
Abstract
Background:
Pediatric nurses experience ethically difficult situations in their everyday work. Several studies have been conducted to reveal ethical issues among pediatric nurses; we do not think their ethical difficulties have been explored sufficiently from their own perspective.
Objectives:
This study aimed to explore the ethical difficulties faced by pediatric nurses during bedside care for hospitalized children.
Methods:
A phenomenological approach was used to collect and analyze interview data from 14 female pediatric nurses in South Korea.
Ethical considerations:
Ethical review was obtained from an ethics committee. The participants were informed about the aim of the study, and voluntary participation, anonymous response, and confidentiality were explained to them.
Findings:
Three themes emerged from the analysis: ethical numbness in a task-oriented context, negative feelings toward family caregivers, and difficulty in expressing oneself in an authoritative climate.
Keywords
Introduction
The United Nations’ Convention on the Rights of Children declared, “the child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection, before as well as after birth.” 1 As ill children are particularly vulnerable, caring for hospitalized children involves an ethical commitment to have relevant knowledge and technical skills to safeguard the patient and to provide high-quality care. 2
Ethical nursing practice refers to what the nurse ought to do to uphold the principles of morally good and right practice. 3 Undoubtedly, the central concern in pediatric ethics is that of doing what is in the best interest of children 4 and nurturing children’s capacity to make independent choices that are in their own best interest. 5 Thus, pediatric nurses are concerned about how appropriate their conduct is with respect to the best interest of pediatric patients and family caregivers, and they take on the important role of mediating the relationships between physicians, family caregivers, and pediatric patients. 6
Unfortunately, pediatric nurses experience ethically difficult situations in their everyday work. For example, pediatric nurse practitioners are concerned about the protection of the child’s rights (e.g. confidentiality, child’s permission, and autonomy) on certain issues, particularly child abuse or sexual behavior. 7 Nurses who care for children with cancer had concerns about deciding on treatment levels and providing care that impairs the child’s growing autonomy. 8
To our knowledge, there is currently no consensus on the definition of ethical difficulties. However, these difficulties have been generally considered to be ethically difficult situations 9 –11 and include ethical issues and ethical dilemmas. 12,13 In the case of ethical dilemmas, there is a conflict between at least two ethical principles; therefore, the nurse experiences difficulty in deciding between two or more alternatives that are equally acceptable or unacceptable. 14 Thus, in this study, the authors use the term “ethical difficulties” to refer to ethically difficult situations related to ethical issues, ethical dilemmas, and moral distress, which is the stress that is experienced due to ethical dilemmas. 15
Thus far, numerous studies have been conducted to examine ethical issues involving children within medical contexts, such as pediatric end-of-life care and/or ethical decision-making. 6,16 –18 children’s rights, 19,20 and child abuse and neglect. 4,21 Some studies 2,7,22,23 explored pediatric nurses’ ethical situations. The major ethical issues in the pediatric intensive care unit included parents refusing treatment, informed consent for treatment (“who decides?”), futile care, end-of-life decision-making, and different attitudes and perspectives on treatment. 23 Pediatric nurse practitioners’ ethical conflict occurred in child/parent/practitioner relationships, particularly in the case of child abuse and confidentiality regarding sexual behavior and pregnancy. 7 Pediatric nurse practitioners are concerned about the child’s autonomy being undermined by the parent, but, however, they need to maintain a supportive relationship with families. 7 Pediatric nurses experienced emotional pain when remembering the children they overlooked and recognized their own bad conscience. 22 Wagner and Hendel 2 identified and compared ethical situations, nurses’ familiarity with the code of ethics, resources for support, and causes of ethical dilemmas between Israeli and foreign pediatric nurses. They concluded that the majority of ethical dilemmas among pediatric nurses are universal, but that their cultural backgrounds should be considered as a factor influencing nurses’ ethical issues.
Although several studies have been conducted to reveal ethical issues among pediatric nurses, we do not think their ethical difficulties have been explored sufficiently from their own perspective. In order to provide support to pediatric nurses, it is very important to reveal and understand their ethical difficulties in their own voices.
