal with ethical issues they have experienced.
Previous research has emphasized significant aspects that influence the outcome of ECR sessions. 10 –14 One aspect is the use of conversation methods that can assist ethics reflection during the ECR session. Two examples of frequently used conversation methods are the dilemma method 15 –17 and the Karolinska model. 8 Another aspect of ECR sessions is the facilitator, who enables ethics reflection by guiding the team through reflection and dialogue about the ethical issue and creates a safe atmosphere. 5 Another aspect is the group’s composition, which is important for group interaction. 18 Awareness of the balance between homogeneity and heterogeneity in the group is essential 19 for the interaction and the dialogue. Heterogeneous group composition was experienced as both positive and negative in ECR sessions. The positive experiences included broadening of horizons and the negative were about different levels of involvement and moral competence among participants. 5
However, information on the social patterns during ECR sessions is still lacking. A previous study within childhood cancer care explored ‘what is going on’, that is, the social patterns, during ECR sessions. 20 In that study, healthcare professionals were striving for a common understanding and a shared view of the child’s care. The social pattern of behaviour that emerged was clarifying perspectives, which involved explaining not only participants’ personal views on the ethical issue but also the professional group’s perspective, including the medical and the nursing perspectives. The different viewpoints and arguments with respect to the ethical issue at stake were expressed by various healthcare professionals. When clarifying their perspectives, healthcare professionals used multiple strategies. For example, they mentioned certain values that were important for them and they reflected upon the meaning of certain facts of the clinical case. The clarification of perspectives during ECR sessions had consequences such as increased understanding, group strengthening and decision grounding. Increased understanding involved various levels of understanding of the medical and the caring situation of the child and family and of the ethical issue. Group strengthening was about the team sharing a view of the child’s situation even if opinions differed as to how the situation should be handled. Finally, decision grounding referred to the decision being grounded because the ECR session provided a multi-perspective view of the situation, including the perspectives of the child and its family as well as the care and the medical perspectives. 20
Although the previously mentioned study 20 contributes to understanding what is going on during ECR sessions, additional analysis of the data was needed on the conditions for clarifying perspectives that could be used to improve the quality of ECR sessions, support the healthcare professionals even more and offer recommendations for implementation and training.
Objective
The aim of this study was to explore conditions for clarifying participants’ perspectives during ECR sessions in childhood cancer care.
Methods
