
Abstract
Background:
The families of brain-dead patients have a significant role in the process of decision making for organ donation. Organ donation is a traumatic experience. The ethical responsibility of healthcare systems respecting organ donation is far beyond the phase of decision making for donation. The principles of donation-related ethics require healthcare providers and organ procurement organizations to respect donor families and protect them against any probable harm. Given the difficult and traumatic nature of donation-related experience, understanding the outcomes of donation appears crucial.
Objective:
The aim of this study was to explore the outcomes of organ donation for the families of brain-dead patients.
Methods:
This was a qualitative descriptive study to which a purposeful sample of 19 donor family members were recruited. Data were collected through holding in-depth semi-structured interviews with the participants. Data analysis was performed by following the qualitative content analysis approach developed by Elo and Kyngäs.
Findings:
The main category of the data was “Decision to organ donation: a challenge from conflict to transcendence.” This main category consisted of 10 subcategories and 3 general categories. The general categories were “challenging outcomes,” “reassuring outcomes,” and “transcending outcomes.”
Ethical considerations:
The study was approved by the regional ethical review board. The ethical principles of informed consent, confidentiality, and non-identification were used.
Conclusion:
Donor families experience different challenges which range from conflict and doubtfulness to confidence, satisfaction, and transcendence. Healthcare providers and organ procurers should not discontinue care and support provision to donor families after obtaining their consent to donate because the post-decision phase is also associated with different complexities and difficulties with which donor families may not be able to cope effectively. In order to help donor families achieve positive outcomes from the tragedy of significant loss, healthcare professionals need to facilitate the process of achieving confidence and transcendence by them.
Introduction
The growing need for donor organs has turned into a worldwide major health concern. 1 Donating the organs of a brain-dead patient is an altruistic and widely applauded practice. 2,3 Nonetheless, families’ refusal to donate their brain-dead member’s organs is a formidable barrier to organ donation. 4 Therefore, many studies have been conducted in recent years in order to identify factors affecting families’ decision to donate and also to encourage families to consent for donation. 3 –9 These families usually need to decide to donate while they are in difficult, complex, and traumatic conditions. 10 –12 Besides, deciding to consent for donation is not an end to families’ distress, and thus, strong post-decision support is needed to alleviate their distress and enhance their psychological stability. 10,13,14 In fact, the need for post-decision support highlights the ethical responsibility of healthcare and organ procurement systems because respect for persons and non-maleficence are the basic principles of ethical practice in the field of organ donation and transplantation. 15
According to Simmons et al. (1983, 1985, 1988) as cited in Burroughs et al.’s 11 study, studies on live donors have shown a positive image of donors’ post-donation lives. However, this image may not be so positive with respect to the families of brain-dead donors. Besides, there are few studies regarding follow-up programs for these families. 1 A qualitative study into Taiwanese donor families’ experiences during the first 6 months after donation showed that organ donation had both negative and positive impacts on donor families. The most significant negative impact was concern over the donor’s afterlife while the most important positive impact of donation was a sense of reward for helping others. 10 In addition, several quantitative studies have been done to assess families’ post-donation experiences and grief. 16 –21 For instance, a study showed that donation had positive effects on the process of grief in that the decision to donate had prevented the donor families from feeling inconsolable and complicated grief. 17 However, two other studies reported that deciding to donate does not spontaneously alleviate donor families’ loss-related pain and suffering. 20,22 Besides, some studies highlighted that making decision about organ donation is an added burden for the families of dead people and can predispose the families to posttraumatic stress disorder. 23,24 Another study also found that 14% of the families who had decided to donate regretted their decision. 11 Such regret can trigger a set of disturbing thoughts which negatively affect bereaved families’ quality of life. 12 All these findings show that there is no consensus over the outcomes of deciding to donate for the families of brain-dead patients. Such conflicting findings may be due to the differences in the methods of the studies as well as the effects of different cultural and religious beliefs of different communities on the perceptions of donor families and the process of organ donation. Besides, previous studies focused mainly on assessing certain predetermined aspects and outcomes of organ donation such as the process of grief, taking donor families’ experiences for granted.
Healthcare providers need to explore donor families’ post-donation experiences in order to understand and manage their needs with greater sensitivity. 25 Acquiring more in-depth knowledge about donor families’ post-donation experiences and understanding their situations can enhance the quality of care provided to these families. Besides, paying closer attention to these families can enhance the reputability and the soundness of organ donation activities, and thereby, it can positively affect organ recovery. 1 This study sought to explore the outcomes of organ donation for the families of brain-dead patients.