The aim of this study was to qualitatively explore the ethical difficulties experienced by pediatric nurses in providing bedside care, from their own perspectives, by also accounting for the impact of their cultural background. This study will enhance our understanding of pediatric nurses’ ethical difficulties, including ethical issues, ethical dilemmas, and moral distress. The findings will facilitate the development of solutions to such difficulties and will contribute to improving the quality of pediatric nursing care.
Methods
Design
This study used Giorgi’s 24 phenomenological research method. Giorgi’s 24 phenomenological method is rooted in Husserl’s phenomenological approach, which focuses on descriptions of individuals’ experiences of a given event or phenomenon to comprehend the meaning of those experiences from the perspective of these individuals. Phenomenology is the study of lived experiences as they appear through consciousness, which consists of a dialogue between a person and the world. 25 Lived experiences are those that we live through, from moment to moment, in everyday life. 26 Thus, phenomenology is “a method for investigating the structures of consciousness and the types of objects that present themselves to consciousness.” 24
Participants/setting
Pediatric nurses were recruited from six hospitals (a national university hospital, a private university hospital, two medical centers, and two children’s hospitals) in the southern area of South Korea, via snowball sampling. The pediatric unit in each of the six hospitals has about 20–30 beds and about 10–20 nurses. One of the coauthors had worked as a pediatric nurse in the selected national university hospital, and she invited other pediatric nurses who she knew. The inclusion criterion was having worked as a pediatric nurse in a pediatric unit for at least 1 year. There were no restrictions on participants’ age or gender. Participants who were interested in the research topic participated voluntarily; two nurses refused to participate because of a lack of time. There were no dropouts during data collection and analysis.
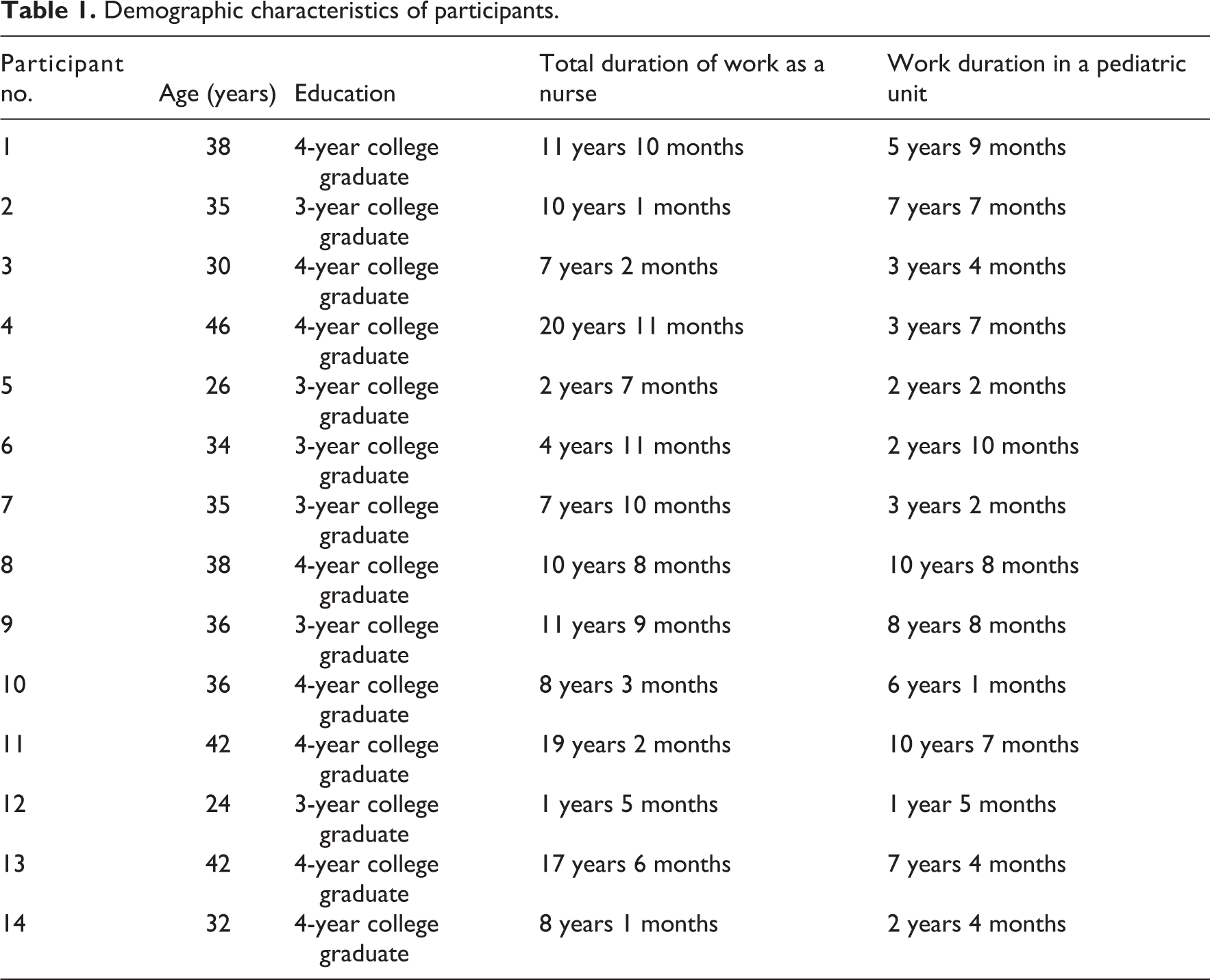