This study is a continuation of a qualitative study 20 using observational data of ECR sessions, as well as individual and informal interviews with healthcare professionals, exploring their experiences of participating in ECR sessions. Grounded theory methodology was chosen as an appropriate design to enable the study of social patterns during ECR sessions about specific cases. Grounded theory also allows the researchers to focus on data conceptualization of what is going on. 21 –23
Sample and participants
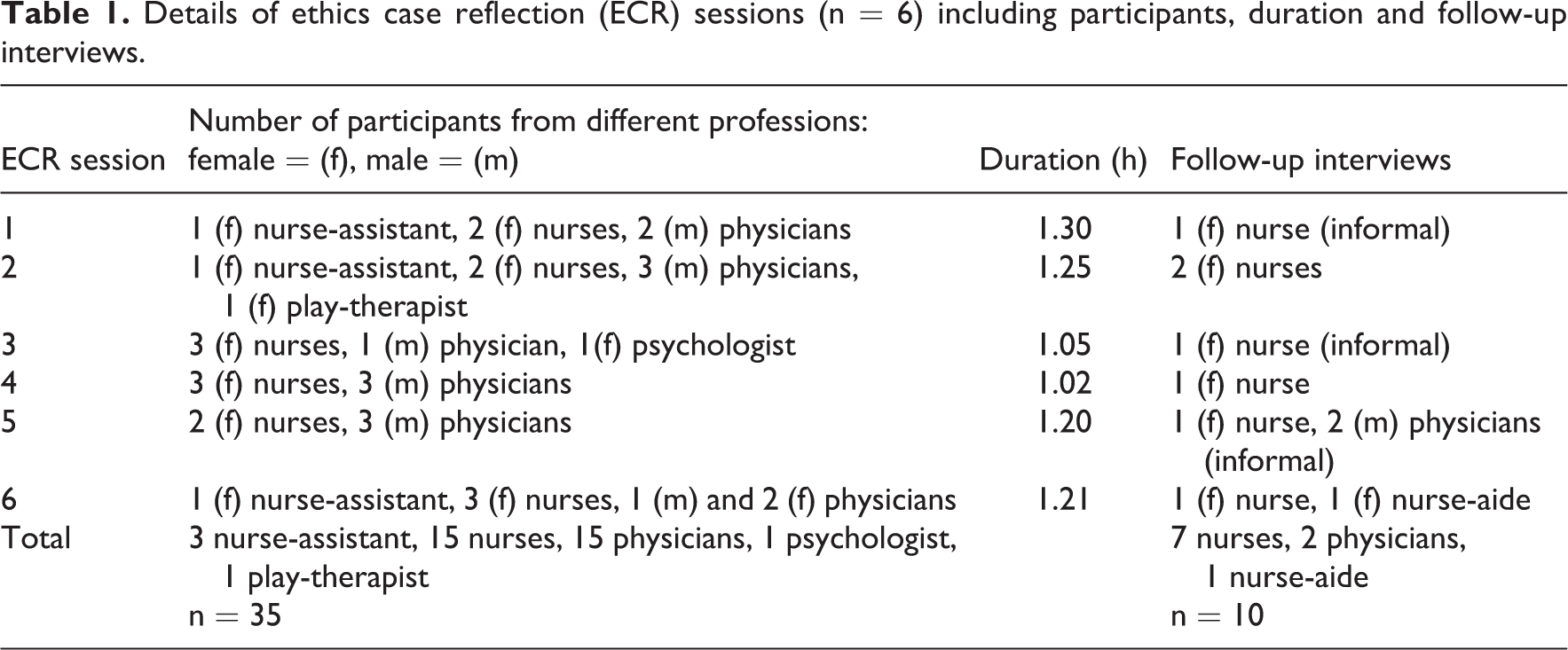
The study was conducted at a ward in a children’s hospital in Sweden. A total of 6 ECR sessions were carried out, attended by 5–7 healthcare professionals, followed by 10 interviews. More extensive details are given in Table 1.
Details of ethics case reflection (ECR) sessions (n = 6) including participants, duration and follow-up interviews.
Observations of ECR sessions
The clinical cases for the ECR sessions were identified, within childhood cancer care, by someone in the participating healthcare team. Patients are often cared for in collaboration between the childhood cancer care unit and the advanced paediatric homecare unit. Applying purposive and convenience sampling, 21 healthcare professionals (physicians, nurses, nurse assistants, psychologists and play-therapist) working at the childhood cancer care unit and the advanced paediatric homecare unit were invited to participate together in one of the ECR sessions concerning a clinical case with which they were familiar. The first author (C.B.) and the consultant nurses extended an invitation to attend the ECR session to the healthcare team members who were involved in the care of the particular child in the clinical case. Since the consultant nurses work with coordination and information and are familiar with the context, they were considered suitable to assist in this process.
Healthcare team members closest to the child in terms of responsibility and caring relationship, for example, the responsible physician and nurse, were invited to participate. Efforts were made to find a time for the ECR session when all invited were able to take part, which meant that those with extensive knowledge related to the case did participate.
Individual interviews
Theoretical sampling of participants for individual interviews and individual informal interviews was conducted to arrive at a deeper analysis of the data. Coding and analysis of the data were conducted jointly with data collection in order to determine what data to collect next and where to find it. Theoretical sampling was thus controlled by the emerging theory and provided more relevant data related to the emerging categories. 21,22,24 Healthcare professionals with experience of participating in ECR sessions in the research project were asked to participate in the interviews; all of the invited nurses accepted participation. Due to a heavy workload and extreme time constraints in the clinic during the time of data collection, physicians had difficulty in finding time for an individual interview; informal interviews were therefore performed with some of them. The facilitators were not invited to participate in the interviews because they were considered to be external ethicists and were thus not part of the team. However, facilitators are included in the observational data.
Data collection
Data collection involved methodological triangulation and included observations, individual interviews and informal interviews.