Methods
An inductive qualitative design was used in this study. This design is used when there are limited theories and research about the intended phenomenon. 26
Participants
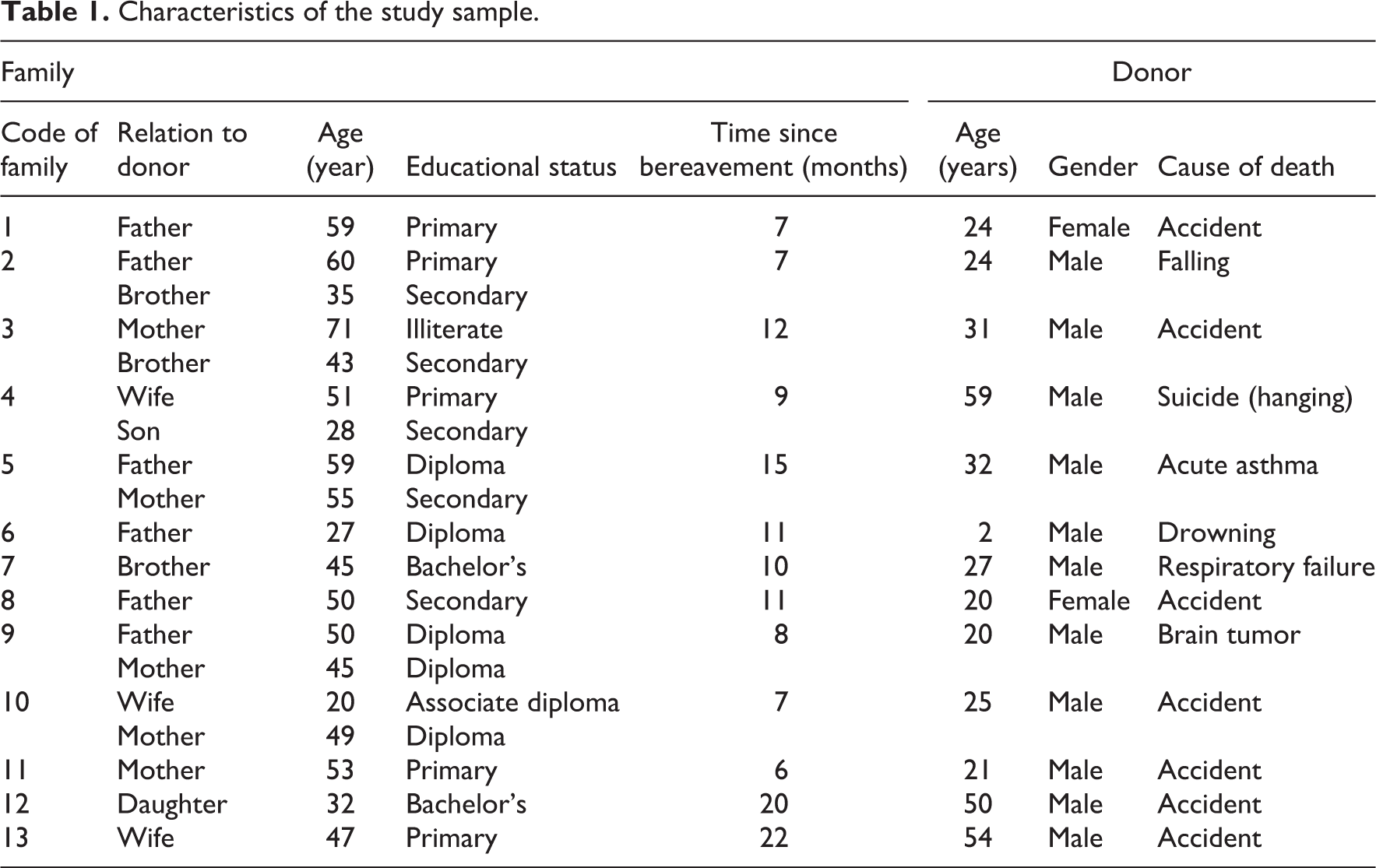
The study population was the family members of brain-dead patients who had been requested to donate their brain-dead member’s organs and had consented to do so. They were recruited from the Transplantation Center of Mashhad University of Medical Sciences, Mashhad, Iran, and were included in the study if at least 6 months had passed from their loved one’s death. Sampling was started in August 2014 and continued until reaching data saturation, that is, when no new data were obtained from the participants. The study data became saturated in June 2015. The participants widely varied in terms of variables such as kinship with their brain-dead family members, place of residence, educational status, social class, and the time period between their loved one’s death and the time of the study. Accordingly, six fathers, five mothers, three brothers, three wives, and two children of brain-dead patients participated in the study. Table 1 shows the participants’ characteristics.
Characteristics of the study sample.