As a result, 14 Korean female pediatric nurses participated in this study until “data saturation” was achieved (Table 1). The average age of the participants was 35 years, with a range of 24–46 years. The average duration of their work experience as a pediatric nurse was about 5 years, ranging from 1 year and 5 months to about 10 years. Six of the nurses had a 3-year associate degree and eight nurses had a 4-year Bachelor of Science in Nursing. At the beginning of the first interview, participants responded to a simple questionnaire on their general characteristics, such as age, gender, educational background, and work experience, after providing informed consent.
Demographic characteristics of participants.
Ethical considerations
The institutional review board of the author’s university approved the study. The participants were informed of the purpose and method of the study and their right to withdraw their participation at any time. The data collection was conducted once the nurses had signed the informed consent form voluntarily.
Data collection
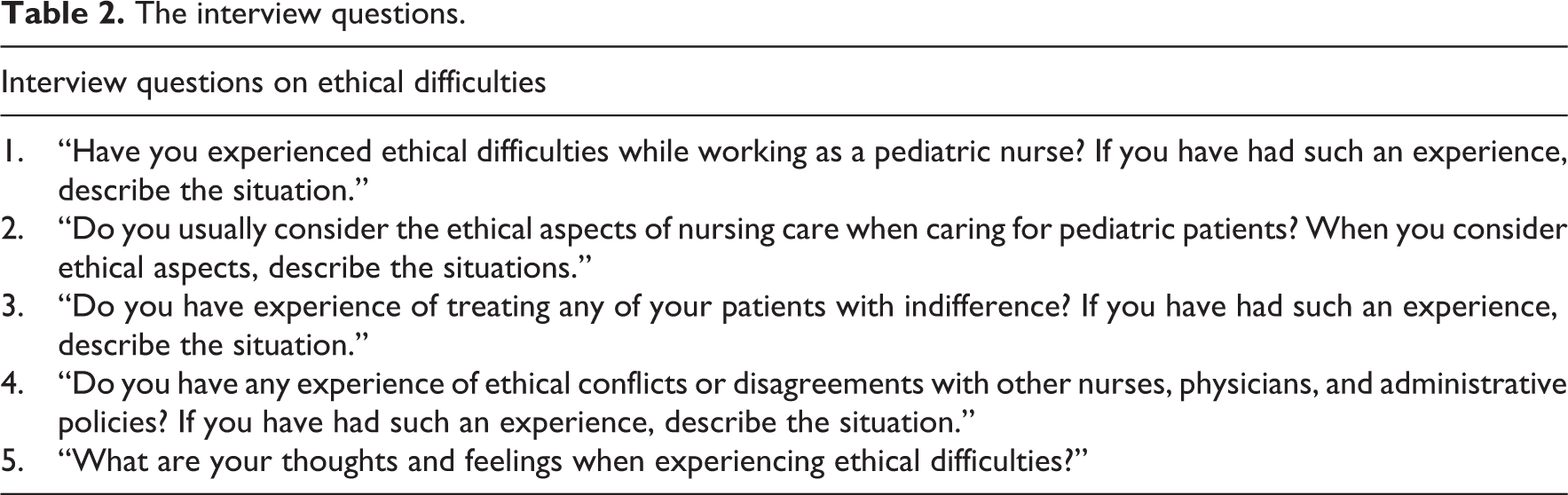
The 14 pediatric nurses were individually interviewed, face-to-face, by the same interviewer (one of the authors). The participants decided the time and location of the interview at their convenience. All participants wanted to be interviewed in a quiet café located near their house, and each interview session lasted for approximately 30–60 min. Unstructured, open-ended questions regarding the ethical difficulties they experienced when caring for children in clinical setting were asked. Interview questions (Table 2) were developed based on the list of nurses’ moral problems suggested by Johnstone. 27 During the interviews, efforts were made to ensure that participants had ample time to share their experiences without interruption. To prevent any omission of the interview data, all interviews were audio-recorded with the participants’ consent, and one of the authors transcribed the interview data.
The interview questions.
Data analysis