Observations of ECR sessions
The first author attended the ECR sessions as a passive observer, that is, was silent and did not participate in the reflection. Each ECR session lasted 1–1.5 h. Furthermore, an external facilitator with expertise in ethics and facilitation was invited to facilitate the ECR session. The ECR facilitators (n = 3), with different professional backgrounds (specialist nurse (1 ECR), ethicist (4 ECR), priest (1 ECR)), guided the reflections according to a modified version of the Karolinska Model for Ethical Analysis.
8
The Karolinska model includes the following steps: 1) Briefly present the background/case, 2) Identify the ethical problem, 3) Bring in the relevant facts, 4) Identify the parties involved, 5) Identify what is at stake (interests, values, and moral principles), 6) Identify available action alternatives, 7) Evaluate each alternative action, 8) Carry out the ethical argumentation; try to reach agreement on a recommendation p.89.
26
Individual interviews
Participants from the ECR sessions were invited to tell their story during open interviews, each of which lasted approximately half an hour and was held in a separate room at the hospital. The interviews took place in close connection with the ECR sessions. One participant was interviewed by telephone. The interviews were conducted, using a semi-structured interview guide with open questions, to gain a richer understanding of the participants’ experiences of the ECR sessions and the facilitator’s role. The technique of open-ended conversations was used in all interviews. 23 In order to get a deeper understanding, laddered probing questions were used, such as ‘What happened?’ ‘How did you deal with it?’ and ‘What do you think about that?’. 27 Four of the 10 interviews were audio-recorded and field notes were taken after each interview. In accordance with grounded theory, data were analysed between the ECR sessions and the interviews, which influenced the questions in subsequent interviews. 21 Field notes were taken during the interviews and memos were written immediately afterwards.
Individual informal interviews
Directly after some of the ECR sessions, informal follow-up questions were put to a theoretical sample of ECR-participating healthcare professionals (Table 1). Examples of addressed questions were as follows: What did you think about the ECR session? and What was important during the ECR session? The informal interviews were carried out in the hallway or in the staff room. The informal interviews lasted 5–10 min and enriched the data collection with further data related to the substantive area. Field notes were taken directly after the informal interviews.
Data analysis
To get a comprehensive overview of the collected data, including both field notes and transcribed audio-recordings, the text was read several times by the first author. Open coding was done when reading the text; recurrent interchangeable indicators in the data created substantive codes. 21 For example, indicators that created organizational conditions were healthcare professionals’ experiences of time, structure and climate. The initial coding was performed in the previous study 20 and in this study selective coding was performed on conditions. 21 Codes were then grouped into categories through constant comparison of incidents and codes. 21
Categories were renamed after discussion among the researchers and during the conceptualization process, trying to capture a pattern that best fitted the empirical data. The ensuing phase involved saturating the categories by theoretical sampling. 24 This was done by interviewing participants to further explore several categories (e.g. space for inter-professional perspectives). During the analysis of the data, memos were frequently written down; they included ideas about a conceptualized pattern of the categories and about comparisons between categories. 24 The last author (P.P.) independently read all of the transcribed data and discussed the coding pattern, which could be seen as investigator triangulation, increasing trustworthiness. Thereafter, four of the authors validated the findings; discussing the analysis until consensus was reached.
Ethical considerations
Oral and written information about the purpose of the study and information about the voluntary nature of participation, stating that participants could end their participation at any time without having to explain why, were given to all healthcare professionals. An option to decline audio recording was also given to the participants. In order to protect the children's and their parents' anonymity names were not mentioned during the reflection sessions or during the follow-up interviews. In the prospective cases oral informed consent was collected from parents. General information about the project was also posted on a notice board placed at the unit during the project. This study was approved by the regional ethical review board in Stockholm (2009/1666-31/5).
Findings
In this study, conditions for clarifying participants’ perspectives during ECR sessions were explored in the data. After repeated joint analyses, ‘organizational enablers and barriers’ as well as ‘team-related enablers and barriers’ emerged. Each category contains several sub-categories, described in Table 2.
Overview of the results including categories and sub-categories.