Setting
Iran is a developing Islamic country and Mashhad is its second largest city. The organ procurement center of Mashhad University of Medical Sciences, Mashhad, Iran, was established following the enactment of the cadaveric organ and tissue donation law in 2000. In this setting, researchers in a quantitative study evaluated factors affecting donor families’ decision to donate the organs of their brain-dead members and reported religious and transplantation-related beliefs as the most important predictors of decision to donate. Their findings showed that Iranians’ firm religious and altruistic beliefs as well as their beliefs in the usefulness of transplantation are significant factors behind their will to donate their brain-dead family members’ organs. 9
Data collection
Semi-structured face-to-face in-depth interviews were held for data collection. The opening interview question was, “Would you please explain about what happened to you after deciding to consent to donate?” Thereafter, the flow of the interviews was managed to cover the aim of the study through asking questions such as “What were the consequences of a decision?” “How did the decision affect your life?” and “What feelings did you experience after the decision?” Besides, in order to clarify the interviewees’ ideas, we used searching questions such as “Can you explain more about…?” and “What did you mean by…?” Six interviews were held with two-person groups of participants while the remaining seven participants were interviewed personally. Therefore, the total number of the interviews was 13. The length of the interviews ranged from 36 to 53 min. All interviews were held by the first author, typed word by word, and managed by using the MAXQDA (v. 10.0) software.
The trustworthiness of the data was ensured based on the criteria proposed by Lincoln and Guba 27 and through adopting techniques such as simultaneous data collection and analysis, recruitment of key informants, thick description of the findings, and peer checking with a qualitative researcher (i.e. the second author) and a transplant coordinator (i.e. the third author) who had a 12-year professional experience of working with donor families. The transplant coordinator was involved in purposive sampling, reviewing the interviews, and checking the congruence between interviews and the generated codes while the qualitative researcher contributed to the process of coding and describing the data.
Data analysis
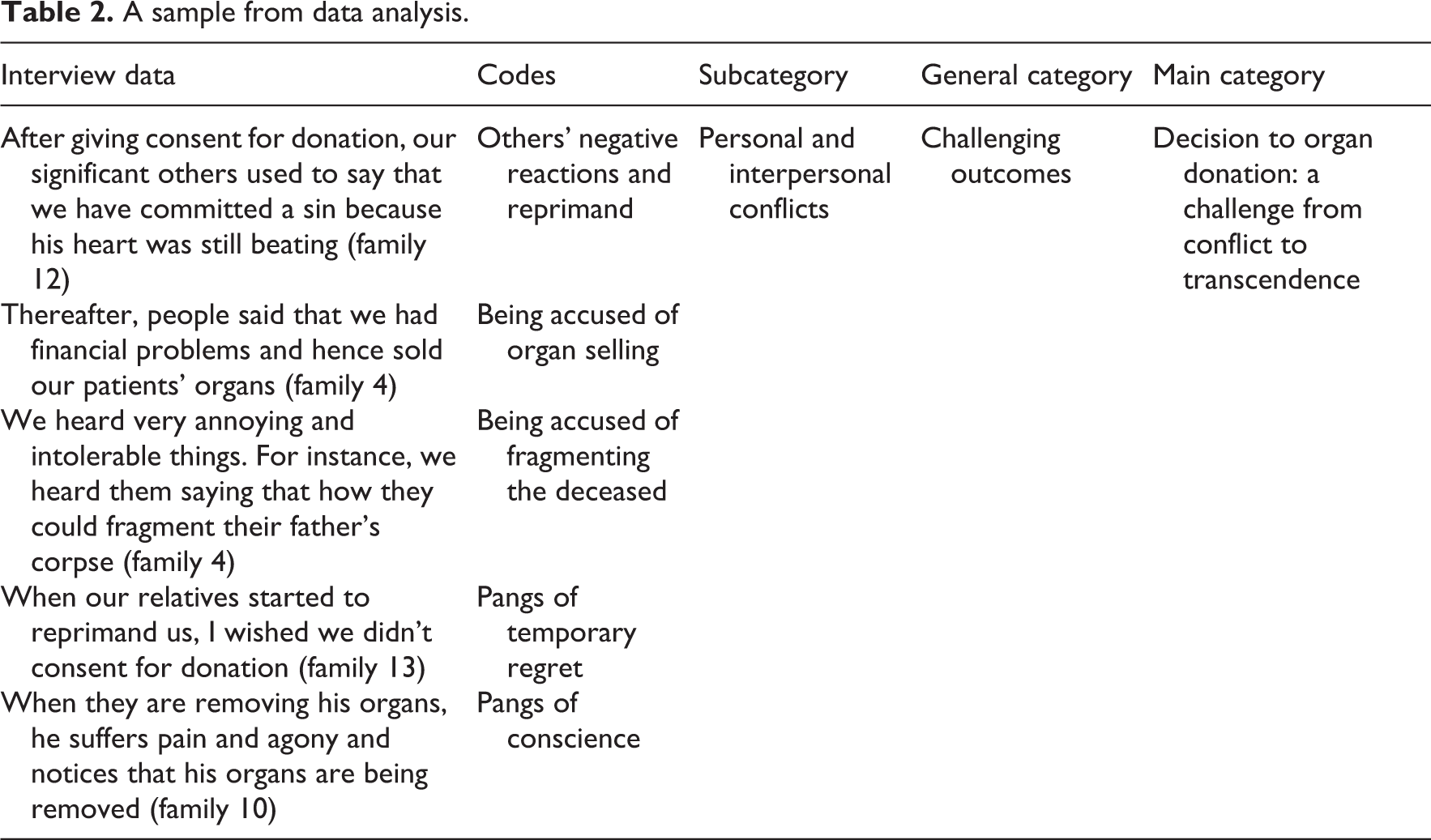
The study data were analyzed through following the qualitative content analysis approach developed by Elo and Kyngäs. 28 In this approach, data analysis is performed in the three phases of preparation, organizing, and reporting. 28 The aim of the preparation phase is to understand and get closer to the data. Consequently, the transcribed interviews were read frequently in order to make sense of the data. The second phase, that is, the organizing phase, includes open coding, categorizing, and abstracting the data. Initially, open coding was done and then the similar codes were grouped into subcategories. Afterward, subcategories with similar contents were grouped to form general categories. Finally, the main category was abstracted from the general categories. A sample from data analysis is presented in Table 2.