Giorgi’s 24 method was used to conduct a three-tiered analysis to describe the participants’ experiences. In the first step, each author read the interview data about three to five times. Each author attempted to obtain a sense of the situation of pediatric nurses’ ethical difficulties and to maintain an attitude of phenomenological reduction. This attitude refers to bracketing the author’s past knowledge about a phenomenon to encounter it freshly, to describe it as it is experienced by the participant, and to consider what is being experienced, as precisely as possible, in terms of the participant’s own perspective. 28 Thus, we tried to avoid leading questions and have a neutral attitude toward the topic, without judging the participants’ response, whether it was right or wrong.
In the second step, authors divided the transcripts into meaning units. Each author demarcated the meaning units in the interview transcripts independently. For example, Nursing work, in general, often involves following prescriptions or orders rather than making an autonomous decision. It is not possible to refuse or ignore the prescription system/There have been incidences in which I felt that this wasn’t right. Why should I follow this [order]?/However, there were no situations in which I could decide, so I could not carry out my duties if I cared about all those conflicts. (Participant 8)
Examples of the third step of the data analysis process.
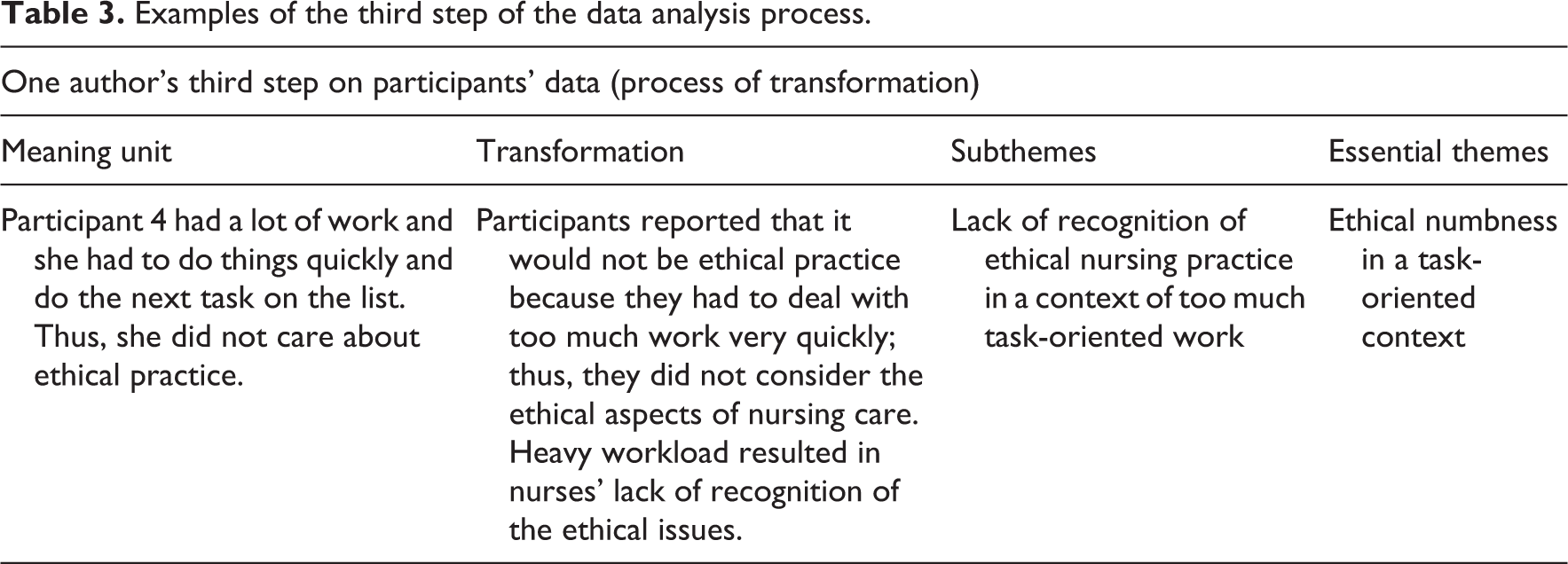
After each author completed all the three steps of the data analysis, all the authors met once a week, over a period of several weeks, to compare the meanings of each coded theme and to extract common themes. While comparing the data previously coded by each author, an agreement was reached on each theme until all the authors agreed. Fortunately, there was no significant disagreement regarding the meaning of the data. When categorizing each subtheme into more abstract concepts, the authors discussed continuously to reach consensus on the main themes. One of the authors was responsible for summarizing the analysis for the coded themes.