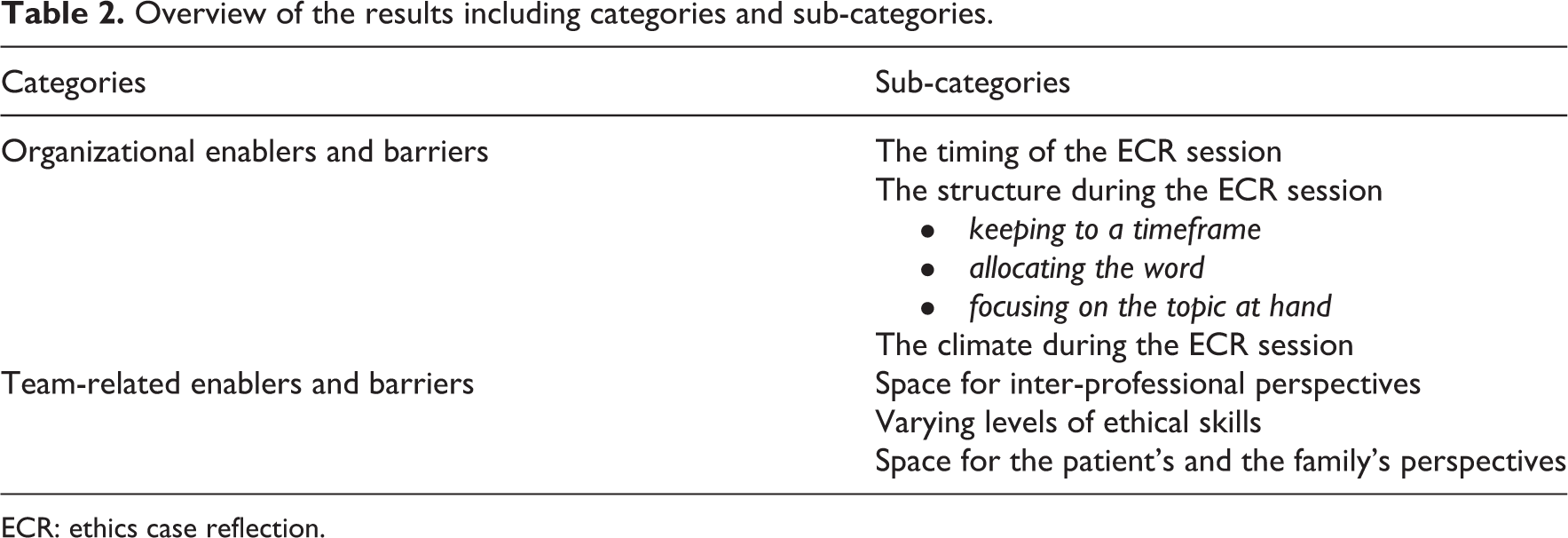
ECR: ethics case reflection.
Organizational enablers and barriers
Organizational enablers and barriers refer to organizational aspects that influence possibilities of clarifying participants’ perspectives during ECR sessions. These aspects include ‘the timing of the ECR session’, ‘the structure during the ECR session’ and ‘the climate during the ECR session’.
The timing of the ECR session
Right timing is an important aspect, enabling professionals to clarify their perspectives to create a common picture of the situation. In this study, timing concerned the point in the child’s healthcare process when the ECR session was held. Healthcare professionals expressed a need for ECR sessions early in the healthcare process because they believed that could have a positive effect on care: We had the ECR session incredibly late [in the child’s healthcare process]; it should have been done much earlier, very much earlier. I think we’ve lost a major source of information about the entire situation of the family and what their experience has been. (Nurse in interview) If we had not stopped and reflected, I think the risk is that it [treatment] had rolled on. I think it is good to capture [the ethical issue] in an earlier stage when it is developing an ethical issue. (Nurse assistant in interview)
The structure during the ECR session
This concerns the structuring of the communication within the ECR session and includes ‘keeping to a timeframe’, ‘allocating the word’ and ‘focusing on the topic at hand’. In this study, the facilitators played an important role for the reflection’s structure. The facilitator addressed the structure of the ECR sessions at the beginning of the session and explained the rules that would apply during the session (e.g. the code of conduct for participants’ behaviour). An example of such a rule is to try to truly and sincerely listen to the others and avoid persuading the others.