A sample from data analysis.
Ethical considerations
The Ethics Committee of a local university in Tehran, Iran, approved the study. A letter of introduction was obtained from the university and provided to the administrators of the study setting. At the first telephone contact with the eligible families, they were provided with information about the study and were asked to voluntarily participate in it. After 1 day, in the next telephone contact by volunteers, the time and the place of interview were determined.
Before the interviews, the aim of the study was explained to the participants and their written informed consent was secured. Besides, we ensured the participants that their data would remain confidential. Considering the emotional burden of remembering and verbalizing traumatic and painful experiences of their loved one’s death, 29 the participants were provided with the opportunity to refrain from sharing their experiences and also to withdraw from the study at any time during its course. They could ask to receive psychological counseling services. Moreover, they were asked to report any probable post-interview emotional distress to us even though none of them withdrew from the study or reported the need for psychological counseling during the study. We attempted to create a comfortable and supportive atmosphere during the interviews. In addition, the participants were provided with the opportunity to select the time and the place of the interviews and also to participate in the interviews in companionship with a close family member. Moreover, we entertained them during interviews and acknowledged their participation by a gift and a thank-you letter at the end of the interviews.
Most families tended to provide a full explanation of their donation-related experiences. Besides, in order to respect their emotions, they were free to verbalize their concerns, fears, and experiences which might have not been directly related to the aims of the study. Such information was used for interpreting and clarifying some aspects of their donation-related experiences. Besides, most of them found interviews as opportunities for verbalizing their feelings and concerns.
Given the potential of the interviews for causing the interviewer emotional distress, 29 she supported emotionally by the members of research team.
Limitations
The participants of this study were selected just from four cities in Khorasan Razavi province, Iran. Due to the wide socio-cultural diversity among Iranian people, the findings may not be transferrable to all Iranians. Further studies in different provinces in Iran may show potential differences.