In qualitative research, validity pertains to whether the study findings have been interpreted correctly. To ensure trustworthiness of this study, we attempted to describe the methods and procedures of data collection and analysis in detail, and we invited the participants to review the analyzed data to confirm the accuracy of the contents of the data they provided. Several participants were part of the review process and confirmed that the results were consistent with their experience.
Results
Three main ethical difficulties emerged from the interviews with pediatric nurses: ethical numbness in a task-oriented context, negative feelings toward family caregivers, and difficulty in expressing oneself in an authoritative climate.
Ethical numbness in a task-oriented context
Most participants stressed on the ethical numbness toward ethical nursing practice in a task-based nursing environment, wherein rapid completion of tasks under a heavy workload was preferred over providing ethical care. As they were busy, the participants treated pediatric patients as immature beings rather than respecting them as a human being, and they failed to follow standard protocol while providing treatment, considering such protocol bothersome and inconvenient. “As I had a lot of work, I needed to get things done quickly and take care of the next task on the list. So I wasn’t able to put much care into it [ethical practice]” (Participant 4), “The biggest problem is that many nurses are not aware of this issue” (Participant 11), “Work is the priority in any way, though nursing is a profession in which we treat a person. As there is a lot of work and few people, we are overwhelmed with work, we don’t care about it [ethical practice]” (Participant 14).
Ethical numbness in a task-oriented work environment elicited negative emotional reactions such as shame or remorse toward pediatric patients. Participants who felt that they were unable to practice nursing care to benefit the pediatric patients indicated that they felt sorry, ashamed, and distressed: “I feel sorry about the times when I ignored the child and aggressively pursued my own tasks” (Participant 9). “Now that I think about it, I feel terribly sorry…or if there is a more meaningful word than sorry, I want to apologize to the patients. I feel awful about it” (Participant 13).