Keeping to a timeframe includes both the total time allocated for the session and the time spent on the various phases of the reflection. In this study, participants were sometimes eager to move on to the next phase in the ethical reflection during the ECR sessions. This could result in a risk of hastening the dialogue and missing important aspects and perspectives of the ethical issue. On the other hand, observational data also revealed that spending too much time on a specific phase of the reflection could lead to a lack of time later on (e.g. when the ethical issue was hard to identify in the beginning of the ECR session, there was less time for analysing it).
Allocating the word, when successful, means that all the participants are given a chance – that is, the necessary time and space – to be heard; this was assisted by the facilitator. Without allocation of the word, there is a risk of getting a limited view of the situation. Interviewed nurses explained that an advantage of allocating the word to all participants was that it brought a feeling of shared participation: Absolutely, there was a space for everyone to say something, if you had something to say, and [space for] what you had to say. One felt included in the discussion! (Nurse in interview)
Focusing on the topic at hand means using strategies to focus on the ethical issue and includes posing questions to explore the meaning of the words used and using a conversation model. An unfocused dialogue could, for example, risk not exploring the meaning of the words used. Questions are used by the facilitator and participants to encourage the expression of examples and the illustration of personal opinions: Are you thinking ahead? [Do you think about] what it means for the patient if we continue the treatment? (Physician in ECR session) Yes, exactly, what kind of life would it be in that case? Does it result in suffering for 24 more months or is it going to be 24 good months? (Nurse in ECR sessions)
At the same time, participants expressed that the model should not be followed too strictly: I think it’s good that you have a model, as long as you’re not being too strict. It’s good to have a model to refer to so things don’t get out of control, but to still be open to other issues so that it doesn’t get too strict, particularly when it comes to ethical issues. (Nurse in interview)
The climate during the ECR session
A good climate within the organization accommodates reasoning and reflection among participants. In this study, a good climate was experienced as tolerant and safe. When a dispute emerged, conceivable hypotheses and speculation were discussed openly. Proposals for action were laid out for examination so that unreasonable proposals could then, after a shared analysis, be jointly rejected. The climate was permissive for the participants to think out loud as well as to express themselves and their personal thoughts. ‘I can understand that. As a parent, I can’t say I wouldn’t grasp at straws myself’ (Nurse in ECR). However, if the prevailing climate was not good, there was a risk of the ECR session being used to try to persuade or pressure someone through authoritarian claims or group pressure.
Not only were organizational conditions identified, but also features of the team that are key enablers and also possible barriers.
Team-related enablers and barriers
This category involves features within the team and its composition that are related positively or negatively to clarifying perspectives during ECR sessions. The team-related enablers and barriers are ‘space for inter-professional perspectives’, ‘varying levels of ethical skills’ and ‘space for the patient’s and the family’s perspectives’.
Space for inter-professional perspectives
This is about the team allowing space for inter-professional perspectives that are affected by, for example, hierarchical structures. Space during the ECR session is needed for different perspectives in order to get a full understanding of the situation and is thus a prerequisite for clarifying perspectives: It is important for me that everyone can have their say and that we represent different professional categories [during ECR sessions] because everyone has various tasks within the care [of the child]. It is also important that everyone gets to hear the others’ experiences, but above all, that everyone can have their say. (Nurse in interview) I felt that the physicians took over and it was a long presentation of the medical situation…actually it was about continuing treatment. One did not really start talking about what was difficult with the nursing care interventions. It would have come up at once if everyone had shared their view…(Nurse in interview)
Varying levels of ethical skills
The levels of ethical skills can vary in a team. Ethical skills include, for example, identification of conflicting values and expressing values and norms in relation to the ethical issue. They also include presenting one’s own perspective and arguments in the discussion. This appeared to be an important team-related condition for clarifying participants’ perspectives. Someone with good ethical skills contributes with arguments and values in the reflection and other participants can learn from that person. However, this could become a barrier if the perspectives of those with lower ethical skills are not being addressed in groups. This was frequently observed among participants in this study during ECR sessions: I’m not the person who puts words on what the problem is. I’m not an analytical person.…So I’m not used to that way…it’s more a feeling like it was difficult to know what one wants, what the purpose was. (Nurse in interview) For him, yes, it was obvious that he was skilled in ethics and knowledgeable…and I thought he understood the situation well. (Nurse in interview)
Space for the patient’s and the family’s perspectives
This team-related sub-category is about whether the team includes the perspective of the child and the family during the ECR session, which could be a condition or a barrier for clarifying perspectives during the ECR session. During the ECR sessions in this study, healthcare professionals assisted each other by sharing information about the child’s and family’s perspectives and situation in the team: It is all the time new information [about the patient’s situation] that we are not familiar with, we do not know everything. But sometimes it can be helpful when you put it on the table like this, one sees additional needed information. (Physician in ECR) I have not been so much involved in this child. I got the information, during the ECR session, about what they thought and why they are doing what they are doing; I think it became clear that it was difficult [for me] to understand and contribute. (Nurse in interview)
Discussion
This study explores organizational and team-related conditions for healthcare professionals when clarifying participants’ perspectives during ECR sessions in childhood cancer care. The organizational enablers and barriers that emerged were named ‘the timing of the ECR session’, ‘the structure during the ECR session’ and ‘the climate during the ECR session’. The discovered team-related enablers and barriers were named ‘space for inter-professional perspectives’, ‘varying levels of ethical skills’ and ‘space for the patient’s and the family’s perspectives’.