Findings
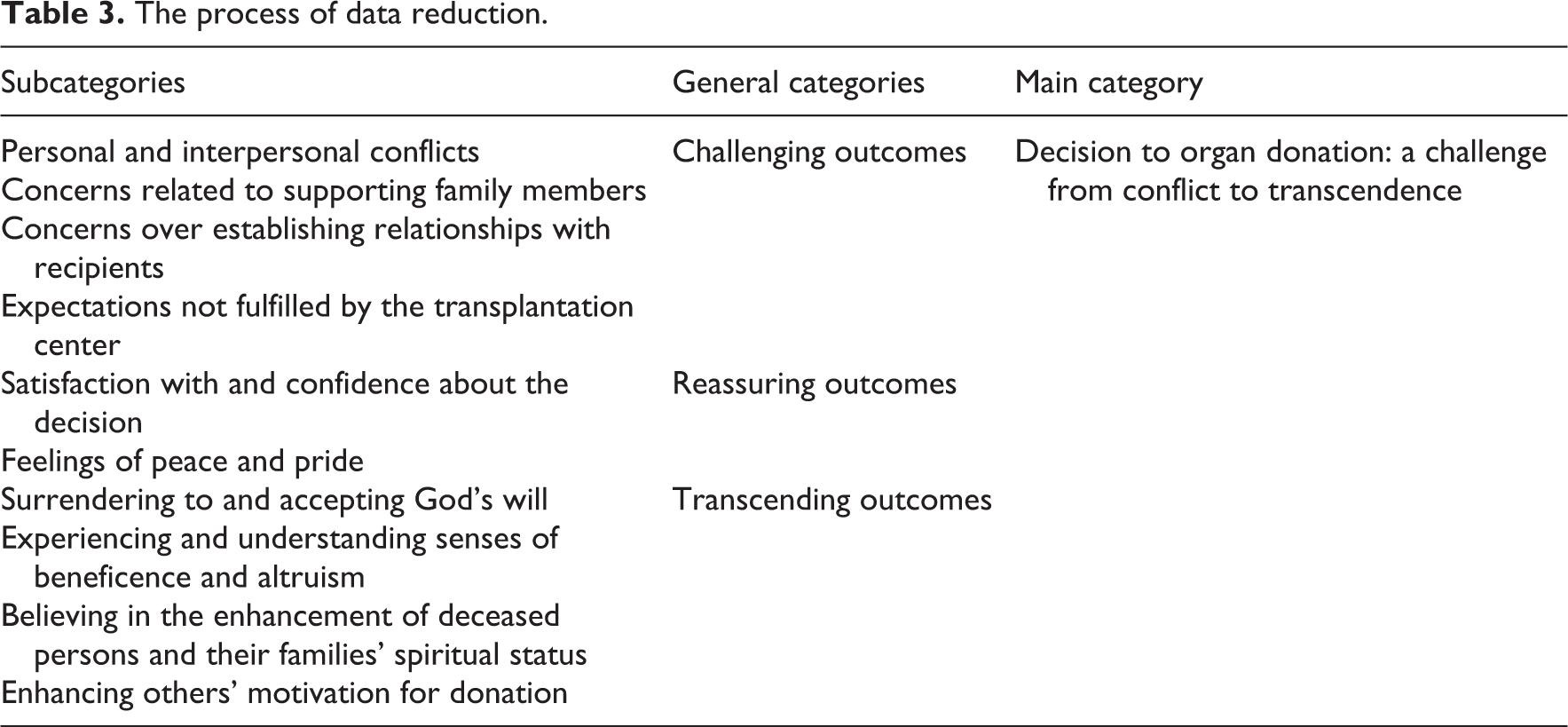
The analysis of the study data yielded to the generation of 361 primary codes, 10 subcategories, 3 general categories, and 1 main category. The main category was “Decision to organ donation: a challenge from conflict to transcendence.” This main category was generated from reducing and abstracting other categories and subcategories. The process of data reduction is presented in Table 3. The general categories of this main theme were “challenging outcomes,” “reassuring outcomes,” and “transcending outcomes.” These categories are explained in detail below.
The process of data reduction.
The challenging outcomes of organ donation
During and after deciding to donate, the donor families had experienced different challenges. The families needed to spend a great deal of energy and make serious attempts in order to deal with these challenges and handle their difficult situations. The different aspects of these challenges were categorized into four subcategories, including personal and interpersonal conflicts, concerns related to supporting family members, concerns over establishing relationships with recipients, and expectations not fulfilled by the transplantation center.
Personal and interpersonal conflicts
The study participants had experienced several personal and interpersonal conflicts. Personal conflicts included, but were not limited to, doubtful thoughts, feeling of guilt, and pangs of conscience: I felt guilty. I thought that he may be dissatisfied. Many instances of “maybe” hit my mind. At the first days, I thought that we did not have the permission to terminate the life of a person whose heart was still beating. (Family 12) I had pangs of conscience and said to myself that if I did not consent to donate, he might show some degree of recovery. (Family 10) When my son’s intimate friend had seen that the eyes of my son’s corpse had been enucleated and sewed, he told us, “At that moment, I hated you very much.” (Family 5) We heard many difficult-to-tolerate things. For example, some people asked us, “How much money did you get?” or “Why did you fragment the body of the child?” As a result, my wife experienced great discomfort. Unfortunately, instead of giving us solace, they made us unhappy. (Family 6)
Concerns related to supporting family members
Some participants had employed preventive strategies in order to support their family members and protect them against others’ negative reactions such as the accusation of selling organs, hypocrisy, and ostentation: I said my mother, “Get ready and never react to others’ sayings. You surely made a right decision. They may say that we have sold his organs.” We didn’t even use condolence cards and banners provided by the transplantation center in order not to be accused of hypocrisy and ostentation. (Family 3) I disagreed with cornea donation although they ensured us that they would enucleate the eyes so that nobody would notice it. Nonetheless, the appearance of a corpse whose eyes are enucleated may not be very pleasant to family members who are visiting the corpse of their loved one for the last time. I considered it likely that the post-enucleation face would differ from relatives’ known image of their loved one’s face. (Family 3) We had donated his cornea. I took to the hospital all relatives who wanted to say goodbye to the corpse and thus, I didn’t allow them to revisit the corpse after organ removal. I wanted the same face which they had seen previously to remain in their minds. (Family 7)
Concerns over establishing relationships with recipients
Communicating with transplant recipients was another main challenge faced by the donor families. Some of them had succeeded in establishing communication, were satisfied with transplant success and recipients’ recovery from their problems, and considered recipients as their own new family members. Nonetheless, despite their great willingness to communicate with the recipients, some of them were not successful in doing so and hence they were deeply dissatisfied: The recipients even neither gave us a condolence nor thanked us. Nobody even made a simple telephone contact with us. This is the outcome of a donation! My daughter really wanted to know about the recipients’ health status and to know that whether the recipient of his eyes is able to see well or not. (Family 4) Sometimes, we think about the possibility of visiting recipients. I’m afraid of the probability of distress and sorrow both for us and them. They may feel that they are indebted to us and hence, they may feel unhappy. (Family 5)