Sometimes, ethical numbness led to ethically wrong behaviors. For example, nurses delegated oral administration of medications or simple treatments to family caregivers, overlooked a child’s pain, used unnecessary restraints, unnecessarily isolated family caregivers from patients, and disregarded patients’ explanations or demands: When I was giving shots to the children, I was concerned about the necessity of isolating the family caregivers from the patients. Most patients or parents wish to observe it, unless [they would rather not] for personal reasons, but, in many cases, we isolate them because we feel that it is inconvenient or we are nervous. Many times, I thought that such practice is more for us that it is for the patients or the family caregivers. (Participant 1) When taking over a new patient, I feel as if there is too much gossip…about the patients’ private affairs, not just about practical problems that they are facing…I often felt these things, that if a patient or a family caregiver overheard what we talk about them during the takeover, they would feel offended. There were many times like that. (Participant 12)
Negative feelings toward family caregivers
Participants expressed negative feelings toward family caregivers as one of the main barriers to ethical caring. Negative perceptions and feelings were aroused when they had conflict with family caregivers or caregivers’ opinions were valued over those of the patient. Participant 2 referred to family caregivers and pediatric patients as if they were the same people, demonstrating that family caregivers were as important to nurses as were the patients. Participants experienced negative feelings toward family caregivers who showed a lack of understanding, were demanding, used derogatory language toward patients/nurses, acted as though they were knowledgeable, looked down upon nurses, only thought about their own children, or came from foreign backgrounds. Such negative feelings toward family caregivers were in turn transferred to pediatric patients, leading the nurses to exhibit ethically problematic behavior, such as neglect: “When the family caregivers do not understand what we were saying after repeated explanations, we tell them, ‘we will just do it, so leave it to us’…we do not explain anymore” (Participant 10). “When the family caregivers complain a lot…once I pinched the baby during treatment because I hated them” (Participant 3). Furthermore, participants experienced ethical difficulties when they observed family caregivers refusing to consent to treatment for patients owing to religious beliefs, poverty, or mistrust of the medical team, or behaving unethically toward children with disabilities by abandoning or physically abusing them: We had a patient whose parents were Jehovah’s Witnesses, and they refused to consent to a blood transfusion when the patient was in need of it. No matter how much the doctors and nurses tried to persuade them, they would not listen. (Participant 2)
Difficulty in expressing oneself in an authoritative climate
Participants reported that they experienced ethical difficulties when they could not express their opinion in favor of patients and family caregivers during clinical decision-making. Participants believed that it was difficult to express their opinions about treatment to physicians owing to the physician-centered authoritative climate of hospital. They thought that this “difficulty in expressing oneself” resulted from the lack of autonomy and perceived the lack of autonomy as an obstacle to ethical caring. Consequently, the present participants, who are meant to serve as patients’ defenders and advocates as a nurse, merely followed orders from physicians or watched passively when physicians enforced treatments or made mistakes: Nursing work, in general, often involves following prescriptions or orders rather than making an autonomous decision. It is not possible to refuse or ignore the prescription system. There have been incidences in which I felt that this wasn’t right. Why should I follow this [order]? (Participant 8)
Participants also said that they had no opportunity to express and discuss their ethical difficulties in the hospital. “Not many people are concerned about ethical issues” (Participant 14). “There was a conference on the topic of ethics, but it is not held frequently, so awareness is not that high, and many issues are dealt with in a case-by-case manner” (Participant 2). Although some participants indicated the necessity of counseling or education regarding ethical issues in nursing practice within the hospital, most participants believed that individuals’ characters or morals were the most important determining factors of ethical behavior. Some participants also mentioned that personal experience, such as getting married or having children, helped them recognize the importance of ethical sensitivity in nursing and ultimately helped them to treat pediatric patients with respect. These participants believed that ethical sensibility was cultivated in nurses as they become parents and begin to regard pediatric patients in the same light as they did their own children: “After I got married, I cared more for the patients. I think about what I would do if this patient were my child. I tend provide more care to patients who resemble my child” (Participant 10).