Our data reveal that in the organization of the ECR session, timing seems to be crucial. One could argue that the point in the healthcare process at which the ECR session is held must be chosen from case to case. In some cases, healthcare professionals need to have a shared reflection early in the healthcare process; in others, the situation must mature before initiating an ECR session. Nevertheless, what is most important is that time is in fact found for reflection in the team and that a dialogue is held about ethical issues and possible actions in care. A recently performed study of the literature of ethics support indicates that systematic reflection on ethical issues can improve the quality of care and make care-givers more satisfied with their work, especially when it is performed in the inter-professional team. 28
Space for inter-professional perspectives in the ECR session was found to be a team-related condition for healthcare professionals to clarify their perspectives. Previous research on inter-disciplinary work gave rise to the theory of pluralistic dialoguing.
29
When the team acknowledges its disciplinary differences and focuses on the patient, inter-disciplinary work is possible. According to McCallin, dialoguing is a basic social process and the core of successful teamwork. The theory explains how pluralistic dialoguing has helped clinicians reanalyse situations, focusing on the patient and looking for a common care intention. Dialoguing facilitates the team’s collaboration.
29
Dialoguing is similar to the idea of a good climate for reasoning that emerged in this study. Without a good climate for reasoning, it can be hard to clarify every perspective.
Kessels et al.
30
wrote,
A dialogue is neither just a conversation, nor a discussion nor a meeting. It is an explicit, joint effort to inquire into something. It is a conversation at its best about who we are and what we have to do. p.17
If someone in the team feels unsure about raising his or her voice in a group consisting of professionals with a higher education or a higher level of decision-making, he or she might choose to remain quiet and not present the value experienced. Hence, all perspectives will not be heard if some team members do not present their relational knowledge and view of the case. Hierarchical structures differ throughout the world. Sweden is perceived as having a relatively low degree of hierarchy in the healthcare system, but our data still reveal that a hierarchy is present during ECR sessions and can be a barrier to clarifying perspectives. Perhaps it is not the hierarchy that constitutes the problem but rather how it is tackled in ECR sessions. Some research indicates that an open, constructive reflection is facilitated by having heterogeneous non-pre-existing groups. 31 A Swedish study by Thylefors on dominance, status and efficiency in Swedish inter-professional teams confirms our findings. Hierarchy was related to profession in the case of verbal dominance and verbal dominance matched the level of education or degree or professionalization. 32 Psychologists, physicians and social workers verbally dominated the team meetings in general, which greatly influenced decision-making, while nurses took a subordinate role, and nurse assistants were found at the lower end of the hierarchy scale. 32 Attention should also be drawn to the facilitators, who gave the word more consistently to those with extensive medical knowledge of the case. This could be addressed in future facilitator training, including theory and practical training about facilitating an inter-professional dialogue.