Expectations not fulfilled by the transplantation center
The transplantation center managed the processes of organ donation request, organ retrieval, and organ transplantation. Besides, it took measures to pacify donor families and fulfill their needs. Issues such as ambiguous information provided by the center to the families, families’ limited knowledge about the authorities of the center, and families’ inability to process, respond to, and manage all suggestions provided by the center were among the challenges faced by the participants. Measures such as sending condolence cards, banners, and gravestone as well as participation of the center staff in the funeral had provided some families with satisfaction. However, as mentioned earlier, some families had refused suggestions of this type in order not to commit hypocrisy and ostentation. On the other hand, some families had had some expectations which had been beyond the authorities of the center: We expect the center to provide us with some insurance facilities. For instance, they could introduce us to insurance organizations and pave the way for some allowances for my dead son’s wife and children. (Family 2) When we took the corpse, we noticed that his eyes have been sewed; but, they didn’t tell us that to whom they had transplanted the eyes. We want to know who has been the recipient. Issues like this annoyed us. (Family 2)
Reassuring outcomes of organ donation
Despite facing some challenges and undergoing some negative experiences, all families felt sure about the rightness of their decision to donate. The reassuring outcomes fell into two subcategories including satisfaction with and confidence about the decision and feelings of peace and pride.
Satisfaction with and confidence about the decision
Most of the participants’ relatives and significant others had approved their decision to donate and hence they were confident about and satisfied with their decision. Such a confidence and satisfaction improved the participants’ stability in their decision: Everyone who heard about it approved our decision. (Family 1) He had personally willed his organs to be donated [after his death]. I said all people that we exactly did the same thing that he had willed. (Family 9) The ability to make the best decision in such a situation greatly satisfies us. (Family 6) I have told my family as well that I will do the same again if I experience the same situation in the future once more. (Family 5)
Feelings of peace and pride
Despite experiencing many challenges and great sufferings, the study participants had acquired senses of peace and pride due to making such a decision: I’m really proud of myself. All my relatives and friends also pride us on making such a decision. (Family 2) My parents are really proud of themselves. My brother was to be placed under the ground. However, several people are using his organs and are feeling better now. (Family 7) Our pride is that several persons are no longer ill and this is really of great for us. (Family 4) Giving life to several persons and its subsequent reward for my father was a relief to us. (Family 12)
Transcending outcomes
A set of the outcomes were related to the positive post-decision feelings which reflected the participants’ spiritual, cultural, and altruistic promotion. This general category consisted of four subcategories which included surrendering to and accepting God’s will, experiencing and understanding senses of beneficence and altruism, believing in the enhancement of deceased persons and their families’ spiritual status, and enhancing others’ motivation for donation.