Discussion
This study explored the ethical difficulties faced by nurses who care for pediatric patients in hospitals. Interviews with pediatric nurses revealed ethical difficulties such as ethical numbness because of the task-centered context of nursing care (as opposed to a patient-centered context), negative feelings toward patients’ family caregivers, and difficulty in expressing oneself in an authoritative climate.
In this study, participants stressed on ethical numbness as one of major ethical difficulties. According to Sørlie et al., 22 pediatric nurses experienced emotional pain when remembering the children they overlooked. In this study, the pediatric nurses reported that they could not provide patient-centered care sufficiently because of the heavy workload and lack of time. Although there may be many reasons for the nurses’ heavy workload in the hospital, nursing shortage might be one of the reasons. “The inability to treat patients appropriately due to the shortage of human resources” was the most common ethical situation encountered by pediatric nurses. 2 Furthermore, insufficiency of human resource management (fewer nurses and more patients) is associated with nursing errors and risk of patient trauma, and such errors have been found to lead to moral distress in nurses. 22,29,30 As a result, ethical numbness from heavy workload could be resolved by having adequate nursing staff and reducing the number of hours spent in performing routine tasks. Therefore, the nursing work system in hospital needs to be upgraded to focus on patients rather than on routine work, to ensure ethical nursing practice.
Having negative feelings toward patients’ family caregivers was another main ethical difficulty among the pediatric nurses in this study. This result implies that family caregivers assume an important position in pediatric nursing. Family-centered pediatric care is necessary in pediatric nursing, 31 but unfortunately, pediatric nurses in this study considered family caregivers as a source of ethical difficulties. Traditionally, the healthcare team considers the child’s parents as the most appropriate decision makers 32 because children rely on their parents and family. 33 Ethical dilemmas most commonly occur when parental preference and the child’s best interest contradict each other and when the family’s cultural background does not fit well with those of the medical team. 7,34,35 However, these ethical dilemmas were not the major problems expressed by the nurses in this study. For pediatric nurses in this study, negative feelings toward family caregivers was a main factor affecting ethical difficulties. It was difficult to work when parents are angry, rude, distrustful, confrontational, or demand special attention. 36
Family caregivers and pediatric nurses are inseparable from each other. Nurses are expected to provide care for family caregivers as well, despite the ethical difficulties caused by the latter. Most of all, parents have an obligation to ensure the survival of their children and mitigate or prevent pain. 5 Therefore, pediatric nursing must consider the provision of family-centered care, in which parents are included in all aspects of treatment and care such as daily activities of child care (e.g. feeding, dressing, bathing, sleeping, and playing), giving oral medicines and observing symptoms as well as decision-making, and nurses must engage in close, collaborative relationships with parents. 36,37 Therefore, even with disrespectful or unreasonable family caregivers, pediatric nurses should make efforts to enhance communication, build trust, and improve relationships for the sake of the children’s health. In this context, it is relevant to consider how the nurses’ negative feelings toward family caregivers could be resolved. While family caregivers’ burden and stress, in particular regarding cancer or chronic disease, have received nursing researchers’ attention, 38 –40 pediatric nurses’ stress resulting from family caregivers has not. We have to focus on pediatric nurses’ emotions as well as on those of family caregivers and develop various strategies such as counseling or ethics rounds for pediatric nurses, to prevent from negative feelings toward family caregivers.
The result of this study showed that pediatric nurses also faced difficulties in terms of expressing their opinions about treatment to physicians and/or family caregivers. Malloy et al. 41 referred to this phenomenon as the “silenced voice.” In the context of ethical decision-making, nurses’ voices were often silenced by the system, physicians, and patients and their families and were sometimes restricted voluntarily. 41 According to Malloy et al., 41 Korean nurses were less dismayed than were Australian, Canadian, and Irish nurses, who believed that they should be heard. This reflects a cultural difference in nurses’ perception.