Varying levels of ethical skills were found to be an additional barrier to clarifying perspectives. Previous research shows that healthcare professionals have poor knowledge of basic ethics. 33 Milliken and Grace stated that patients risk harm when there is a lack of ethical awareness and that this may lead to inaction or routine care. The harm is due to the care not being directed by the patient’s goals and wishes and this could be potentially harmful in regard to outcomes. 34 Space for the patient’s and the family’s perspectives emerged as important to clarify participants’ perspectives of the situation. Familiarity about the facts and the ethical issue at stake in the case have not been described as relevant for participants in research using models where a case presenter presents a case that is unknown to the other participants. In those situations, participants need to ask the case presenter questions to be able to decide what values are most important in the specific case. 6,16 In previous studies, a sense of unconcern 31 and different levels of involvement 5 have been described as negative experiences of ECR sessions. This did not emerge as a major concern in our study, which could be explained by all the participants having relational knowledge of the specific case, being members of the inter-professional team caring for the child. One could argue that, in models using a case presenter, this person’s responsibility could be burdensome, both to present the case and to encourage involvement of the other participants. Furthermore, familiarity with the case will be only from the case presenter’s perspective.
Discussion on methods
The validity and reliability of qualitative research is often assessed by its trustworthiness, which involves triangulation; methodological and investigator triangulation have been used in this study.
Sometimes we as researchers should ask ourselves whether and when categories are saturated and no more data needs to be collected. The clinical situation at the childhood cancer unit during data collection was burdensome for the healthcare professionals who experienced lack of time. Thus, time constraints influenced saturation and data collection and, in our case, more specifically the theoretical sampling. However, the emerging categories were discovered early on. Bearing in mind the clinical conditions and the participants, the decision to end data collection was made and the total of 6 ECR sessions and 10 follow-up interviews was considered sufficient to achieve scientific quality. One could argue that it would be interesting to use the results of this study as a basis, for example, to explore the identified enablers and barriers in a questionnaire study, making it possible to reach a larger population and other contexts as well.
When studying the team members in a presumed hierarchical situation, data richness could be limited when participation is affected by power issues. However, interviewing individuals afterwards gave the participants the opportunity to tell their story of how they experienced the team reflection.
Another limitation of the study is that facilitators were not individually interviewed after each ECR session. For example, when it transpired that they were giving the word more consistently to those with extensive medical knowledge, it would have been interesting to explore the facilitators’ experiences on this to see how they perceived the situation observed in data. This can be addressed in further research.
Conclusion
In this study, in childhood cancer care, the timing of the ECR session, the structure during the ECR session and the climate during the ECR session were identified as enablers and potential barriers related to the organization. The team-related enablers and barriers were identified as space for inter-professional perspectives, varying levels of ethical skills and space for the patient’s and the family’s perspectives. When both the organizational and the team-related enablers are present and the barriers, identified in this study, have been overcome, clarifying participants’ perspectives is possible during ECR sessions. Knowledge about the importance of timing, structure and a good climate are relevant because these enablers are essential for the organization of ECR sessions. Awareness of the potential advantage of medical perspectives over nursing perspectives could reduce the somewhat unilateral attention and contribute to an inter-professionally shared reflection. Dealing with ethical issues is becoming more and more a future element of professional competence and for that reason healthcare professionals need training in how to perform a dialogue about ethical issues. When organizing training in ECR sessions, the new knowledge of the enablers and barriers can improve the training by taking them into account.
The added value of this research, in relation to the existing literature on clinical ethics support, is that the results provide important theoretical and practical knowledge about the conditions for ECR sessions in childhood cancer care. The results could be applicable to other healthcare settings that are about to implement ECR sessions and could contribute to the quality of ongoing ECR session although modifications may be needed to fit the context.
Clinical implications
The results of this study can contribute to making healthcare professionals across disciplines more able to facilitate the implementation of ECR sessions and improve their quality. When evidence-based reflections are performed about ethical issues in clinical practice, it will most likely lead to better care for patients and families.
Footnotes
Acknowledgements
The authors thank all healthcare professionals who contributed to this study and the facilitators and consultant nurses for their valuable work.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by AFA Insurance (Grant no. 120019), the Swedish Cancer Foundation (Grant no. CAN 2009/912) and the Swedish Childhood Cancer Foundation (Grant no. FoAss 13/07).