Surrendering to and accepting God’s will
One of the main reasons behind the participants’ decision to donate was to please God. They noted that in the process of deciding to donate, they surrendered to God’s will and aimed to return a deposit to Him: Undergoing such a fate was God’s will. A child is God’s best gift for parents. He gave a child to us as a deposit and reclaimed it again. (Family 6) The success was God’s will because the doctor had said that he didn’t think my husband’s organs were suitable for donation. (Family 4)
Experiencing and understanding senses of beneficence and altruism
The participants empathized with the recipients and expressed their satisfaction at seeing recipients’ recovery. They had good feelings about their ability to promote several persons’ recovery and save their lives. Moreover, they were truly worried about the development of senses such as indebtedness and shamefulness among recipients: I told the administrators of the center that it isn’t necessary to establish face-to-face contact between me and recipient families because they might feel ashamed. (Family 11)
Believing in the enhancement of the deceased persons and their families’ spiritual status
The participants noted that deciding to donate had provided them and their dead loved one with spiritual rewards from God. They also believed that donation was associated with recipients’ being prayerful for their dead member: This can be some kind of good righteous deeds for our dead member. Those who are living with his organs may remember him more than us and say prayer for him. (Family 5)
Enhancing others’ motivation for donation
The donor families highlighted the need for encouraging other people to donate. Therefore, they had either signed organ donation form or verbally communicated their will for donation of their own organs. Besides, they believed that their decision to donate has motivated others to become donation volunteer: The outcome of this decision was the enhancement of others’ motivation for organ donation. All our relatives, particularly the young adults, filled out and signed the organ donation form. (Family 7)
Discussion
The aim of this qualitative study was to explore the outcomes of organ donation for the families of brain-dead patients. The participants had experienced different outcomes after deciding to donate. The main category of the study showed that families’ decision to donate can be a challenging experience which ranges from conflict to confidence, satisfaction, and transcendence.
Transcending outcomes were a novel and interesting finding of the study. This finding has not been reported by previous studies. The results of a study into the negative and positive outcomes of families’ decision to organ donation reported “having a feeling of reward for helping others” and “having an increased appreciation of life” as the positive impacts of donation. 10 Researchers in another study also conceptualized the positive aspect of donation as “serenity in eternal freedom.” 30 Other studies also investigated stability and satisfaction of decision as the positive outcomes of donation. 11,12 However, besides feelings of serenity, confidence, and satisfaction, the participants of this study pointed to the acquisition of transcendent beliefs, humanistic emotions, and internalized experiences due to deciding to donate. Outcomes such as surrender to God’s will, cultivation of a better spiritual attitude, enhancement of their own and their dead members’ spiritual status, and change of others’ attitudes toward organ donation were considered by the participants as valuable outcomes of their decision to donate.
In a loss situation, decision to donate is a strategy for donor families to change their situation toward a positive meaning. 31 This might be true in the early phases of deciding to donate in the difficult and complicated situation of a loved one’s brain death and an anticipatory loss. However, while experiencing loss-related challenges, feelings, and emotions, our participants had also experienced transcending outcomes of donation.
Grief theorists have proposed the theory of “Grief to personal development.” This theory holds that grief can lead to personal development. Most grief-related theories are based on overcoming grief and returning to normal life; however, the “Grief to personal development” theory originates from qualitative changes due to the loss of a loved one. This theory explains a route from grief to finding a new meaning in life. 32 The nature of grief for families who are asked to donate their dead family members’ organs maybe different from and more complex than grief in other situations. Therefore, the “Grief to personal development” cannot cover all experiences of these families. However, the outcomes of grief in this theory are close to the findings of this study. Facilitating the process of achieving such positive outcomes after the tragedy of a loved one’s loss can help improve bereaved families’ quality of life and enhance the value of organ donation in communities.
One of the findings of this study was “reassuring outcomes.” The participants felt that they made the best decision despite being in a chaotic and difficult situation. They were confident about their own self-efficacy in such a situation and also about the rightness of their decision. One factor behind such confidence was their respect for their dead loved one’s will and intention. Previous studies also reported deceased persons’ will to donate as a significant factor contributing to families’ decision to donate. 3,12,33 Another study also found that the presence of an organ donation card was the most apparent way of conveying deceased persons’ donation-related beliefs to their families. 8 These findings highlighted the necessity for family members’ talking about donation and their donation-related wills. Besides, our findings revealed that knowing a deceased person’s will and intention not only can positively affect families’ decision to donate but also protect families against conflicts.
The participating families had experienced different challenges such as personal and interpersonal conflicts. They had also been accused of selling their loved one’s organs and had faced others’ negative reactions, reprimands, and refusals. Researchers in a study also reported that donor family members undergone considerable stress due to their own controversies over the decision as well as others’ devaluation of donation because of the acceptance of money paid to them by hospital as a reward. 10 Similarly, the findings of a previous study also showed that donor families are accused of getting money for donation. 30
Significant others’ approval of donor families’ decision to donate has a significant role in enhancing families’ confidence about their decision. Contrarily, negative reactions can cause families considerable stress, discomfort, uncertainty, and regret. The findings of this study showed that although some participants had experienced pangs of temporary regret, they had finally resolved their uncertainties and were satisfied with their decision. These findings highlighted the necessity to clarify legal issues relating to the donation of a brain-dead patient’s organs and also to provide education to communities based on their educational needs.