Advocacy of the patients’ needs and welfare is a fundamental part of the nurse’s role. However, nurses are not included in discussions regarding ethical decision-making. 42,43 Nurses recognize that they are less able than physicians to participate in decisions, and therefore, they experience discomfort due to the hierarchical difficulties. 8,30 In Korea, nurses believe that they have less autonomy than the other health professionals do, 44 and they perceive the nursing organizational culture in hospitals as conservative and hierarchical. 45 Nurses should care for patients and respond to their and their family’s needs and demands, but institutional constraints such as a lack of facilities, lack of power to enact institutional change, and organizational policies and procedures cause nurses moral distress, ultimately leading to nurses’ dissatisfaction and a reduction in the quality of care. 30 Moreover, an inhibitive medical power structure, and institutional policies or legal considerations have been found to be causative factors for moral distress in nurses. 46 –48
Nurses felt lonely because of the lack of an open dialogue about ethical difficulties. 22 It is important that nurses have the opportunity to express their ethical concerns and discuss ethics and perceived access to advice and support. 46 Ethical climate in hospitals is the most important factor affecting nurses’ positional and professional turnover intentions. 49 Nurses who had opportunities to discuss ethical concerns found such opportunities personally and professionally sustaining. However, majority of the nurses did not have these opportunities. 50 In order to deal with nurses’ ethical difficulties, institutional support structures such as ethics education, ethics rounds, committees, and consultations and peer support meetings are required. 51,52 As a nurse’s ability to solve ethical problems is affected by the organization’s ethical climate, 46,49 there is a need to improve the ethical climate in hospitals.
This study was limited in that all the pediatric nurses who participated are female nurses who work in pediatric units of hospitals in only one region of South Korea. Therefore, the findings of this study may have limited application to other pediatric nurses working in other hospitals, regions, or countries, and to male nurses. Additionally, we did not consider the demographic characteristics and differences in work duration in pediatric units during data collection and analysis. However, we suggest that our major findings relate to nurses in many countries, particularly perhaps to junior and student nurses and unqualified nursing assistants. The findings are also relevant for senior nurses, either directly in their own practice or in how they can support their juniors and work to improve the ethical climate and routines in their services.
Conclusion and implications
The results of this study highlighted a need to develop guidelines to help pediatric nurses deal with their ethical difficulties. For example, we suggest the implementation of the Magnet Recognition Program, developed by the American Nurses Credentialing Center, to recognize healthcare organizations that provide nursing excellence. The Magnet Recognition Program included transformational leadership and structural empowerment for nurses. 53 This program supports nurses in achieving their ethical and professional responsibilities. We need to develop strategies to manage ethical difficulties at an institutional level.
Furthermore, it is important that pediatric nurses have the opportunity to communicate with fellow nurses and other medical staff regarding ethical difficulties. A counseling office should be prepared to receive consultations about ethical difficulties. In addition, cultivation of pediatric nurses’ moral, ethical, and philosophical thinking patterns requires the immediate provision of continuous education in nursing ethics at the site of clinical nursing, time to discuss ethical difficulties, and other supportive measures (e.g. the development of continued education, guidelines on ethics, and a clinical ethics support service). Above all, improving nurses’ attitudes toward pediatric patients’ rights is of the utmost importance.
For future research, we need to explore how pediatric nurses deal with their ethical difficulties using the grounded theory methodology and to develop educational programs to cultivate ethical sensitivity to combat ethical numbness among pediatric nurses and evaluate the effects of such programs.
Pediatric nurses should be aware of children’s rights and know how to respect children’s dignity and provide good care. This study is important because it analyzed pediatric nurses’ ethical difficulties from these nurses’ perspectives. The pediatric nurses have experienced ethical difficulties with respect to their ethical numbness, family caregivers’ demands, and interacting with physicians in the authoritarian climate of hospitals. Therefore, in order to provide ethical care to pediatric patients and their family caregivers, the nurses should be given opportunities to express and discuss their ethical difficulties, which would enable them to fulfill their roles as a defender of pediatric patients’ rights.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Chung-Ang University Research Grant, Seoul, Republic of Korea.