The participants had felt feeling of guilt and pangs of conscience due to paying no attention to their brain-dead members’ beating heart and consenting to donate. Categorized as personal conflicts, these feelings showed the participants’ poor understanding of brain death. The results of a study in Taiwan also showed donor families’ difficulties in accepting brain death despite their decision to donate. 34 Other studies also showed that 28.9% of donor families had not understood brain death 33 and 60.2% were confused about brain death and its acceptance. 35 Donor families usually experience high level of stress after their members’ brain death and cannot understand and accept that their brain-dead member who has a warm and pink face is really dead. 36 Besides, the expression “brain death” is a technical term which describes death using several neurologic criteria, about which lay people have poor understanding. Therefore, contrary to cardiac death, brain-dead people’s family members do not consider brain death as real death and thus they need extensive information about it. 37
Besides, providing necessary informational and emotional support during and after making decision to donate can reduce the probability of experiencing irritating outcomes such as doubtful thoughts, feelings of guilt, and pangs of conscience.
Another main challenge experienced by the participants was concerns related to communicate with transplant recipients. Families who had communicated with the recipients referred to this communication as a positive outcome. On the other hand, families who could not communicate with recipients despite having the desire for it considered it as a negative outcome. Donation was reported to be a mechanism for maintaining relationship with the deceased person through identifying and communicating with recipients. Therefore, donor families consider it as a defense mechanism against grief. Inability to establish such communication can leave donor families with the feelings of guilt, depression, anxiety, and deeper grief. 38 Another study into donor families’ experiences of communicating with recipients showed that such a communication helps donor families fulfill their need for appreciation as well as their need for overcoming loneliness caused by their loved one’s death. 39 The findings of a qualitative study in Iran also showed that Iranian donor families tend to communicate with recipients. 30 However, contrary to the findings of previous studies, some of our participants were doubtful about communicating with their recipients in order not to cause them trouble, discomfort, or feeling of indebtedness. Other reasons behind such doubtfulness were donor families’ concerns over experiencing discomfort or negative emotions during or after communicating with recipients. The findings of another study into recipient families’ emotional and psychological experiences of communicating with donor families also showed that such communication can cause some degrees of anxiety to recipients. Accordingly, they recommended that in order to minimize the negative effects of anxiety on transplant success, such communication should be established under the close supervision of counseling specialists and psychologists. 40 All these findings denote the ethical and technical sensitivity of donor–recipient communication and highlight the importance of considering the preferences of both donors and recipients.
Organ donation is a multifaceted issue which includes financial, ethical, moral, psychological, legal, social, and cultural aspects. The promotion of each aspect has a significant role in the success of organ procurement organizations. 30 It also should be taken into account that organ donation is a death-and-life situation which greatly affects the involved people. Decisions which are made according to the principles of donation ethics and based on a clear understanding of all aspects of donation can alleviate the pain and suffering of donor families. Thus, both communities and healthcare providers need to adopt a positive and objective therapeutic approach to the ethical, religious, and social issues of organ donation. 41
Conclusion
The findings of the study reveal that besides senses of confidence and inner peace, organ donation has other positive outcomes such as spiritual, altruistic, and cultural transcendence. The main category of the study was “Decision to organ donation: a challenge from conflict to transcendence” which denotes that donor families experience different difficulties during and after making decision to donate. In other words, confidence and transcendence are achieved through undergoing a difficult process. Donor families’ experiences of the difficulties and the outcomes of organ donation are affected by different factors including the process of donation request, families’ own conditions and information, and the immediate socio-cultural context.
The findings of this study open up new horizons. It was found that the negative outcomes of donation are not limited to doubtfulness and regret. Rather, decision to donate faces families with a wide range of challenges and difficulties which together with the grief at the loss of a loved one bring about a complex difficult situation for the families. On the other hand, healthcare professionals and organ procurers may consider giving consent to donate as the end of families’ donation-related negative experiences. In other words, the ethical responsibility to provide care for donor families may be missed after deciding to donation.
However, the study findings show that post-decision phase is also full of complexities and difficulties with which donor families may not be able to cope effectively. In order to promote positive outcomes of donation, healthcare professionals need to facilitate the process of achieving confidence and transcendence by families. It is noteworthy that families’ inability to cope with donation-related challenges may negatively affect positive outcomes of donation, reduce families’ quality of life, and reduce others’ motivation for donation. Therefore, organ procurement organizations should be responsible both to the needs of society and the special needs of families who are exposed to such a moral decision making. No doubt by following ethical goals in this process will design environment with the ability to promote values that favor the community.
Future studies are recommended to evaluate the effects of planned interventions on the outcomes of donation. Moreover, concerning the effects of the immediate socio-cultural context on donation-related outcomes, replication of this study in other communities is recommended.
Footnotes
Acknowledgements
The authors would like to thank the Transplant Center of Mashhad University of Medical Sciences, Mashhad, Iran, as well as all donor families who shared their experiences.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.